
Symptomatic SARS-CoV-2 Infection with Ageusia after Two mRNA Vaccine Doses

 , ,
, , 
{kind=link}
Abstract
:1. Introduction
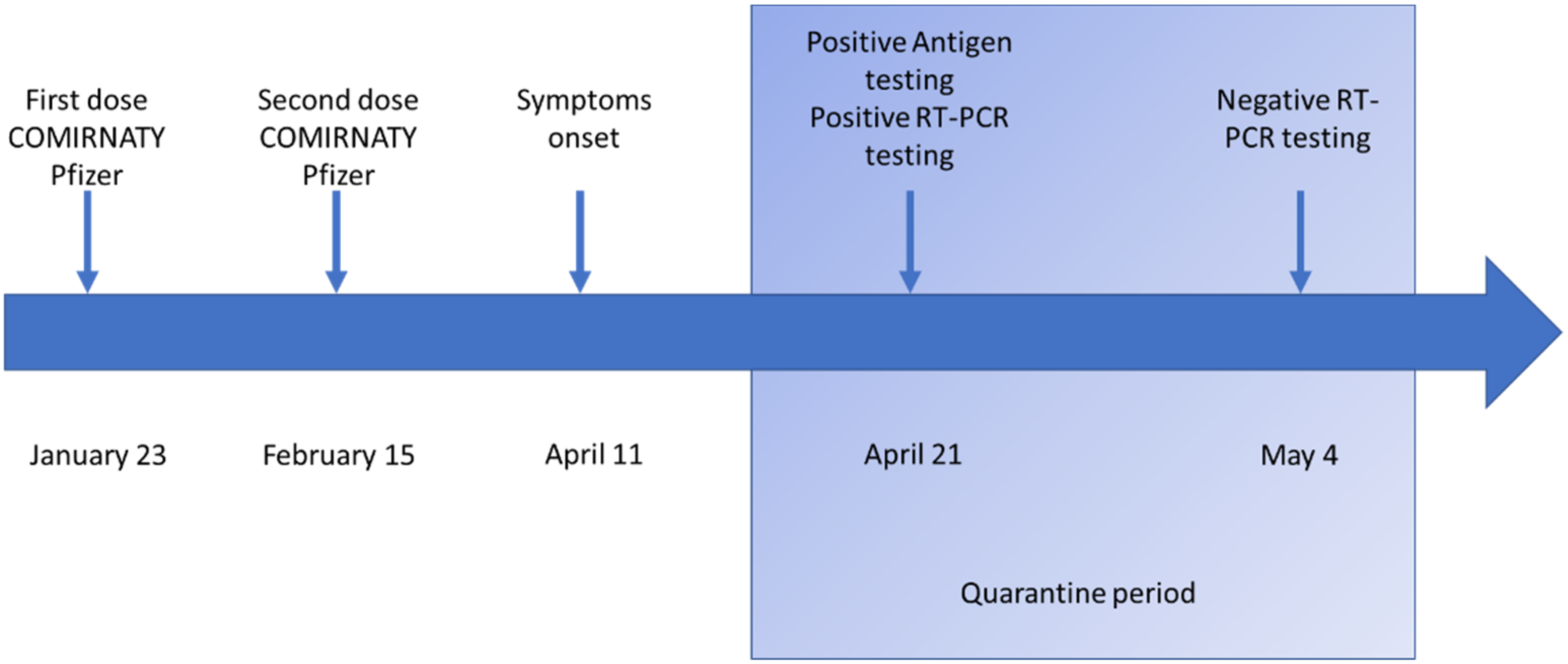
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Dagan, N.; Barda, N.; Kepten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernán, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 mRNA COVID-19 Vaccine in a Nationwide Mass Vaccination Setting. N. Engl. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef] [PubMed]
- Brussow, H. mRNA vaccines against COVID-19: A showcase for the importance of microbial biotechnology. Microb. Biotechnol. 2022, 15, 135–148. [Google Scholar] [CrossRef] [PubMed]
- Grupper, A.; Rabinowich, L.; Schwartz, D.; Schwartz, I.F.; Ben-Yehoyada, M.; Shashar, M.; Katchman, E.; Halperin, T.; Turner, D.; Goykhman, Y.; et al. Reduced humoral response to mRNA SARS-CoV-2 BNT162b2 vaccine in kidney transplant recipients without prior exposure to the virus. Am. J. Transpl. 2021, 21, 2719–2726. [Google Scholar] [CrossRef] [PubMed]
- Angel, Y.; Spitzer, A.; Henig, O.; Saiag, E.; Sprecher, E.; Padova, H.; Ben-Ami, R. Association Between Vaccination with BNT162b2 and Incidence of Symptomatic and Asymptomatic SARS-CoV-2 Infections Among Health Care Workers. JAMA 2021, 325, 2457–2465. [Google Scholar] [CrossRef] [PubMed]
- Kweon, O.J.; Lim, Y.K.; Kim, H.R.; Choi, Y.; Kim, M.C.; Choi, S.H.; Chung, J.W.; Lee, M.K. Evaluation of rapid SARS-CoV-2 antigen tests, AFIAS COVID-19 Ag and ichroma COVID-19 Ag, with serial nasopharyngeal specimens from COVID-19 patients. PLoS ONE 2021, 16, e0249972. [Google Scholar] [CrossRef] [PubMed]
- Ulhaq, Z.S.; Soraya, G.V.; Indriana, K. Breakthrough COVID-19 case after full-dose administration of CoronaVac vaccine. Indian J. Med. Microbiol. 2021, 39, 562–563. [Google Scholar] [CrossRef] [PubMed]
- Hacisuleyman, E.; Hale, C.; Saito, Y.; Blachere, N.E.; Bergh, M.; Conlon, E.G.; Schaefer-Babajew, D.J.; DaSilva, J.; Muecksch, F.; Gaebler, C.; et al. Vaccine Breakthrough Infections with SARS-CoV-2 Variants. N. Engl. J. Med. 2021, 384, 2212–2218. [Google Scholar] [CrossRef] [PubMed]
- Dyer, O. COVID-19: Chinese vaccines may need changes to improve efficacy, admits official. BMJ 2021, 373, n969. [Google Scholar] [CrossRef] [PubMed]
- Prasun, P. COVID-19: A Mitochondrial Perspective. DNA Cell Biol. 2021, 40, 713–719. [Google Scholar] [CrossRef] [PubMed]
- Mancuso, M.; La Morgia, C.; Valentino, M.L.; Ardissone, A.; Lamperti, C.; Procopio, E.; Garone, C.; Siciliano, G.; Musumeci, O.; Toscano, A.; et al. SARS-CoV-2 infection in patients with primary mitochondrial diseases: Features and outcomes in Italy. Mitochondrion 2021, 58, 243–245. [Google Scholar] [CrossRef] [PubMed]
- Stamatatos, L.; Czartoski, J.; Wan, Y.-H.; Homad, L.J.; Rubin, V.; Glantz, H.; Neradilek, M.; Seydoux, E.; Jennewein, M.F.; MacCamy, A.J.; et al. mRNA vaccination boosts cross-variant neutralizing antibodies elicited by SARS-CoV-2 infection. Science 2021, 372, 1413–1418. [Google Scholar] [CrossRef] [PubMed]
- Planas, D.; Bruel, T.; Grzelak, L.; Guivel-Benhassine, F.; Staropoli, I.; Porrot, F.; Planchais, C.; Buchrieser, J.; Rajah, M.M.; Bishop, E.; et al. Sensitivity of infectious SARS-CoV-2 B.1.1.7 and B.1.351 variants to neutralizing antibodies. Nat. Med. 2021, 27, 917–924. [Google Scholar] [CrossRef] [PubMed]
- Duerr, R.; Dimartino, D.; Marier, C.; Zappile, P.; Wang, G.; Lighter, J.; Elbel, B.; Troxel, A.B.; Heguy, A. Dominance of Alpha and Iota variants in SARS-CoV-2 vaccine breakthrough infections in New York City. J. Clin. Investig. 2021, 110, 761–769. [Google Scholar] [CrossRef] [PubMed]
- Rana, K.; Mohindra, R.; Pinnaka, L. Vaccine Breakthrough Infections with SARS-CoV-2 Variants. N. Engl. J. Med. 2021, 385, e7. Available online: https://europepmc.org/article/MED/34077641 (accessed on 21 November 2021). [CrossRef] [PubMed]
- Nixon, D.F.; Ndhlovu, L.C. Vaccine Breakthrough Infections with SARS-CoV-2 Variants. N. Engl. J. Med. 2021, 385, e7. Available online: https://europepmc.org/article/MED/34077640 (accessed on 21 November 2021). [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caponio, V.C.A.; Lipsi, M.R.; Fortunato, F.; Arena, F.; Lo Muzio, L. Symptomatic SARS-CoV-2 Infection with Ageusia after Two mRNA Vaccine Doses. Int. J. Environ. Res. Public Health 2022, 19, 886. https://doi.org/10.3390/ijerph19020886
Caponio VCA, Lipsi MR, Fortunato F, Arena F, Lo Muzio L. Symptomatic SARS-CoV-2 Infection with Ageusia after Two mRNA Vaccine Doses. International Journal of Environmental Research and Public Health. 2022; 19(2):886. https://doi.org/10.3390/ijerph19020886
Chicago/Turabian StyleCaponio, Vito Carlo Alberto, Maria Rosaria Lipsi, Francesca Fortunato, Fabio Arena, and Lorenzo Lo Muzio. 2022. "Symptomatic SARS-CoV-2 Infection with Ageusia after Two mRNA Vaccine Doses" International Journal of Environmental Research and Public Health 19, no. 2: 886. https://doi.org/10.3390/ijerph19020886