
COVID-19 Impact on Public Dental Healthcare in Bosnia and Herzegovina: Current Situation and Ongoing Perspectives
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
- -
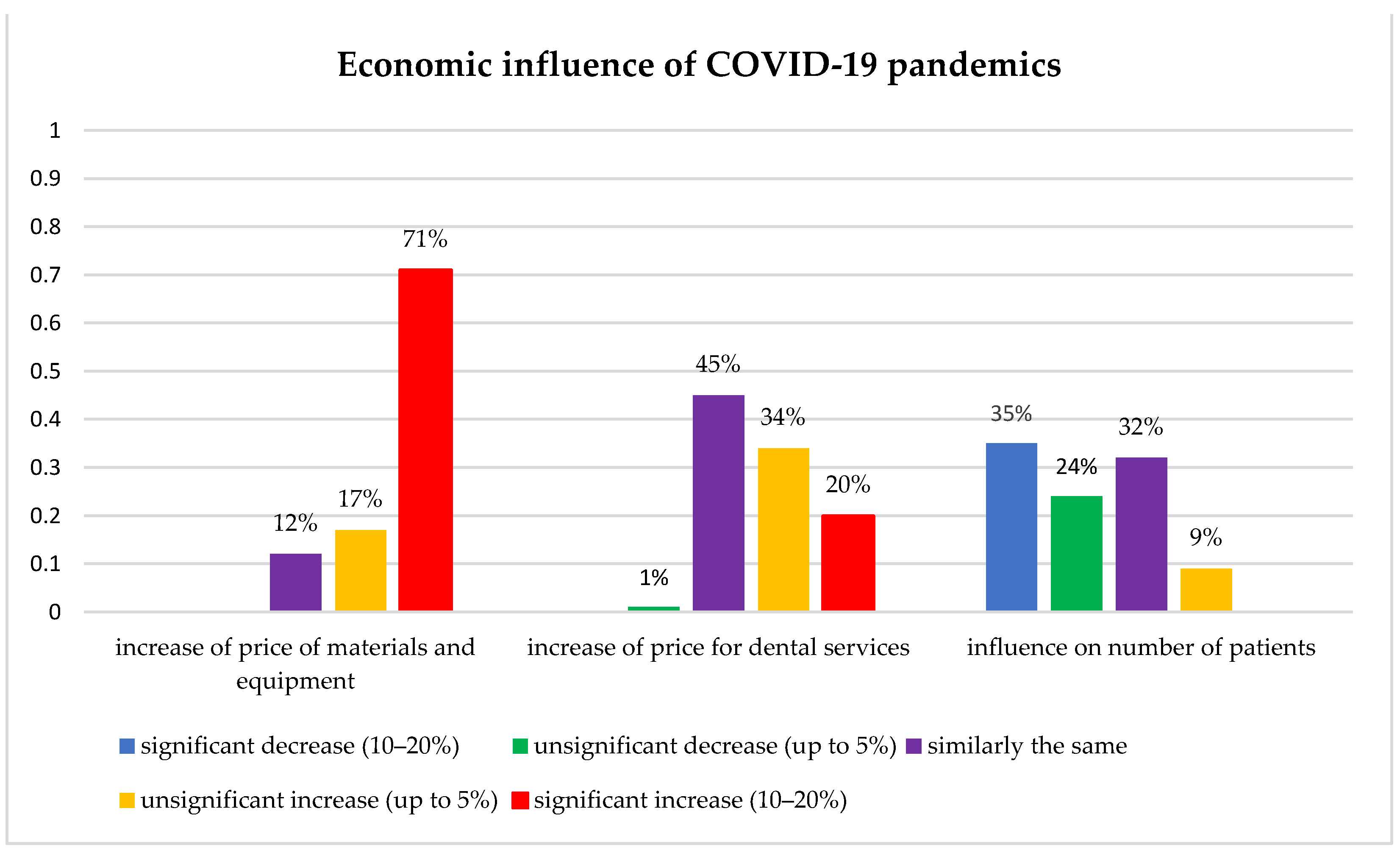
- Demographic characteristics of the study sample, results regarding participants’ COVID-19 status, level and usage of prescribed measures and PPE, vaccination status, and attitudes about the economical impact of COVID-19, were analyzed by their total and relative counts and are presented in tables and charts;
- -
- Significant differences between obtained study results were determined using the Chi-square test.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- WHO. COVID-19 Dashboard; World Health Organization: Geneva, Switzerland, 2020. Available online: https://covid19.who.int/ (accessed on 27 June 2022).
- WHO Dashboard of COVID-19 Related Recommendations. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 27 June 2022).
- Giwa, A.L.; Desai, A.; Duca, A. Novel 2019 coronavirus SARS-CoV-2 (COVID-19): An overview for emergency clinicians. Pediatr. Emerg. Med. Pract. 2020, 17, 1–24. [Google Scholar] [PubMed]
- Megna, R. First month of the epidemic caused by COVID-19 in Italy: Current status and real-time outbreak development forecast. Glob. Health Res. Policy 2020, 5, 43. [Google Scholar] [CrossRef] [PubMed]
- Bezzini, D.; Schiavetti, I.; Manacorda, T.; Franzone, G.; Battaglia, M.A. First Wave of COVID-19 Pandemic in Italy: Data and Evidence. Adv. Exp. Med. Biol. 2021, 1353, 91–113. [Google Scholar] [CrossRef] [PubMed]
- Arabi, Y.M.; Azoulay, E.; Al-Dorzi, H.M.; Phua, J.; Salluh, J.; Binnie, A.; Hodgson, C.; Angus, D.C.; Cecconi, M.; Du, B.; et al. How the COVID-19 pandemic will change the future of critical care. Intensive Care Med. 2021, 47, 282–291. [Google Scholar] [CrossRef] [PubMed]
- Moynihan, R.; Sanders, S.; Michaleff, Z.A.; Scott, A.M.; Clark, J.; To, E.J.; Jones, M.; Kitchener, E.; Fox, M.; Johansson, M.; et al. Impact of COVID-19 pandemic on utilisation of healthcare services: A systematic review. BMJ Open 2021, 11, e045343. [Google Scholar] [CrossRef] [PubMed]
- Butt, R.T.; Janjua, O.S.; Qureshi, S.M.; Shaikh, M.S.; Guerrero-Gironés, J.; Rodríguez-Lozano, F.J.; Zafar, M.S. Dental Healthcare Amid the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 11008. [Google Scholar] [CrossRef] [PubMed]
- Chamorro, C.; Carreras-Presas, C.M.; Sanz-Marchena, A.; A Rodríguez-Fernández, M.; Suárez-Quintanilla, J.M.; Rivas-Mundiña, B.; Suárez-Quintanilla, J.; Pérez-Sayáns, M. Assessment of the Economic and Health-Care Impact of COVID-19 (SARS-CoV-2) on Public and Private Dental Surgeries in Spain: A Pilot Study. Int. J. Environ. Res. Public Health 2020, 17, 5139. [Google Scholar] [CrossRef]
- Ahmed, M.A.; Jouhar, R.; Ahmed, N.; Adnan, S.; Aftab, M.; Zafar, M.S.; Khurshid, Z. Fear and Practice Modifications among Dentists to Combat Novel Coronavirus Disease (COVID-19) Outbreak. Int. J. Environ. Res. Public Health 2020, 17, 2821. [Google Scholar] [CrossRef]
- Ministry of Civil Affairs of Bosnia and Herzegovina. Bosnia and Herzegovina: Council of Ministers of Bosnia and Herzegovina. Available online: http://mcp.gov.ba/Publication/Category/projekti?category=7&lang=bs (accessed on 1 August 2022).
- Institute for Public Health FB&H. Sarajevo: Federation of Bosnia and Herzegovina. Available online: https://www.covid-19.ba/ (accessed on 27 June 2022).
- Institute for Public Health of Republic of Srpska. Banja Luka: Republic of Srpska. Available online: https://www.phi.rs.ba/index.php?view=kategorija&id=45&lang=SR-CIR (accessed on 27 June 2022).
- Villani, F.A.; Aiuto, R.; Paglia, L.; Re, D. COVID-19 and Dentistry: Prevention in Dental Practice, a Literature Review. Int. J. Environ. Res. Public Health 2020, 17, 4609. [Google Scholar] [CrossRef]
- Induri, S.; Chun, Y.; Chun, J.; Fleisher, K.; Glickman, R.; Xu, F.; Ioannidou, E.; Li, X.; Saxena, D. Protective Measures against COVID-19: Dental Practice and Infection Control. Healthcare 2021, 9, 679. [Google Scholar] [CrossRef]
- Abrar, E.; Abduljabbar, A.S.; Naseem, M.; Panhwar, M.; Vohra, F.; Abduljabbar, T. Evaluating the Influence of COVID-19 Among Dental Practitioners After Lockdown. INQUIRY J. Health Care Organ. Provis. Financ. 2021, 58, 00469580211060753. [Google Scholar] [CrossRef] [PubMed]
- Arapović, J.; Sulaver, Ž.; Rajič, B.; Pilav, A. The 2019 measles epidemic in Bosnia and Herzegovina: What is wrong with the mandatory vaccination program? Bosn. J. Basic Med. Sci. 2019, 19, 210–212. [Google Scholar] [CrossRef] [PubMed]
- Campus, G.; Diaz-Betancourt, M.; Cagetti, M.; Carvalho, J.; Carvalho, T.; Cortés-Martinicorena, J.; Deschner, J.; Douglas, G.; Giacaman, R.; Machiulskiene, V.; et al. Study Protocol for an Online Questionnaire Survey on Symptoms/Signs, Protective Measures, Level of Awareness and Perception Regarding COVID-19 Outbreak among Dentists. A Global Survey. Int. J. Environ. Res. Public Health 2020, 17, 5598. [Google Scholar] [CrossRef] [PubMed]
- COVIDental Collaboration Group. The COVID-19 pandemic and its global effects on dental practice. An International survey. J. Dent. 2021, 114, 103749. [Google Scholar] [CrossRef]
- Cagetti, M.G.; Cairoli, J.L.; Senna, A.; Campus, G. COVID-19 Outbreak in North Italy: An Overview on Dentistry. A Questionnaire Survey. Int. J. Environ. Res. Public Health 2020, 17, 3835. [Google Scholar] [CrossRef] [PubMed]
- Estrich, C.G.; Mikkelsen, M.; Morrissey, R.; Geisinger, M.L.; Ioannidou, E.; Vujicic, M.; Araujo, M.W.B. Estimating COVID-19 prevalence and infection control practices among US dentists. J. Am. Dent. Assoc. 2020, 151, 815–824. [Google Scholar] [CrossRef] [PubMed]
- Alencar, C.M.; Silva, A.M.; Jural, L.A.; Magno, M.B.; Campos, E.A.; Silva, C.M.; Coqueiro, R.D.S.; Pithon, M.M.; Maia, L.C. Factors associated with depression, anxiety and stress among dentists during the COVID-19 pandemic. Braz. Oral Res. 2021, 35, e084. [Google Scholar] [CrossRef]
- Salehiniya, H.; Abbaszadeh, H. Prevalence of corona-associated anxiety and mental health disorder among dentists during the COVID-19 pandemic. Neuropsychopharmacol. Rep. 2021, 41, 223–229. [Google Scholar] [CrossRef]
- Carvalho, J.C.; Declerck, D.; Jacquet, W.; Bottenberg, P. Dentist Related Factors Associated with Implementation of COVID-19 Protective Measures: A National Survey. Int. J. Environ. Res. Public Health 2021, 18, 8381. [Google Scholar] [CrossRef]
- Gopakumar, R.; Mahesh, J.; Alexander, B.; Arya, K.S.; John, S.; Kumbla, S. Acceptance of COVID-19 Vaccine among Dental Professionals: A Cross-Sectional Study among Practitioners, Residents, and Students. J. Pharm. Bioallied Sci. 2021, 13, S985–S988. [Google Scholar] [CrossRef]
- Lin, G.S.S.; Lee, H.Y.; Leong, J.Z.; Sulaiman, M.M.; Loo, W.F.; Tan, W.W. COVID-19 vaccination acceptance among dental students and dental practitioners: A systematic review and meta-analysis. PLoS ONE 2022, 17, e0267354. [Google Scholar] [CrossRef] [PubMed]
- Raja, S.M.; Osman, M.E.; Musa, A.O.; Hussien, A.A.; Yusuf, K. COVID-19 vaccine acceptance, hesitancy, and associated factors among medical students in Sudan. PLoS ONE 2022, 17, e0266670. [Google Scholar] [CrossRef] [PubMed]
- Riad, A.; Abdulqader, H.; Morgado, M.; Domnori, S.; Koščík, M.; Mendes, J.J.; Klugar, M.; Kateeb, E.; Iads-Score, O.B.O. Global Prevalence and Drivers of Dental Students’ COVID-19 Vaccine Hesitancy. Vaccines 2021, 9, 566. [Google Scholar] [CrossRef] [PubMed]
- Witton, R.; Plessas, A.; Wheat, H.; Baines, R.; Delgado, M.B.; Mills, I.; Paisi, M. The future of dentistry post-COVID-19: Perspectives from Urgent Dental Care centre staff in England. Br. Dent. J. 2021, 1–5. [Google Scholar] [CrossRef]
- Moharrami, M.; Bohlouli, B.; Amin, M. Frequency and pattern of outpatient dental visits during the COVID-19 pandemic at hospital and community clinics. J. Am. Dent. Assoc. 2022, 153, 354–364.e1. [Google Scholar] [CrossRef]
- Andrade, C. The Limitations of Online Surveys. Indian J. Psychol. Med. 2020, 42, 575–576. [Google Scholar] [CrossRef]
- Singh, S.; Sagar, R. A critical look at online survey or questionnaire-based research studies during COVID-19. Asian J. Psychiatry 2021, 65, 102850. [Google Scholar] [CrossRef]
- Wu, M.-J.; Zhao, K.; Fils-Aime, F. Response rates of online surveys in published research: A meta-analysis. Comput. Hum. Behav. Rep. 2022, 7, 100206. [Google Scholar] [CrossRef]
- Bahans, C.; Leymarie, S.; Malauzat, D.; Girard, M.; Demiot, C. Ethical considerations of the dynamics of clinical trials in an epidemic context: Studies on COVID-19. Ethics Med. Public Health 2021, 16, 100621. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Descriptive Characteristics | ||||
| Number of Surveyed Dentists | 2020 Sample | 2022 Sample | ||
| Frequency | % | Frequency | % | |
| Number of surveyed dentists | 2233 | 2233 | ||
| Number of fulfilled forms | 213 | 9.54 | 136 | 6.09 |
| Total | 213 | 9.54 | 136 | 6.09 |
| Gender of study participants | 2020 sample | 2022 sample | ||
| Frequency | % | Frequency | % | |
| Male | 64 | 30.00 | 31 | 22.80 |
| Female | 149 | 70.00 | 105 | 77.20 |
| Total | 213 | 100.00 | 136 | 100.00 |
| Age of study participants | 2020 sample | 2022 sample | ||
| Mean | Std. Deviation | Mean | Std. Deviation | |
| 38.2911 | 8.07043 | 41.0735 | 8.16372 | |
| Demographic characteristics | ||||
| Workplace of study participants | 2020 sample | 2022 sample | ||
| Frequency | % | Frequency | % | |
| Federation of B&H | 126 | 59.20 | 82 | 60.30 |
| Republic of Srpska | 84 | 39.40 | 54 | 39.70 |
| Brčko district | 3 | 1.40 | ― | ― |
| Total | 213 | 100.00 | 136 | 100.00 |
| Working status of study participants | 2020 sample | 2022 sample | ||
| Frequency | % | Frequency | % | |
| Private practice (owner) | 58 | 27.20 | 44 | 32.40 |
| Private practice (salaried) | 65 | 30.50 | 38 | 27.90 |
| Private and public sector | 11 | 5.20 | 4 | 2.90 |
| Public sector | 73 | 34.30 | 42 | 30.90 |
| Academic/research | 6 | 2.80 | 8 | 5.90 |
| Total | 213 | 100.00 | 136 | 100.00 |
| Dentistry field of study participants | 2020 sample | 2022 sample | ||
| Frequency | % | Frequency | % | |
| General dentist | 139 | 65.30 | 77 | 56.60 |
| Dental specialist | 74 | 34.70 | 59 | 43.40 |
| Total | 213 | 100.00 | 136 | 100.00 |
| Confirmed COVID-19 Cases | |||
| 2020 Sample | 2022 Sample | ||
| Frequency | % | Frequency | % |
| 1 | 0.47 | 88 | 64.70 |
| Report of suffering COVID-19 referable symptoms | |||
| 2020 sample | 2022 sample | ||
| Frequency | % | Frequency | % |
| 29 | 13.61 | 88 | 64.70 |
| COVID-19 Symptom | Chi-Square | p | COVID-19 Symptom | Chi- Square | p |
|---|---|---|---|---|---|
| Fever | 92.327 | p ≤ 0.0005 | Headaches | 31.121 | p ≤ 0.0005 |
| Cough | 33.161 | p ≤ 0.0005 | Fatigue | 40.474 | p ≤ 0.0005 |
| Sore throat | 18.664 | p ≤ 0.0005 | Muscle pain | 79.733 | p ≤ 0.0005 |
| Running nose | 5.403 | p = 0.020 | Diarrhea | 12.884 | p ≤ 0.0005 |
| Nasal congestion | 22.851 | p ≤ 0.0005 | Loss of smell | 70.226 | p ≤ 0.0005 |
| Difficult breathing | 10.568 | p = 0.001 | Loss of taste | 50.626 | p ≤ 0.0005 |
| Status | Frequency | % | Dose | Frequency | % |
| Not vaccinated | 19 | 14.00 | 1st dose | 2 | 1.50 |
| Vaccinated | 117 | 86.00 | 2nd dose | 59 | 43.40 |
| Total | 136 | 100.00 | 3rd dose | 56 | 41.20 |
| Reasons not to take the COVID-19 vaccine | Frequency | % | |||
| Personal medical reasons | 8 | 5.90 | |||
| Disbelief in COVID-19 vaccine efficacy | 6 | 4.40 | |||
| General disbelief in vaccination | 1 | 0.70 | |||
| No reasons for COVID-19 vaccination | 4 | 2.90 | |||
| Differences within the 2020 Sample | Differences between the 2020 and 2022 Sample | ||||
|---|---|---|---|---|---|
| Measure | Chi-Square | p | Measure | Chi-Square | p |
| Phone triage | 86.014 | p ≤ 0.0005 | Ventilation of the waiting room | 7.008 | p = 0.008 |
| No overcrowding in the waiting room | 11.093 | p = 0.001 | Mouth rinsing of patients with H2O2 | 13.283 | p ≤ 0.0005 |
| Postponement of treatment | 29.259 | p ≤ 0.0005 | Mouth rinsing of patients with povidone-iodine | 7.769 | p = 0.005 |
| Measuring the body temperature of dental team members | 6.568 | p = 0.010 | Surface disinfection with NaOCl | 5.121 | p = 0.024 |
| Sanitizing patient’s hands | 4.264 | p = 0.039 | Surface disinfection with active ingredients solutions | 15.902 | p ≤ 0.0005 |
| Space distance between patients | 8.835 | p = 0.003 | Hand disinfection of dentists | 27.409 | p ≤ 0.0005 |
| Not using of aerosol producing handpieces | 44.558 | p ≤ 0.0005 | Disposal of single and disinfection of multiple-use equipment | 37.004 | p ≤ 0.0005 |
| Not using of aerosol producing handpieces | 41.980 | p ≤ 0.0005 | |||
| Differences within the 2020 Sample | Differences between 2020 and 2022 Sample | ||||
|---|---|---|---|---|---|
| PPE | Chi-Square | p | PPE | Chi-Square | p |
| FFP2/N95 mask | 4.197 | p = 0.040 | FFP2/N95 mask | 11.490 | p = 0.001 |
| Water repellent disposable gown | 9.197 | p = 0.002 | Visor | 23.632 | p ≤ 0.0005 |
| Goggles | 3.996 | p = 0.046 | Breathable disposable gown | 15.197 | p ≤ 0.0005 |
| Prolonged use of PPE | 10.547 | p = 0.001 | Water repellent disposable gown | 13.328 | p ≤ 0.0005 |
| Prolonged use of PPE | 39.918 | p ≤ 0.0005 | |||
| Protective caps single use | 14.399 | p ≤ 0.0005 | |||
| Professional Risk of Infection for Dentists | 2020 Sample | 2022 Sample | ||
| Frequency | % | Frequency | % | |
| Very unlikely | 4 | 1.90 | 6 | 4.40 |
| Unlikely | 7 | 3.30 | 20 | 14.70 |
| Likely | 64 | 30.00 | 58 | 42.60 |
| Very likely | 138 | 64.80 | 52 | 38.20 |
| Total | 213 | 100.00 | 136 | 100.0 |
| Possibility of avoiding infection | 2020 sample | 2022 sample | ||
| Frequency | % | Frequency | % | |
| Totally sure | 5 | 2.30 | 3 | 2.20 |
| Pretty sure | 25 | 11.70 | 15 | 11.00 |
| Pretty unsure | 118 | 55.40 | 81 | 59.60 |
| Totally unsure | 65 | 30.50 | 37 | 27.20 |
| Total | 213 | 100.00 | 136 | 100.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bajrić, E.; Zukanović, A.; Marković, N.; Arslanagić, A.; Huseinbegović, A.; Selimović-Dragaš, M.; Kobašlija, S.; Popovac, A.; Marković, D. COVID-19 Impact on Public Dental Healthcare in Bosnia and Herzegovina: Current Situation and Ongoing Perspectives. Int. J. Environ. Res. Public Health 2022, 19, 11816. https://doi.org/10.3390/ijerph191811816
Bajrić E, Zukanović A, Marković N, Arslanagić A, Huseinbegović A, Selimović-Dragaš M, Kobašlija S, Popovac A, Marković D. COVID-19 Impact on Public Dental Healthcare in Bosnia and Herzegovina: Current Situation and Ongoing Perspectives. International Journal of Environmental Research and Public Health. 2022; 19(18):11816. https://doi.org/10.3390/ijerph191811816
Chicago/Turabian StyleBajrić, Elmedin, Amila Zukanović, Nina Marković, Amra Arslanagić, Amina Huseinbegović, Mediha Selimović-Dragaš, Sedin Kobašlija, Aleksandra Popovac, and Dejan Marković. 2022. "COVID-19 Impact on Public Dental Healthcare in Bosnia and Herzegovina: Current Situation and Ongoing Perspectives" International Journal of Environmental Research and Public Health 19, no. 18: 11816. https://doi.org/10.3390/ijerph191811816