
Believing Processes during the COVID-19 Pandemic: A Qualitative Analysis
 , , , , , and
, , , , , and
Abstract
:1. Introduction
- Proposition: In our example, “eatable” is the propositional content of a bab/clum. Bab is a neologism that was coined as a central unit of the functional process model of credition. As the believing process partly remains subliminal, it is important to integrate the aspect of subconsciousness. Blob and clum is the term which designates a subconscious bab. Thus, in the terminology of the model of credition, the mental mindset of someone is forced to start a believing process is called bab–blob configuration.
- Certainty: Regarding doubtable issues, persons may differ whether they are sure about them or not. In the language of the model of credition, we call this degree of certainty. In our example, the degree of certainty may differ between different persons. If someone has a degree of certainty of, for instance, 90%, they will be more ready to accept the clum “eatable” in their bab configuration than another person whose degree of certainty is only 55%.
- Emotional loading: The emotional loading of the clum eatable may be “disgusting”. In this case, it will be less likely that the clum can be integrated (i.e., believing that the meat is eatable) than in the case that the emotional loading might be shaped by “a little bit strange but interesting”.
- Sense of mightiness: The perspective of a subject is not limited to the emotions of a bab. It also includes the intensity of the emotion reflected by the sense of mightiness. If the emotional loading of disgust is mighty, it is less likely that the meat will be eaten than in the case that the disgust is more temporary and of a lower intensity.
- How do individuals experience the COVID-19 outbreak and which believing processes can be found?
- Which credition profiles can be generated (proposition, certainty, emotional loading, sense of mightiness)?
- Is the propositional content related to the emotion and vice versa?
- What is the association between beliefs and psychological symptoms (depression, anxiety, somatization, global symptom load, and sleep quality)?
2. Materials and Methods
2.1. Procedure
2.2. Participants
2.3. Psychological Inventories
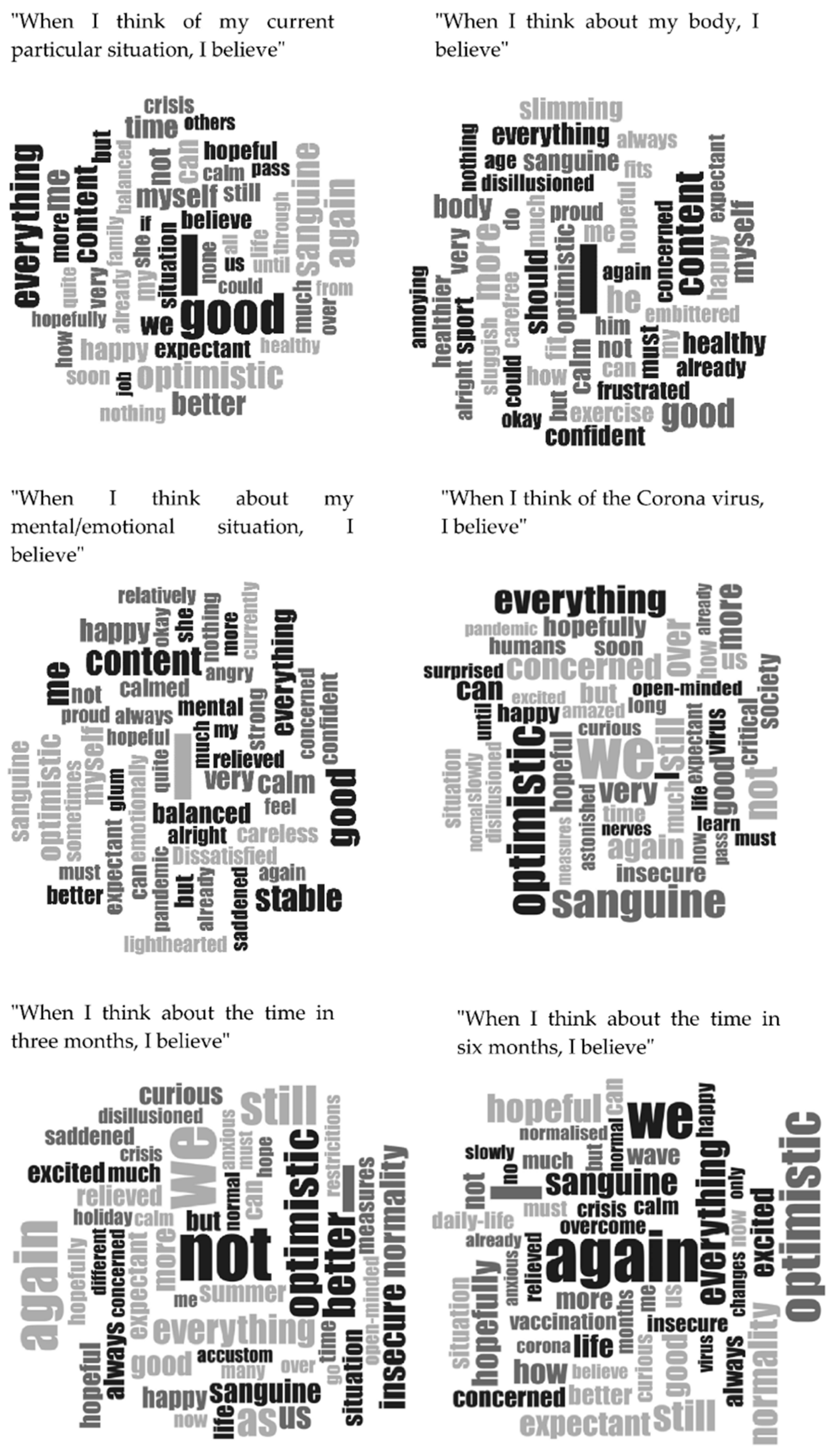
- When I think of the current very special situation, I believe:
- When I think about my body, I believe:
- When I think about my mental/emotional situation, I believe:
- When I think of the coronavirus disease (COVID-19), I believe:
- When I think about the time in three months, I believe:
- When I think about the time in six months, I believe:
2.4. Data Analysis and Statistical Methods
3. Results
3.1. Descriptive Statistics
3.2. Correlations between Psychological Variables and Credition Parameters
3.3. Word Clouds
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Daly, M.; Sutin, A.R.; Robinson, E. Longitudinal Changes in Mental Health and the COVID-19 Pandemic: Evidence from the UK Household Longitudinal Study. Psychol. Med. 2020, 1–10. [Google Scholar] [CrossRef]
- Castellini, G.; Rossi, E.; Cassioli, E.; Sanfilippo, G.; Innocenti, M.; Gironi, V.; Silvestri, C.; Voller, F.; Ricca, V. A Longitudinal Observation of General Psychopathology before the COVID-19 Outbreak and during Lockdown in Italy. J. Psychosom. Res. 2021, 141, 110328. [Google Scholar] [CrossRef]
- Godinić, D.; Obrenovic, B.; Khudaykulov, A. Effects of Economic Uncertainty on Mental Health in the COVID-19 Pandemic Context: Social Identity Disturbance, Job Uncertainty and Psychological Well-being Model. Int. J. Innov. Econ. Dev. 2020, 6, 61–74. [Google Scholar] [CrossRef]
- de Kloet, E.R.; Joels, M.; Holsboer, F. Stress and the Brain: From Adaptation to Disease. Nat. Rev. Neurosci. 2005, 6, 463–475. [Google Scholar] [CrossRef]
- Morales-Rodriguez, F.M.; Martinez-Ramon, J.P.; Mendez, I.; Ruiz-Esteban, C. Stress, Coping, and Resilience before and After COVID-19: A Predictive Model Based on Artificial Intelligence in the University Environment. Front. Psychol. 2021, 12, 647964. [Google Scholar] [CrossRef]
- Taylor, S.E.; Stanton, A.L. Coping Resources, Coping Processes, and Mental Health. Annu. Rev. Clin. Psychol. 2007, 3, 377–401. [Google Scholar] [CrossRef]
- Bauerle, A.; Teufel, M.; Musche, V.; Weismuller, B.; Kohler, H.; Hetkamp, M.; Dorrie, N.; Schweda, A.; Skoda, E.M. Increased Generalized Anxiety, Depression and Distress during the COVID-19 Pandemic: A Cross-Sectional Study in Germany. J. Public Health 2020, 42, 672–678. [Google Scholar] [CrossRef]
- Flesia, L.; Monaro, M.; Mazza, C.; Fietta, V.; Colicino, E.; Segatto, B.; Roma, P. Predicting Perceived Stress Related to the COVID-19 Outbreak through Stable Psychological Traits and Machine Learning Models. J. Clin. Med. 2020, 9, 3350. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The Psychological Impact of Quarantine and how to Reduce it: Rapid Review of the Evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef]
- Jones, E.A.K.; Mitra, A.K.; Bhuiyan, A.R. Impact of COVID-19 on Mental Health in Adolescents: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 2470. [Google Scholar] [CrossRef]
- Pieh, C.; Budimir, S.; Probst, T. The Effect of Age, Gender, Income, Work, and Physical Activity on Mental Health during Coronavirus Disease (COVID-19) Lockdown in Austria. J. Psychosom. Res. 2020, 136, 110186. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.E.; Mottershaw, A.L.; Egan, M.; Waller, J.; Marteau, T.M.; Rubin, G.J. The Impact of Believing You have had COVID-19 on Self-Reported Behaviour: Cross-Sectional Survey. PLoS ONE 2020, 15, e0240399. [Google Scholar] [CrossRef]
- Tietz, S.; Wagner-Skacel, J.; Angel, H.; Ratzenhofer, M.; Fellendorf, F.T.; Fleischmann, E.; Körner, C.; Reininghaus, E.Z.; Seitz, R.J.; Dalkner, N. Believing Processes during the COVID-19 Pandemic in Individuals with Bipolar Disorder: An Exploratory Study. World J. Psychiatry 2022, 12, 929–943. [Google Scholar] [CrossRef]
- Frith, C.D.; Frith, U. The Neural Basis of Mentalizing. Neuron 2006, 50, 531–534. [Google Scholar] [CrossRef]
- Bernroider, G.; Panksepp, J. Mirrors and Feelings: Have You seen the Actors Outside? Neurosci. Biobehav. Rev. 2011, 35, 2009–2016. [Google Scholar] [CrossRef] [PubMed]
- Bastiaansen, L.; Hopwood, C.J.; Van den Broeck, J.; Rossi, G.; Schotte, C.; de Fruyt, F. The Twofold Diagnosis of Personality Disorder: How do Personality Dysfunction and Pathological Traits Increment each Other at Successive Levels of the Trait Hierarchy? Personal. Disord. 2016, 7, 280–292. [Google Scholar] [CrossRef]
- Panksepp, J.; Solms, M. What is Neuropsychoanalysis? Clinically Relevant Studies of the Minded Brain. Trends Cogn. Sci. 2012, 16, 6–8. [Google Scholar] [CrossRef]
- Seitz, R.J.; Paloutzian, R.F.; Angel, H.F. From Believing to Belief: A General Theoretical Model. J. Cogn. Neurosci. 2018, 30, 1254–1264. [Google Scholar] [CrossRef] [PubMed]
- Churchland, P.S.; Churchland, P.M. The Neural Basis of Human Belief Systems, 1st ed.; Psychology Press: Hove, UK, 2013; pp. 1–18. [Google Scholar]
- Baumann, Z. Modernity as History of Time. Concepts Transform. 1999, 4, 229–248. [Google Scholar] [CrossRef]
- Angel, H.F.; Seitz, R.J. Violations of Expectations as Matter for the Believing Process. Front. Psychol. 2017, 8, 772. [Google Scholar] [CrossRef] [Green Version]
- Seitz, R.J.; Angel, H.F. Processes of Believing—A Review and Conceptual Account. Rev. Neurosci. 2012, 23, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Seitz, R.J.; Angel, H.F. Belief Formation—A Driving Force for Brain Evolution. Brain Cogn. 2020, 140, 105548. [Google Scholar] [CrossRef]
- Iriki, A.; Taoka, M. Triadic (Ecological, Neural, Cognitive) Niche Construction: A Scenario of Human Brain Evolution Extrapolating Tool use and Language from the Control of Reaching Actions. Philos. Trans. R. Soc. B Biol. Sci. 2012, 367, 10–23. [Google Scholar] [CrossRef] [PubMed]
- Seitz, R.J. Believing and Beliefs-Neurophysiological Underpinnings. Front. Behav. Neurosci. 2022, 16, 880504. [Google Scholar] [CrossRef]
- Aguilar-Raab, C.; Grevenstein, D.; Gotthardt, L.; Jarczok, M.N.; Hunger, C.; Ditzen, B.; Schweitzer, J. Changing Me, Changing Us: Relationship Quality and Collective Efficacy as Major Outcomes in Systemic Couple Therapy. Fam. Process 2018, 57, 342–358. [Google Scholar] [CrossRef]
- Seitz, R.J.; Paloutzian, R.F.; Angel, H.F. Believing is Representation Mediated by the Dopamine Brain System. Eur. J. Neurosci. 2019, 49, 1212–1214. [Google Scholar] [CrossRef]
- Bongelli, R.; Canestrari, C.; Fermani, A.; Muzi, M.; Riccioni, I.; Bertolazzi, A.; Burro, R. Associations between Personality Traits, Intolerance of Uncertainty, Coping Strategies, and Stress in Italian Frontline and Non-Frontline HCWs during the COVID-19 Pandemic-A Multi-Group Path-Analysis. Healthcare 2021, 9, 1086. [Google Scholar] [CrossRef]
- Nussmayr, K. 15 Grafiken, die die Verbreitung des Coronavirus in Österreich und der Welt erklären. Die Presse. 2020. Available online: https://www.diepresse.com/5785804/15-grafiken-die-die-verbreitung-des-coronavirusin-osterreich-und-der-welt-erklaren (accessed on 8 June 2022).
- Dalkner, N.; Ratzenhofer, M.; Fleischmann, E.; Fellendorf, F.T.; Bengesser, S.; Birner, A.; Maget, A.; Großschädl, K.; Lenger, M.; Platzer, M.; et al. Psychological and Behavioral Response on the COVID-19 Pandemic in Individuals with Bipolar Disorder: A Multicenter Study. Psychiatry Res. 2022, 310, 114451. [Google Scholar] [CrossRef]
- Derogatis, L.R.; Fitzpatrick, M. The SCL-90-R, the Brief Symptom Inventory (BSI), and the BSI-18. In The Use of Psychological Testing for Treatment Planning and Outcomes Assessment: Instruments for Adults, 3rd ed.; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 2004; Volume 3, pp. 1–41. [Google Scholar]
- Derogatis, L.R.; Unger, R. Symptom Checklist-90-Revised. In The Corsini Encyclopedia of Psychology; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2010; pp. 1–2. [Google Scholar]
- Spitzer, C.; Hammer, S.; Löwe, B.; Grabe, H.J.; Barnow, S.; Rose, M.; Wingenfeld, K.; Freyberger, H.J.; Franke, G.H. The Short Version of the Brief Symptom Inventory (BSI -18): Preliminary Psychometric Properties of the German Translation. Fortschr. Neurol. 2011, 79, 517–523. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A New Instrument for Psychiatric Practice and Research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Ekman, P. An Argument for Basic Emotions. Cogn. Emot. 1992, 6, 169–200. [Google Scholar] [CrossRef]
- VERBI Software. MAXQDA 2020 [Computer-Software]. 2019. Available online: https://www.maxqda.de (accessed on 5 January 2022).
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer Publishing Company: New York, NY, USA, 1984. [Google Scholar]
- Bonanno, G.A.; Burton, C.L. Regulatory Flexibility: An Individual Differences Perspective on Coping and Emotion Regulation. Perspect. Psychol. Sci. 2013, 8, 591–612. [Google Scholar] [CrossRef]
- McLelland, V.C.; Devitt, A.L.; Schacter, D.L.; Addis, D.R. Making the Future Memorable: The Phenomenology of Remembered Future Events. Memory 2015, 23, 1255–1263. [Google Scholar] [CrossRef]
- Burgdorf, J.; Panksepp, J. The Neurobiology of Positive Emotions. Neurosci. Biobehav. Rev. 2006, 30, 173–187. [Google Scholar] [CrossRef]
- Garces, M.; Finkel, L. Emotional Theory of Rationality. Front. Integr. Neurosci. 2019, 13, 11. [Google Scholar] [CrossRef]
- Stavros, M. Lehrbuch Der Psychodynamik: Die Funktion Der Dysfunktionalität Psychischer Störungen, 8th ed.; Vandenhoeck & Ruprecht: Göttingen, Germany, 2017. [Google Scholar]
- Panksepp, J. Behavior. Empathy and the Laws of Affect. Science 2011, 334, 1358–1359. [Google Scholar] [CrossRef]
- Seligman, M.E.; Steen, T.A.; Park, N.; Peterson, C. Positive Psychology Progress: Empirical Validation of Interventions. Am. Psychol. 2005, 60, 410–421. [Google Scholar] [CrossRef]
- Sedgwick, P. Michel Foucault: The Anti-History of Psychiatry. Psychol. Med. 1981, 11, 235–248. [Google Scholar] [CrossRef] [PubMed]
- Oglesby, M.E.; Short, N.A.; Albanese, B.J.; Portero, A.K.; Schmidt, N.B. Negative Interpretations of Distress-Related Information: A Novel Assessment Tool for Distress Tolerance. J. Anxiety Disord. 2018, 60, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Compas, B.E.; Jaser, S.S.; Bettis, A.H.; Watson, K.H.; Gruhn, M.A.; Dunbar, J.P.; Williams, E.; Thigpen, J.C. Coping, Emotion Regulation, and Psychopathology in Childhood and Adolescence: A Meta-Analysis and Narrative Review. Psychol. Bull. 2017, 143, 939–991. [Google Scholar] [CrossRef]
- Kernberg, O.F. An Ego Psychology Object Relations Theory of the Structure and Treatment of Pathologic Narcissism. An Overview. Psychiatr. Clin. N. Am. 1989, 12, 723–729. [Google Scholar] [CrossRef]
- Newen, A. The Embodied Self, the Pattern Theory of Self, and the Predictive Mind. Front. Psychol. 2018, 9, 2270. [Google Scholar] [CrossRef]
- Solms, M.; Panksepp, J. The “Id” Knows More than the “Ego” Admits: Neuropsychoanalytic and Primal Consciousness Perspectives on the Interface between Affective and Cognitive Neuroscience. Brain Sci. 2012, 2, 147–175. [Google Scholar] [CrossRef]
- Frings, C.; Wentura, D. Self-Priorization Processes in Action and Perception. J. Exp. Psychol. Hum. Percept. Perform. 2014, 40, 1737–1740. [Google Scholar] [CrossRef]
- Aldao, A.; Nolen-Hoeksema, S.; Schweizer, S. Emotion-Regulation Strategies across Psychopathology: A Meta-Analytic Review. Clin. Psychol. Rev. 2010, 30, 217–237. [Google Scholar] [CrossRef]
- Drubach, D.A. The Purpose and Neurobiology of Theory of Mind Functions. J. Relig. Health 2008, 47, 354–365. [Google Scholar] [CrossRef]
- Fonagy, P.; Allison, E. The Role of Mentalizing and Epistemic Trust in the Therapeutic Relationship. Psychotherapy 2014, 51, 372–380. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| M | SD | Min. | Max. | |
|---|---|---|---|---|
| BSI-18 GSI | 5.0 | 5.3 | 0 | 31 |
| BSI-18 Somatization | 1.1 | 1.8 | 0 | 12 |
| BSI-18 Depression | 2.1 | 2.7 | 0 | 17 |
| BSI-18 Anxiety | 1.8 | 2.1 | 0 | 11 |
| PSQI | 4.2 | 2.5 | 0 | 13 |
| Positive narratives | 3.7 | 1.6 | 0 | 6 |
| Negative narratives | 1.1 | 1.2 | 0 | 4 |
| Indifferent narratives | 1.2 | 1.1 | 0 | 5 |
| Positive emotions | 4.0 | 1.7 | 0 | 6 |
| Negative emotions | 1.7 | 1.6 | 0 | 6 |
| Indifferent emotions | 0.3 | 0.7 | 0 | 5 |
| Incongruence 1 | 1.5 | 1.2 | 0 | 5 |
| Certainty 2 | 82.6 | 12.2 | 25.7 | 100 |
| Mightiness 2 | 75.3 | 15.0 | 26.8 | 100 |
| Narrative | Emotion | Incongruence 1 | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Positive | Negative | Indifferent | Positive | Negative | Indifferent | Yes | No | |||||||||
| Item When I think …, I believe | n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % |
| …of my current particular situation… | 118 | 75.6 | 17 | 10.9 | 21 | 13.5 | 130 | 83.3 | 23 | 14.7 | 3 | 1.9 | 30 | 19.2 | 126 | 80.8 |
| …about my body… | 91 | 58.3 | 24 | 15.2 | 41 | 26.3 | 104 | 66.7 | 46 | 29.5 | 6 | 3.8 | 46 | 29.5 | 110 | 70.5 |
| …about my mental/emotional situation | 113 | 72.4 | 24 | 15.4 | 19 | 12.2 | 122 | 78.2 | 31 | 19.6 | 3 | 1.9 | 27 | 17.3 | 129 | 82.7 |
| ..of the coronavirus disease (COVID-19)… | 72 | 46.2 | 47 | 30.1 | 37 | 23.7 | 80 | 51.6 | 61 | 39.4 | 14 | 9.0 | 41 | 26.5 | 114 | 73.5 |
| … about the time in three months … | 86 | 55.1 | 36 | 23.1 | 34 | 21.8 | 88 | 56.4 | 53 | 34.0 | 15 | 9.6 | 49 | 31.4 | 107 | 68.6 |
| … about the time in six months … | 99 | 63.9 | 28 | 18.1 | 28 | 18.1 | 99 | 63.5 | 45 | 28.8 | 12 | 7.7 | 37 | 24.0 | 117 | 76.0 |
| Item When I think …, I believe | Certainty | Mightiness | ||||||
|---|---|---|---|---|---|---|---|---|
| M | SD | Min | Max | M | SD | Min | Max | |
| …of my current particular situation… | 85.2 | 14.9 | 19 | 100 | 76.1 | 16.9 | 25 | 100 |
| …about my body… | 84.5 | 17.3 | 5 | 100 | 73.3 | 22.6 | 0 | 100 |
| …about my mental/emotional situation | 84.7 | 15.8 | 23 | 100 | 78.0 | 19.3 | 23 | 100 |
| ..of the coronavirus disease (COVID-19)… | 85.6 | 15.4 | 23 | 100 | 76.3 | 18.9 | 14 | 100 |
| … about the time in three months … | 79.6 | 17.8 | 18 | 100 | 74.5 | 18.4 | 25 | 100 |
| … about the time in six months … | 75.7 | 19.3 | 15 | 100 | 73.5 | 20.2 | 15 | 100 |
| BSI-18 GSI | BSI-18 Soma | BSI-18 Depr | BSI-18 Anxi | PSQI6 | |
|---|---|---|---|---|---|
| Positive narratives | −0.24 * | −0.17 * | −0.28 *** | −0.10 | −0.10 |
| Negative narratives | 0.29 *** | 0.17 * | 0.36 *** | 0.13 | 0.14 |
| Indifferent narratives | 0.04 | 0.04 | 0.04 | 0.01 | −0.03 |
| Positive emotions | −0.36 *** | −0.29 *** | −0.40 *** | −0.16 | −0.17 * |
| Negative emotions | 0.39 *** | 0.23 ** | 0.45 *** | 0.21 ** | 0.16 |
| Indifferent emotions | −0.02 | 0.17 * | −0.07 | −0.10 | 0.05 |
| Incongruence 1 | 0.08 | 0.14 | 0.04 | 0.03 | 0.02 |
| Certainty | −0.13 | −0.07 | −0.11 | −0.13 | −0.14 |
| Mightiness | −0.06 | −0.03 | −0.02 | −0.09 | −0.04 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wagner-Skacel, J.; Tietz, S.; Fleischmann, E.; Fellendorf, F.T.; Bengesser, S.A.; Lenger, M.; Reininghaus, E.Z.; Mairinger, M.; Körner, C.; Pieh, C.; et al. Believing Processes during the COVID-19 Pandemic: A Qualitative Analysis. Int. J. Environ. Res. Public Health 2022, 19, 11997. https://doi.org/10.3390/ijerph191911997
Wagner-Skacel J, Tietz S, Fleischmann E, Fellendorf FT, Bengesser SA, Lenger M, Reininghaus EZ, Mairinger M, Körner C, Pieh C, et al. Believing Processes during the COVID-19 Pandemic: A Qualitative Analysis. International Journal of Environmental Research and Public Health. 2022; 19(19):11997. https://doi.org/10.3390/ijerph191911997
Chicago/Turabian StyleWagner-Skacel, Jolana, Sophie Tietz, Eva Fleischmann, Frederike T. Fellendorf, Susanne A. Bengesser, Melanie Lenger, Eva Z. Reininghaus, Marco Mairinger, Christof Körner, Christoph Pieh, and et al. 2022. "Believing Processes during the COVID-19 Pandemic: A Qualitative Analysis" International Journal of Environmental Research and Public Health 19, no. 19: 11997. https://doi.org/10.3390/ijerph191911997