

Compliance to Guidelines in Prescribing Empirical Antibiotics for Individuals with Uncomplicated Urinary Tract Infection in a Primary Health Facility of Ghana, 2019–2021
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting
2.2.1. General Setting
2.2.2. Specific Setting
2.2.3. Management of Uncomplicated UTI
2.2.4. Electronic Medical Records
2.3. Study Population and Period
2.4. Data Variables, Collection and Source of Data
2.5. Data Analysis
3. Results
3.1. Socio-Demographic and Clinical Characteristics
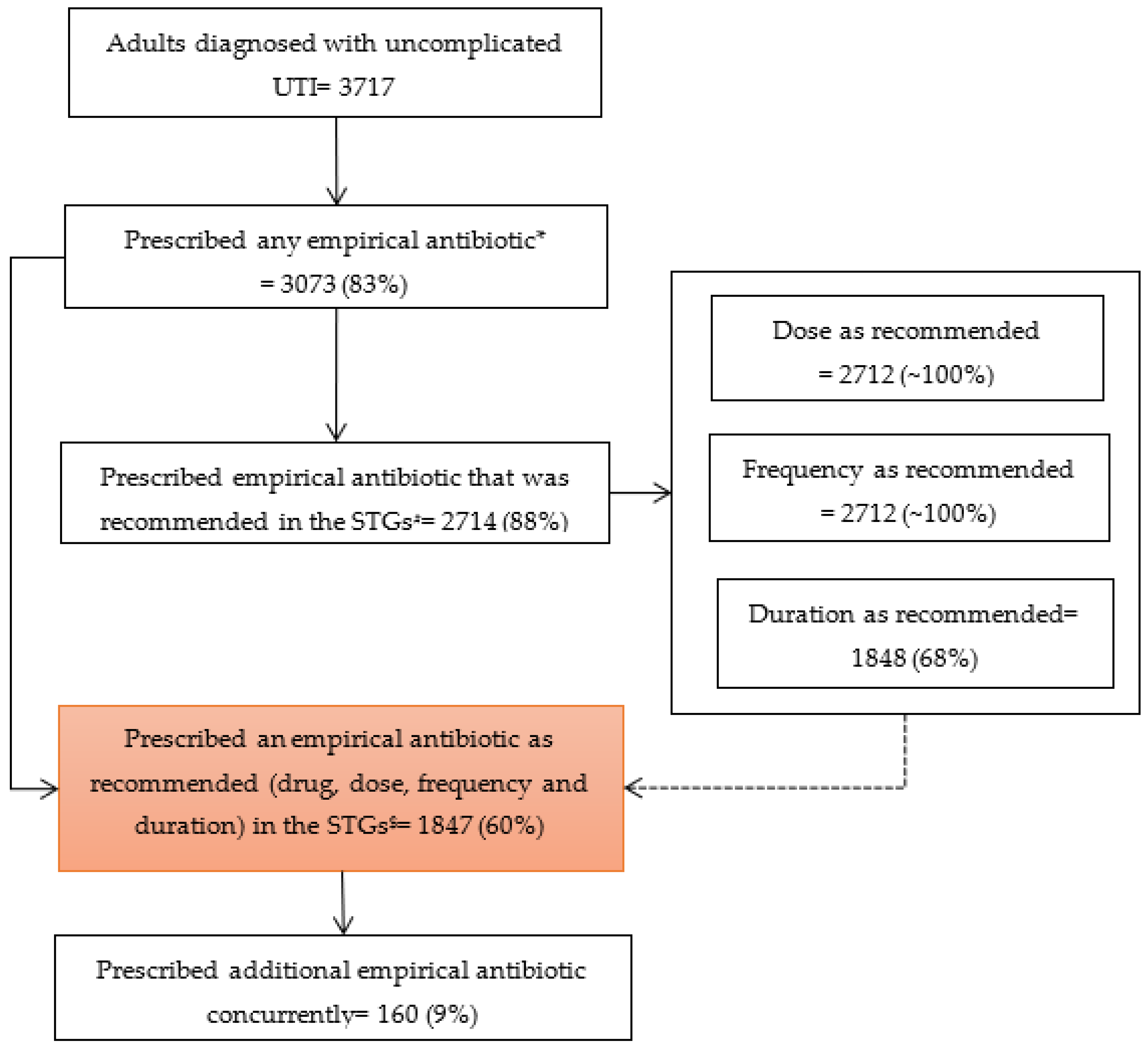
3.2. Prescription of Empirical Antibiotic
3.3. Prescription of Empirical Antibiotics as Recommended in STGs (Dose, Frequency and Duration)
3.4. Patient and Prescriber Characteristics Associated with Prescription of Empirical Antibiotics Not as Recommended in the STGs
3.5. Distribution of Prescribed Empirical Antibiotics across the WHO AWaRe Category
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tandogdu, Z.; Wagenlehner, F. Global Epidemiology of Urinary Tract Infections. Curr. Opin. Infect. Dis. 2016, 29, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Foxman, B. Epidemiology of Urinary Tract Infections: Incidence, Morbidity, and Economic Costs. Am. J. Med. 2002, 113 Suppl. S1A, 5–13. [Google Scholar] [CrossRef]
- Foxman, B. The Epidemiology of Urinary Tract Infection. Nat. Rev. Urol. 2010, 7, 653–660. [Google Scholar] [CrossRef] [PubMed]
- Edmond, P. Urinary Tract Infection in Adults. Clin. Microbiol. Open Access 2014, 3, 1000el20. [Google Scholar] [CrossRef]
- Flores-Mireles, A.L.; Walker, J.N.; Caparon, M.; Hultgren, S.J. Urinary Tract Infections: Epidemiology, Mechanisms of Infection and Treatment Options. Nat. Rev. Microbiol. 2015, 13, 269–284. [Google Scholar] [CrossRef]
- Ong Lopez, A.; Tan, C.; Yabon, A.; Masbang, A. Symptomatic Treatment (Using NSAIDS) versus Antibiotics in Uncomplicated Lower Urinary Tract Infection: A Meta-Analysis and Systematic Review of Randomized Controlled Trials. BMC Infect. Dis. 2021, 21, 619. [Google Scholar] [CrossRef]
- Falagas, M.E.; Kotsantis, I.K.; Vouloumanou, E.K.; Rafailidis, P.I. Antibiotics versus Placebo in the Treatment of Women with Uncomplicated Cystitis: A Meta-Analysis of Randomized Controlled Trials. J. Infect. 2009, 58, 91–102. [Google Scholar] [CrossRef]
- Gupta, K.; Grigoryan, L.; Trautner, B. Urinary Tract Infection. Ann. Intern. Med. 2017, 167, ITC49–ITC64. [Google Scholar] [CrossRef]
- Gupta, K.; Hooton, T.M.; Naber, K.G.; Rn Wullt, B.; Colgan, R.; Miller, L.G.; Moran, G.J.; Nicolle, L.E.; Raz, R.; Schaeffer, A.J.; et al. International Clinical Practice Guidelines for the Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in Women: A 2010 Update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin. Infect. Dis. 2011, 52, e103–e120. [Google Scholar] [CrossRef]
- Wang, R.; LaSala, C. Role of Antibiotic Resistance in Urinary Tract Infection Management: A Cost-Effectiveness Analysis. Am. J. Obstet. Gynecol. 2021, 225, 550.e1–550.e10. [Google Scholar] [CrossRef]
- Appaneal, H.; Shireman, T.; Lopes, V.; Mor, V.; Dosa, D.; LaPlante, K.; Caffrey, A. Poor Clinical Outcomes Associated with Suboptimal Antibiotic Treatment among Older Long-Term Care Facility Residents with Urinary Tract Infection: A Retrospective Cohort Study. BMC Geriatr. 2021, 21, 436. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Chen, Y.; Hang, Y.; Luo, H.; Fang, X.; Xiao, Y.; Cao, X.; Zou, S.; Hu, X.; Hu, L.; et al. Impact of Inappropriate Empirical Antibiotic Treatment on Clinical Outcomes of Urinary Tract Infections Caused by Escherichia Coli: A Retrospective Cohort Study. J. Glob. Antimicrob. Resist. 2021, 26, 148–153. [Google Scholar] [CrossRef] [PubMed]
- Bryce, A.; Hay, A.; Lane, I.; Thornton, H.; Wootton, M.; Costelloe, C. Global Prevalence of Antibiotic Resistance in Paediatric Urinary Tract Infections Caused by Escherichia Coli and Association with Routine Use of Antibiotics in Primary Care: Systematic Review and Meta-Analysis. BMJ 2016, 352, i939. [Google Scholar] [CrossRef] [PubMed]
- Sugianli, A.K.; Ginting, F.; Parwati, I.; de Jong, M.D.; van Leth, F.; Schultsz, C. Antimicrobial Resistance among Uropathogens in the Asia-Pacific Region: A Systematic Review. JAC-Antimicrob. Resist. 2021, 3, dlab003. [Google Scholar] [CrossRef]
- Bernabé, K.; Langendorf, C.; Ford, N.; Ronat, J.; Murphy, R. Antimicrobial Resistance in West Africa: A Systematic Review and Meta-Analysis. Int. J. Antimicrob. Agents 2017, 50, 629–639. [Google Scholar] [CrossRef]
- Mulder, M.; Baan, E.; Verbon, A.; Stricker, B.; Verhamme, K. Trends of Prescribing Antimicrobial Drugs for Urinary Tract Infections in Primary Care in the Netherlands: A Population-Based Cohort Study. BMJ Open 2019, 9, e027221. [Google Scholar] [CrossRef]
- Isberg, H.K.; Hedin, K.; Melander, E.; Mölstad, S.; Beckman, A. Increased Adherence to Treatment Guidelines in Patients with Urinary Tract Infection in Primary Care: A Retrospective Study. PLoS ONE 2019, 14, e0214572. [Google Scholar] [CrossRef]
- Langner, J.L.; Chiang, K.F.; Stafford, R.S. Current Prescribing Practices and Guideline Concordance for the Treatment of Uncomplicated Urinary Tract Infections in Women. Am. J. Obstet. Gynecol. 2021, 225, 272.e1–272.e11. [Google Scholar] [CrossRef]
- Grigoryan, L.; Zoorob, R.; Wang, H.; Trautner, B.W. Low Concordance With Guidelines for Treatment of Acute Cystitis in Primary Care. Open Forum Infect. Dis. 2015, 2, ofv159. [Google Scholar] [CrossRef]
- Durkin, M.J.; Keller, M.; Butler, A.M.; Kwon, J.H.; Dubberke, E.R.; Miller, A.C.; Polgreen, P.M.; Olsen, M.A. An Assessment of Inappropriate Antibiotic Use and Guideline Adherence for Uncomplicated Urinary Tract Infections. Open Forum Infect. Dis. 2018, 5, ofy198. [Google Scholar] [CrossRef]
- Wong, C.; Kung, K.; Au-Doung, P.; Ip, M.; Lee, N.; Fung, A.; Wong, S. Antibiotic Resistance Rates and Physician Antibiotic Prescription Patterns of Uncomplicated Urinary Tract Infections in Southern Chinese Primary Care. PLoS ONE 2017, 12, e0177266. [Google Scholar] [CrossRef] [PubMed]
- Kabbara, W.K.; Meski, M.M.; Ramadan, W.H.; Maaliki, D.S.; Salameh, P. Adherence to International Guidelines for the Treatment of Uncomplicated Urinary Tract Infections in Lebanon. Can. J. Infect. Dis. Med. Microbiol. 2018, 2018, 7404095. [Google Scholar] [CrossRef] [PubMed]
- Wiedenmayer, K.; Ombaka, E.; Kabudi, B.; Canavan, R.; Rajkumar, S.; Chilunda, F.; Sungi, S.; Stoermer, M. Adherence to Standard Treatment Guidelines among Prescribers in Primary Healthcare Facilities in the Dodoma Region of Tanzania. BMC Health Serv. Res. 2021, 21, 272. [Google Scholar] [CrossRef]
- World Health Organization. Antimicrobial Stewardship Programmes in Health-Care Facilities in Low- and Middle-Income Countries. A WHO Practical Toolkit; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Donkor, E.S.; Horlortu, P.Z.; Dayie, N.T.K.D.; Obeng-Nkrumah, N.; Labi, A.K. Community Acquired Urinary Tract Infections among Adults in Accra, Ghana. Infect. Drug Resist. 2019, 12, 2059–2067. [Google Scholar] [CrossRef] [PubMed]
- Gambrah, E.; Owusu-Ofori, A.; Biney, E.; Oppong, C.; Coffin, S.E. Diagnosis and Treatment of Urinary Tract Infections in Hospitalized Adults in Ghana: The Role of the Clinical Microbiology Laboratory in Improving Antimicrobial Stewardship. Int. J. Infect. Dis. 2021, 102, 497–500. [Google Scholar] [CrossRef]
- Ministry of Health. Ghana National Drugs Programme Urinary Tract Infection. In Standard Treatment Guidelines, 7th ed.; Ministry of Health: Accra, Ghana, 2017; pp. 401–403. ISBN 9789988257873. [Google Scholar]
- Abdulai, A.-F.; Adam, F. Health Providers’ Readiness for Electronic Health Records Adoption: A Cross-Sectional Study of Two Hospitals in Northern Ghana. PLoS ONE 2020, 15, e0231569. [Google Scholar] [CrossRef]
- Ghana Statistical Service. 2021 Population and Housing Census- Press Release on Provisional Results; Ghana Statistical Service: Accra, Ghana, 2021.
- The World Bank Ghana Overview: Development News, Research, Data|World Bank. Available online: https://www.worldbank.org/en/country/ghana/overview#1 (accessed on 6 November 2021).
- Alhassan, R.K.; Nketiah-Amponsah, E.; Arhinful, D.K. A Review of the National Health Insurance Scheme in Ghana: What Are the Sustainability Threats and Prospects? PLoS ONE 2016, 11, e0165151. [Google Scholar] [CrossRef]
- Akazili, J.; McIntyre, D.; Kanmiki, E.W.; Gyapong, J.; Oduro, A.; Sankoh, O.; Ataguba, J.E. Assessing the Catastrophic Effects of Out-of-Pocket Healthcare Payments Prior to the Uptake of a Nationwide Health Insurance Scheme in Ghana. Glob. Health Action 2017, 10, 1289735. [Google Scholar] [CrossRef]
- Wang, H.; Otoo, N.; Dsane-Selby, L. Ghana National Health Insurance Scheme: Improving Financial Sustainability Based on Expenditure Review; World Bank: Washington, DC, USA, 2017; ISBN 978-1-4648-1117-3. [Google Scholar]
- National Health Insurance Agency National Health Insurance Scheme. Available online: http://www.nhis.gov.gh/Default.aspx (accessed on 6 November 2021).
- Ayanore, M.A.; Pavlova, M.; Kugbey, N.; Fusheini, A.; Tetteh, J.; Ayanore, A.A.; Akazili, J.; Adongo, P.B.; Groot, W. Health Insurance Coverage, Type of Payment for Health Insurance, and Reasons for Not Being Insured under the National Health Insurance Scheme in Ghana. Health Econ. Rev. 2019, 9, 39. [Google Scholar] [CrossRef]
- Zhen, L.; Jin, C.; Xu, H.N. The Impact of Prescriptions Audit and Feedback for Antibiotic Use in Rural Clinics: Interrupted Time Series with Segmented Regression Analysis. BMC Health Serv. Res. 2018, 18, 777. [Google Scholar] [CrossRef] [Green Version]
- Murray, C.J.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Robles Aguilar, G.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E.; et al. Global Burden of Bacterial Antimicrobial Resistance in 2019: A Systematic Analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Lim, A.H.; Thian, S.Y.; Hor, Y.Y.; Wong, S.T.; Tew, W.Y.; Chiew, S.Y.; Lee, X.; Yunus, M.A.M. Antibiotic Prescribing Pattern in Primary Care Practice in Federal Territory Kuala Lumpur and Putrajaya. Int. J. Infect. Dis. 2020, 101, 92. [Google Scholar] [CrossRef]
- Sefah, I.A.; Essah, D.O.; Kurdi, A.; Sneddon, J.; Alalbila, T.M.; Kordorwu, H.; Godman, B. Assessment of Adherence to Pneumonia Guidelines and Its Determinants in an Ambulatory Care Clinic in Ghana: Findings and Implications for the Future. JAC-Antimicrob. Resist. 2021, 3, dlab080. [Google Scholar] [CrossRef] [PubMed]
- O’Keefe, C.; Thompson, A.; McKenzie, D.; Lee, K. Concordance with Antibiotic Guidelines in Australian Primary Care: A Retrospective Study of Prior-to-hospital Therapy. Int. J. Clin. Pract. 2019, 73, e13427. [Google Scholar] [CrossRef]
- Phamnguyen, T.J.; Murphy, G.; Hashem, F. Single Centre Observational Study on Antibiotic Prescribing Adherence to Clinical Practice Guidelines for Treatment of Uncomplicated Urinary Tract Infection. Infect. Dis. Health 2019, 24, 75–81. [Google Scholar] [CrossRef]
- Spellberg, B.; Rice, L.B. Duration of Antibiotic Therapy: Shorter Is Better. Ann. Intern. Med. 2019, 171, 210. [Google Scholar] [CrossRef]
- Pouwels, K.B.; Hopkins, S.; Llewelyn, M.J.; Walker, A.S.; McNulty, C.A.; Robotham, J.V. Duration of Antibiotic Treatment for Common Infections in English Primary Care: Cross Sectional Analysis and Comparison with Guidelines. BMJ 2019, 364, 440. [Google Scholar] [CrossRef]
- Palin, V.; Welfare, W.; Ashcroft, D.M.; Van Staa, T.P. Shorter and Longer Courses of Antibiotics for Common Infections and the Association With Reductions of Infection-Related Complications Including Hospital Admissions. Clin. Infect. Dis. 2021, 73, 1805–1812. [Google Scholar] [CrossRef]
- Morgan, D.J.; Coffey, K.C. Shorter Courses of Antibiotics for Urinary Tract Infection in Men. JAMA 2021, 326, 309–310. [Google Scholar] [CrossRef]
- Germanos, G.J.; Trautner, B.W.; Zoorob, R.J.; Salemi, J.L.; Drekonja, D.; Gupta, K.; Grigoryan, L. No Clinical Benefit to Treating Male Urinary Tract Infection Longer Than Seven Days: An Outpatient Database Study. Open Forum Infect. Dis. 2019, 6, ofz216. [Google Scholar] [CrossRef] [PubMed]
- Plate, A.; Kronenberg, A.; Risch, M.; Mueller, Y.; Di Gangi, S.; Rosemann, T.; Senn, O. Treatment of Urinary Tract Infections in Swiss Primary Care: Quality and Determinants of Antibiotic Prescribing. BMC Fam. Pract. 2020, 21, 125. [Google Scholar] [CrossRef]
- Llor, C.; Bjerrum, L. Antimicrobial Resistance: Risk Associated with Antibiotic Overuse and Initiatives to Reduce the Problem. Ther. Adv. Drug Saf. 2014, 5, 229. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.J.; Wattles, B.A. Appropriate Antibiotic Prescribing—The Safer and Less Expensive Choice. JAMA Netw. Open 2022, 5, e2214160. [Google Scholar] [CrossRef] [PubMed]
- Bader, M.S.; Loeb, M.; Leto, D.; Brooks, A.A. Treatment of Urinary Tract Infections in the Era of Antimicrobial Resistance and New Antimicrobial Agents. Postgrad. Med. 2020, 132, 234–250. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Total | Empirical Antibiotic Use | p Value e | ||
|---|---|---|---|---|---|
| N | (%) a | n | (%) b | ||
| Total | 3717 | (100) | 3073 | (83) | |
| Age in years | |||||
| 18–29 | 757 | (20.4) | 632 | (83.5) | 0.262 |
| 30–44 | 919 | (24.7) | 775 | (84.3) | |
| 45–59 | 804 | (21.6) | 661 | (82.2) | |
| ≥60 | 1237 | (33.3) | 1005 | (81.2) | |
| Gender | |||||
| Male | 1064 | (28.6) | 878 | (82.5) | 0.874 |
| Female | 2653 | (71.4) | 2195 | (82.7) | |
| Occupation | |||||
| Employed | 1909 | (51.4) | 1577 | (82.6) | 0.993 |
| Unemployed | 592 | (15.9) | 489 | (82.6) | |
| Student | 320 | (8.6) | 267 | (83.4) | |
| Retired | 238 | (6.4) | 195 | (81.9) | |
| Not recorded | 658 | (17.7) | 545 | (82.8) | |
| NHIS | |||||
| Yes | 2920 | (78.6) | 2402 | (82.3) | 0.202 |
| No | 797 | (21.4) | 671 | (84.2) | |
| Year | |||||
| 2019 | 644 | (17.3) | 533 | (82.8) | 0.255 |
| 2020 | 1746 | (47.0) | 1426 | (81.7) | |
| 2021 | 1327 | (35.7) | 1114 | (84.0) | |
| Comorbidities c | |||||
| Diabetes Mellitus | 621 | (16.7) | 497 | (80.0) | 0.111 |
| Hypertension | 1231 | (33.1) | 1024 | (83.2) | 0.508 |
| Urine routine examination | |||||
| Not done | 1137 | (30.5) | 979 | (86.1) | 0.001 |
| Done | 2574 | (69.3) | 2089 | (81.2) | |
| Missing | 6 | (0.2) | 5 | (83.3) | |
| Prescriber gender | |||||
| Male | 2084 | (56.0) | 1719 | (82.5) | 0.915 |
| Female | 1623 | (43.7) | 1346 | (83.0) | |
| Missing | 10 | (0.3) | 8 | (80.0) | |
| Prescriber rank d | |||||
| Physician Assistant | 36 | (1.0) | 27 | (75.5) | 0.570 |
| Medical Officer | 1616 | (43.5) | 1349 | (83.5) | |
| Senior/Deputy Medical Officer | 348 | (9.4) | 290 | (83.3) | |
| Resident | 1136 | (30.6) | 936 | (82.4) | |
| Specialist | 578 | (15.6) | 469 | (81.1) | |
| Missing | |||||
| Characteristics | Total | Empirical Antibiotics not as Recommended in STGs | Unadjusted b | Adjusted c | |||
|---|---|---|---|---|---|---|---|
| N | n | (%) a | PR | (95% CI) | aPR | (95% CI) | |
| Total | 3073 | 1226 | (39.9) | ||||
| Age in years | |||||||
| 18–29 | 632 | 234 | (37.0) | 1 | 1 | ||
| 30–44 | 775 | 313 | (40.4) | 1.1 | (1.0–1.3) | 1.1 | (1.0–1.2) |
| 45–59 | 661 | 251 | (38.0) | 1.0 | (0.9–1.2) | 1.0 | (0.9–1.2) |
| ≥60 | 1005 | 428 | (42.6) | 1.1 | (1.0–1.3) | 1.0 | (0.9–1.2) |
| Gender | |||||||
| Male | 878 | 819 | (93.3) | 5.0 | (4.6–5.5) | 5.0 | (4.6–5.5) f |
| Female | 2195 | 407 | (18.5) | 1 | 1 | ||
| Occupation | |||||||
| Employed | 1577 | 632 | (40.1) | 0.9 | (0.9–1.1) | 1.0 | (0.8–1.1) |
| Unemployed | 489 | 200 | (40.9) | 1 | 1 | ||
| Student | 267 | 99 | (37.1) | 0.9 | (0.8–1.1) | 0.9 | (0.8–1.2) |
| Retired | 195 | 96 | (49.2) | 1.2 | (1.0–1.5) | 1.0 | (0.8–1.1) |
| Not recorded | 545 | 199 | (36.5) | 0.9 | (0.8–1.1) | 0.9 | (0.8–1.0) |
| NHIS | |||||||
| Yes | 2402 | 938 | (39.1) | 1 | 1 | ||
| No | 671 | 288 | (42.9) | 1.1 | (1.0–1.3) | 1.0 | (0.9–1.1) |
| Year | |||||||
| 2019 | 533 | 200 | (37.5) | 1 | 1 | ||
| 2020 | 1426 | 565 | (39.6) | 1.0 | (0.9–1.2) | 1.0 | (0.9–1.1) |
| 2021 | 1114 | 461 | (41.4) | 1.1 | (1.0–1.3) | 1.2 | (1.0–1.3) f |
| Comorbidities d | |||||||
| Diabetes Mellitus | 497 | 197 | (39.6) | 1.0 | (0.8–1.1) | 1.0 | (0.9–1.1) |
| Hypertension | 1024 | 412 | (40.2) | 1.0 | (0.9–1.1) | 1.0 | (0.9–1.1) |
| Urine routine examination | |||||||
| Done | 2089 | 867 | (41.5) | 1 | 1 | ||
| Not done | 979 | 356 | (36.4) | 0.9 | (0.8–1.0) | 0.9 | (0.8–1.0) |
| Not recorded | 5 | 3 | (60.0) | 1.5 | (0.7–3.3) | 1.3 | (0.7–2.3) |
| Prescriber gender | |||||||
| Male | 1719 | 708 | (41.2) | 1 | 1 | ||
| Female | 1346 | 516 | (38.3) | 0.9 | (0.9–1.0) | 0.9 | (0.9–1.0) |
| Missing | 8 | 2 | (25.0) | 0.6 | (0.2–2.0) | 0.5 | (0.1–1.9) |
| Prescriber rank e | |||||||
| Physician Assistant | 27 | 11 | (40.7) | 0.8 | (0.5–1.3) | 1.0 | (0.6–1.5) |
| Medical Officer | 1349 | 545 | (40.4) | 0.9 | (0.8–1.0) | 1.0 | (0.9–1.1) |
| Senior/Deputy Medical Officer | 290 | 133 | (46.0) | 1 | 1 | ||
| Resident | 936 | 367 | (39.2) | 0.8 | (0.7–1.0) | 1.0 | (0.9–1.1) |
| Specialist | 469 | 169 | (36.0) | 0.8 | (0.6–0.9) | 0.9 | (0.7–1.0) |
| Missing | 2 | 1 | (50.0) | 0.9 | (0.2–4.3) | 1.3 | (0.4–4.8) |
| Antibiotic | N | (%) |
|---|---|---|
| Total * | 3378 | (100) # |
| Access | ||
| Tinidazole | 119 | (3.5) |
| Nitrofurantoin | 90 | (2.7) |
| Doxycycline | 88 | (2.6) |
| Amoxicillin/clavulanic acid | 52 | (1.5) |
| Secnidazole | 20 | (0.6) |
| Metronidazole | 8 | (0.2) |
| Clindamycin | 2 | (0.06) |
| Amoxicillin | 1 | (0.03) |
| Sulfamethoxazole/trimethoprim | 1 | (0.03) |
| Watch | ||
| Cefuroxime | 1831 | (54.2) |
| Ciprofloxacin | 1036 | (30.7) |
| Cefixime | 38 | (1.1) |
| Ceftriaxone | 33 | (1.0) |
| Levofloxacin | 31 | (0.9) |
| Azithromycin | 23 | (0.7) |
| Cefpodoxime | 3 | (0.1) |
| Clarithromycin | 2 | (0.1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Owusu, H.; Thekkur, P.; Ashubwe-Jalemba, J.; Hedidor, G.K.; Corquaye, O.; Aggor, A.; Steele-Dadzie, A.; Ankrah, D. Compliance to Guidelines in Prescribing Empirical Antibiotics for Individuals with Uncomplicated Urinary Tract Infection in a Primary Health Facility of Ghana, 2019–2021. Int. J. Environ. Res. Public Health 2022, 19, 12413. https://doi.org/10.3390/ijerph191912413
Owusu H, Thekkur P, Ashubwe-Jalemba J, Hedidor GK, Corquaye O, Aggor A, Steele-Dadzie A, Ankrah D. Compliance to Guidelines in Prescribing Empirical Antibiotics for Individuals with Uncomplicated Urinary Tract Infection in a Primary Health Facility of Ghana, 2019–2021. International Journal of Environmental Research and Public Health. 2022; 19(19):12413. https://doi.org/10.3390/ijerph191912413
Chicago/Turabian StyleOwusu, Helena, Pruthu Thekkur, Jacklyne Ashubwe-Jalemba, George Kwesi Hedidor, Oksana Corquaye, Asiwome Aggor, Allen Steele-Dadzie, and Daniel Ankrah. 2022. "Compliance to Guidelines in Prescribing Empirical Antibiotics for Individuals with Uncomplicated Urinary Tract Infection in a Primary Health Facility of Ghana, 2019–2021" International Journal of Environmental Research and Public Health 19, no. 19: 12413. https://doi.org/10.3390/ijerph191912413