
The Efficacy and Effectiveness of Education for Preventing and Treating Non-Specific Low Back Pain in the Hispanic Cultural Setting: A Systematic Review

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
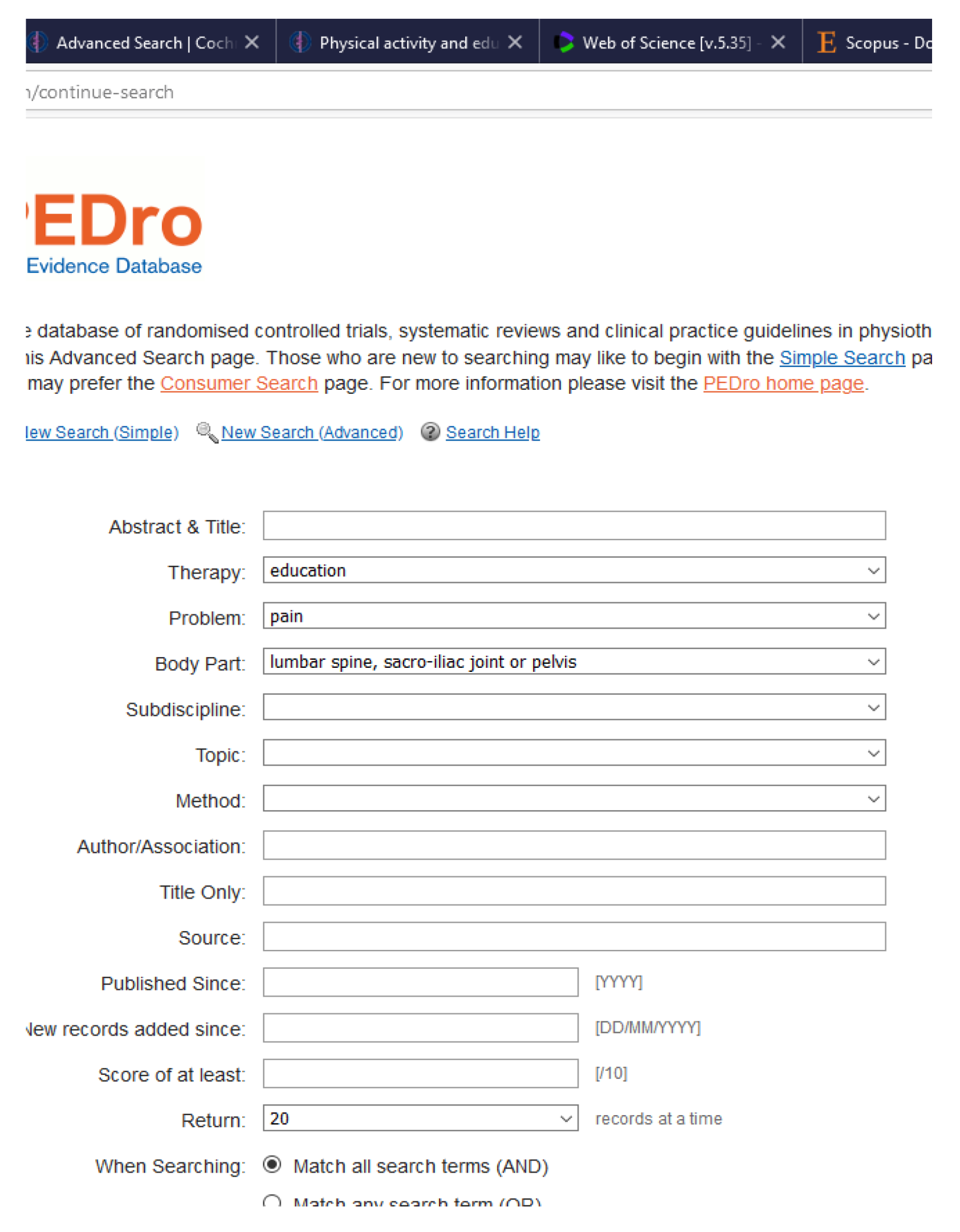
2.1. Search and Study Selection
- (a)
- Design: Randomized controlled clinical trials (RCTs).
- (b)
- Study population: Spanish-speaking, healthy subjects (for studies on prevention) or subjects with LBP, without any age limits. Studies including Spanish-speaking and non-Spanish speaking participants, and studies including participants with and without pain, or with LBP and with other conditions, could be included only when data had been analyzed separately.
- (c)
- Sample size: ≥10 subjects per group must have completed the study.
- (d)
- Interventions: ≥1 group must have received education of any type.
- (e)
- Comparators: natural history, placebo, sham or any health technology intended to prevent or treat LBP (including other types of education).
- (f)
- Outcomes: ≥1 of following outcomes had to have been assessed: pain severity (LBP or referred pain), LBP-related disability, health-related quality of life, knowledge (on strategies to prevent or treat LBP.
- (g)
- Location: studies conducted in any country in which Spanish can be used in Governmental documents and to communicate with the Administration.
2.2. Data Collection Process, Quality Assessment and Data Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A


References
- Waddell, G. The Back Pain Revolution; Churchill-Livingstone: London, UK, 2004; pp. 1–61. [Google Scholar]
- Hartvigsen, J.; Hancock, M.J.; Kongsted, A.; Louw, Q.; Ferreira, M.L.; Genevay, S.; Hoy, D.; Karppinen, J.; Pransky, G.; Sieper, J.; et al. What low back pain is and why we need to pay attention. Lancet 2018, 391, 2356–2367. [Google Scholar] [CrossRef] [Green Version]
- Global Burden of Disease Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1545–1602. [Google Scholar] [CrossRef] [Green Version]
- Van Tulder, M.; Becker, A.; Bekkering, T.; Breen, A.; Gil del Real, M.T.; Hutchinson, A.; Koes, B.; Laerum, E.; Malmivaara, A.; On behalf of the COST B13 Working Group on Guidelines for the Management of Acute Low Back Pain in Primary Care. European guidelines for the management of acute nonspecific low back pain in primary care. Eur. Spine J. 2006, 15, S169–S191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Airaksinen, O.; Brox, J.I.; Cedraschi, C.; Hildebrandt, J.; Klaber-Moffett, J.; Kovacs, F.M.; Mannion, A.F.; Reis, S.; Staal, J.B.; Ursin, H.; et al. European guidelines for the management of chronic nonspecific low back pain. Eur. Spine J. 2006, 15, S192–S299. [Google Scholar] [CrossRef] [Green Version]
- Chou, R.; Deyo, R.; Friedly, J.; Skelly, A.; Hashimoto, R.; Weimer, M.; Fu, R.; Dana, T.; Kraegel, P.; Griffin, J.; et al. Nonpharmacologic Therapies for Low Back Pain: A Systematic Review for an American College of Physicians Clinical Practice Guideline. Ann. Intern. Med. 2017, 166, 493–505. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, C.B.; Maher, C.G.; Pinto, R.Z.; Traeger, A.C.; Lin, C.C.; Chenot, J.F.; van Tulder, M.; Koes, B.W. Clinical practice guidelines for the management of non-specific low back pain in primary care: An updated overview. Eur. Spine J. 2018, 27, 2791–2803. [Google Scholar] [CrossRef] [Green Version]
- Buruck, G.; Tomaschek, A.; Wendsche, J.; Ochsmann, E.; Dörfel, D. Psychosocial areas of worklife and chronic low back pain: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 2019, 20, 480. [Google Scholar] [CrossRef] [PubMed]
- Ramond, A.; Bouton, C.; Richard, I.; Roquelaure, Y.; Baufreton, C.; Legrand, E.; Huez, J.F. Psychosocial risk factors for chronic low back pain in primary care. A systematic review. Fam. Pract. 2011, 28, 12–21. [Google Scholar] [CrossRef] [Green Version]
- Pincus, T.; Burton, A.K.; Vogel, S.; Field, A.P. A systematic review of psychological factors as predictors of chronicity/disability in prospective cohorts of low back pain. Spine 2002, 27, E109–E120. [Google Scholar] [CrossRef]
- Smeets, R.J.; Vlaeyen, J.; Kester, A.D.; Knottnerus, J.A. Reduction of pain catastrophizing mediates the outcome of both physical and cognitive-behavioral treatment in chronic low back pain. J. Pain 2006, 7, 261–271. [Google Scholar] [CrossRef] [PubMed]
- Smeets, R.J.; Maher, C.G.; Nicholas, M.K.; Refshauge, K.M.; Herbert, R.D. Do psychological characteristics predict response to exercise and advice for subacute low back pain? Arthritis Rheum. 2009, 61, 1202–1209. [Google Scholar] [CrossRef]
- Spinhoven, P.; Ter Kuile, M.; Kole-Snijders, A.M.; Hutten Mansfeld, M.; Den Ouden, D.J.; Vlaeyen, J.W. Catastrophizing and internal pain control as mediators of outcome in the multidisciplinary treatment of chronic low back pain. Eur. J. Pain 2004, 8, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Truchon, M.; Côté, D. Predictive validity of the Chronic Pain Coping Inventory in subacute low back pain. Pain 2005, 116, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Wand, B.M.; McAuley, J.H.; Marston, L.; De Souza, L.H. Predicting outcome in acute low back pain using different models of patient profiling. Spine 2009, 34, 1970–1975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kovacs, F.M.; Muriel, A.; Abraira, V.; Medina, J.M.; Castillo Sanchez, M.D.; Olabe, J.; Spanish Back Pain Research Network. The influence of fear avoidance beliefs on disability and quality of life is sparse in Spanish low back pain patients. Spine 2005, 30, E676–E682. [Google Scholar] [CrossRef]
- Kovacs, F.; Abraira, V.; Santos, S.; Díaz, E.; Gestoso, M.; Muriel, A.; Gil del Real, M.T.; Mufraggi, N.; Noguera, J.; Zamora, J.; et al. A Comparison of Two Short Education Programs for Improving Low Back Pain-Related Disability in the Elderly: A Cluster Randomized Controlled Trial. Spine 2007, 32, 1053–1059. [Google Scholar] [CrossRef]
- Albadalejo, C.; Kovacs, F.M.; Royuela, A.; del Pino, R.; Zamora, J.; Spanish Back Pain Research Network. The efficacy of a short education program and a short physiotherapy program for treating low back pain in primary care: A cluster randomized trial. Spine 2010, 35, 483–496. [Google Scholar] [CrossRef]
- Kovacs, F.; Abraira, V.; Cano, A.; Royuela, A.; Gil del Real, M.T.; Gestoso, M.; Mufraggi, N.; Muriel, A.; Zamora, J.; Spanish Back Pain Research Network. Fear Avoidance Beliefs do not influence disability and quality of life in Spanish elderly subjects with low back pain. Spine 2007, 32, 2133–2138. [Google Scholar] [CrossRef]
- Kovacs, F.M.; Noguera, J.; Abraira, V.; Royuela, A.; Cano, A.; Gil del Real, M.T.; Zamora, J.; Gestoso, M.; Muriel, A.; Mufraggi, N. The influence of psychological factors on low back pain-related disability in community-dwelling older persons. Pain Med. 2008, 9, 871–880. [Google Scholar] [CrossRef] [Green Version]
- Moix, J.; Kovacs, F.M.; Martín, A.; Plana, M.N.; Royuela, A.; The Spanish Back Pain Research Network. Catastrophizing, state-anxiety, anger and depressive symptoms do not correlate with disability when variations of trait-anxiety are taken into account. A study of chronic low back pain patients treated in Spanish pain units [NCT00360802]. Pain Med. 2011, 12, 1008–1017. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions. Version 5. The Cochrane Collaboration. 2011. Available online: www.cochrane-handbook.org (accessed on 22 October 2021).
- Furlan, A.D.; Malmivaara, A.; Chou, R.; Maher, C.G.; Deyo, R.A.; Schoene, M.; Bronfort, G.; van Tulder, M.W.; Editorial Board of the Cochrane Back, Neck Group. 2015 Updated method guideline for systematic reviews in the Cochrane Back and Neck Group. Spine 2015, 40, 1660–1673. [Google Scholar] [CrossRef] [PubMed]
- Berenguera, A.; Pujol-Ribera, E.; Rodriguez-Blanco, T.; Violan, C.; Casajuana, M.; de Kort, N.; Trapero-Bertran, M. Study protocol of cost-effectiveness and cost-utility of a biopsychosocial multidisciplinary intervention in the evolution of non-specific sub-acute low back pain in the working population: Cluster randomised trial. BMC Musculoskelet. Disord. 2011, 12, 194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Denis, A.; Zelmar, A.; Le Pogam, M.A.; Chaleat-Valayer, E.; Bergeret, A.; Colin, C. The PRESLO study: Evaluation of a global secondary low back pain prevention program for health care personnel in a hospital setting. Multicenter, randomized intervention trial Randomized Controlled Trial. BMC Musculoskelet. Disord. 2012, 13, 234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García-Martínez, E.; Soler-González, J.; Rubí-Carnacea, F.; García-Martínez, B.; Climent-Sanz, C.; Blanco-Blanco, J.; Valenzuela-Pascual, F. The influence of an educational internet-based intervention in the beliefs and attitudes of primary care professionals on non-specific chronic low back pain: Study protocol of a mixed methods approach. BMC Fam. Pract. 2019, 20, 31. [Google Scholar] [CrossRef]
- Rodriguez-Blanco, T.; Fernández-San-Martin, I.; Balagué-Corbella, M.; Berenguera, A.; Moix, J.; Montiel-Morillo, E.; Núñez-Juárez, E.; González-Moneo, M.J.; Pie-Oncins, M.; Martín-Peñacoba, R.; et al. Study protocol of effectiveness of a biopsychosocial multidisciplinary intervention in the evolution of non-specific sub-acute low back pain in the working population: Cluster randomised trial. BMC Health Serv. Res. 2010, 10, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuesta-Vargas, A.I.; García-Romero, J.C.; Arroyo-Morales, M.; Diego-Acosta, A.M.; Daly, D.J. Exercise, manual therapy, and education with or without high-intensity deep-water running for nonspecific chronic low back pain: A pragmatic randomized controlled trial. Am. J. Phys. Med. Rehabil. 2011, 90, 526–534. [Google Scholar] [CrossRef]
- Beltran-Alacreu, H.; López-de-Uralde-Villanueva, I.; Fernández-Carnero, J.; La Touche, R. Manual therapy, therapeutic patient education, and therapeutic exercise, an effective multimodal treatment of nonspecific chronic neck pain: A randomized controlled trial. Am. J. Phys. Med. Rehabil. 2015, 94, 887–897. [Google Scholar] [CrossRef] [PubMed]
- Díaz-Arribas, M.J.; Kovacs, F.M.; Royuela, A.; Fernández-Serrano, M.; Gutiérrez-Fernández, L.; San Martín-Pariente, O.; Abraira, V.; Ramos-Sánchez, M.; Llorca-Palomera, R.; Pardo-Hervás, P.; et al. Effectiveness of the Godelieve Denys-Struyf (GDS) Method in People with Low Back Pain: Cluster Randomized Controlled Trial. Phys. Ther. 2015, 95, 319–336. [Google Scholar] [CrossRef] [Green Version]
- Valenzuela-Pascual, F.; Molina, F.; Corbi, F.; Blanco-Blanco, J.; Gil, R.M.; Soler-Gonzalez, J. The influence of a biopsychosocial educational internet-based intervention on pain, dysfunction, quality of life, and pain cognition in chronic low back pain patients in primary care: A mixed methods approach. BMC Med. Inform. Decis. Mak. 2015, 15, 97. [Google Scholar] [CrossRef] [Green Version]
- Mas, R.R.; López-Jiménez, T.; Pujol-Ribera, E.; Martín, M.I.F.; Moix-Queraltó, J.; Montiel-Morillo, E.; Rodríguez-Blanco, T.; Casajuana-Closas, M.; González-Moneo, M.J.; Juárez, E.N.; et al. Effectiveness of a multidisciplinary biopsychosocial intervention for non-specific subacute low back pain in a working population: A cluster randomized clinical trial. BMC Health Serv. Res. 2019, 19, 962. [Google Scholar] [CrossRef] [Green Version]
- Grande-Alonso, M.; Suso-Martí, L.; Cuenca-Martínez, F.; Pardo-Montero, J.; Gil-Martínez, A.; La Touche, R. Physiotherapy based on a Biobehavioral Approach with or Without Orthopedic Manual Physical Therapy in the Treatment of Nonspecific Chronic Low Back Pain: A Randomized Controlled Trial. Pain Med. 2019, 20, 2571–2587. [Google Scholar] [CrossRef]
- Galan-Martin, M.A.; Montero-Cuadrado, F.; Lluch-Girbes, E.; Coca-López, M.C.; Mayo-Iscar, A.; Cuesta-Vargas, A. Pain Neuroscience Education and Physical Therapeutic Exercise for Patients with Chronic Spinal Pain in Spanish Physiotherapy Primary Care: A Pragmatic Randomized Controlled Trial. J. Clin. Med. 2020, 9, 1201. [Google Scholar] [CrossRef]
- Moix, J.; Cañellas, M.; Osorio, C.; Bel, X.; Girvent, F.; Martos, A.; Ortigosa, L.; Sánchez, C.; Portell, M.; Multidisciplinary Team for the Management of Back Pain. Efficacy of an interdisciplinary educational program in patients with chronic back pain. Rev. Soc. Esp. Dolor 2003, 11, 141–149. [Google Scholar]
- Abásolo, L.; Blanco, M.; Bachiller, J.; Candelas, G.; Collado, P.; Lajas, C.; Revenga, M.; Ricci, P.; Lázaro, P.; Aguilar, M.D.; et al. A health system program to reduce work disability related to musculoskeletal disorders. Ann. Intern. Med. 2005, 143, 404–414. [Google Scholar] [CrossRef]
- Méndez, F.J.; Gómez-Conesa, A. Postural hygiene program to prevent low back pain. Spine 2001, 26, 1280–1286. [Google Scholar] [CrossRef]
- Díaz-Cerrillo, J.L.; Rondón-Ramos, A.; Pérez-González, R.; Clavero-Cano, S. Non-randomised trial of an educational intervention based on cognitive-behavioural principles for patients with chronic low back pain attended in Primary Care Physiotherapy. Aten Primaria 2016, 48, 440–448. [Google Scholar] [CrossRef] [Green Version]
- Cáceres-Muñoz, V.S.; Magallanes-Meneses, A.; Torres-Coronel, D.; Copara-Moreno, P.; Escobar-Galindo, M.; Mayta-Tristán, P. Efecto de un programa de pausa activa más folletos informativos en la disminución de molestias musculoesqueléticas en trabajadores administrativos. Rev. Perú. Med. Exp. Salud Publica 2017, 34, 611–618. [Google Scholar] [CrossRef] [Green Version]
- Miñana-Signes, V.; Monfort-Pañego, M.; Rosaleny-Maiques, S. Improvement of knowledge and postural habits after an educational intervention program in school students. J. Human Sport Exerc. 2019, 14, 47–60. [Google Scholar] [CrossRef] [Green Version]
- Núñez, M.; Núñez, E.; Yoldi, C.; Quintó, L.; Hernández, M.V.; Muñoz-Gómez, J. A therapeutic education and functional readaptation program for Spanish patients with musculoskeletal chronic diseases. Clin. Rheumatol. 2006, 25, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Berríos-López, Y.; Cádiz-Blackman, J.; Vélez-Hernández, Y.; Venegas, H.L.; Ortiz, A. Effectiveness of a back school program in the application of body mechanics principles. P. R. Health Sci. J. 2009, 28, 48–53. [Google Scholar]
- Téllez-García, M.; de-la-Llave-Rincón, A.; Salom-Moreno, J.; Palacios-Ceña, M.; Ortega-Santiago, R.; Fernández-de-Las-Peñas, C. Neuroscience education in addition to trigger point dry needling for the management of patients with mechanical chronic low back pain: A preliminary clinical trial. J. Bodyw. Mov. Ther. 2015, 19, 464–472. [Google Scholar] [CrossRef]
- del Pozo-Cruz, B.; Gusi, N.; del Pozo-Cruz, J.; Adsuar, J.C.; Hernandez-Mocholí, M.; Parraca, J.A. Clinical effects of a nine-month web-based intervention in subacute non-specific low back pain patients: A randomized controlled trial. Clin. Rehabil. 2013, 27, 28–39. [Google Scholar] [CrossRef] [PubMed]
- Bodes Pardo, G.; Lluch Girbés, E.; Roussel, N.A.; Gallego Izquierdo, T.; Jiménez Penick, V.; Pecos Martín, D. Pain Neurophysiology Education and Therapeutic Exercise for Patients with Chronic Low Back Pain: A Single-Blind Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2018, 99, 338–347. [Google Scholar] [CrossRef]
- Kovacs, F.M.; Oliver-Frontera, M.; Plana, M.N.; Royuela, A.; Muriel, A.; Gestoso, M.; Spanish Back Pain Research Network. Improving schoolchildren’s knowledge of methods for the prevention and management of low back pain: A cluster randomized controlled trial. Spine 2011, 36, E505–E512. [Google Scholar] [CrossRef] [PubMed]
- Vidal, J.; Borras, P.A.; Ortega, F.B.; Cantallops, J.; Ponseti, X.; Palou, P. Effects of postural education on daily habits in children. Int. J. Sports Med. 2011, 32, 303–338. [Google Scholar] [CrossRef]
- Gallardo Vidal, M.I.; Vidal, M.I.G.; Barrientos, R.R.; Olivas, A.B. Evaluación de la efectividad de una intervención educativa para disminuir el peso de la mochila escolar en los alumnos de 3.° y 4.° de educación primaria. Fisioterapia 2013, 35, 58–65. [Google Scholar] [CrossRef]
- Rodríguez-García, P.L.; López-Miñarro, P.A.; Santonja, F.M. The effect of school physical education programmes on low-back pain in schoolchildren. J. Phys. Educ. Health Soc. Perspect. 2013, 2, 43–48. [Google Scholar]
- Vidal, J.; Borràs, P.A.; Ponseti, F.J.; Cantallops, J.; Ortega, F.B.; Palou, P. Effects of a postural education program on school backpack habits related to low back pain in children. Eur. Spine J. 2013, 22, 782–787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Oosterwijck, J.; Nijs, J.; Meeus, M.; Truijen, S.; Craps, J.; Van den Keybus, N.; Paul, L. Pain neurophysiology education improves cognitions, pain thresholds, and movement performance in people with chronic whiplash: A pilot study. J. Rehabil. Res. Dev. 2011, 48, 43–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ito, T.; Shirado, O.; Suzuki, H.; Takahashi, M.; Kaneda, K.; Strax, T.E. Lumbar trunk muscle endurance testing: An inexpensive alternative to a machine for evaluation. Arch. Phys. Med. Rehabil. 1996, 77, 75–79. [Google Scholar] [CrossRef]
- Kovacs, F.M.; Abraira, V.; Royuela, A.; Corcoll, J.; Alegre, L.; Cano, A.; Muriel, A.; Zamora, J.; Gil del Real, M.T.; Gestoso, M.; et al. Minimal clinically important change for pain intensity and disability in patients with nonspecific low back pain. Spine 2007, 32, 2915–2920. [Google Scholar] [CrossRef] [PubMed]
- Díaz Arribas, M.J.; Fernández-Serrano, M.; Royuela, A.; Kovacs, F.M.; Gallego-Izquierdo, T.; Ramos-Sánchez, M.; Llorca-Palomera, R.; Pardo-Hervás, P.; San Martín-Pariente, O. Minimal Clinically Important Change in quality of life for patients with low back pain. Spine 2017, 42, 1908–1916. [Google Scholar] [CrossRef]
- Ashar, Y.K.; Gordon, A.; Schubiner, H.; Uipi, C.; Knight, K.; Anderson, Z.; Carlisle, J.; Polisky, L.; Geuter, S.; Flood, T.F.; et al. Effect of Pain Reprocessing Therapy vs Placebo and Usual Care for Patients with Chronic Back Pain: A Randomized Clinical Trial. JAMA Psychiatry 2022, 79, 13–23. [Google Scholar] [CrossRef]
- Jones, C.; Shaheed, C.A.; Ferreira, G.E.; Kharel, P.; Lin, C.W.C.; Maher, C. Advice and education provide small short-term improvements in pain and disability in people with non-specific spinal pain: A systematic review. J. Physiother. 2021, 67, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Chou, R.; Deyo, R.; Friedly, J.; Skelly, A.; Weimer, M.; Fu, R.; Dana, T.; Kraegel, P.; Griffin, J.; Grusing, S. Systemic Pharmacologic Therapies for Low Back Pain: A Systematic Review for an American College of Physicians Clinical Practice Guideline. Ann. Intern. Med. 2017, 166, 480–492. [Google Scholar] [CrossRef]
- Dahm, K.T.; Brurberg, K.G.; Jamtvedt, G.; Hagen, K.B. Advice to rest in bed versus advice to stay active for acute low-back pain and sciatica. Cochrane Database Syst. Rev. 2010, 16, CD007612. [Google Scholar] [CrossRef] [PubMed]
- Steffens, D.; Maher, C.G.; Pereira, L.S.M.; Stevens, A.L.; Oliveira, V.C.; Chapple, M.; Teixeira-Salmela, L.F.; Hancock, M.J. Prevention of Low Back Pain: A Systematic Review and Meta-analysis. JAMA Intern. Med. 2016, 176, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Hayden, J.A.; Wilson, M.N.; Sterwart, S.; Cartwright, J.; Smith, A.O.; Riley, R.D.; van Tulder, M.; Bendix, T.; Cecchi, F.; Costa, L.; et al. Exercise treatment effect modifiers in persistent low back pain: An individual participant data meta-analysis of 3514 participants from 27 randomized controlled trials. Br. J. Sports Med. 2019, 54, 1277–1278. [Google Scholar] [CrossRef]
- Wood, L.; Hendrick, P.A. A systematic review and meta-analysis of pain neuroscience education for chronic low back pain: Short-and long-term outcomes of pain and disability. Eur. J. Pain 2019, 23, 234–249. [Google Scholar] [CrossRef]
- Huang, R.; Ning, J.; Chuter, V.H.; Taylor, J.B.; Christophe, D.; Meng, Z.; Xu, Y.; Jiang, L. Exercise alone and exercise combined with education both prevent episodes of low back pain and related absenteeism: Systematic review and network meta-analysis of randomised controlled trials (RCTs) aimed at preventing back pain. Br. J. Sports Med. 2020, 54, 766–770. [Google Scholar] [CrossRef] [PubMed]
- Calvo-Muñoz, I.; Kovacs, F.M.; Roqué, M.; Gago-Fernández, I.; Seco, J. Risk factors for low back pain in childhood and adolescence. A systematic review. Clin. J. Pain 2018, 34, 468–484. [Google Scholar] [CrossRef] [PubMed]
- Calvo-Muñoz, I.; Kovacs, F.M.; Roqué, M.; Seco-Calvo, J. The association between the weight of schoolbags and low back pain among schoolchildren. A systematic review, meta-analysis and individual patient data meta-analysis. Eur. J. Pain 2019, 24, 91–109. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Study | Study Design | Setting | Follow-Up | N° of Subjects Included in the Analysis | Age (Years) 1 | Intervention/s in the Experimental Group/s (EG) | Intervention/s in the Control Group (CG) | Statistical Analysis | Comments |
|---|---|---|---|---|---|---|---|---|---|
| Kovacs et al., 2007 [17] | Cluster randomized trial | Nursing homes | 6 months | N = 661 EG1 = 232 EG2 = 189 CG = 240 | M(R) EG1 = 80.2 (77.0–83.1) EG2 = 81.6 (79.2–85.1) CG = 80.4 (76.5–83.4) | Usual care + 20 min talk, provided to groups of ≤20 participants, followed by hand out of a booklet (content consistent with the talk) Content: EG1 = Active management EG2 = Postural hygiene | Usual care + 20 min talk, provided to groups of ≤20 participants, followed by hand out of a booklet (content consistent with the talk) Content: Cardiovascular health | Mixed linear random-effects models | The same physician provided the education programs to all groups. He was told that the same effect was expected in both EGs, he had no opinion on their comparative effectiveness (both before and after the study) and was blind to subjects’ recruitment and assessment. An independent observer was present at the talks, and reported no differences across groups |
| Albaladejo et al., 2010 [18] | Cluster randomized trial | Primary care | 6 months | N = 348 EG1 = 215 EG2 = 139 CG = 171 | M(IQR) EG1 = 51.0 (42.0; 58.0) EG2 = 51.0 (42.0; 59.7) CG = 52.5 (45.0; 61.7) | Usual care + EG1 and EG2: one 15 min talk on active management for low back pain, provided to groups of ≤20 participants, and handing out of a booklet with a consistent content EG2: + One additional 15 min talk, provided to groups of ≤20 participants, and handing out of a booklet on postural hygiene + Four 1 h/week sessions of physical therapy (exercise + stretching), in groups of ≤20 participants, and advice to continue at home | Usual care + one 15 min talk on the importance of weight control and healthy nutrition habits for the management of low back pain, provided to groups of ≤20 participants, and handing out of a booklet with a consistent content | Generalized estimating equations models | Subjects in the CG were told that weight control was very important for LBP |
| Kovacs et al., 2011 [47] | Cluster randomized trial | School | 98 days | N = 497 EG = 266 CG = 231 | M(R) 1 8 (7–9) | Handing out of a booklet on active management in class, adapted for 8-year-old children | No intervention | Intraclass correlation coefficient estimated by one-way ANOVA for the difference between scores (from baseline to end of follow-up) | |
| Vidal et al., 2011 [48] | Cluster randomized trial | School | 3 months | N = 137 EG = 63 CG = 74 | M(SD) 10.72 (0.672) EG = 10.83 (0.636) CG = 10.64 (0.694) | 6, one-hour sessions on postural hygiene + 4 talks on anatomy and physiology of the spine, pathophysiology of low back pain, risk factors, ergonomics, and postural hygiene + 2 “practical sessions”; postural analysis, carrying objects, balance, analysis of the content and form of carry for schoolbags, breathing and relaxation | No intervention | Repeated-measures analysis of co-variance (ANCOVA) | |
| Del Pozo-Cruz et al., 2012 [45] | Randomized controlled trial | Primary care | 9 months | N = 100 EG = 50 CG = 50 | M(SD) EG = 45.50 (7.02) CC = 46.83 (9.13) | Usual care + face-to-face explanation of the program to each participant + As many contacts with researchers as participants wished (they could contact the research team by phone 5 days/week), with at least one face-to-face patient visit once a year + a website-based, educational program, including videos in which explanations were provided using audio and subtitles. Three videos were planned to be seen daily, from Monday to Friday, for 9 months:
| Usual care | Student’s t test for independent samples | |
| Gallardo et al., 2013 [49] | Cluster randomized trial | School | 3 months | N = 357 EG = 271 CG = 86 | M(R) 8–10 (7–11) 1 | One educational session on ergonomic criteria for selecting, loading and carrying a backpack (including the criterion to restrict carried items in the backpack to the minimum required). The content and distribution of items in the backpack on that very day, were analyzed | No intervention | Student’s t test | |
| Rodríguez-García et al., 2013 [50] | Cluster randomized trial | School | 8 months | N = 84 EG = 44 CG = 40 | M(SD) 1 Children = 10.27 (0.31) Teenagers: 13.46 (0.68) | Education on physical exercise, in two 13 min sessions of exercise per week, during 32 weeks The exercises included hamstring stretching, endurance strength of abdominal and lumbar muscles, and anterior and posterior pelvic tilt | No intervention | Chi-square and Mann–Whitney U tests | |
| Vidal et al., 2013 [51] | Cluster randomized trial | School | 3 months | N = 137 EG = 63 CG = 74 | M(SD) 1 10.72 (0.672) EG = 10.83 (0.64) CG = 10.64(0.70) | 6, one-hour sessions on postural hygiene 4 talks on anatomy and physiology of the spine, pathophysiology of low back pain, risk factors, ergonomics, and postural hygiene + 2 “practical sessions”; postural analysis, carrying objects, balance, analysis of the content and way to carry schoolbags, breathing and relaxation | No intervention | One-way analysis of variance (ANOVA) or chi-square tests, to compare baseline values. Repeated-measures analysis of co-variance (ANCOVA), to to examine the effect of the intervention | |
| Bodes Pardo et al., 2018 [46] | RCT | Physical therapy practices | 3 months | N = 56 EG = 28 EG = 28 | M(SD) EG = 44.9(9.6); CG = 49.2(10.5) | Usual care + exercise (motor control exercises, stretching, and aerobic exercise):
| Usual care + exercise (motor control exercises, stretching, and aerobic exercise):
| Pearson chi-square test and Student t test. Effect sizes were calculated by Hedges’ g |
| Study | Outcome | Results (At the End of Follow-Up) | Comments |
|---|---|---|---|
| Kovacs et al., 2007 [17] (CG = cardiovascular health; EG1 = active management; EG2 = postural hygiene) (see Table 1 for details) | Disability (RMDQ) Pain (VAS) Quality of life (PCS SF-12) Quality of life (MCS SF-12) Fear avoidance beliefs about physical activity (FAB-Phys), |
Results at the cluster level. Results from mixed linear random-effects models: additional improvement over the control group [effect size (95%IC)]: EG1 = 1.0 (0.6, 3.4) EG2 = 1.1 (−0.5, 2.7) Change from baseline to the end of follow-up [mean (range)] EG1 = 3.3 (3.1–3.6) to 0.7 (0.3–1.1) EG2 = 3.5 (3.0- 4.0) to 1.2 (0.9–1.5) CG = 3.4 (3.3–3.5) to 1.4 (1.3;1.5) Change from baseline to the end of follow-up [mean (range)] EG1 = 35.8 (32.4–39.6) to 40.9 (37.7–44.3) EG2 = 31.7 (27.9–36.7) to 36.0 (34.5–38.4) CG = 34.4 (33.0–37.0) to 37.5 (36.5–39.3) Change from baseline to the end of follow-up [mean (range)] EG1 = 58.4 (57.4–59.3) to 58.9 (58.0–59.5) EG2 = 49.4 (45.0–52.9) to 57.7 (56.7–59.3) CG = 57.1 (57.0–57.2) to 58.6 (57.7–59.8) Change from baseline to the end of follow-up [mean (range)] EG1 = 16.9 (16.5–17.2) to 19.2 (18.8–19.6) EG2 = 19.4 (19.3–19.5) to 18.5 (18.4–18.7) CG = 18.9 (18.6–19.2) to 19.0 (18.8–19.1) | This study included subjects with and without low back pain when entering the study. Additional improvements of disability, over the CG, specifically in the subset of subjects who reported low back pain when entering the study, were: EG1: 3.0 (1.5, 4.5) EG2: 1.0 (−0.6, 2.7) |
| Albaladejo et al., 2010 [18] (CG = weight control, EG1 = active management, EG2 = active management + postural hygiene + exercise supervised and unsupervised at home) (see Table 1 for details) | Disability (RMDQ) Low Back Pain (VAS) Referred pain (VAS) Catastrophizing (CSQ) Physical quality of life (PCS, SF12) Mental quality of life (MCS, SF12) | Results of the generalized estimating equations (GEE), adjusted for potential confounders, reflecting the improvement in each experimental group additional to the one in the control group [effect size (95% CI)] EG1 = 1.970 (1.252, 2.687) EG2 = 2.187 (1.413, 2.961) EG1 = 1.767 (1.363, 2.171) EG2 = 2.096 (1.660, 2.533) EG1 = 1.327 (0.831, 1.823) EG2 = 1.616 (1.055, 2.177) EG1 = 1.594 (0.659, 2.529) EG2 = 1.838 (0.834, 2.842) EG1 = 2.904 (1.256, 4.553) EG2 = 2.934 (1.163, 4.705) EG1 = 3.687 (1.711, 5.664) EG2 = 5.067 (2.933, 7.201) | |
| Kovacs et al., 2011 [47] (CG = no intervention, EG = minimal intervention on active management) (see Table 1 for details) | Appropriate knowledge (scoring ≥ 80% of maximum possible correct responses in a questionnaire on back pain prevention and management) | Results of the generalized estimating equations (GEE), adjusted for potential confounders, reflecting the probability of “appropriate knowledge” in the EG over the CG [effect size (95% CI)] 1.61 (1.03–2.52) | |
| Vidal et al., 2011 [48] (CG = no intervention, EG = intensive program on postural hygiene) (see Table 1 for details) | Healthy habits score (1 point given for each of the following items: “correct use of sofa”, “stooping correctly”, “taking care to sit correctly at home”, “taking care to sit correctly at school”, “frequent posture change on chair at home” and “frequent posture change on chair at school”) Range values: 0 (most “unhealthy” habits) to 6 (healthiest). | Results from a repeated-measures analysis of co-variance (ANCOVA) Comparison of scores before and after the intervention, showed a significant improvement in the EG (p < 0.001), but not in the CG (p > 0.6) | Actual scores in each group, are not disclosed (only graphically represented, separately for each of the items scored) |
| Del Pozo-Cruz et al., 2012 [45] (CG = no intervention, EG = intense program on postural hygiene and exercise) (see Table 1 for details) | Disability RMDQ Number of episodes of LBP during the previous 9 months (i.e., prior to baseline vs. during the follow-up period) Quality of life (EQ-5D-3L, TTO score) Lumbar endurance test (Shirado–Ito test—measured in seconds) * Abdominal endurance test (Shirado–Ito test—measured in seconds) * | Change from baseline to post-intervention assessment (“intention to treat” analysis). Student’s t test for independent samples [mean ± standard deviation (95% CI)] EG: −6.76 ± 4.01 (−7.91, −5.61 p < 0.001 CG: 1.66 ± 2.59 (0.92, 2.39) p < 0.001 EG = −1.58 ± 6.73 (−1.77, −1.38) p < 0.001 CG = 0.18 ± 0.62 (0.001, 0.359) p = 0.048 EG = 0.20 ± 0.11 (0.17, 0.23) p < 0.001 CG = −0.01 ± 0.10 (−0.04, 0.01) p = 0.211 EG = 13.32 ± 26.58 (5.76, 20.87) p < 0.001 CG = −5.18 ± 20.19 (−10.91, 0.55) p = 0.076 EG = 13.98 ± 23.82 (7.20, 20.75) p < 0.001 CG = −4.66 ± 21.52 (−10.77, 1.45) p = 0.132 | Only results from the “intention to treat” analysis are shown. Results from the “per protocol” analysis were consistent “p” values refer to intra-group differences (baseline values vs. value at the end of the 9 month, follow-up period) |
| Gallardo et al., 2013 [49] (CG = no intervention, EG = one session on use of backpack) (see Table 1 for details) | Weight of the backpack (kg) (mean ± SD) Subjects carrying a backpack weighing <15% of bodyweight [n(%)] | Student’s t test At baseline: EG = 5.4 ± 1.5 CG = 5.9 ± 1.2 p = 0.011 Three months later: EG = 3.83 ± 1.47 CG = 5.89 ± 1.39 p < 0.001 At baseline: EG = 112 (41.3%) CG = 27 (31.4%) p = 0.100 Three months later: EG = 224 (82.7%) CG = 24 (27.0%) p < 0.001 | Calculations based on the Number Needed to Treat (NNT) suggest that for every 100 children following the education program, 51 will reduce the weight of their backpacks to <15% of their bodyweight |
| Rodríguez-García et al., 2013 [50] (CG = no intervention, EG = intensive program on exercise) (see Table 1 for details) | Number (%) of subjects reporting LBP in the previous week Pain severity | Student’s t test EG: Baseline: 8 (9.5%), 8 months follow-up: 2 (2.4%) CG: Baseline: 10 (11.9%) 8 months follow-up: 19 (22.6%) p < 0.05 No differences found (no data disclosed) | |
| Vidal et al., 2013 [51] (CG = no intervention, EG = intensive program on postural hygiene) (see Table 1 for details) | “Healthy backpack use habits score” (1 point given for each of the following items: “try to load the minimum wight possible in the backpack”, “carry backpack on two shoulders”, “belief that backpack weight does not affect the back”, and “use of locker at school”). Range values: 0 (most “unhealthy” habits related to backpack) to 4 (healthiest). | Repeated-measures analysis of co-variance (ANCOVA): EG: the score improved at follow-up (p = 0.001) CG: no significant improvement in the score at follow-up (p = 0.2) | Actual scores in each group are not disclosed (only graphically represented, separately for each of the items scored) |
| Bodes Pardo et al., 2018 [46] (CG = intensive program on exercise, supervised and unsupervised at home. EG = same program + education on neurophysiology of pain) (see Table 1 for details) | Disability (RMDQ), differences between scores at baseline and at 3 month follow-up pain (NPRS), differences between scores at baseline and at 3 month follow-up Physical quality of life (PCS, SF12), differences between scores at baseline and at 3 month follow-up Kinesiophobia (TSK-11), differences between scores at baseline and at 3 month follow-up Pressure pain thresholds (kg/cm2, using an analog Fisher algometer), differences between scores at baseline and at 3 month follow-up: On spinal process L3 On lateral epicondyle Finger to floor distance (cm), differences from baseline to 1 month follow-up Self-perception of improvement (PGIC) | Between-group difference in the variation of the score (Pearson chi-square or Student’s t test where appropriate) (mean (95%CI) −2.7 (−3.9, −1.4), p < 0.001 −2.2 (−2.93, −1.28), p < 0.001 −10.6 (−13.1, −8.06), p < 0.001 −8.5 (−11.0, −6.0), p < 0.001 1.21 (1.00, 1.41), p < 0.001 0.0 (−0.1, 0.01), p > 0.05 −2.6 (−4.5, −0.7), p < 0.05 p < 0.05 | All differences were in favor of EG (a clinically positive change may imply a positive or negative score across variables, due to differences in the measuring instruments) Differences with regard to PGIC were reported in favor of the EG. However, actual values in each group were not provided; there were only graphically represented |
| Bias Domain | Source of Bias | Studies | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Kovacs et al. (2007) [17] | Albadalejo et al. (2010) [18] | Kovacs et al. (2011) [47] | Vidal et al. (2011) [48] | Del Pozo-Cruz et al. (2012) [45] | Gallardo Vidal et al. (2013) [49] | Rodriguez Garcia et al. (2013) [50] | Vidal et al. (2013) [51] | Bodes-Pardo et al. (2018) [46] | ||
| Selection | (1) Was the method of randomization adequate? |  | | |  | | |  | | |
| Selection | (2) Was treatment allocation concealed? | | | | | | | | | |
| Performance | (3) Was the patient blinded to the intervention? 1 | | | | | | | | | |
| Performance | (4) Was the care provider blinded to the intervention? 2 | | | | | | | | | |
| Detection | (5) Was the outcome assessor blinded to the intervention? | | | | | | | | | |
| Attrition | (6) Was the drop-out rate described and acceptable? | | | | | | | | | |
| Attrition | (7) Were all randomized participants analyzed in the group which they were allocated? | | | | | | | | | |
| Reporting | (8) Are reports of the study free of suggestion of selective outcome reporting? | | | | | | | | | |
| Selection | (9) Were the groups similar at baseline regarding the most important prognostic indicators, or were potential differences adjusted for at the analysis phase? | | | | | | | | | |
| Performance | (10) Were cointerventions avoided or similar? | | | | | | | | | |
| Performance | (11) Was the compliance acceptable in all groups? | | | | | | | | | |
| Detection | (12) Was the timing of the outcome assessment similar in all groups? | | | | | | | | | |
| Other | (13) Are other sources of potential bias unlikely? | | | | | | | | | |
| Total | 11/13 | 11/13 | 11/13 | 06/13 | 10/13 | 06/13 | 02/13 | 05/13 | 10/13 | |
No Unsure .Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kovacs, F.M.; Burgos-Alonso, N.; Martín-Nogueras, A.M.; Seco-Calvo, J. The Efficacy and Effectiveness of Education for Preventing and Treating Non-Specific Low Back Pain in the Hispanic Cultural Setting: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 825. https://doi.org/10.3390/ijerph19020825
Kovacs FM, Burgos-Alonso N, Martín-Nogueras AM, Seco-Calvo J. The Efficacy and Effectiveness of Education for Preventing and Treating Non-Specific Low Back Pain in the Hispanic Cultural Setting: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(2):825. https://doi.org/10.3390/ijerph19020825
Chicago/Turabian StyleKovacs, Francisco M., Natalia Burgos-Alonso, Ana María Martín-Nogueras, and Jesús Seco-Calvo. 2022. "The Efficacy and Effectiveness of Education for Preventing and Treating Non-Specific Low Back Pain in the Hispanic Cultural Setting: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 2: 825. https://doi.org/10.3390/ijerph19020825