
Risk Factors for Pressure Injuries in Adult Patients: A Narrative Synthesis

 , ,
, , {kind=link}
{kind=link}
Abstract
:1. Introduction
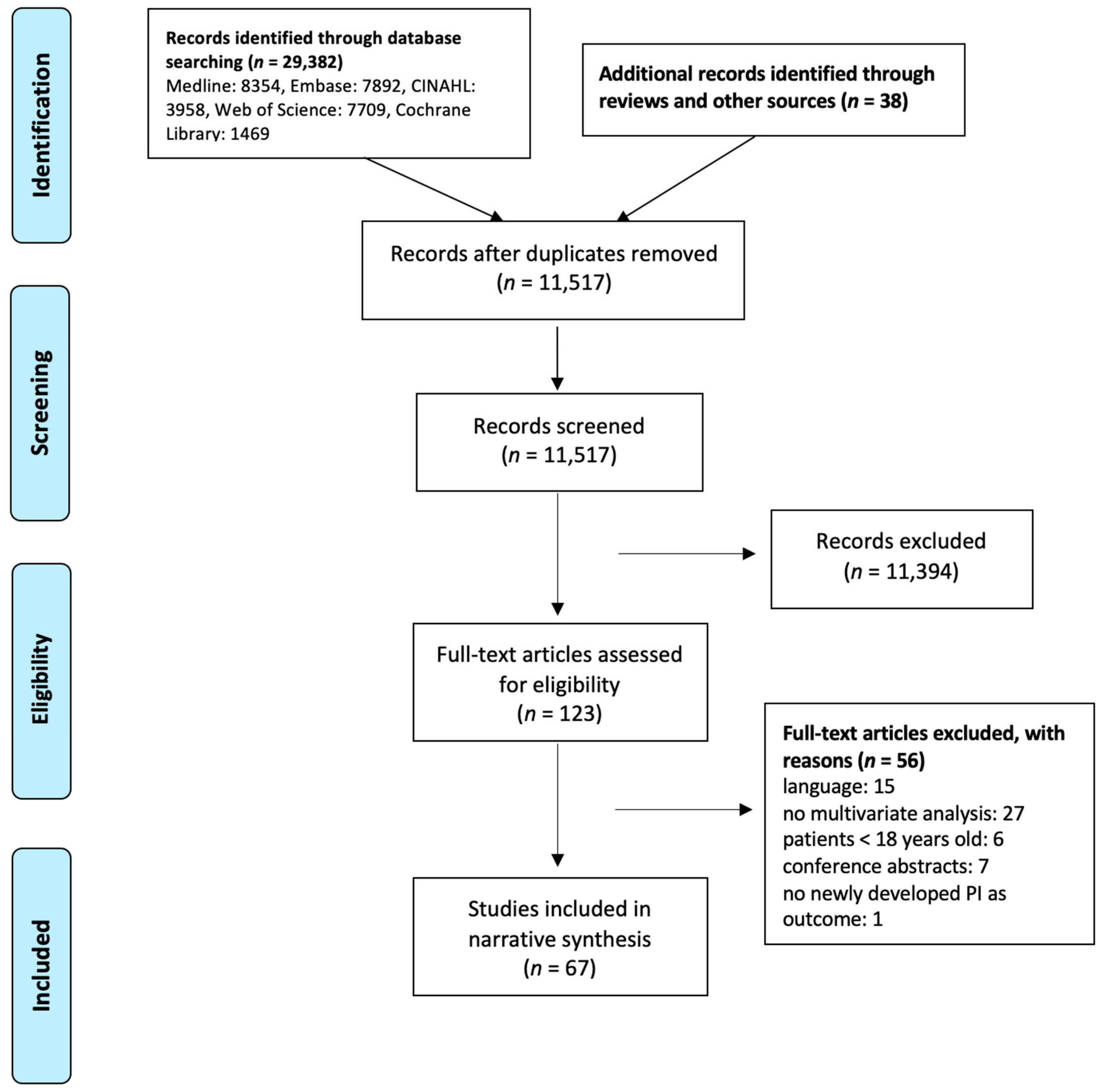
2. Materials and Methods
2.1. Data Collection
2.2. Data Extraction
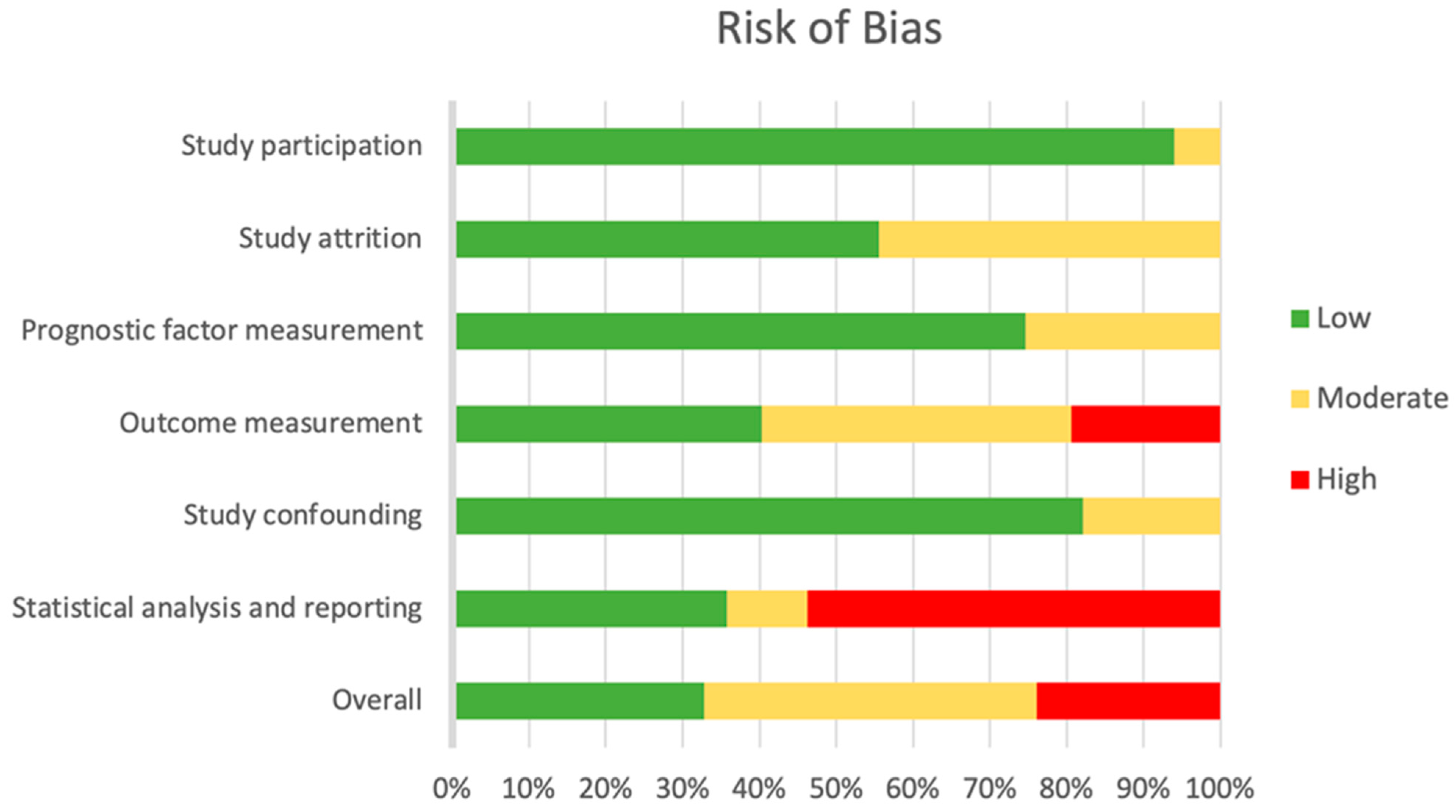
2.3. Risk of Bias
2.3.1. Study Participation
2.3.2. Study Attrition
2.3.3. Prognostic Factor Measurement
2.3.4. Outcome Measurement
2.3.5. Study Confounding
2.3.6. Statistical Analysis and Reporting
2.4. Data Synthesis
3. Results
3.1. Study Characteristics
3.2. Pressure Injury Outcome
3.3. Risk of Bias
3.4. Risk Factor Domains
3.4.1. Domain 1: Mechanical Boundary Conditions
- Body size
- 2.
- Friction/shear
- 3.
- Interface pressure
- 4.
- Subdomain Immobility
- 5.
- Sensory perception
- 6.
- Mental status/neurological disorders
- 7.
- Turning and repositioning
3.4.2. Domain 2: Susceptibility and Tolerance of the Individual
- Age
- 2.
- Sex
- 3.
- Ethnic group
- 4.
- Laboratory values
- 5.
- Nutrition
- 6.
- Body temperature
- 7.
- Health status
- 8.
- Diagnosis
- 9.
- Subdomain Skin/pressure injury status
- 10.
- Subdomain poor perfusion
3.4.3. Additional Domain: Diagnosis and Treatment
- Admission Type
- 2.
- Length of stay
- 3.
- Medication
- 4.
- Risk assessment
- 5.
- Nursing/treatment
4. Discussion
- Mechanical boundary conditions
- 2.
- Susceptibility and tolerance of the individual
- 3.
- Diagnosis and Treatment
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Li, Z.; Lin, F.; Thalib, L.; Chaboyer, W. Global prevalence and incidence of pressure injuries in hospitalised adult patients: A systematic review and meta-analysis. Int. J. Nurs. Stud. 2020, 105, 103546. [Google Scholar] [CrossRef]
- Roth, G.A.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef] [Green Version]
- Aboyans, V.; GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet Lond. Engl. 2015, 385, 117–171. [Google Scholar] [CrossRef]
- Coleman, S.; Gorecki, C.; Nelson, E.A.; Closs, S.J.; Defloor, T.; Halfens, R.; Farrin, A.; Brown, J.; Schoonhoven, L.; Nixon, J. Patient risk factors for pressure ulcer development: Systematic review. Int. J. Nurs. Stud. 2013, 50, 974–1003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alderden, J.; Rondinelli, J.; Pepper, G.; Cummins, M.; Whitney, J. Risk factors for pressure injuries among critical care patients: A systematic review. Int. J. Nurs. Stud. 2017, 71, 97–114. [Google Scholar] [CrossRef] [PubMed]
- Coleman, S.; Nixon, J.; Keen, J.; Wilson, L.; McGinnis, E.; Dealey, C.; Stubbs, N.; Farrin, A.; Dowding, D.; Schols, J.M.G.A.; et al. A new pressure ulcer conceptual framework. J. Adv. Nurs. 2014, 70, 2222–2234. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. J. Clin. Epidemiol. 2021, 134, 178–189. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (Updated February 2021). Available online: www.training.cochrane.org/handbook (accessed on 1 January 2022).
- Gail, M.H.; Altman, D.G.; Cadarette, S.M.; Collins, G.; Evans, S.J.; Sekula, P.; Williamson, E.; Woodward, M. Design choices for observational studies of the effect of exposure on disease incidence. BMJ Open 2019, 9, e031031. [Google Scholar] [CrossRef] [Green Version]
- Hayden, J.A.; van der Windt, D.A.; Cartwright, J.L.; Côté, P.; Bombardier, C. Assessing bias in studies of prognostic factors. Ann. Intern. Med. 2013, 158, 280–286. [Google Scholar] [CrossRef]
- Westby, M.J.; Dumville, J.C.; Stubbs, N.; Norman, G.; Wong, J.K.; Cullum, N.; Riley, R.D. Protease activity as a prognostic factor for wound healing in venous leg ulcers. Cochrane Database Syst. Rev. 2018, 9, CD012841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furlan, A.D.; Pennick, V.; Bombardier, C.; van Tulder, M. 2009 Updated Method Guidelines for Systematic Reviews in the Cochrane Back Review Group. Spine 2009, 34, 1929–1941. [Google Scholar] [CrossRef]
- European Pressure Ulcer Advisory Panel; National Pressure Injury Advisory Panel (U.S.); Pan Pacific Pressure Injury Alliance. Prevention and Treatment of Pressure Ulcers/Injuries: Quick Reference Guide; Haesler, E., Ed.; EPUAP/NPIAP/PPPIA: Westford, MA, USA, 2019. [Google Scholar]
- Lovaasen, K.R.; Schwerdtfeger, J. ICD-9-CM Coding: Theory and Practice with ICD-10; Elsevier Health Sciences: Amsterdam, The Netherlands, 2013; ISBN 978-0-323-27772-3. [Google Scholar]
- Harrell, F.E.; Lee, K.L.; Califf, R.M.; Pryor, D.B.; Rosati, R.A. Regression modelling strategies for improved prognostic prediction. Stat. Med. 1984, 3, 143–152. [Google Scholar] [CrossRef] [PubMed]
- Harrell, F.E.; Lee, K.L.; Mark, D.B. Multivariable Prognostic Models: Issues in Developing Models, Evaluating Assumptions and Adequacy, and Measuring and Reducing Errors. Stat. Med. 1996, 15, 361–387. [Google Scholar] [CrossRef]
- Peduzzi, P.; Concato, J.; Kemper, E.; Holford, T.R.; Feinstein, A.R. A simulation study of the number of events per variable in logistic regression analysis. J. Clin. Epidemiol. 1996, 49, 1373–1379. [Google Scholar] [CrossRef]
- Aghazadeh, A.; Lotfi, M.; Asgarpour, H.; Khajehgoodari, M.; Nobakht, A. Frequency and risk factors of pressure injuries in clinical settings of affiliated to Tabriz University of Medical Sciences. Nurs. Open 2021, 8, 808–814. [Google Scholar] [CrossRef] [PubMed]
- Allman, R.M.; Goode, P.S.; Patrick, M.M.; Burst, N.; Bartolucci, A.A. Pressure Ulcer Risk Factors Among Hospitalized Patients With Activity Limitation. JAMA 1995, 273, 865–870. [Google Scholar] [CrossRef]
- Anrys, C.; Van Tiggelen, H.; Verhaeghe, S.; Van Hecke, A.; Beeckman, D. Independent risk factors for pressure ulcer development in a high-risk nursing home population receiving evidence-based pressure ulcer prevention: Results from a study in 26 nursing homes in Belgium. Int. Wound J. 2019, 16, 325–333. [Google Scholar] [CrossRef] [PubMed]
- Artico, M.; Piredda, M.; D’Angelo, D.; Lusignani, M.; Giannarelli, D.; Marchetti, A.; De Chirico, C.; Mastroianni, C.; De Marinis, M.G. Prevalence, incidence and associated factors of pressure injuries in hospices: A multicentre prospective longitudinal study. Int. J. Nurs. Stud. 2020, 111, 103760. [Google Scholar] [CrossRef] [PubMed]
- Baumgarten, M.; Margolis, D.; Doorn, C.V.; Gruber-Baldini, A.L.; Hebel, J.R.; Zimmerman, S.; Magaziner, J. Black/White Differences in Pressure Ulcer Incidence in Nursing Home Residents. J. Am. Geriatr. Soc. 2004, 52, 1293–1298. [Google Scholar] [CrossRef]
- Bergstrom, N.; Braden, B.; Kemp, M.; Champagne, M.; Ruby, E. Multi-site Study of Incidence of Pressure Ulcers and the Relationship Between Risk Level, Demographic Characteristics, Diagnoses, and Prescription of Preventive Interventions. J. Am. Geriatr. Soc. 1996, 44, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Bergstrom, N.; Braden, B. A prospective study of pressure sore risk among institutionalized elderly. J. Am. Geriatr. Soc. 1992, 40, 747–758. [Google Scholar] [CrossRef] [PubMed]
- Boyle, M.; Green, M. Pressure sores in intensive care: Defining their incidence and associated factors and assessing the utility of two pressure sore risk assessment tools. Aust. Crit. Care 2001, 14, 24–30. [Google Scholar] [CrossRef]
- Brandeis, G.H.; Ooi, W.L.; Hossain, M.; Morris, J.N.; Lipsitz, L.A. A Longitudinal Study of Risk Factors Associated with the Formation of Pressure Ulcers in Nursing Homes. J. Am. Geriatr. Soc. 1994, 42, 388–393. [Google Scholar] [CrossRef] [PubMed]
- Chan, E.-Y.; Tan, S.-L.; Lee, C.K.-S.; Lee, J.-Y. Prevalence, incidence and predictors of pressure ulcers in a tertiary hospital in Singapore. J. Wound Care 2005, 14, 383–388. [Google Scholar] [CrossRef]
- de Laat, E.H.; Pickkers, P.; Schoonhoven, L.; Verbeek, A.L.; Feuth, T.; van Achterberg, T. Guideline implementation results in a decrease of pressure ulcer incidence in critically ill patients*. Crit. Care Med. 2007, 35, 815–820. [Google Scholar] [CrossRef] [PubMed]
- Ek, C.-A. Prediction of Pressure Sore Development. Scand. J. Caring Sci. 1987, 1, 77–84. [Google Scholar] [CrossRef]
- Gao, L.; Yang, L.; Li, X.; Chen, J.; Du, J.; Bai, X.; Yang, X. The use of a logistic regression model to develop a risk assessment of intraoperatively acquired pressure ulcer. J. Clin. Nurs. 2018, 27, 2984–2992. [Google Scholar] [CrossRef]
- González-Méndez, M.I.; Lima-Serrano, M.; Martín-Castaño, C.; Alonso-Araujo, I.; Lima-Rodríguez, J.S. Incidence and risk factors associated with the development of pressure ulcers in an intensive care unit. J. Clin. Nurs. 2018, 27, 1028–1037. [Google Scholar] [CrossRef]
- Goodridge, D.M.; Sloan, J.A.; LeDoyen, Y.M.; McKenzie, J.-A.; Knight, W.E.; Gayari, M. Risk-Assessment Scores, Prevention Strategies, and the Incidence of Pressure Ulcers among the Elderly in Four Canadian Health-Care Facilities. Can. J. Nurs. Res. Arch. 1998, 30, 23–44. [Google Scholar]
- Halfens, R.J.G.; Van Achterberg, T.; Bal, R.M. Validity and reliability of the Braden scale and the influence of other risk factors: A multi-centre prospective study. Int. J. Nurs. Stud. 2000, 37, 313–319. [Google Scholar] [CrossRef]
- Lannering, C.; Ernsth Bravell, M.; Midlöv, P.; Östgren, C.-J.; Mölstad, S. Factors related to falls, weight-loss and pressure ulcers—More insight in risk assessment among nursing home residents. J. Clin. Nurs. 2016, 25, 940–950. [Google Scholar] [CrossRef]
- Latimer, S.; Chaboyer, W.; Thalib, L.; McInnes, E.; Bucknall, T.; Gillespie, B.M. Pressure injury prevalence and predictors among older adults in the first 36 hours of hospitalisation. J. Clin. Nurs. 2019, 28, 4119–4127. [Google Scholar] [CrossRef] [PubMed]
- Magny, E.; Vallet, H.; Cohen-Bittan, J.; Raux, M.; Meziere, A.; Verny, M.; Riou, B.; Khiami, F.; Boddaert, J. Pressure ulcers are associated with 6-month mortality in elderly patients with hip fracture managed in orthogeriatric care pathway. Arch. Osteoporos. 2017, 12, 77. [Google Scholar] [CrossRef] [PubMed]
- Manzano, F.; Pérez, A.-M.; Colmenero, M.; Aguilar, M.-M.; Sánchez-Cantalejo, E.; Reche, A.-M.; Talavera, J.; López, F.; Frías-Del Barco, S.; Fernández-Mondejar, E. Comparison of alternating pressure mattresses and overlays for prevention of pressure ulcers in ventilated intensive care patients: A quasi-experimental study. J. Adv. Nurs. 2013, 69, 2099–2106. [Google Scholar] [CrossRef] [PubMed]
- Okuwa, M.; Sanada, H.; Sugama, J.; Inagaki, M.; Konya, C.; Kitagawa, A.; Tabata, K. A Prospective Cohort Study of Lower-Extremity Pressure Ulcer Risk Among Bedfast Older Adults. Adv. Skin Wound Care 2006, 19, 391–397. [Google Scholar] [CrossRef] [Green Version]
- Osis, S.L.; Diccini, S. Incidence and risk factors associated with pressure injury in patients with traumatic brain injury. Int. J. Nurs. Pract. 2020, 26, e12821. [Google Scholar] [CrossRef]
- Perneger, T.V.; Raë, A.-C.; Gaspoz, J.-M.; Borst, F.; Vitek, O.; Héliot, C. Screening for pressure ulcer risk in an acute care hospital: Development of a brief bedside scale. J. Clin. Epidemiol. 2002, 55, 498–504. [Google Scholar] [CrossRef]
- Popow, A.; Szewczyk, M.T.; Cierzniakowska, K.; Kozłowska, E.; Mościcka, P.; Cwajda-Białasik, J. Risk factors for bedsore development among hospitalised patients. Pielęgniarstwo Chir. Angiol. Vasc. Nurs. 2019, 2018, 152–158. [Google Scholar]
- Schoonhoven, L.; Defloor, T.; van der Tweel, I.; Buskens, E.; Grypdonck, M.H.F. Risk indicators for pressure ulcers during surgery. Appl. Nurs. Res. 2002, 15, 163–173. [Google Scholar] [CrossRef]
- Serpa, L.F.; Oliveira, A.S.; Nogueira, P.C.; de Gouveia Santos, V.L. Risk for undernutrition and development of pressure injury in hospitalised patients in Brazil: Multicentre prospective cohort study. Int. Wound J. 2020, 17, 916–924. [Google Scholar] [CrossRef]
- Shaw, L.F.; Chang, P.-C.; Lee, J.-F.; Kung, H.-Y.; Tung, T.-H. Incidence and predicted risk factors of pressure ulcers in surgical patients: Experience at a medical center in Taipei, Taiwan. BioMed Res. Int. 2014, 2014, 416896. [Google Scholar] [CrossRef] [PubMed]
- Suriadi; Sanada, H.; Sugama, J.; Thigpen, B.; Subuh, M. Development of a new risk assessment scale for predicting pressure ulcers in an intensive care unit. Nurs. Crit. Care 2008, 13, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Tourtual, D.M.; Riesenberg, L.A.; Korutz, C.J.; Semo, A.H.; Asef, A.; Talati, K.; Gill, R.D. Predictors of hospital acquired heel pressure ulcers. Ostomy. Wound Manag. 1997, 43, 24–28, 30, 32–34 passim. [Google Scholar]
- Tsaousi, G.; Stavrou, G.; Ioannidis, A.; Salonikidis, S.; Kotzampassi, K. Pressure ulcers and malnutrition: Results from a snapshot sampling in a university hospital. Med. Princ. Pract. Int. J. Kuwait Univ. Health Sci. Cent. 2015, 24, 11–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsaras, K.; Chatzi, M.; Kleisiaris, C.F.; Fradelos, E.C.; Kourkouta, L.; Papathanasiou, I.V. Pressure Ulcers: Developing Clinical Indicators in Evidence-based Practice. A Prospective Study. Med. Arch. 2016, 70, 379–383. [Google Scholar] [CrossRef] [Green Version]
- Yatabe, M.S.; Taguchi, F.; Ishida, I.; Sato, A.; Kameda, T.; Ueno, S.; Takano, K.; Watanabe, T.; Sanada, H.; Yatabe, J. Mini nutritional assessment as a useful method of predicting the development of pressure ulcers in elderly inpatients. J. Am. Geriatr. Soc. 2013, 61, 1698–1704. [Google Scholar] [CrossRef] [Green Version]
- Aloweni, F.; Ang, S.Y.; Fook-Chong, S.; Agus, N.; Yong, P.; Goh, M.M.; Tucker-Kellogg, L.; Soh, R.C. A prediction tool for hospital-acquired pressure ulcers among surgical patients: Surgical pressure ulcer risk score. Int. Wound J. 2019, 16, 164–175. [Google Scholar] [CrossRef] [Green Version]
- Bergquist, S.; Frantz, R. Pressure ulcers in community-based older adults receiving home health care. Prevalence, incidence, and associated risk factors. Adv. Wound Care J. Prev. Heal. 1999, 12, 339–351. [Google Scholar]
- Chen, J.-H.; Wu, S.-C.; Chen, H.-J.; Kao, C.-H.; Tseng, C.-H.; Tsai, C.-H. Risk of developing pressure sore in amyotrophic lateral sclerosis patients—A nationwide cohort study. J. Eur. Acad. Dermatol. Venereol. JEADV 2018, 32, 1589–1596. [Google Scholar] [CrossRef]
- Compton, F.; Hoffmann, F.; Hortig, T.; Strauß, M.; Frey, J.; Zidek, W.; Schäfer, J.-H. Pressure ulcer predictors in ICU patients: Nursing skin assessment versus objective parameters. J. Wound Care 2008, 17, 417–424. [Google Scholar] [CrossRef]
- Cox, J. Predictors of pressure ulcers in adult critical care patients. Am. J. Crit. Care Off. Publ. Am. Assoc. Crit.-Care Nurses 2011, 20, 364–375. [Google Scholar] [CrossRef] [Green Version]
- Cox, J.; Schallom, M.; Jung, C. Identifying Risk Factors for Pressure Injury in Adult Critical Care Patients. Am. J. Crit. Care 2020, 29, 204–213. [Google Scholar] [CrossRef]
- Dukes, S.F.; Maupin, G.M.; Thomas, M.E.; Mortimer, D.L. Pressure Injury Development in Patients Treated by Critical Care Air Transport Teams: A Case-Control Study. Crit. Care Nurse 2018, 38, 30–36. [Google Scholar] [CrossRef]
- Galivanche, A.R.; Kebaish, K.J.; Adrados, M.; Ottesen, T.D.; Varthi, A.G.; Rubin, L.E.; Grauer, J.N. Postoperative Pressure Ulcers After Geriatric Hip Fracture Surgery Are Predicted by Defined Preoperative Comorbidities and Postoperative Complications. J. Am. Acad. Orthop. Surg. 2020, 28, 342–351. [Google Scholar] [CrossRef]
- Han, S.-H.; Kim, Y.-S.; Hwang, J.; Lee, J.; Song, M.R. Predictors of hospital-acquired pressure ulcers among older adult inpatients. J. Clin. Nurs. 2018, 27, 3780–3786. [Google Scholar] [CrossRef]
- Kim, J.; Lee, J.-Y.; Lee, E. Risk factors for newly acquired pressure ulcer and the impact of nurse staffing on pressure ulcer incidence. J. Nurs. Manag. 2019, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Milićević, S.; Bukumirić, Z.; Karadžov-Nikolić, A.; Babović, R.; Sekulić, A.; Stevanović, S.; Janković, S. Predictors of pressure ulcers in patients with spinal cord injuries. Serb. J. Exp. Clin. Res. 2012, 13, 43–47. [Google Scholar] [CrossRef] [Green Version]
- Miller, M.W.; Emeny, R.T.; Snide, J.A.; Freed, G.L. Patient-specific factors associated with pressure injuries revealed by electronic health record analyses. Health Inform. J. 2020, 26, 474–485. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, D.D.; Shanks, A.M.; Talsma, A.; Brenner, P.S.; Ramachandran, S.K. Intraoperative risk factors associated with postoperative pressure ulcers in critically ill patients: A retrospective observational study. Crit. Care Med. 2014, 42, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Ooi, W.L.; Morris, J.N.; Brandeis, G.H.; Hossain, M.; Lipsitz, L.A. Nursing home characteristics and the development of pressure sores and disruptive behaviour. Age Ageing 1999, 28, 45–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.K.; Park, H.-A. Factors Affecting the Time to Occurrence of Hospital-Acquired Pressure Ulcers Using EHR Data. Stud. Health Technol. Inform. 2017, 245, 1113–1117. [Google Scholar]
- Rademakers, L.M.F.; Vainas, T.; van Zutphen, S.W.A.M.; Brink, P.R.G.; van Helden, S.H. Pressure Ulcers and Prolonged Hospital Stay in Hip Fracture Patients Affected by Time-to-Surgery. Eur. J. Trauma Emerg. Surg. Off. Publ. Eur. Trauma Soc. 2007, 33, 238–244. [Google Scholar] [CrossRef] [Green Version]
- Reed, R.L.; Hepburn, K.; Adelson, R.; Center, B.; McKnight, P. Low serum albumin levels, confusion, and fecal incontinence: Are these risk factors for pressure ulcers in mobility-impaired hospitalized adults? Gerontology 2003, 49, 255–259. [Google Scholar] [CrossRef]
- Rondinelli, J.; Zuniga, S.; Kipnis, P.; Kawar, L.N.; Liu, V.; Escobar, G.J. Hospital-Acquired Pressure Injury: Risk-Adjusted Comparisons in an Integrated Healthcare Delivery System. Nurs. Res. 2018, 67, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Sala, J.J.; Mayampurath, A.; Solmos, S.; Vonderheid, S.C.; Banas, M.; D’Souza, A.; LaFond, C. Predictors of pressure injury development in critically ill adults: A retrospective cohort study. Intensive Crit. Care Nurs. 2020, 62, 102924. [Google Scholar] [CrossRef] [PubMed]
- Salzberg, C.A.; Byrne, D.W.; Kabir, R.; Van Niewerburgh, P.; Cayten, C.G. Predicting Pressure Ulcers during Initial Hospitalization for Acute Spinal Cord Injury. Wounds 1999, 11, 45–57. [Google Scholar]
- Sardo, P.M.G.; Guedes, J.A.D.; Alvarelhão, J.J.M.; Machado, P.A.P.; Melo, E.M.O.P. Pressure ulcer incidence and Braden subscales: Retrospective cohort analysis in general wards of a Portuguese hospital. J. Tissue Viability 2018, 27, 95–100. [Google Scholar] [CrossRef]
- Sternal, D.; Wilczyński, K.; Szewieczek, J. Pressure ulcers in palliative ward patients: Hyponatremia and low blood pressure as indicators of risk. Clin. Interv. Aging 2016, 12, 37–44. [Google Scholar] [CrossRef] [Green Version]
- Strazzieri-Pulido, K.C.; González, C.V.S.; Nogueira, P.C.; Padilha, K.G.; Santos, V.L.C.G. Pressure injuries in critical patients: Incidence, patient-associated factors, and nursing workload. J. Nurs. Manag. 2019, 27, 301–310. [Google Scholar] [CrossRef] [PubMed]
- Tescher, A.N.; Branda, M.E.; Byrne, T.J.O.; Naessens, J.M. All at-risk patients are not created equal: Analysis of Braden pressure ulcer risk scores to identify specific risks. J. Wound Ostomy Cont. Nurs. Off. Publ. Wound Ostomy Cont. Nurses Soc. 2012, 39, 282–291. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, M.; Iizaka, S.; Kohno, M.; Nagata, O.; Yamasaki, T.; Mae, T.; Haruyama, N.; Sanada, H. Risk factors associated with intraoperatively acquired pressure ulcers in the park-bench position: A retrospective study. Int. Wound J. 2016, 13, 1206–1213. [Google Scholar] [CrossRef] [PubMed]
- Zarei, E.; Madarshahian, E.; Nikkhah, A.; Khodakarim, S. Incidence of pressure ulcers in intensive care units and direct costs of treatment: Evidence from Iran. J. Tissue Viability 2019, 28, 70–74. [Google Scholar] [CrossRef]
- Bourdel-Marchasson, I.; Barateau, M.; Rondeau, V.; Dequae-Merchadou, L.; Salles-Montaudon, N.; Emeriau, J.-P.; Manciet, G.; Dartigues, J.-F. A multi-center trial of the effects of oral nutritional supplementation in critically ill older inpatients. Nutrition 2000, 16, 1–5. [Google Scholar] [CrossRef]
- Defloor, T.; Grypdonck, M.F. Pressure ulcers: Validation of two risk assessment scales. J. Clin. Nurs. 2005, 14, 373–382. [Google Scholar] [CrossRef]
- Donnelly, J.; Winder, J.; Kernohan, W.G.; Stevenson, M. An RCT to determine the effect of a heel elevation device in pressure ulcer prevention post-hip fracture. J. Wound Care 2011, 20, 309–312, 314–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ek, A.-C.; Unosson, M.; Larsson, J.; Von Schenck, H.; Bjurulf, P. The development and healing of pressure sores related to the nutritional state. Clin. Nutr. 1991, 10, 245–250. [Google Scholar] [CrossRef]
- Forni, C.; D’Alessandro, F.; Gallerani, P.; Genco, R.; Bolzon, A.; Bombino, C.; Mini, S.; Rocchegiani, L.; Notarnicola, T.; Vitulli, A.; et al. Effectiveness of using a new polyurethane foam multi-layer dressing in the sacral area to prevent the onset of pressure ulcer in the elderly with hip fractures: A pragmatic randomised controlled trial. Int. Wound J. 2018, 15, 383–390. [Google Scholar] [CrossRef] [Green Version]
- Manzano, F.; Colmenero, M.; Pérez-Pérez, A.M.; Roldán, D.; del Mar Jiménez-Quintana, M.; Mañas, M.R.; Sánchez-Moya, M.A.; Guerrero, C.; Moral-Marfil, M.Á.; Sánchez-Cantalejo, E.; et al. Comparison of two repositioning schedules for the prevention of pressure ulcers in patients on mechanical ventilation with alternating pressure air mattresses. Intensive Care Med. 2014, 40, 1679–1687. [Google Scholar] [CrossRef] [PubMed]
- Nixon, J.; Cranny, G.; Iglesias, C.; Nelson, E.A.; Hawkins, K.; Phillips, A.; Torgerson, D.; Mason, S.; Cullum, N. Randomised, controlled trial of alternating pressure mattresses compared with alternating pressure overlays for the prevention of pressure ulcers: PRESSURE (pressure relieving support surfaces) trial. BMJ 2006, 332, 1413. [Google Scholar] [CrossRef] [Green Version]
- Schultz, A.A.; Bien, M.; Dumond, K.; Brown, K.; Myers, A. Etiology and Incidence of Pressure Ulcers in Surgical Patients. AORN J. 1999, 70, 434–449. [Google Scholar] [CrossRef]
- Vanderwee, K.; Grypdonck, M.; Bacquer, D.D.; Defloor, T. The identification of older nursing home residents vulnerable for deterioration of grade 1 pressure ulcers. J. Clin. Nurs. 2009, 18, 3050–3058. [Google Scholar] [CrossRef]
- Royston, P.; Altman, D.G.; Sauerbrei, W. Dichotomizing continuous predictors in multiple regression: A bad idea. Stat. Med. 2006, 25, 127–141. [Google Scholar] [CrossRef]
- Bergstrom, N.; Braden, B.J.; Laguzza, A.; Holman, V. The Braden Scale for Predicting Pressure Sore Risk. Nurs. Res. 1987, 36, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Wake, W. Pressure Ulcers: What Clinicians Need to Know. Perm. J. 2010, 14, 56–60. [Google Scholar] [CrossRef] [Green Version]
- Fletcher, J. Pressure ulcer education 3: Skin assessment and care. Nurs. Times Online 2019, 115, 26–29. [Google Scholar]
- Kim, G.; Park, M.; Kim, K. The Effect of Pressure Injury Training for Nurses: A Systematic Review and Meta-analysis. Adv. Skin Wound Care 2020, 33, 1–11. [Google Scholar] [CrossRef]
- Takahashi, M.; Black, J.; Dealey, C.; Gefen, A. Pressure in context. In International review. Pressure Ulcer Prevention: Pressure, Shear, Friction and Microclimate in Context. A Consensus Document; Wounds International: London, UK, 2010. [Google Scholar]
- De Benoist, B.; World Health Organization; Centers for Disease Control and Prevention (U.S.). Worldwide Prevalence of Anaemia 1993–2005 of: WHO Global Database of Anaemia; World Health Organization: Geneva, Switzerland, 2008; ISBN 978-92-4-159665-7. [Google Scholar]
- Keast, D.H.; Fraser, C. Treatment of chronic skin ulcers in individuals with anemia of chronic disease using recombinant human erythropoietin (EPO): A review of four cases. Ostomy. Wound Manag. 2004, 50, 64–70. [Google Scholar]
- Böhmer, A.; Defosse, J.; Geldner, G.; Rossaint, R.; Zacharowski, K.; Zwißler, B.; Wappler, F. Die aktualisierte Version der ASA-Klassifikation. Anästh Intensivmed 2021, 62, 223–228. [Google Scholar] [CrossRef]
- Beckman, J.A.; Creager, M.A. Vascular Complications of Diabetes. Circ. Res. 2016, 118, 1771–1785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huxley, R.; Ansary-Moghaddam, A.; Berrington de González, A.; Barzi, F.; Woodward, M. Type-II diabetes and pancreatic cancer: A meta-analysis of 36 studies. Br. J. Cancer 2005, 92, 2076–2083. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ling, S.; Brown, K.; Miksza, J.K.; Howells, L.; Morrison, A.; Issa, E.; Yates, T.; Khunti, K.; Davies, M.J.; Zaccardi, F. Association of Type 2 Diabetes With Cancer: A Meta-analysis With Bias Analysis for Unmeasured Confounding in 151 Cohorts Comprising 32 Million People. Diabetes Care 2020, 43, 2313–2322. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.J.; Béland, M.; Clyde, M.; Gariépy, G.; Pagé, V.; Badawi, G.; Rabasa-Lhoret, R.; Schmitz, N. Association of diabetes with anxiety: A systematic review and meta-analysis. J. Psychosom. Res. 2013, 74, 89–99. [Google Scholar] [CrossRef] [PubMed]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetc, R.; Currie, M.; Lisy, K.; Qureshi, R.; Mattis, P.; et al. Chapter 7: Systematic Reviews of Etiology and Risk. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020; Available online: https://synthesismanual.jbi.global (accessed on 1 January 2022).


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chung, M.-L.; Widdel, M.; Kirchhoff, J.; Sellin, J.; Jelali, M.; Geiser, F.; Mücke, M.; Conrad, R. Risk Factors for Pressure Injuries in Adult Patients: A Narrative Synthesis. Int. J. Environ. Res. Public Health 2022, 19, 761. https://doi.org/10.3390/ijerph19020761
Chung M-L, Widdel M, Kirchhoff J, Sellin J, Jelali M, Geiser F, Mücke M, Conrad R. Risk Factors for Pressure Injuries in Adult Patients: A Narrative Synthesis. International Journal of Environmental Research and Public Health. 2022; 19(2):761. https://doi.org/10.3390/ijerph19020761
Chicago/Turabian StyleChung, Man-Long, Manuel Widdel, Julian Kirchhoff, Julia Sellin, Mohieddine Jelali, Franziska Geiser, Martin Mücke, and Rupert Conrad. 2022. "Risk Factors for Pressure Injuries in Adult Patients: A Narrative Synthesis" International Journal of Environmental Research and Public Health 19, no. 2: 761. https://doi.org/10.3390/ijerph19020761