
Access to COVID-19 Vaccination during the Pandemic in the Informal Settlements of Rome

 , and
, and {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. Vulnerable People during the Pandemic
1.2. Ethical Distribution of Vaccines
1.3. Population of Informal Settlements
1.4. Distrust and Collaboration
1.5. The Importance of Communication
1.6. Objectives
2. Methods
2.1. Data Sources
2.2. Study Area
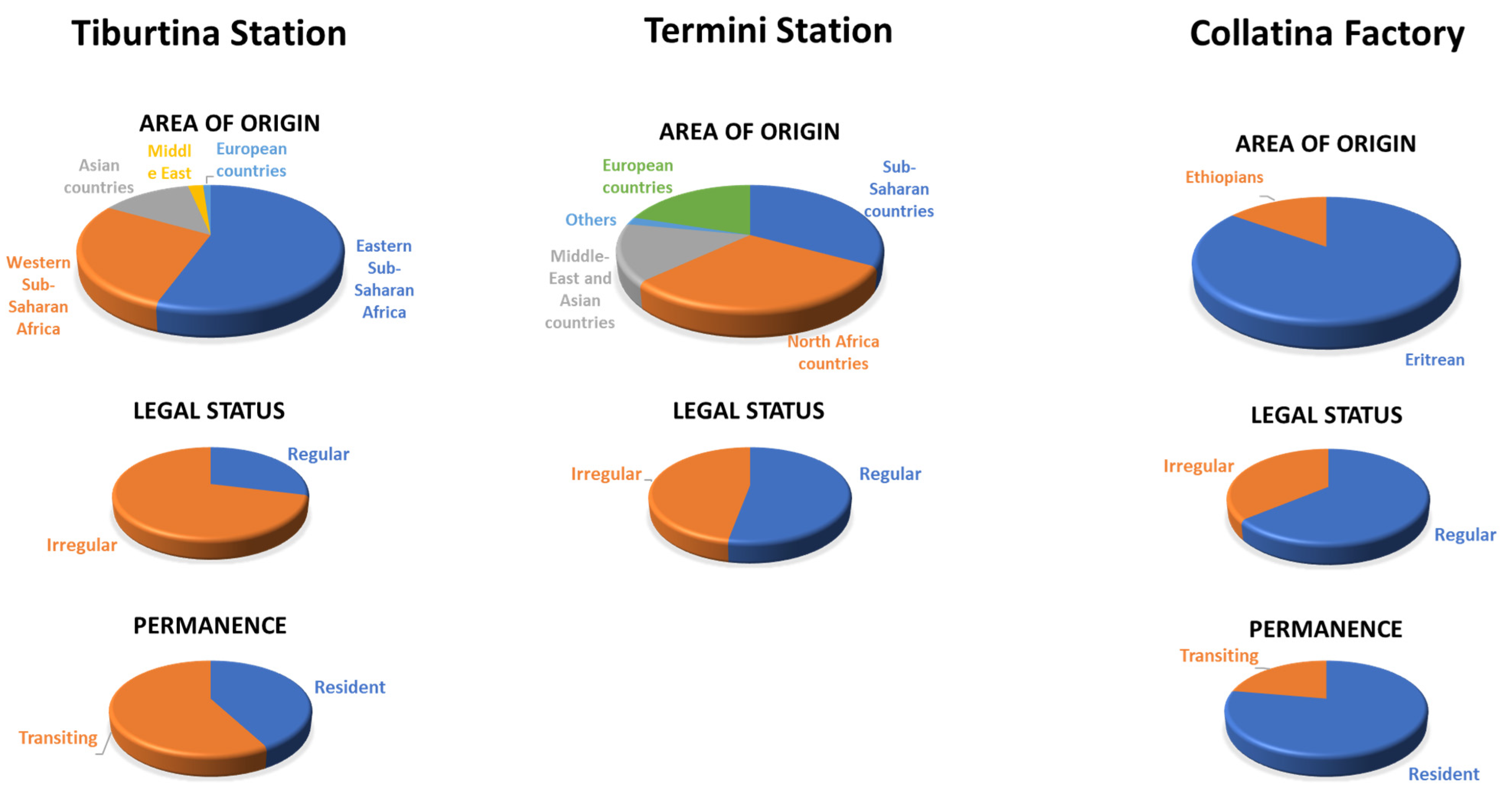
2.2.1. Tiburtina Station
2.2.2. Termini Station
2.2.3. Collatina Factory
2.3. Data Collection
2.3.1. Qualitative Data Collection
Fieldwork
Weekly Meetings
2.3.2. Quantitative Data Collection
3. Results
3.1. Our Experience
3.1.1. Practical Approaches to Reduce Barriers
3.1.2. Communication
3.1.3. Involvement of Local Committee
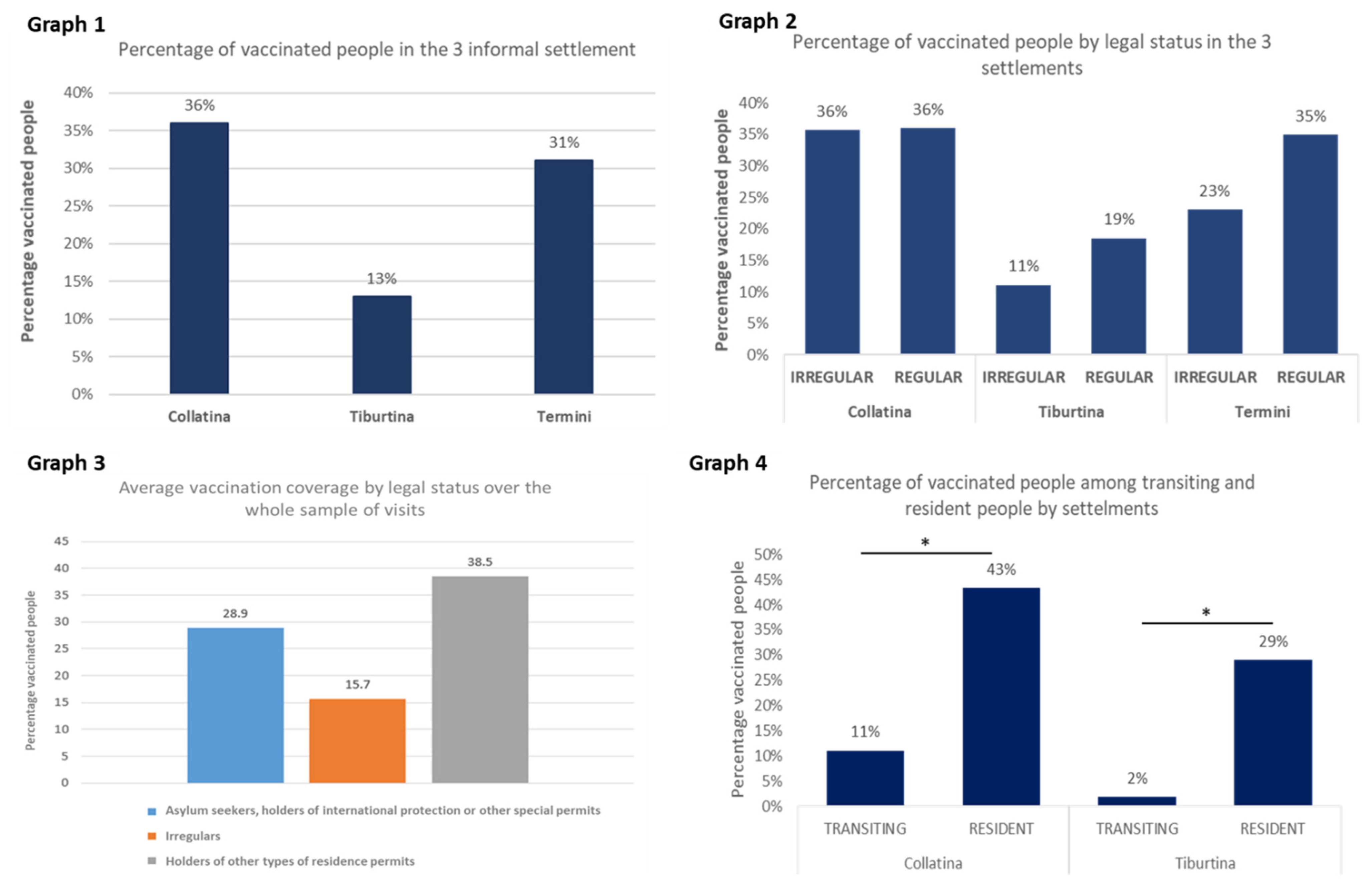
3.2. Vaccination Coverage in the Informal Settlements
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Smith-Spark, L. Global COVID-19 Deaths Pass 1 Million. Experts Fear the Toll May Double before a Vaccine Is Ready—CNN. 2020. Available online: https://edition.cnn.com/2020/09/28/health/coronavirus-million-global-deaths-intl/index.html (accessed on 11 October 2021).
- Yunus, M.; Donaldson, C.; Perron, J.L. COVID-19 Vaccines A Global Common Good. Lancet Healthy Longev. 2020, 1, e6–e8. [Google Scholar] [CrossRef]
- Barbieri, A. COVID-19 in Italy: Homeless population needs protection. Recenti Progress. Med. 2020, 111, 295–296. [Google Scholar] [CrossRef]
- World Health Organization. Beyond the Barriers: Framing Evidence on Health System Strengthening to Improve the Health of Migrants Experiencing Poverty and Social Exclusion. World Health Organization, 2017. Available online: https://apps.who.int/iris/handle/10665/259486 (accessed on 30 September 2021).
- Di Meo, S.; Bentivegna, E. Migrants’ Quarantine and COVID-19 Pandemic in Italy: A Medico-anthropological View. SN Compr. Clin. Med. 2021, 3, 1858–1862. [Google Scholar] [CrossRef] [PubMed]
- Choudhari, R. COVID 19 pandemic: Mental health challenges of internal migrant workers of India. Asian J. Psychiatry 2020, 54, 102254. [Google Scholar] [CrossRef] [PubMed]
- Mukumbang, F.C.; Ambe, A.N.; Adebiyi, B.O. Unspoken inequality: How COVID-19 has exacerbated existing vulner abilities of asylum-seekers, refugees, and undocumented migrants in South Africa. Int. J. Equity Health 2020, 19, 141. [Google Scholar] [CrossRef] [PubMed]
- Mukumbang, F.C. Are asylum seekers, refugees and foreign migrants considered in the COVID-19 vaccine discourse? BMJ Glob. Health 2020, 5, e004085. [Google Scholar] [CrossRef] [PubMed]
- International Organisation for Migration. Handbook on Protection and Assistance for Migrants Vulnerable to Violence, Exploitation and Abuse; IOM: Geneva, Switzerland, 2019. [Google Scholar]
- Emanuel, E.J.; Persad, G.; Kern, A.; Buchanan, A.; Fabre, C.; Halliday, D.; Heath, J.; Herzog, L.; Leland, R.J.; Lemango, E.T.; et al. An ethical framework for global vaccine allocation. Science. 2020, 369, 1309–1312. [Google Scholar] [CrossRef] [PubMed]
- United Nations Human Rights, Office of the High Commissioner (OHCHR). The Rights and Health of Refugees, Migrants and Stateless Must Be Protected in COVID-19 Response: A Joint Statement by UNHCR, IOM, OHCHR and WHO. 2020. Available online: https://www.ohchr.org/EN/NewsEvents/Pages/DisplayNews.aspx?NewsID=25762&LangID=E (accessed on 22 December 2020).
- World Health Organization. How WHO Is Supporting Refugees and Migrants during the COVID-19 Pandemic. 2020. Available online: https://www.who.int/news-room/feature-stories/detail/how-who-is-supporting-refugees-and-migrants-during-the-covid-19-pandemic (accessed on 11 October 2021).
- Burki, T. Statelessness in the COVID-19 pandemic. Lancet 2021, 397, 1529–1530. [Google Scholar] [CrossRef]
- Teerawattananon, Y.; Teo, Y.Y.; Lim, J.F.Y.; Hsu, L.Y.; Dabak, S. Vaccinating undocumented migrants against COVID-19. BMJ 2021, 373, n1608. [Google Scholar] [CrossRef] [PubMed]
- United Nations Network on Migration. Striving for Equitable Access to COVID-19 Vaccines to Leave no Migrant behind. 2021. Available online: https://migrationnetwork.un.org/striving-equitable-access-covid-19-vaccines-leave-no-migrant-behind (accessed on 30 September 2021).
- Gavi the Vaccine Alliance. Gavi and IOM Join Forces to Improve Immunisation Coverage for Migrants. 2020. Available online: https://www.gavi.org/news/media-room/gavi-and-iom-join-forces-improve-immunisation-coverage-migrants (accessed on 30 September 2021).
- National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Population Health and Public Health Practice; Board on Health Sciences Policy; Committee on Equitable Allocation of Vaccine for the Novel Coronavirus. Framework for Equitable Allocation of COVID-19 Vaccine; Kahn, B., Brown, L., Foege, W., Gayle, H., Eds.; National Academies Press (US): Washington, DC, USA, 2020. [Google Scholar]
- Thomas, C.M.; Osterholm, M.T.; Stauffer, W.M. Critical Considerations for COVID-19 Vaccination of Refugees, Immigrants, and Migrants. Am. J. Trop. Med. Hyg. 2021, 104, 433–435. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO SAGE Values Framework for the Allocation and Prioritization of COVID-19 Vaccination. 2020. Available online: https://apps.who.int/iris/handle/10665/334299 (accessed on 30 September 2021).
- Sattar, N.; Gill, J.M. Type 2 diabetes in migrant south Asians: Mechanisms, mitigation, and management. Lancet Diabetes Endocrinol. 2015, 3, 1004–1016. [Google Scholar] [CrossRef] [Green Version]
- Centres for Disease Prevention and Control. Health Equity Considerations and Racial and Ethnic Minority Groups. 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/community/health-equity/race-ethnicity.html (accessed on 30 September 2021).
- Reidy, E. How COVID-19 Is Being Exploited to Harden Migration Policies. the New Humanitarian. 2020. Available online: https://www.thenewhumanitarian.org/analysis/2020/04/17/coronavirus-global-migration-policies-exploited (accessed on 11 October 2021).
- Anderlini, J.; Di Meo, S. Approccio Hotspot E Navi Quarantena. Rivista il Mulino. 29 November 2021. Available online: https://www.rivistailmulino.it/a/approccio-hotspot-e-navi-quarantena (accessed on 20 December 2020).
- Legido-Quigley, H.; Pocock, N.; Tan, S.T.; Pajin, L.; Suphanchaimat, R.; Wickramage, K.; McKee, M.; Pottie, K. Healthcare is not universal if undocumented migrants are excluded. BMJ 2019, 366, l4160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raposo, V.L.; Violante, T. Access to Health Care by Migrants with Precarious Status during a Health Crisis: Some Insights from Portugal. Hum. Rights Rev. 2021, 22, 459–482. [Google Scholar] [CrossRef]
- In Dialogue with Germany, Human Rights Committee Commends Solidarity in Receiving Refugees, and Asks about COVID-19 Pandemic Response. 12 October 2021. Available online: https://www.ohchr.org/EN/NewsEvents/Pages/DisplayNews.aspx?NewsID=27649&LangID=E (accessed on 30 September 2021).
- Medici per i diritti umani (MEDU) Homepage. Available online: https://mediciperidirittiumani.org/en/about-us/ (accessed on 11 October 2021).
- Wilson, L.; Rubens-Augustson, T.; Murphy, M.; Jardine, C.; Crowcroft, N.; Hui, C.; Wilson, K. Barriers to immunization among newcomers: A systematic review. Vaccine 2018, 36, 1055–1062. [Google Scholar] [CrossRef] [PubMed]
- Merry, L.; Pelaez, S.; Edwards, N.C. Refugees, asylum-seekers and undocumented migrants and the experience of parenthood: A synthesis of the qualitative literature. Glob. Health 2017, 13, 75. [Google Scholar] [CrossRef] [Green Version]
- Report Vaccini Anti COVID-19. Available online: https://www.governo.it/it/cscovid19/report-vaccini/ (accessed on 30 September 2021).




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bentivegna, E.; Di Meo, S.; Carriero, A.; Capriotti, N.; Barbieri, A.; Martelletti, P. Access to COVID-19 Vaccination during the Pandemic in the Informal Settlements of Rome. Int. J. Environ. Res. Public Health 2022, 19, 719. https://doi.org/10.3390/ijerph19020719
Bentivegna E, Di Meo S, Carriero A, Capriotti N, Barbieri A, Martelletti P. Access to COVID-19 Vaccination during the Pandemic in the Informal Settlements of Rome. International Journal of Environmental Research and Public Health. 2022; 19(2):719. https://doi.org/10.3390/ijerph19020719
Chicago/Turabian StyleBentivegna, Enrico, Silvia Di Meo, Anita Carriero, Nadia Capriotti, Alberto Barbieri, and Paolo Martelletti. 2022. "Access to COVID-19 Vaccination during the Pandemic in the Informal Settlements of Rome" International Journal of Environmental Research and Public Health 19, no. 2: 719. https://doi.org/10.3390/ijerph19020719