
Factors Associated with the Acceptability of Mass Drug Administration for Filariasis: A Systematic Review
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
- Population: general population.
- Exposure: mass drug administration for filariasis.
- Outcome: associated factors of acceptability.
2.1. Searching Strategy
2.2. Eligibility Criteria
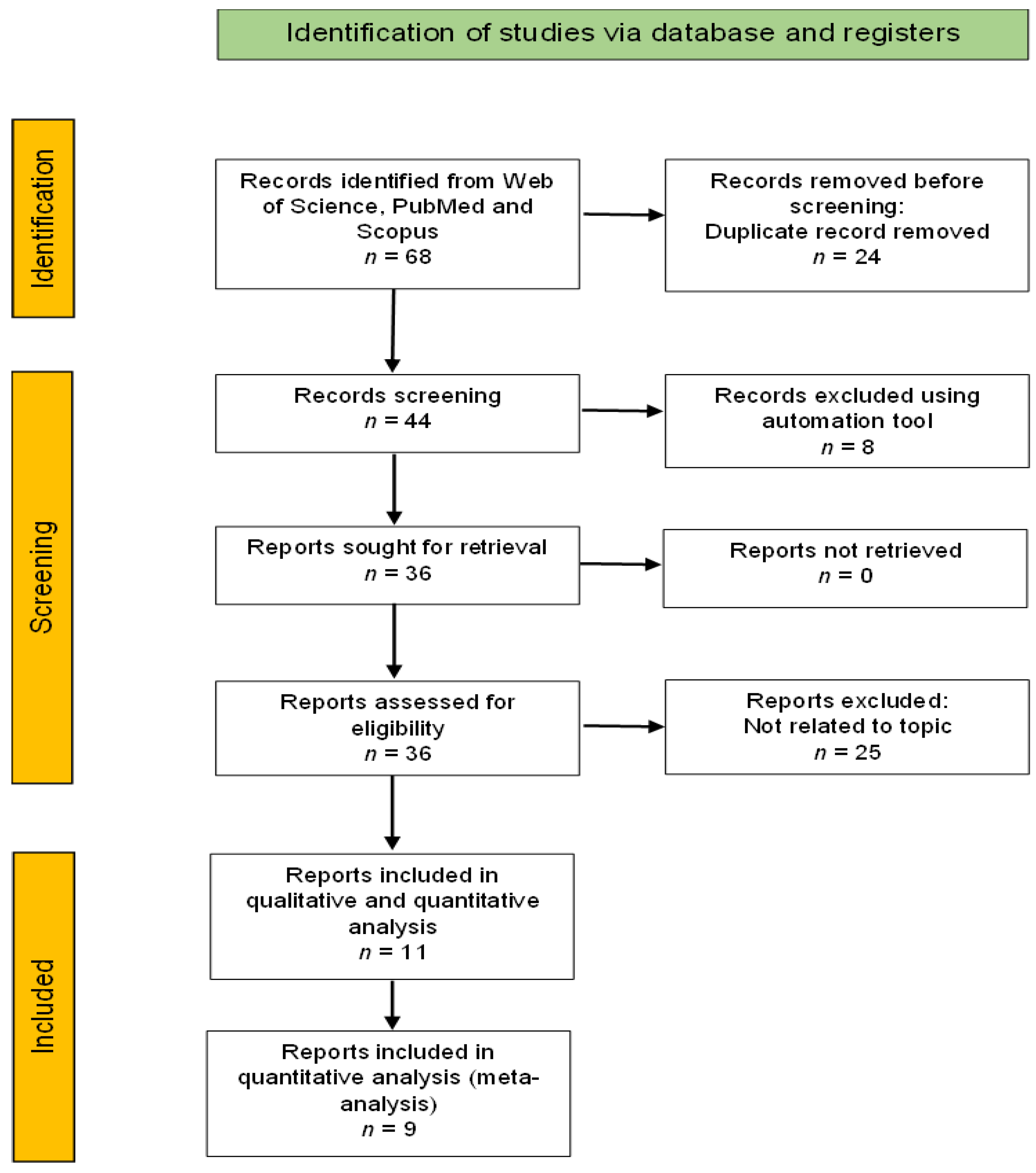
2.3. Study Selection
2.4. Critical Appraisal and Data Extraction
2.5. Data Analysis
3. Results
3.1. Acceptability of Mass Drug Therapy
3.2. Factors Associated with Acceptability of Mass Drug Administration (MDA) for Filariasis
3.2.1. Knowledge, Attitude and Perception
3.2.2. Communication, Delivery and Access of the MDA
3.2.3. Gender and Age
3.2.4. Risk of Bias
3.2.5. Meta-Analysis
4. Discussion
4.1. Knowledge, Attitude and Perception
4.2. Communication, Delivery and Access of the MDA
4.3. Age and Gender
4.4. Recommendation
4.5. Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Taylor, M.J.; Hoerauf, A.; Bockarie, M. Lymphatic Filariasis and Onchocerciasis. Lancet 2010, 376, 1175–1185. [Google Scholar] [CrossRef]
- WHO. Lymphatic Filariasis; WHO: Geneva, Switzerland, 2022. [Google Scholar]
- Ottesen, E.A. The Global Programme to Eliminate Lymphatic Filariasis. Trop. Med. Int. Health 2000, 5, 5. [Google Scholar] [CrossRef] [PubMed]
- Gyapong, J.O.; Kumaraswami, V.; Biswas, G.; Ottesen, E.A. Treatment Strategies Underpinning the Global Programme to Eliminate Lymphatic Filariasis. Expert Opin Pharmacother. 2005, 6, 179–200. [Google Scholar] [CrossRef] [PubMed]
- WHO. Guideline: Alternative Mass Drug Administration Regimens to Eliminate Lymphatic Filariasis; WHO: Geneva, Switzerland, 2017; ISBN 9789241550161. [Google Scholar]
- Michael, E.; Malecela-Lazaro, M.N.; Simonsen, P.E.; Pedersen, E.M.; Barker, G.; Kumar, A.; Kazura, J.W. Mathematical Modelling and the Control of Lymphatic Filariasis. Lancet Infect. Dis. 2004, 4, 223–234. [Google Scholar] [CrossRef]
- Stolk, W.A.; Swaminathan, S.; Van Oortmarssen, G.J.; Das, P.K.; Habbema, J.D.F. Prospects for Elimination of Bancroftian Filariasis by Mass Drug Treatment in Pondicherry India: A Simulation Study. J. Infect. Dis. 2003, 188, 1371–1381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Monitoring and Epidemiological Assessment of Mass Drug Administration in the Global Programme to Eliminate Lymphatic Filariasis: A Manual for National Elimination Programmes; WHO: Geneva, Switzerland, 2011; ISBN 978 92 4 150148 4. [Google Scholar]
- Niles, R.A.; Thickstun, C.R.; Cox, H.; Dilliott, D.; Burgert-Brucker, C.R.; Harding-Esch, E.M.; Clementson, N.; Sampson, A.; Alexandre, J.S.; Morice Trejos, A.C.; et al. Assessing Factors Influencing Communities’ Acceptability of Mass Drug Administration for the Elimination of Lymphatic Filariasis in Guyana. PLoS Negl. Trop. Dis. 2021, 15, e0009596. [Google Scholar] [CrossRef] [PubMed]
- Krentel, A.; Fischer, P.U.; Weil, G.J. A Review of Factors That Influence Individual Compliance with Mass Drug Administration for Elimination of Lymphatic Filariasis. PLoS Negl. Trop. Dis. 2013, 7, e2447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sekhon, M.; Cartwright, M.; Francis, J.J. Acceptability of Healthcare Interventions: An Overview of Reviews and Development of a Theoretical Framework. BMC Health Serv. Res. 2017, 17, 88. [Google Scholar] [CrossRef] [Green Version]
- Hill, J.; Hoyt, J.; Achieng, F.; Ouma, P.; L’lanziva, A.; Kariuki, S.; Desai, M.; Webster, J. User and Provider Acceptability of Intermittent Screening and Treatment and Intermittent Preventive Treatment with Dihydroartemisinin-Piperaquine to Prevent Malaria in Pregnancy in Western Kenya. PLoS ONE 2016, 11, e0150259. [Google Scholar] [CrossRef] [Green Version]
- Liau, A.; Zimet, G.D. The Acceptability of HIV Immunization: Examining Vaccine Characteristics as Determining Factors. AIDS Care—Psychol Socio-Med. Asp AIDS/HIV 2001, 13, 643–650. [Google Scholar] [CrossRef]
- Tingstrom, D.H. Acceptability of Time-out: The Influence of Problem Behavior Severity, Interventionist, and Reported Effectiveness. J. Sch. Psychol. 1990, 28, 165–169. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef]
- Munn, Z.; Stern, C.; Aromataris, E.; Lockwood, C.; Jordan, Z. What Kind of Systematic Review Should i Conduct? A Proposed Typology and Guidance for Systematic Reviewers in the Medical and Health Sciences. BMC Med. Res. Methodol. 2018, 18, 5. [Google Scholar] [CrossRef] [Green Version]
- Bramer, W.M.; Giustini, D.; De Jonge, G.B.; Holland, L.; Bekhuis, T. De-Duplication of Database Search Results for Systematic Reviews in EndNote. J. Med. Libr. Assoc. 2016, 104, 240–243. [Google Scholar] [CrossRef]
- Hong, Q.N.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.P.; Griffiths, F.; Nicolau, B.; O’Cathain, A.; et al. The Mixed Methods Appraisal Tool (MMAT) Version 2018 for Information Professionals and Researchers. Educ. Inf. 2018, 34, 285–291. [Google Scholar] [CrossRef] [Green Version]
- Rosanti, T.I.; Mardihusodo, S.J.; Artama, W.T. Directly Observed Treatment Increases Drug Compliance in Lymphatic Filariasis Mass Drug Administration. Universa Med. 2016, 35, 119–127. [Google Scholar] [CrossRef] [Green Version]
- Bhatia, V.; Giri, P.P.; Sahoo, S.S.; Preeti, P.S.; Sahu, D.P. Mass Drug Administration (MDA) for Elimination of Lymphatic Filariasis: Experiences from Nayagarh District of Odisha, India. Indian J. Community Health 2018, 30, 287–292. [Google Scholar] [CrossRef]
- Putri, I.W.; Mutahar, R.; Sitorus, R.J.; Novrikasari; Rosyada, A.; Andarini, D. Factors Determining Drug Uptake during Mass Drug Administration in Banyuasin District, South Sumatera, Indonesia. Int. J. Recent Technol. Eng. 2019, 8, 113–117. [Google Scholar] [CrossRef]
- Nujum, Z.; Rajmohanan, K.; Remadevi, S.; Indu, P.; Nair, S.; Nirmala, C. Factors Determining Noncompliance to Mass Drug Administration for Lymphatic Filariasis Elimination. Trop. Parasitol. 2012, 2, 109. [Google Scholar] [CrossRef] [Green Version]
- Krentel, A.; Wellings, K. The Role of Gender Relations in Uptake of Mass Drug Administration for Lymphatic Filariasis in Alor District, Indonesia. Parasites Vectors 2018, 11, 179. [Google Scholar] [CrossRef]
- Amarillo, M.L.E.; Belizario, V.Y.; Sadiang-Abay, J.T.; Sison, S.A.M.; Dayag, A.M.S. Factors Associated with the Acceptance of Mass Drug Administration for the Elimination of Lymphatic Filariasis in Agusan Del Sur, Philippines. Parasites Vectors 2008, 1, 14. [Google Scholar] [CrossRef] [Green Version]
- Mathieu, E.; Lammie, P.J.; Radday, J.; Beach, M.J.; Streit, T.; Wendt, J.; Addiss, D.G. Factors Associated with Participation in a Campaign of Mass Treatment against Lymphatic Filariasis, in Leogane, Haiti. Ann. Trop. Med. Parasitol. 2004, 98, 703–714. [Google Scholar] [CrossRef]
- Adekeye, O.; Ozano, K.; Dixon, R.; Elhassan, E.O.; Lar, L.; Schmidt, E.; Isiyaku, S.; Okoko, O.; Thomson, R.; Theobald, S.; et al. Mass Administration of Medicines in Changing Contexts: Acceptability, Adaptability and Community Directed Approaches in Kaduna and Ogun States, Nigeria. PLoS Negl. Trop. Dis. 2020, 14, e0008857. [Google Scholar] [CrossRef]
- Parker, M.; Allen, T. Will Mass Drug Administration Eliminate Lymphatic Filariasis? Evidence from Northern Coastal Tanzania. J. Biosoc. Sci. 2013, 45, 517–545. [Google Scholar] [CrossRef] [Green Version]
- Kisoka, W.J.; Simonsen, P.E.; Malecela, M.N.; Tersbøl, B.P.; Mushi, D.L.; Meyrowitsch, D.W. Factors Influencing Drug Uptake during Mass Drug Administration for Control of Lymphatic Filariasis in Rural and Urban Tanzania. PLoS ONE 2014, 9, e109316. [Google Scholar] [CrossRef] [Green Version]
- Abd Elaziz, K.M.; El-Setouhy, M.; Bradley, M.H.; Ramzy, R.M.R.; Weil, G.J. Knowledge and Practice Related to Compliance with Mass Drug Administration during the Egyptian National Filariasis Elimination Program. Am. J. Trop. Med. Hyg. 2013, 89, 260–264. [Google Scholar] [CrossRef] [Green Version]
- Ramzy, R.M.R.; Goldman, A.S.; Kamal, H.A. Defining the Cost of the Egyptian Lymphatic Filariasis Elimination Programme. Filaria J. 2005, 4, 7. [Google Scholar] [CrossRef] [Green Version]
- Saleem, F.; Hassali, M.; Shafie, A.; Atif, M. Drug Attitude and Adherence: A Qualitative Insight of Patients with Hypertension. J. Young Pharm. 2012, 4, 101–107. [Google Scholar] [CrossRef] [Green Version]
- Al-Abd, N.M.; Nor, Z.M.; Ahmed, A.; Al-Adhroey, A.H.; Mansor, M.; Kassim, M. Lymphatic Filariasis in Peninsular Malaysia: A Cross-Sectional Survey of the Knowledge, Attitudes, and Practices of Residents. Parasites Vectors 2014, 7, 545. [Google Scholar] [CrossRef]
- Zakaria, N.D.; Avoi, R. Prevalence and Risk Factors for Positive Lymphatic Filariasis Antibody in Sabah, Malaysia: A Cross-Sectional Study. Trans. R Soc. Trop. Med. Hyg. 2022, 116, 369–374. [Google Scholar] [CrossRef]
- Kim, S. Medication Adherence of Elderly with Hypertension and/OrDiabetes-Mellitus and Its’ Influencing Factors. Korean J. Clin. Pharm. 2011, 21, 81–89. [Google Scholar]
- Adhikari, R.K.; Sherchand, J.B.; Mishra, S.R.; Ranabhat, K.; Devkota, P.; Mishra, D.; Ghimire, Y.C.; Gelal, K.; Mishra, R.; Paudel, R.; et al. Factors Determining Non-Compliance to Mass Drug Administration for Lymphatic Filariasis Elimination in Endemic Districts of Nepal. J. Nepal Health Res. Counc. 2014, 12, 124–129. [Google Scholar] [CrossRef] [PubMed]
- Njomo, D.W.; Amuyunzu-Nyamongo, M.; Magambo, J.K.; Njenga, S.M. The Role of Personal Opinions and Experiences in Compliance with Mass Drug Administration for Lymphatic Filariasis Elimination in Kenya. PLoS ONE 2012, 7, e48395. [Google Scholar] [CrossRef] [PubMed]
- Hussain, M.A.; Sitha, A.K.; Swain, S.; Kadam, S.; Pati, S. Mass Drug Administration for Lymphatic Filariasis Elimination in a Coastal State of India: A Study on Barriers to Coverage and Compliance. Infect. Dis. Poverty 2014, 3, 31. [Google Scholar] [CrossRef] [Green Version]
- Clement, Y.N.; Morton-Gittens, J.; Basdeo, L.; Blades, A.; Francis, M.-J.; Gomes, N.; Janjua, M.; Singh, A. Perceived Efficacy of Herbal Remedies by Users Accessing Primary Healthcare in Trinidad. BMC Complement. Altern. Med. 2007, 7, 4. [Google Scholar] [CrossRef] [Green Version]
- Manyeh, A.K.; Chirwa, T.; Ramaswamy, R.; Baiden, F.; Ibisomi, L. Evaluating Context-Specific Evidence-Based Quality Improvement Intervention on Lymphatic Filariasis Mass Drug Administration in Northern Ghana Using the RE-AIM Framework. Trop. Med. Health 2021, 49, 16. [Google Scholar] [CrossRef]
- Wynd, S.; Carron, J.; Selve, B.; Leggat, P.A.; Melrose, W.; Durrheim, D.N. Qualitative Analysis of the Impact of a Lymphatic Filariasis Elimination Programme Using Mass Drug Administration on Misima Island, Papua New Guinea. Filaria J. 2007, 6, 1. [Google Scholar] [CrossRef] [Green Version]
- Owusu, I.O.; Frances, B.; Mensah, O.; Gyapong, M. Elimination of Lymphatic Filariasis: Current Perspectives on Mass Drug Administration. Res. Rep. Trop. Med. 2018, 9, 25–33. [Google Scholar] [CrossRef] [Green Version]
- Allen, T.; Parker, M. Will Increased Funding for Neglected Tropical Diseases Really Make Poverty History? Lancet 2012, 379, 1097–1098. [Google Scholar] [CrossRef]
- Dembélé, M.; Bamani, S.; Dembélé, R.; Traoré, M.O.; Goita, S.; Traoré, M.N.; Sidibe, A.K.; Sam, L.; Tuinsma, M.; Toubali, E.; et al. Implementing Preventive Chemotherapy through an Integrated National Neglected Tropical Disease Control Program in Mali. PLoS Negl. Trop. Dis. 2012, 6, e1574. [Google Scholar] [CrossRef] [Green Version]
- Al Shamsi, H.; Almutairi, A.G.; Al Mashrafi, S.; Al Kalbani, T. Implications of Language Barriers for Healthcare: A Systematic Review. Oman Med. J 2020, 35, e122. [Google Scholar] [CrossRef]
- Ipa, M.; Astuti, E.; Ridwan, W.; Soerachman, R. Qualitative Study: Leverage and Barrier Factors of Mass Drug Administration for Lymphatic Filariasis Elimination Program in Tangerang and Subang Regency. In Proceedings of the 5th Universitas Ahmad Dahlan Public Health Conference (UPHEC 2019), Yogyakarta, Indonesia, 3–4 July 2019; Atlantis Press: Paris, France, 2020; pp. 116–121. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.-L.; Lee, W.-L.; Liang, T.; Liao, I.-C. Factors Associated with Gender Differences in Medication Adherence: A Longitudinal Study. J. Adv. Nurs. 2014, 70, 2031–2040. [Google Scholar] [CrossRef]
- Manteuffel, M.; Williams, S.; Chen, W.; Verbrugge, R.R.; Pittman, D.G.; Steinkellner, A. Influence of Patient Sex and Gender on Medication Use, Adherence, and Prescribing Alignment with Guidelines. J. Womens Health 2014, 23, 112–119. [Google Scholar] [CrossRef]
- Zopf, Y.; Rabe, C.; Neubert, A.; Gassmann, K.G.; Rascher, W.; Hahn, E.G.; Brune, K.; Dormann, H. Women Encounter ADRs More Often than Do Men. Eur. J. Clin. Pharmacol. 2008, 64, 999–1004. [Google Scholar] [CrossRef]
- Feinberg, L.; Reinhard, S.; Houser, A.; Choula, R. Valuing the Invaluable: 2011 Update the Growing Contributions and Costs of Family Caregiving; Insight Issues; AARP Public Policy Institute: Washington, DC, USA, 2010; p. 51. [Google Scholar]
- Thunander Sundbom, L.; Bingefors, K. Women and Men Report Different Behaviours in, and Reasons for Medication Non-Adherence: A Nationwide Swedish Survey. Pharm Pract. 2012, 10, 207–221. [Google Scholar] [CrossRef] [Green Version]
- Petersen, I.; Gilbert, R.E.; Evans, S.J.W.; Man, S.-L.; Nazareth, I. Pregnancy as a Major Determinant for Discontinuation of Antidepressants: An Analysis of Data from The Health Improvement Network. J. Clin. Psychiatry 2011, 72, 979–985. [Google Scholar] [CrossRef]
- Einarson, A.; Selby, P.; Koren, G. Abrupt Discontinuation of Psychotropic Drugs during Pregnancy: Fear of Teratogenic Risk and Impact of Counselling. J. Psychiatry Neurosci. 2001, 26, 44–48. [Google Scholar] [CrossRef]
- Theobald, S.; MacPherson, E.E.; Dean, L.; Jacobson, J.; Ducker, C.; Gyapong, M.; Hawkins, K.; Elphick-Pooley, T.; Mackenzie, C.; Kelly-Hope, L.A.; et al. 20 Years of Gender Mainstreaming in Health: Lessons and Reflections for the Neglected Tropical Diseases Community. BMJ Glob. Health 2017, 2, e000512. [Google Scholar] [CrossRef] [Green Version]
- Widawati, M.; Astuti, E.P.; Ruliansyah, A.; Yuliasih, Y. Sociodemographic, Knowledge, and Attitude Determinants of Lymphatic Filariasis Medication Adherence in Subang, Indonesia. In Proceedings of the 5th Universitas Ahmad Dahlan Public Health Conference (UPHEC 2019), Yogyakarta, Indonesia, 3–4 July 2019; Atlantis Press: Paris, France, 2020; pp. 1–6. [Google Scholar] [CrossRef] [Green Version]
- Rilkoff, H.; Tukahebwa, E.M.; Fleming, F.M.; Leslie, J.; Cole, D.C. Exploring Gender Dimensions of Treatment Programmes for Neglected Tropical Diseases in Uganda. PLoS Negl. Trop. Dis. 2013, 7, e2312. [Google Scholar] [CrossRef]
- Dickson, B.F.R.; Graves, P.M.; Aye, N.N.; Nwe, T.W.; Wai, T.; Win, S.S.; Shwe, M.; Douglass, J.; Wood, P.; Wangdi, K.; et al. Risk Factors for Lymphatic Filariasis and Mass Drug Administration Non-Participation in Mandalay Region, Myanmar. Parasit Vectors 2021, 14, 72. [Google Scholar] [CrossRef]
- Kim, S.J.; Kwon, O.D.; Han, E.B.; Lee, C.M.; Oh, S.-W.; Joh, H.-K.; Oh, B.; Kwon, H.; Cho, B.; Choi, H.C. Impact of Number of Medications and Age on Adherence to Antihypertensive Medications: A Nationwide Population-Based Study. Medicine 2019, 98, e17825. [Google Scholar] [CrossRef]
- Njomo, D.W.; Kibe, L.W.; Kimani, B.W.; Okoyo, C.; Omondi, W.P.; Sultani, H.M. Addressing Barriers of Community Participation and Access to Mass Drug Administration for Lymphatic Filariasis Elimination in Coastal Kenya Using a Participatory Approach. PLoS Negl. Trop. Dis. 2020, 14, e0008499. [Google Scholar] [CrossRef]
- Taddeo, D.; Egedy, M.; Frappier, J.-Y. Adherence to Treatment in Adolescents. Paediatr. Child Health 2008, 13, 19–24. [Google Scholar] [CrossRef] [Green Version]
- Nandha, B.; Sadanandane, C.; Jambulingam, P.; Das, P. Delivery Strategy of Mass Annual Single Dose DEC Administration to Eliminate Lymphatic Filariasis in the Urban Areas of Pondicherry, South India: 5 Years of Experience. Filaria J. 2007, 6, 7. [Google Scholar] [CrossRef] [Green Version]
- Tavakoli, R. The survey of important socio- economic & cltural variables influencing self-medication. Daneshvar Med. 2001, 8, 9–12. [Google Scholar]
- Smaje, A.; Davis, D.; Ranjana, M.W.; Mine, R.; Rawle, M. Factors Associated with Medication Adherence in Older Patients: A Systematic Review. Aging Med. 2018, 1, 254–266. [Google Scholar] [CrossRef] [Green Version]
- Krentel, A.; Damayanti, R.; Titaley, C.R.; Suharno, N.; Bradley, M.; Lynam, T. Improving Coverage and Compliance in Mass Drug Administration for the Elimination of LF in Two ‘Endgame’ Districts in Indonesia Using Micronarrative Surveys. PLoS Negl. Trop. Dis. 2016, 10, e0005027. [Google Scholar] [CrossRef] [Green Version]
- Babu, B.V.; Kar, S.K. Coverage, Compliance and Some Operational Issues of Mass Drug Administration during the Programme to Eliminate Lymphatic Filariasis in Orissa, India. Trop. Med. Int. Health 2004, 9, 702–709. [Google Scholar] [CrossRef] [PubMed]
- Khaemba, C.; Barry, A.; Omondi, W.P.; Bota, K.; Matendechero, S.; Wandera, C.; Siyoi, F.; Kirui, E.; Oluka, M.; Nambwa, P.; et al. Safety and Tolerability of Mass Diethylcarbamazine and Albendazole Administration for the Elimination of Lymphatic Filariasis in Kenya: An Active Surveillance Study. Pharmaceuticals 2021, 14, 264. [Google Scholar] [CrossRef] [PubMed]
- Parker, M.; Allen, T. Does Mass Drug Administration for the Integrated Treatment of Neglected Tropical Diseases Really Work? Assessing Evidence for the Control of Schistosomiasis and Soil-Transmitted Helminths in Uganda. Health Res. Policy Syst. 2011, 9, 3. [Google Scholar] [CrossRef] [PubMed]
- WHO. Towards Universal Coverage for Preventive Chemotherapy for Neglected Tropical Diseases: Guidance for Assessing “Who Is Being Left behind and Why”; WHO/WFC/17.3; WHO: Geneva, Switzerland, 2017. [Google Scholar]



{kind=link}
{kind=link}
| Study Location | Authors |
| Guyana | Niles et al. 2021 [9] |
| Nigeria | Adekeye et al. 2020 [19] |
| Indonesia | Rosanti, Mardihusodo, & Artama 2016., Krentel & Wellings 2018, Putri et al. 2019 [20,21,22] |
| India | Bhatia et al. 2018, Nujum et al. 2012 [23,24] |
| Tanzania | Kisoka et al. 2014, Parker & Allen 2013 [25,26] |
| Philippines | Amarillo et al. 2008 [27] |
| Haiti | Mathieu et al. 2004 [28] |
| Study Design | Authors |
| Cross-sectional | Niles et al. 2021, Putri et al. 2019, Kisoka et al. 2014, Mathieu et al. 2004 [9,22,25,28] |
| Longitudinal study | Rosanti, Mardihusodo, Artama 2016 [20] |
| Case-control | Nujum et al. 2012 [24] |
| Qualitative study | Adekeye et al. 2020, Krentel et al. 2018, Parker & Allen 2013 [19,21,26] |
| Mixed method | Bhatia et al. 2018, Amarillo et al. 2008 [23,27] |
| Author (Year) | Title | Study Design | Sample Size | Types of Drug Therapy/Regime | Acceptability | Factors |
|---|---|---|---|---|---|---|
| Niles RA et al. 2021 [9] | Assessing factors influencing communities’ acceptability of mass drug administration for the elimination of lymphatic filariasis in Guyana | Cross-sectional | 390 | Triple drug therapy regimen IDA (Ivermectin, DEC, and Albendazole | Intervention Rating Profile tool. Mean acceptability scores ranged from 24.6 to 29.3, above the threshold of acceptability (a score of 22.5). |
|
| Adekeye et al. 2020 [19] | Mass administration of medicines in changing contexts: Acceptability, adaptability and community-directed approaches in Kaduna and Ogun states, Nigeria | Qualitative study | 42 | Ivermectin |
| |
| Putri et al. 2019 [22] | Factors determining drug uptake during mass drug administration in Banyuasin district, South Sumatera, Indonesia | Cross-sectional | 200 | Combination of DEC 6 mg/kg body weight, Albendazole 400 mg and Paracetamol 500 mg given once a year for a minimum of 5 consecutive years | Uptake rate 75.5% |
|
| Bhatia et al. 2018 [23] | Mass drug administration (MDA) for the elimination of lymphatic filariasis: Experiences from Nayagarh district of Odisha, India | Mixed method | 551 | DEC and Albendazole | Drug compliance rate (77.7%) Coverage compliance gap (22.3%) | Barriers for uptake are
|
| Krentel & Wellings 2018 [21] | The role of gender relations in uptake of mass drug administration for lymphatic filariasis in Alor District, Indonesia | Qualitative Study | 43 | A single dose of DEC or Ivermectin (in those areas where onchocerciasis or loiasis is endemic) in combination with Albendazole | 24/43 compliant treatment (55.8%) 19/43 non-compliant (44.2%) | Gender relations emerged as a key theme in the access, uptake, and compliance with MDA. Four models of responsibility for health decision-making emerged:
|
| Kisoka et al. 2014 [25] | Factors influencing drug uptake during mass drug administration for control of lymphatic filariasis in rural and urban Tanzania | Cross-sectional | 3279 | Combination of Ivermectin (150–200 µg/kg body weight) and Albendazole (400 mg) | Overall drug uptake rate was 55.1% (range of 44.5–75.6% between districts) | Factors associated with high uptake:
|
| Parker & Allen 2013 [26] | Will mass drug administration eliminate lymphatic filariasis? evidence from Northern Coastal Tanzania | Qualitative Study | 108 villagers | Albendazole, in combination with either DEC or Ivermectin; | Mwembeni village uptake 2007: 306 (34%) Jaira village uptake in 2007: 160 (42%) | Factors associated with low uptake:
|
| Amarillo et al. 2008 [27] | Factors associated with the acceptance of mass drug administration for the elimination of lymphatic filariasis in Agusan del Sur, Philippines | Mixed method | 437 | DEC and Albendazole | Acceptance rate: 60% |
|
| Mathieu et al. 2004 [28] | Factors associated with participation in a campaign of mass treatment against lymphatic filariasis in Leogane, Haiti | Cross-sectional | 305 | DEC and Albendazole | MDA coverage: 63.9% |
|
| Rosanti et al. 2016 [20] | Directly observed treatment increases drug compliance in lymphatic filariasis mass drug administration | Longitudinal study | 90 | A single dose of DEC (three 100 mg tablets for persons weighing 50 kg) with the addition of a single 400 mg dose of Albendazole | Drug compliance rate was 86.80% | Reasons for failing to take drugs:
|
| Nujum et al. 2012 [24] | Factors determining noncompliance to mass drug administration for lymphatic filariasis elimination | Case control | 99 cases (non-compliant), 70 control (compliant) | Single dose DEC | 39.52% taken the drug (247/625) | Non-compliant status associated with
|
| Author | Type of Study | 1.1 | 1.2 | 1.3 | 1.4 | 1.5 |
|---|---|---|---|---|---|---|
| Is the sampling strategy relevant to address the research question? | Is the sample representative of the target population? | Are the measurements appropriate? | Is the risk of nonresponse bias low? | Is the statistical analysis appropriate to answer the research question? | ||
| Niles RA et al. 2021 [9] | Quantitative descriptive | Yes | Yes | Yes | Yes | Yes |
| Putri et al. 2019 [22] | Quantitative descriptive | Yes | Yes | Yes | No | Yes |
| Kisoka et al. 2014 [25] | Quantitative descriptive | Yes | Yes | Yes | Can’t tell | Yes |
| Mathieu et al. 2004 [28] | Quantitative descriptive | Yes | Yes | Yes | Yes | Yes |
| Rosanti et al. 2016 [20] | Quantitative descriptive | Yes | Yes | Yes | Yes | Yes |
| Nujum et al. 2012 [24] | Quantitative descriptive | Yes | Yes | Yes | Yes | Yes |
| Is the qualitative approach appropriate to answer the research question? | Are the qualitative data collection methods adequate to address the research question? | Are the findings adequately derived from the data? | Is the interpretation of results sufficiently substantiated the data? | Is there coherence between qualitative data sources, collection, analysis and interpretation? | ||
| Adekeye et al. 2020 [19] | Qualitative | Yes | Yes | Yes | Yes | Yes |
| Krentel & Wellings 2018 [21] | Qualitative | Yes | Yes | Yes | Yes | Yes |
| Parker & Allen 2013 [26] | Qualitative | Yes | Yes | Yes | Yes | Yes |
| Is there an adequate rationale for using a mixed methods design to address the research question? | Are the different components of the study effectively integrated to answer the research question? | Are the outputs of the integration of qualitative and quantitative component adequately interpreted? | Are the divergences and inconsistencies between quantitative and qualitative results adequately addresses? | Do the different components of the study adhere to the quality criteria of each tradition of the methods involved? | ||
| Amarillo et al. 2008 [27] | Mixed-method | Yes | No | No | No | No |
| Bhatia et al. 2018 [23] | Mixed-method | Yes | Yes | Yes | No | Yes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdul Halim, A.F.N.; Ahmad, D.; Miaw Yn, J.L.; Masdor, N.A.; Ramly, N.; Othman, R.; Kandayah, T.; Hassan, M.R.; Dapari, R. Factors Associated with the Acceptability of Mass Drug Administration for Filariasis: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 12971. https://doi.org/10.3390/ijerph191912971
Abdul Halim AFN, Ahmad D, Miaw Yn JL, Masdor NA, Ramly N, Othman R, Kandayah T, Hassan MR, Dapari R. Factors Associated with the Acceptability of Mass Drug Administration for Filariasis: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(19):12971. https://doi.org/10.3390/ijerph191912971
Chicago/Turabian StyleAbdul Halim, Ahmad Farid Nazmi, Dzulfitree Ahmad, Jane Ling Miaw Yn, Noor Azreen Masdor, Nurfatehar Ramly, Rahayu Othman, Thinakaran Kandayah, Mohd Rohaizat Hassan, and Rahmat Dapari. 2022. "Factors Associated with the Acceptability of Mass Drug Administration for Filariasis: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 19: 12971. https://doi.org/10.3390/ijerph191912971