

Impact of Different Resistance Training Protocols on Balance, Quality of Life and Physical Activity Level of Older Women

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Design
2.2. Sample and Ethical Procedures
2.2.1. Resistance Training Protocol
2.2.2. Anthropometric Measures and Balance
2.2.3. Level of Physical Activity and Quality of Life
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Population Division, Department of Economic and Social Affaires, United Nations. World Population Prospects: The 2017 Revision. 2017. Available online: https://www.un.org/development/desa/publications/world-population-prospects-the-2017-revision.html (accessed on 20 July 2022).
- Leitão, L.; Marocolo, M.; de Souza, H.L.R.; Arriel, R.A.; Vieira, J.G.; Mazini, M.; Louro, H.; Pereira, A. Can Exercise Help Regulate Blood Pressure and Improve Functional Capacity of Older Women with Hypertension against the Deleterious Effects of Physical Inactivity? Int. J. Environ. Res. Public Health 2021, 18, 9117. [Google Scholar] [CrossRef]
- Borde, R.; Hortobágyi, T.; Granacher, U. Dose-Response Relationships of Resistance Training in Healthy Old Adults: A Systematic Review and Meta-Analysis. Sports Med. 2015, 45, 1693–1720. [Google Scholar] [CrossRef] [PubMed]
- Sampaio, A.; Marques-Aleixo, I.; Seabra, A.; Mota, J.; Marques, E.; Carvalho, J. Physical fitness in institutionalized older adults with dementia: Association with cognition, functional capacity and quality of life. Aging Clin. Exp. Res. 2020, 32, 2329–2338. [Google Scholar] [CrossRef]
- Lepsy, E.; Radwańska, E.; Żurek, G.; Żurek, A.; Kaczorowska, A.; Radajewska, A.; Kołcz, A. Association of physical fitness with quality of life in community-dwelling older adults aged 80 and over in Poland: A cross-sectional study. BMC Geriatr. 2021, 21, 491. [Google Scholar] [CrossRef]
- College, A.; Sports, M.; Chodzko-Zajko, W.J.; Proctor, D.N.; Singh, M.A.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S. American College of Sports Medicine Position Stand. Exercise and Physical Activity for Older Adults. Med. Sci. Sports Exerc. 2009, 41, 1510–1530. [Google Scholar]
- Fragala, M.S.; Cadore, E.L.; Dorgo, S.; Izquierdo, M.; Kraemer, W.J.; Peterson, M.D.; Ryan, E.D. Resistance Training for Older Adults: Position Statement from the National Strength and Conditioning Association. J. Strength Cond. Res. 2019, 33, 2019–2052. [Google Scholar] [CrossRef] [PubMed]
- Leitão, L.; Marocolo, M.; de Souza, H.L.R.; Arriel, R.A.; Campos, Y.; Mazini, M.; Junior, R.P.; Figueiredo, T.; Louro, H.; Pereira, A. Three-Month vs. One-Year Detraining Effects after Multicomponent Exercise Program in Hypertensive Older Women. Int. J. Environ. Res. Public Health 2022, 19, 2871. [Google Scholar] [CrossRef] [PubMed]
- Leitão, L.; Marocolo, M.; de Souza, H.L.R.; Arriel, R.A.; Vieira, J.G.; Mazini, M.; Figueiredo, T.; Louro, H.; Pereira, A. Multicomponent Exercise Program for Improvement of Functional Capacity and Lipidic Profile of Older Women with High Cholesterol and High Triglycerides. Int. J. Environ. Res. Public Health 2021, 18, 10731. [Google Scholar] [CrossRef] [PubMed]
- Filho, M.M.; Venturini, G.R.; Moreira, O.C.; Leitão, L.; Mira, P.A.C.; de Castro, J.B.P.; Aidar, F.J.; Novaes, J.D.S.; Vianna, J.M.; Ferreira, M.E.C. Effects of Different Types of Resistance Training and Detraining on Functional Capacity, Muscle Strength, and Power in Older Women: A Randomized Controlled Study. J. Strength Cond. Res. 2022, 36, 984–990. [Google Scholar] [CrossRef]
- Hart, P.D.; Buck, D.J. The effect of resistance training on health-related quality of life in older adults: Systematic review and meta-analysis. Health Promot. Perspect. 2019, 9, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Toselli, S.; Campa, F.; Spiga, F.; Grigoletto, A.; Simonelli, I.; Gualdi-Russo, E. The association between body composition and quality of life among elderly Italians. Endocrine 2020, 68, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Puciato, D.; Borysiuk, Z.; Rozpara, M. Quality of life and physical activity in an older working-age population. Clin. Interv. Aging 2017, 12, 1627–1634. [Google Scholar] [CrossRef] [PubMed]
- Inaba, Y.; Obuchi, S.; Arai, T.; Satake, K.; Takahira, N. The long-term effects of progressive resistance training on health-related quality in older adults. J. Physiol. Anthropol. 2008, 27, 57–61. [Google Scholar] [CrossRef]
- Pucci, G.; Reis, R.S.; Rech, C.R.; Hallal, P.C. Quality of life and physical activity among adults: Population-based study in Brazilian adults. Qual. Life Res. 2012, 21, 1537–1543. [Google Scholar] [CrossRef] [PubMed]
- Haraldstad, K.; Rohde, G.; Stea, T.H.; Lohne-Seiler, H.; Hetlelid, K.; Paulsen, G.; Berntsen, S. Changes in health-related quality of life in elderly men after 12 weeks of strength training. Eur. Rev. Aging Phys. Act. 2017, 14, 8. [Google Scholar] [CrossRef]
- Foster, C.; Boullosa, D.; McGuigan, M.; Fusco, A.; Cortis, C.; Arney, B.E.; Orton, B.; Dodge, C.; Jaime, S.; Radtke, K.; et al. 25 Years of Session Rating of Perceived Exertion: Historical Perspective and Development. Int. J. Sports Physiol. Perform. 2021, 16, 612–621. [Google Scholar] [CrossRef] [PubMed]
- Sayers, S.P.; Gibson, K. High-Speed Power Training in Older Adults. J. Strength Cond. Res. 2014, 28, 616–621. [Google Scholar] [CrossRef] [PubMed]
- Kennis, E.; Verschueren, S.M.; Bogaerts, A.; Van Roie, E.; Boonen, S.; Delecluse, C. Long-Term Impact of Strength Training on Muscle Strength Characteristics in Older Adults. Arch. Phys. Med. Rehabil. 2013, 94, 2054–2060. [Google Scholar] [CrossRef] [PubMed]
- Patti, A.; Zangla, D.; Sahin, F.N.; Cataldi, S.; Lavanco, G.; Palma, A.; Fischietti, F. Physical exercise and prevention of falls. Effects of a Pilates training method compared with a general physical activity program. Medicine 2021, 100, e25289. [Google Scholar] [CrossRef]
- Jeon, Y.-J.; Kim, G.-M. Comparison of the Berg Balance Scale and Fullerton Advanced Balance Scale to predict falls in community-dwelling adults. J. Phys. Ther. Sci. 2017, 29, 232–234. [Google Scholar] [CrossRef] [PubMed]
- Gouveia, R.; Maia, J.A.; Beunen, G.P.; Blimkie, C.J.; Fena, E.M.; Freitas, D.L. Functional Fitness and Physical Activity of Portuguese Community-Residing Older Adults. J. Aging Phys. Act. 2013, 21, 1–19. [Google Scholar] [CrossRef]
- Lucas-Carrasco, R.; Laidlaw, K.; Power, M.J. Suitability of the WHOQOL-BREF and WHOQOL-OLD for Spanish older adults. Aging Ment. Health 2011, 15, 595–604. [Google Scholar] [CrossRef] [PubMed]
- Zouita, S.; Zouhal, H.; Ferchichi, H.; Paillard, T.; Dziri, C.; Hackney, A.C.; Laher, I.; Granacher, U.; Zouita, A.B.M. Effects of Combined Balance and Strength Training on Measures of Balance and Muscle Strength in Older Women With a History of Falls. Front. Physiol. 2020, 11, 619016. [Google Scholar] [CrossRef] [PubMed]
- Haider, S.; Luger, E.; Kapan, A.; Titze, S.; Lackinger, C.; Schindler, K.E.; Dorner, T.E. Associations between daily physical activity, handgrip strength, muscle mass, physical performance and quality of life in prefrail and frail community-dwelling older adults. Qual. Life Res. 2016, 25, 3129–3138. [Google Scholar] [CrossRef] [PubMed]
- Scarabottolo, C.C.; Tebar, W.R.; Gobbo, L.A.; Ohara, D.; Ferreira, A.D.; Canhin, D.D.S.; Christofaro, D.G.D. Analysis of different domains of physical activity with health-related quality of life in adults: 2-year cohort. Health Qual. Life Outcomes 2022, 20, 71. [Google Scholar] [CrossRef] [PubMed]
- Giuliano, C.; Karahalios, A.; Neil, C.; Allen, J.; Levinger, I. The effects of resistance training on muscle strength, quality of life and aerobic capacity in patients with chronic heart failure—A meta-analysis. Int. J. Cardiol. 2017, 227, 413–423. [Google Scholar] [CrossRef]
- White, R.L.; Bennie, J.; Abbott, G.; Teychenne, M. Work-related physical activity and psychological distress among women in different occupations: A cross-sectional study. BMC Public Health 2020, 20, 1007. [Google Scholar] [CrossRef] [PubMed]
- Saint-Maurice, P.F.; Coughlan, D.; Kelly, S.; Keadle, S.; Cook, M.B.; Carlson, S.A.; Fulton, J.E.; Matthews, C.E. Association of Leisure-Time Physical Activity Across the Adult Life Course With All-Cause and Cause-Specific Mortality. JAMA Netw. Open 2019, 2, e190355. [Google Scholar] [CrossRef] [PubMed]
- White, R.L.; Babic, M.J.; Parker, P.D.; Lubans, D.R.; Astell-Burt, T.; Lonsdale, C. Domain-Specific Physical Activity and Mental Health: A Meta-analysis. Am. J. Prev. Med. 2017, 52, 653–666. [Google Scholar] [CrossRef]
- Meneguci, J.; Sasaki, J.; Santos, A.; Scatena, L.M.; Damião, R. Sitting Time and Quality of Life in Older Adults: A Population-Based Study. J. Phys. Act. Health 2015, 12, 1513–1519. [Google Scholar] [CrossRef] [PubMed]
- Wong, F.Y.; Yang, L.; Yuen, J.W.M.; Chang, K.K.P.; Wong, F.K.Y. Assessing quality of life using WHOQOL-BREF: A cross-sectional study on the association between quality of life and neighborhood environmental satisfaction, and the mediating effect of health-related behaviors. BMC Public Health 2018, 18, 1113. [Google Scholar] [CrossRef] [Green Version]
- Crocker, T.F.; Brown, L.; Clegg, A.; Farley, K.; Franklin, M.; Simpkins, S.; Young, J. Quality of life is substantially worse for community-dwelling older people living with frailty: Systematic review and meta-analysis. Qual. Life Res. 2019, 28, 2041–2056. [Google Scholar] [CrossRef]
- Borges-Machado, F.; Barros, D.; Teixeira, L.; Ribeiro, O.; Carvalho, J. Health-related physical indicators and self-rated quality of life in older adults with neurocognitive disorder. Qual. Life Res. 2021, 30, 2255–2264. [Google Scholar] [CrossRef]
- Kwon, J.; Yoshida, Y.; Yoshida, H.; Kim, H.; Suzuki, T.; Lee, Y. Effects of a Combined Physical Training and Nutrition Intervention on Physical Performance and Health-Related Quality of Life in Prefrail Older Women Living in the Community: A Randomized Controlled Trial. J. Am. Med. Dir. Assoc. 2015, 16, 263.e1–263.e8. [Google Scholar] [CrossRef]
- Paw, M.J.; de Jong, N.; Schouten, E.; van Staveren, W.A.; Kok, F.J. Physical exercise or micronutrient supplementation for the wellbeing of the frail elderly? A randomized controlled trial. Br. J. Sports Med. 2002, 36, 126–131. [Google Scholar] [CrossRef]
- Eime, R.; Harvey, J.; Payne, W. Dose-response of women’s health-related quality of life (HRQoL) and life satisfaction to physical activity. J. Phys. Act. Health 2014, 11, 330–338. [Google Scholar] [CrossRef]
- Gil-Lacruz, M.; Gil-Lacruz, A.I.; Domingo-Torrecilla, P.; Canñete-Lairla, M.A. Health-Related Quality of Life and Physical Activity in a Community Setting. Int. J. Environ. Res. Public Health 2021, 18, 7301. [Google Scholar] [CrossRef]
- Kisvetrová, H.; Herzig, R.; Bretšnajdrová, M.; Tomanová, J.; Langová, K.; Školoudík, D. Predictors of quality of life and attitude to ageing in older adults with and without dementia. Aging Ment. Health 2021, 25, 535–542. [Google Scholar] [CrossRef]
- Van Leeuwen, K.M.; Van Loon, M.S.; Van Nes, F.A.; Bosmans, J.; De Vet, H.C.W.; Ket, J.C.; Widdershoven, G.A.M.; Ostelo, R. What does quality of life mean to older adults? A thematic synthesis. PLoS ONE 2019, 14, e0213263. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Variable | SET (n = 20) | PWT (n = 19) | TRT (n = 17) | AST (n = 20) | CG (n = 19) |
|---|---|---|---|---|---|
| Age (years) | 64.1 ± 4.10 | 66.21 ± 3.10 | 67.21 ± 5.10 | 67.12 ± 5.81 | 69.03 ± 3.42 |
| Height (cm) | 154.38 ± 5.24 | 158.21 ± 4.55 | 154.79 ± 7.55 | 157.86 ± 5.64 | 156.24 ± 6.30 |
| Body weight (kg) | 69.10 ± 14.8 | 71.90 ± 16.03 | 61.40 ± 10.51 | 75.61 ± 67.2 | 67.21 ± 11.46 |
| BMI (kg/m2) | 29.03 ± 5.53 | 28.73 ± 5.74 | 25.74 ± 4.64 | 30.72 ± 5.74 | 27.42 ± 5.41 |
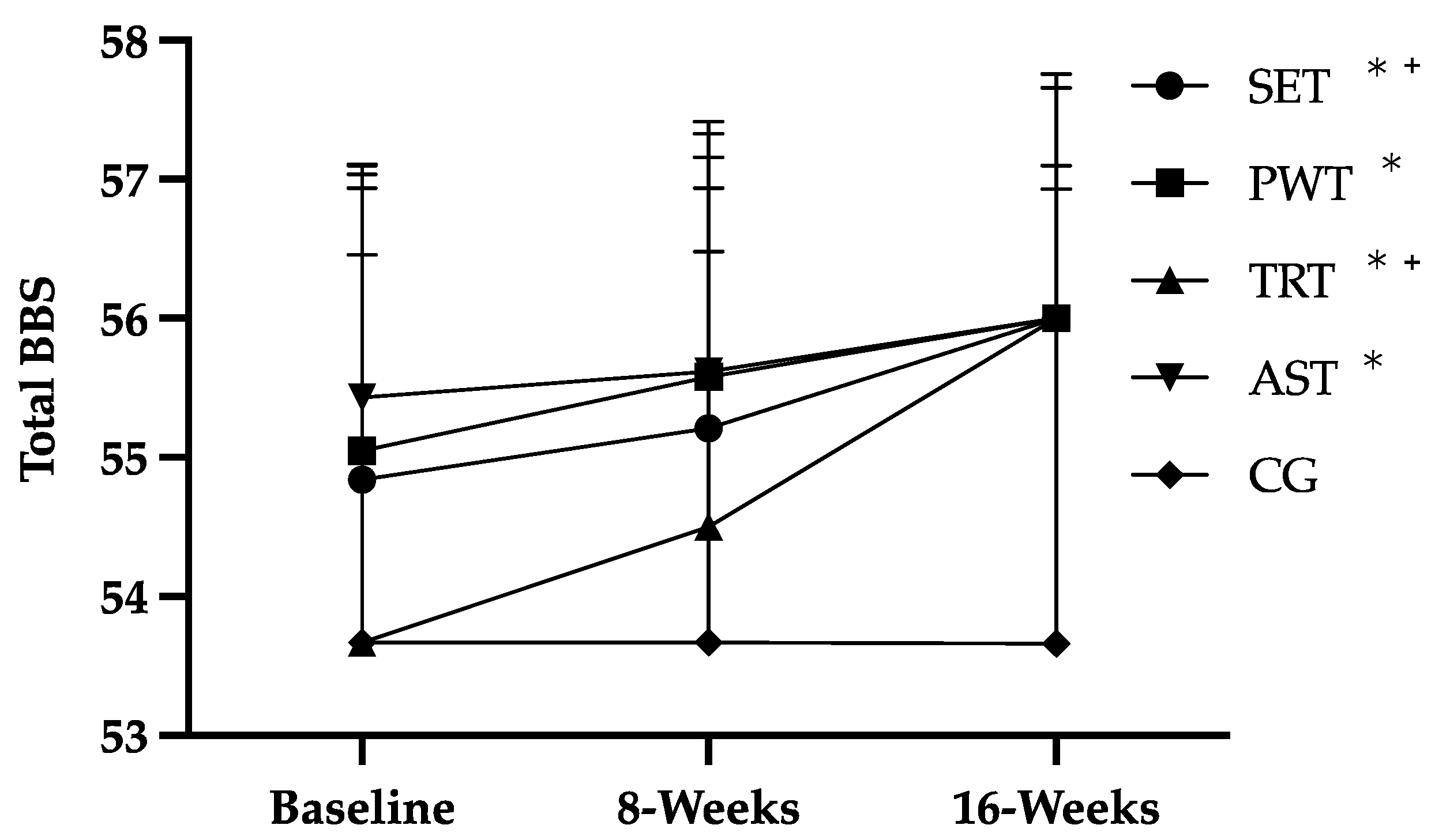
| Baseline | 8 Week | 16 Week | Baseline vs. 16-Week p-Value | |
|---|---|---|---|---|
| SET | 54.57 ± 2.32 | 55.05 ± 2.12 + | 55.89 ± 0.32 * | 0.02 |
| PWT | 54.95 ± 1.96 | 55.47 ± 1.84 | 55.95 ± 0.23 * | 0.04 |
| TRT | 53.55 ± 3.38 | 54.50 ± 2.66 + | 55.89 ± 0.47 * | 0.01 |
| AST | 55.43 ± 1.03 | 55.62 ± 0.87 | 55.95 ± 0.22 * | 0.02 |
| CG | 53.44 ± 3.28 | 53.28 ± 3.39 | 53.56 ± 3.18 | 0.43 |
| Group | Baseline | 8 Week | 16 Week | Baseline vs. 16-Week p-Value | ||
|---|---|---|---|---|---|---|
| PA Levels | Occupational PA | SET | 2.11 ± 0.32 | 2.17 ± 0.37 | 2.25 ± 0.41 | 0.25 |
| PWT | 1.97 ± 0.32 | 2.03 ± 0.34 | 2.04 ± 0.36 | 0.08 | ||
| TRT | 1.97 ± 0.25 | 1.99 ± 0.32 | 2.07 ± 0.27 | 0.09 | ||
| AST | 2.05 ± 0.35 | 2.11 ± 0.4 | 2.14 ± 0.38 | 0.51 | ||
| CG | 1.88 ± 0.12 | 1.91 ± 0.38 | 1.89 ± 0.38 | 0.91 | ||
| Leisure Sports Practice | SET | 2.21 ± 0.16 | 2.22 ± 1.18 | 2.2 ± 1.15 | 0.33 | |
| PWT | 2.03 ± 0.80 | 2.12 ± 0.78 | 2.12 ± 1.78 | 0.07 | ||
| TRT | 2.11 ± 0.96 | 2.87 ± 1.96 | 2.81 ± 1.90 * | 0.04 | ||
| AST | 1.83 ± 0.12 | 1.91 ± 0.78 | 2.4 ± 0.21 * | 0.03 | ||
| CG | 1.46 ± 0.68 | 1.43 ± 0.68 | 1.38 ± 1.62 | 0.85 | ||
| Leisure and locomotion PA | SET | 2.99 ± 1.82 | 3.43 ± 1.89 | 3.06 ± 1.15 | 0.07 | |
| PWT | 1.36 ± 0.91 | 2.18 ± 1.49 | 2.47 ± 1.37 * | 0.05 | ||
| TRT | 1.27 ± 0.57 | 1.82 ± 0.95 | 1.81 ± 0.95 * | 0.02 | ||
| AST | 1.69 ± 0.82 | 1.91 ± 0.58 | 2.21 ± 0.69 * | 0.02 | ||
| CG | 1.41 ± 0.31 | 1.52 ± 0.6 | 1.43 ± 0.41 | 0.97 | ||
| Total PA | SET | 7.31 ± 1.73 | 7.82 ± 1.95 | 7.51 ± 1.41 | 0.31 | |
| PWT | 5.36 ± 1.02 | 6.33 ± 1.53 | 6.63 ± 1.62 * | 0.04 | ||
| TRT | 5.35 ± 1.24 | 6.68 ± 1.30 | 6.69 ± 1.13 * | 0.05 | ||
| AST | 5.57 ± 1.37 | 5.93 ± 1.91 | 6.75 ± 1.79 * | 0.04 | ||
| CG | 4.75 ± 1.71 | 4.86 ± 1.52 | 4.71 ± 1.06 | 0.92 | ||
| WHOQOL-BREF | Physical | SET | 76.32 ± 15.02 | 77.26 ± 16.16 | 79.32 ± 15.04 * | 0.05 |
| PWT | 74.01 ± 16.88 | 75.20 ± 19.31 | 73.21 ± 18.34 | 0.86 | ||
| TRT | 72.06 ± 12.71 | 76.72 ± 14.89 * | 74.58 ± 12.62 | 0.71 | ||
| AST | 71.99 ± 15.89 | 76.13 ± 15.48 * | 73.12 ± 16.17 | 0.51 | ||
| CG | 72.56 ± 15.62 | 72.37 ± 16.49 | 73.50 ± 15.85 | 0.98 | ||
| Psychological | SET | 78.29 ± 14.27 | 80.04 ± 11.69 | 78.29 ± 10.72 | 0.94 | |
| PWT | 78.47 ± 15.41 | 79.40 ± 15.82 | 73.38 ± 14.09 | 0.31 | ||
| TRT | 75.98 ± 15.13 | 75.00 ± 16.21 | 73.78 ± 14.19 | 0.46 | ||
| AST | 78.51 ± 11.64 | 76.97 ± 15.30 | 76.10 ± 11.85 | 0.51 | ||
| CG | 79.39 ± 12.69 | 82.68 ± 12.75 | 80.26 ± 11.69 | 0.74 | ||
| Social | SET | 77.19 ± 16.16 | 75.88 ± 18.40 | 78.07 ± 15.27 | 0.83 | |
| PWT | 82.41 ± 12.75 | 79.17 ± 11.52 * | 76.85 ± 15.54 * | 0.04 | ||
| TRT | 75.49 ± 16.53 | 72.06 ± 18.85 * | 66.18 ± 21.14 * | 0.02 | ||
| AST | 78.51 ± 17.42 | 78.51 ± 17.19 | 75.88 ± 15.19 | 0.41 | ||
| CG | 77.19 ± 14.12 | 79.39 ± 14.26 | 78.07 ± 13.38 | 0.86 | ||
| Environment | SET | 71.38 ± 21.93 | 74.34 ± 18.30 | 72.86 ± 12.42 | 0.77 | |
| PWT | 65.97 ± 13.55 | 68.75 ± 17.58 | 68.58 ± 16.66 | 0.57 | ||
| TRT | 66.54 ± 17.04 | 67.83 ± 15.18 | 66.18 ± 13.22 | 0.96 | ||
| AST | 71.22 ± 16.91 | 70.39 ± 15.81 | 65.63 ± 14.47 * | 0.05 | ||
| CG | 74.84 ± 13.20 | 73.85 ± 13.27 | 74.01 ± 14.06 | 0.84 | ||
| Total WHOQOL-BREF | SET | 75.76 ± 13.98 | 77.02 ± 14.05 | 77.18 ± 9.09 | 0.61 | |
| PWT | 73.88 ± 12.27 | 75.11 ± 14.16 | 72.70 ± 13.87 | 0.76 | ||
| TRT | 72.18 ± 10.96 | 73.14 ± 12.14 | 71.32 ± 8.33 | 0.71 | ||
| AST | 74.55 ± 10.98 | 75.30 ± 12.28 | 72.12 ± 10.20 | 0.41 | ||
| CG | 75.46 ± 11.32 | 76.16 ± 11.62 | 75.71 ± 11.14 | 0.92 | ||
| WHOQOL-OLD | Total WHOQOL-OLD | SET | 54.66 ± 11.18 | 55.76 ± 11.60 | 58.96 ± 10.56 * | 0.02 |
| PWT | 56.91 ± 10.03 | 57.89 ± 11.09 | 66.83 ± 9.42 * | 0.01 | ||
| TRT | 52.14 ± 11.54 | 55.39 ± 14.43 | 61.15 ± 11.62 * | 0.02 | ||
| AST | 57.55 ± 9.83 | 63.80 ± 12.62 * | 65.89 ± 10.70 * | 0.05 | ||
| CG | 62.05 ± 10.41 | 61.97 ± 10.72 | 62.16 ± 10.73 | 0.89 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leitão, L.; Venturini, G.R.O.; Junior, R.P.; Monteiro, E.R.; Telles, L.G.; Araújo, G.; Novaes, J.; Tavares, C.; Marques-Neto, S.; Mazini, M. Impact of Different Resistance Training Protocols on Balance, Quality of Life and Physical Activity Level of Older Women. Int. J. Environ. Res. Public Health 2022, 19, 11765. https://doi.org/10.3390/ijerph191811765
Leitão L, Venturini GRO, Junior RP, Monteiro ER, Telles LG, Araújo G, Novaes J, Tavares C, Marques-Neto S, Mazini M. Impact of Different Resistance Training Protocols on Balance, Quality of Life and Physical Activity Level of Older Women. International Journal of Environmental Research and Public Health. 2022; 19(18):11765. https://doi.org/10.3390/ijerph191811765
Chicago/Turabian StyleLeitão, Luis, Gabriela R. O. Venturini, Ricardo Pace Junior, Estêvão Rios Monteiro, Luiz Guilherme Telles, Gleisson Araújo, Jefferson Novaes, Carlos Tavares, Sílvio Marques-Neto, and Mauro Mazini. 2022. "Impact of Different Resistance Training Protocols on Balance, Quality of Life and Physical Activity Level of Older Women" International Journal of Environmental Research and Public Health 19, no. 18: 11765. https://doi.org/10.3390/ijerph191811765