
Appraisal of the New Posture Analyzing and Virtual Reconstruction Device (PAViR) for Assessing Sagittal Posture Parameters: A Prospective Observational Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Assessment
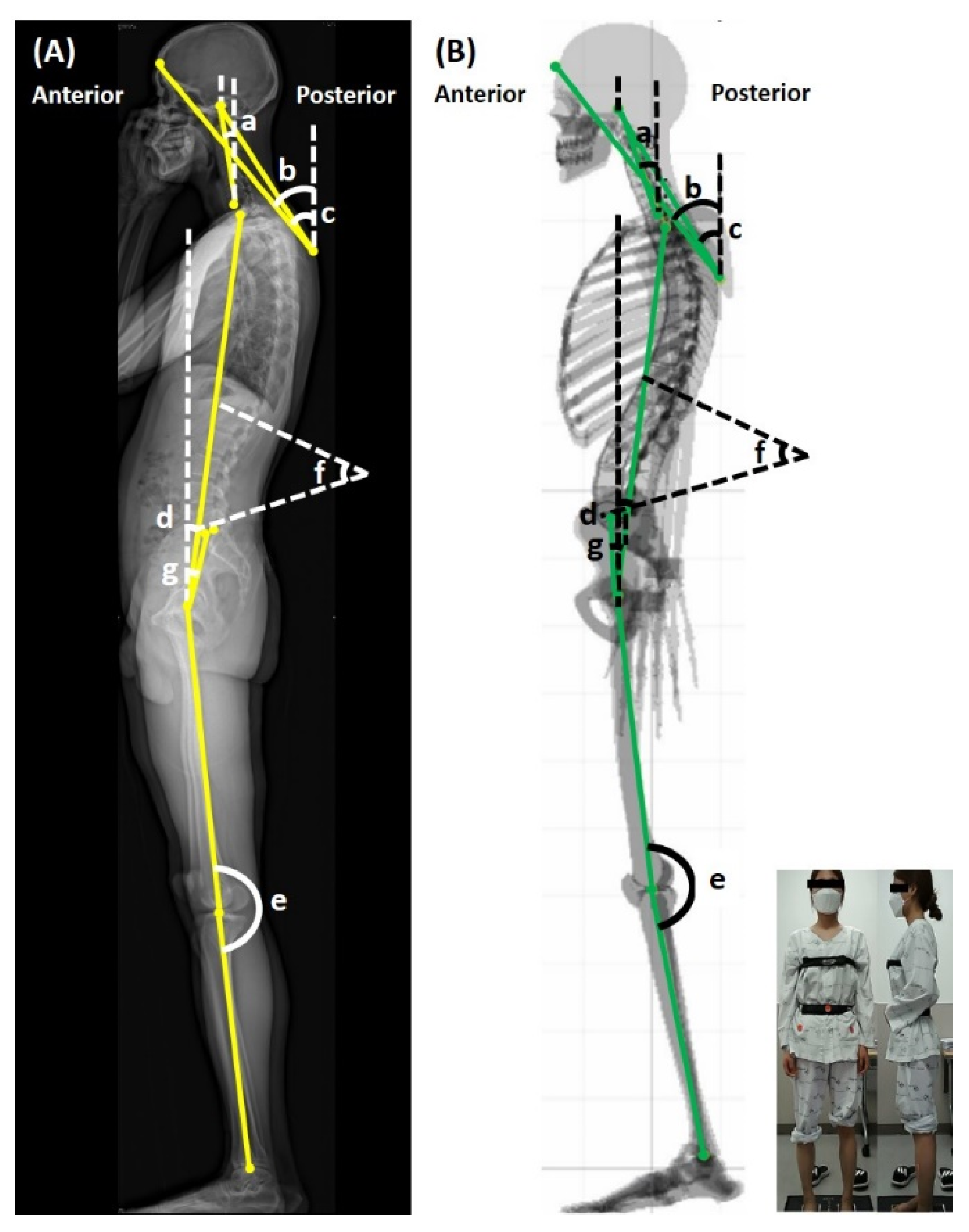
2.2.1. Posture Assessment
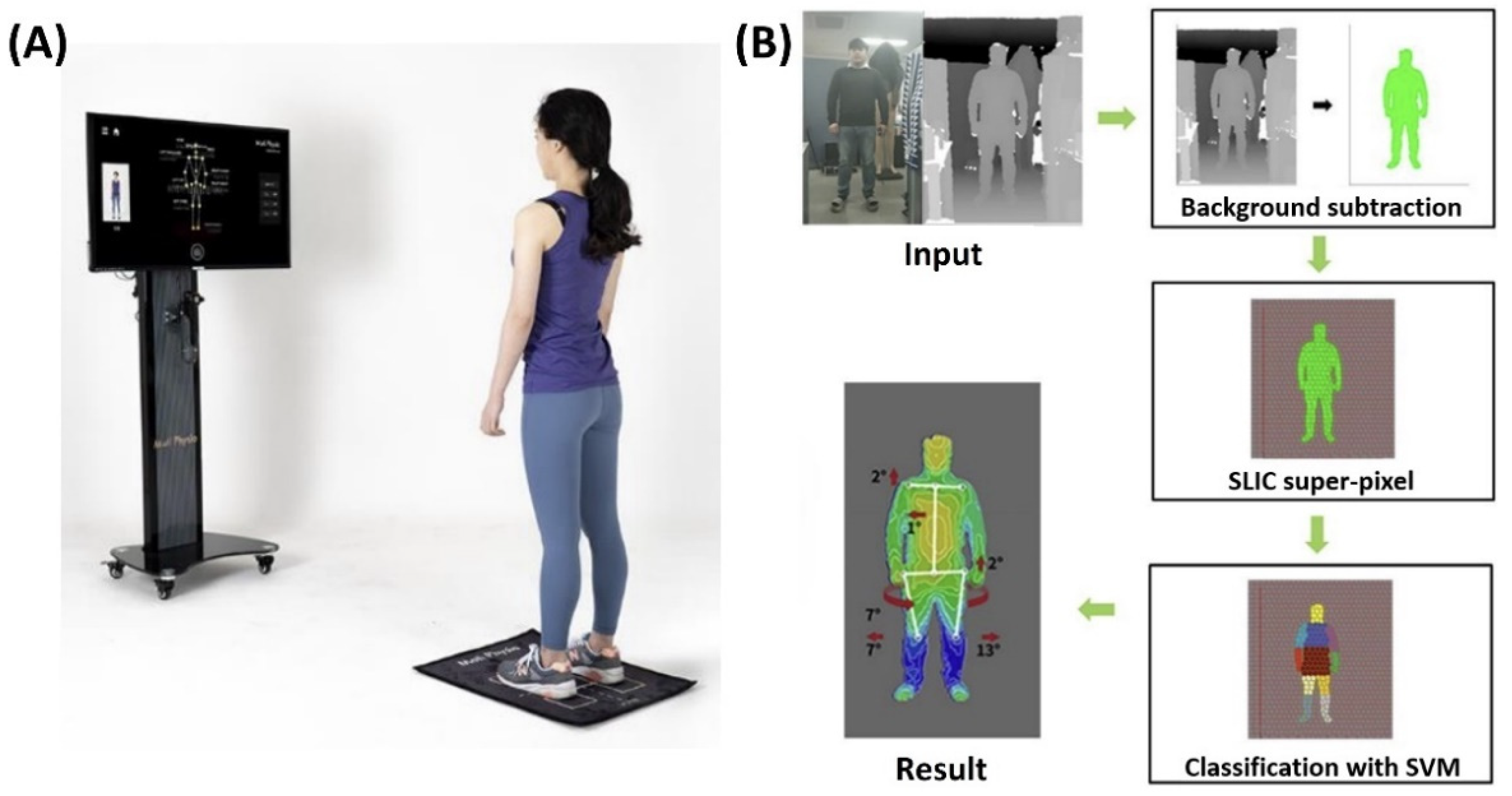
2.2.2. PAViR
2.2.3. Outcome Measures
2.3. Data Analysis
3. Results
3.1. Participants
3.2. Descriptive Outcome Values
3.3. Validity of PAViR Measurement
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pope, P.M. Severe and Complex Neurological Disability: Management of the Physical Condition; Butterworth-Heinemann Elsevier: Oxford, UK, 2007. [Google Scholar]
- Takasaki, H.; May, S. Mechanical diagnosis and therapy has similar effects on pain and disability as ‘wait and see’ and other approaches in people with neck pain: A systematic review. J. Physiother. 2014, 60, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Jackson, R.P.; Peterson, M.D.; McManus, A.C.; Hales, C. Compensatory spinopelvic balance over the hip axis and better reliability in measuring lordosis to the pelvic radius on standing lateral radiographs of adult volunteers and patients. Spine (Phila Pa 1976) 1998, 23, 1750–1767. [Google Scholar] [CrossRef] [PubMed]
- Vedantam, R.; Lenke, L.G.; Keeney, J.A.; Bridwell, K.H. Comparison of standing sagittal spinal alignment in asymptomatic adolescents and adults. Spine (Phila Pa 1976) 1998, 23, 211–215. [Google Scholar] [CrossRef] [PubMed]
- Fedorak, C.; Ashworth, N.; Marshall, J.; Paull, H. Reliability of the visual assessment of cervical and lumbar lordosis: How good are we? Spine (Phila Pa 1976) 2003, 28, 1857–1859. [Google Scholar] [CrossRef]
- Fortin, C.; Feldman, D.E.; Cheriet, F.; Labelle, H. Clinical methods for quantifying body segment posture: A literature review. Disabil. Rehabil. 2011, 33, 367–383. [Google Scholar] [CrossRef]
- Bryan, J.M.; Mosner, E.; Shippee, R.; Stull, M.A. Investigation of the validity of postural evaluation skills in assessing lumbar lordosis using photographs of clothed subjects. J. Orthop. Sports Phys. Ther. 1990, 12, 24–29. [Google Scholar] [CrossRef]
- Kendall, F.P.; McCreary, E.K.; Provance, P.G.; Rodgers, M.M.; Romani, W.A. Muscles: Testing and Function with Posture and Pain; Lippincott Williams & Wilkins Baltimore: Baltimore, MD, USA, 2005; Volume 5. [Google Scholar]
- Dubousset, J.; Charpak, G.; Dorion, I.; Skalli, W.; Lavaste, F.; Deguise, J.; Kalifa, G.; Ferey, S. A new 2D and 3D imaging approach to musculoskeletal physiology and pathology with low-dose radiation and the standing position: The EOS system. Bull. Acad. Natl. Med. 2005, 189, 287–297; discussion 297–300. [Google Scholar] [PubMed]
- Somoskeöy, S.; Tunyogi-Csapó, M.; Bogyó, C.; Illés, T. Accuracy and reliability of coronal and sagittal spinal curvature data based on patient-specific three-dimensional models created by the EOS 2D/3D imaging system. Spine J. 2012, 12, 1052–1059. [Google Scholar] [CrossRef]
- Deschênes, S.; Charron, G.; Beaudoin, G.; Labelle, H.; Dubois, J.; Miron, M.C.; Parent, S. Diagnostic imaging of spinal deformities: Reducing patients radiation dose with a new slot-scanning X-ray imager. Spine (Phila Pa 1976) 2010, 35, 989–994. [Google Scholar] [CrossRef] [PubMed]
- Luo, T.D.; Stans, A.A.; Schueler, B.A.; Larson, A.N. Cumulative Radiation Exposure With EOS Imaging Compared With Standard Spine Radiographs. Spine Deform. 2015, 3, 144–150. [Google Scholar] [CrossRef]
- Cohen, L.; Kobayashi, S.; Simic, M.; Dennis, S.; Refshauge, K.; Pappas, E. Non-radiographic methods of measuring global sagittal balance: A systematic review. Scoliosis Spinal Disord. 2017, 12, 30. [Google Scholar] [CrossRef]
- Knott, P.; Mardjetko, S.; Rollet, M.; Baute, S.; Riemenschneider, M.; Muncie, L. Evaluation of the reproducibility of the formetric 4D measurements for scoliosis. Scoliosis 2010, 5 (Suppl. S1), O10. [Google Scholar] [CrossRef]
- Faro, F.D.; Marks, M.C.; Pawelek, J.; Newton, P.O. Evaluation of a functional position for lateral radiograph acquisition in adolescent idiopathic scoliosis. Spine (Phila Pa 1976) 2004, 29, 2284–2289. [Google Scholar] [CrossRef]
- Steffen, J.S.; Obeid, I.; Aurouer, N.; Hauger, O.; Vital, J.M.; Dubousset, J.; Skalli, W. 3D postural balance with regard to gravity line: An evaluation in the transversal plane on 93 patients and 23 asymptomatic volunteers. Eur. Spine J. 2010, 19, 760–767. [Google Scholar] [CrossRef]
- Camplani, M.; Salgado, L. Background foreground segmentation with RGB-D Kinect data: An efficient combination of classifiers. J. Vis. Commun. Image Represent. 2014, 25, 122–136. [Google Scholar] [CrossRef]
- Kim, H.; Lee, S.; Lee, D.; Choi, S.; Ju, J.; Myung, H. Real-time human pose estimation and gesture recognition from depth images using superpixels and SVM classifier. Sensors 2015, 15, 12410–12427. [Google Scholar] [CrossRef]
- Achanta, R.; Shaji, A.; Smith, K.; Lucchi, A.; Fua, P.; Süsstrunk, S. SLIC superpixels compared to state-of-the-art superpixel methods. IEEE Trans. Pattern Anal. Mach. Intell. 2012, 34, 2274–2282. [Google Scholar] [CrossRef]
- Straka, M.; Hauswiesner, S.; Rüther, M.; Bischof, H. (Eds.) Skeletal Graph Based Human Pose Estimation in Real-Time. In Proceedings of the BMVC, Dundee, UK, 29 August 29–2 September 2011; pp. 1–12. [Google Scholar]
- Akoglu, H. User’s guide to correlation coefficients. Turk. J. Emerg. Med. 2018, 18, 91–93. [Google Scholar] [CrossRef]
- Tatsumi, M.; Mkoba, E.M.; Suzuki, Y.; Kajiwara, Y.; Zeidan, H.; Harada, K.; Bitoh, T.; Nishida, Y.; Nakai, K.; Shimoura, K.; et al. Risk factors of low back pain and the relationship with sagittal vertebral alignment in Tanzania. BMC Musculoskelet. Disord. 2019, 20, 584. [Google Scholar] [CrossRef]
- Hira, K.; Nagata, K.; Hashizume, H.; Asai, Y.; Oka, H.; Tsutsui, S.; Takami, M.; Iwasaki, H.; Muraki, S.; Akune, T.; et al. Relationship of sagittal spinal alignment with low back pain and physical performance in the general population. Sci. Rep. 2021, 11, 20604. [Google Scholar] [CrossRef]
- Zsidai, A.; Kocsis, L. Ultrasound-based spinal column examination systems. Facta Univ. -Ser. Phys. Educ. Sport 2001, 1, 1–12. [Google Scholar]
- Yeras, A.M.; Peña, R.G.; Junco, R. Moiré topography: Alternative technique in health care. Opt. Lasers Eng. 2003, 40, 105–116. [Google Scholar] [CrossRef]
- Goldberg, C.J.; Kaliszer, M.; Moore, D.P.; Fogarty, E.E.; Dowling, F.E. Surface topography, Cobb angles, and cosmetic change in scoliosis. Spine (Phila Pa 1976) 2001, 26, E55–E63. [Google Scholar] [CrossRef]
- Whittaker, D. Multidisciplinary approaches to breathing pattern disorders. Australas. Chiropr. Osteopathy 2002, 10, 111. [Google Scholar]
- Sahlstrand, T. The clinical value of Moiré topography in the management of scoliosis. Spine (Phila Pa 1976) 1986, 11, 409–417. [Google Scholar] [CrossRef] [PubMed]
- Rousseau, M.A.; Brusson, A.; Lazennec, J.Y. Assessment of the axial rotation of the pelvis with the EOS® imaging system: Intra- and inter-observer reproducibility and accuracy study. Eur. J. Orthop. Surg. Traumatol. 2014, 24, 891–895. [Google Scholar] [CrossRef] [PubMed]
- Metaxas, V.I.; Messaris, G.A.; Lekatou, A.N.; Petsas, T.G.; Panayiotakis, G.S. PATIENT DOSES IN COMMON DIAGNOSTIC X-RAY EXAMINATIONS. Radiat. Prot. Dosim. 2019, 184, 12–27. [Google Scholar] [CrossRef]
- Hui, S.C.; Pialasse, J.P.; Wong, J.Y.; Lam, T.P.; Ng, B.K.; Cheng, J.C.; Chu, W.C. Radiation dose of digital radiography (DR) versus micro-dose x-ray (EOS) on patients with adolescent idiopathic scoliosis: 2016 SOSORT- IRSSD “John Sevastic Award” Winner in Imaging Research. Scoliosis Spinal Disord. 2016, 11, 46. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Parameter | Parameter’ Full Name | Description |
|---|---|---|
| FHP (C7-CAC), ° | Forward head posture (C7-center of auditory canal), ° | Angle formed between the center of the 7th cervical vertebra (C7) to the center of the auditory canal |
| FHP (T4-FH), ° | Forward head posture (T4-frontal head), ° | Angle formed between the back at the 4th thoracic vertebra (T4) to the frontal head |
| FHP (T4-CAC), ° | Forward head posture (T4-center of auditory canal), ° | Angle formed between the back at the 4th thoracic vertebra (T4) to the center of the auditory canal |
| T1t, ° | T1 tilt angle, ° | Angle formed between the center of the 1st thoracic vertebra (T1) and the vertical axis traversing the center of the femoral head |
| KF, ° | Knee flexion angle, ° | Angle formed by the axis joining the center of the hip joint to the center of the knee joint and the axis joining the center of the knee joint to the center of the ankle joint |
| LL, ° | Lumbar lordosis angle, ° | Angle formed between the line extending from the upper plate of the 1st lumbar vertebra (L1) and the other extending from the lower plate of the 5th lumbar vertebra (L5) |
| PT, ° | Pelvic tilt angle, ° | Angle formed between the vertical axis traversing the center of the femoral head and the midpoint of the sacral endplate |
| Characteristics | Median (IQR) | Range (Min–Max) |
|---|---|---|
| Sex, n (%) | ||
| Male | 30 (42.86) | |
| Female | 40 (57.14) | |
| Age, yr | 55 (38–63) | 23–82 |
| Height, cm | 165 (159–172) | 147–185 |
| Weight, kg | 65 (56.25–73.00) | 43–100 |
| BMI, kg/m2 | 23.62 (21.69–25.33) | 16.38–31.25 |
| Sagittal Parameters | EOS Imaging System | PAViR | ||
|---|---|---|---|---|
| Median (IQR) | Range (Min–Max) | Median (IQR) | Range (Min–Max) | |
| FHP (C7-CAC), ° | 8.80 (5.13–15.50) | −2.10–30.80 | 10.24 (6.35–14.47) | −6.30–29.00 |
| FHP (T4-FH), ° | 41.40 (39.43–43.73) | 32.00–54.20 | 40.54 (39.08–41.90) | 33.90–47.00 |
| FHP (T4-CAC), ° | 31.60 (28.25–34.80) | 20.40–45.10 | 32.85 (30.23–35.10) | 21.80–54.30 |
| T1t, ° | 4.75 (2.83–6.48) | −5.70–11.30 | 2.95 (2.01–4.60) | −0.83–12.50 |
| KF, ° | 2.50 (1.23–5.28) | 0–18.90 | 3.90 (2.02–5.38) | −4.05–13.80 |
| LL, ° | 34.00 (29.00–42.00) | 7.00–61.00 | 34.55 (31.10–38.65) | 23.00–45.80 |
| PT, ° | 12.55 (6.53–17.93) | −2.50–35.00 | 9.35 (6.05–10.48) | 0.70–22.40 |
| Sagittal Parameters | Wilcoxon Signed Rank Test | Spearman’s Correlation | ||
|---|---|---|---|---|
| Median (IQR) of Difference | p-Value | Correlation Coefficient | p-Value | |
| FHP (C7-CAC), ° | 1.87 (0.83–4.38) | 0.418 | 0.741 | <0.001 |
| FHP (T4-FH), ° | 1.90 (0.86–3.05) | 0.034 | 0.795 | <0.001 |
| FHP (T4-CAC), ° | 1.84 (0.78–3.05) | <0.001 | 0.761 | <0.001 |
| T1t, ° | 1.50 (0.67–2.67) | 0.017 | 0.621 | <0.001 |
| KF, ° | 1.40 (0.80–3.35) | 0.207 | 0.514 | 0.004 |
| LL, ° | 4.05 (1.63–7.28) | 0.701 | 0.536 | 0.004 |
| PT, ° | 3.05 (1.23–6.58) | 0.046 | 0.692 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jang, C.W.; Park, J.; Cho, H.E.; Park, J.H. Appraisal of the New Posture Analyzing and Virtual Reconstruction Device (PAViR) for Assessing Sagittal Posture Parameters: A Prospective Observational Study. Int. J. Environ. Res. Public Health 2022, 19, 11109. https://doi.org/10.3390/ijerph191711109
Jang CW, Park J, Cho HE, Park JH. Appraisal of the New Posture Analyzing and Virtual Reconstruction Device (PAViR) for Assessing Sagittal Posture Parameters: A Prospective Observational Study. International Journal of Environmental Research and Public Health. 2022; 19(17):11109. https://doi.org/10.3390/ijerph191711109
Chicago/Turabian StyleJang, Chan Woong, Jihyun Park, Han Eol Cho, and Jung Hyun Park. 2022. "Appraisal of the New Posture Analyzing and Virtual Reconstruction Device (PAViR) for Assessing Sagittal Posture Parameters: A Prospective Observational Study" International Journal of Environmental Research and Public Health 19, no. 17: 11109. https://doi.org/10.3390/ijerph191711109