
Public Health Services, Health Human Capital, and Relative Poverty of Rural Families


Abstract
:1. Introduction
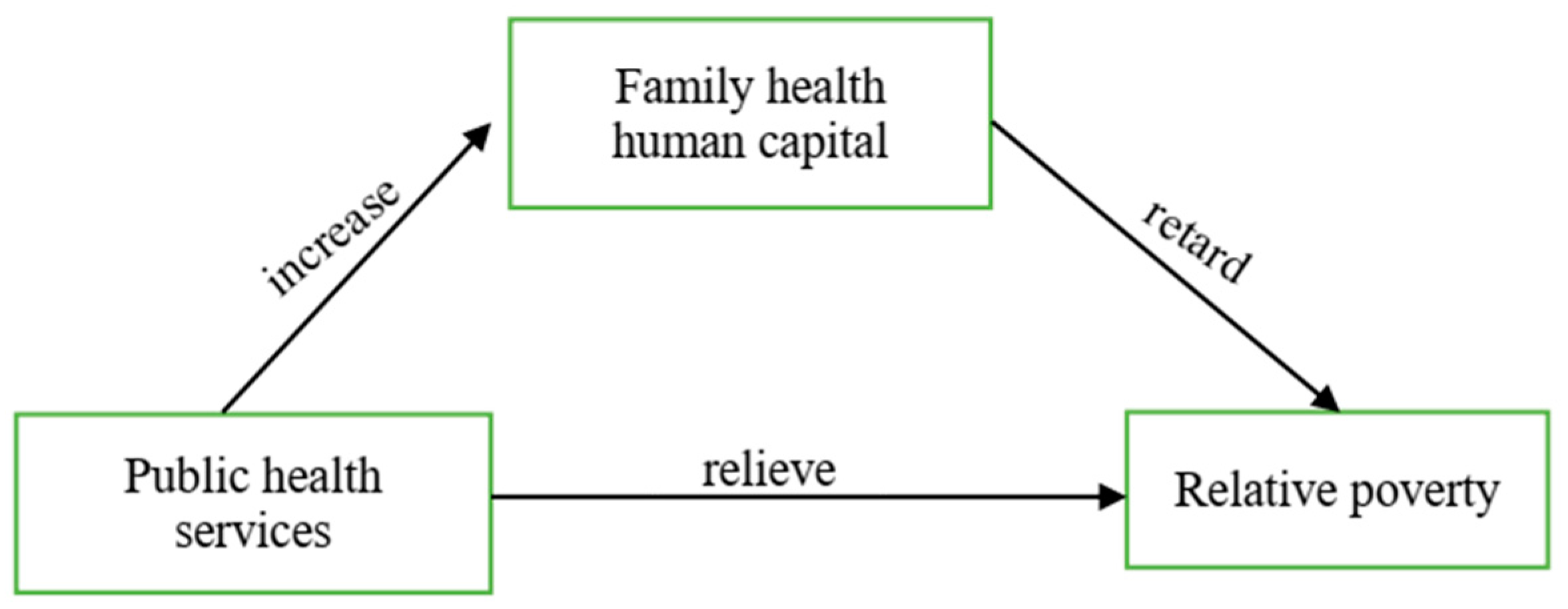
2. Analysis Framework and Research Assumptions
3. Model Setting, Data Source, and Variable Description
3.1. Model Setting
3.2. Data source and Variable Description
4. Analysis of Empirical Results
4.1. Basic Regression of Poverty Reduction in Public Health Services
4.2. Mediating Effect of Family Health Human Capital
4.3. Robustness Test
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hao, X.; Huang, N.; Zhuang, Y. Research on the Effect of Public Services on Rural Multidimensional Poverty Reduction from the Perspective of Rural Revitalization. China Soft Sci. 2019, 1, 72–81. [Google Scholar]
- Zhu, L. Health Investment and Human Capital Theory. Econ. Dyn. 2002, 8, 56–60. [Google Scholar]
- Li, Y.; Shen, K. Fiscal Expenditure Structure, Relative Poverty and Economic Growth. Manag. World 2007, 11, 14–26. [Google Scholar]
- Townsend, P. Poverty in the United Kingdom: A Survey of Household Resources and Standards of Living; Penguin Books: Harmonsworth, UK, 1979; pp. 46–49. [Google Scholar]
- Sun, J.; Xia, T. China’s Poverty Alleviation Strategy and the Delineation of Relative Poverty Line after 2020—Analysis Based on Theory, Policy and Data. China Rural. Econ. 2019, 10, 98–113. [Google Scholar]
- Shen, Y.; Li, S. How to Determine the Relative Poverty Standard—Also on the Feasible Scheme of “Urban and Rural Integration” Relative Poverty. J. South China Norm. Univ. 2020, 2, 91–101. [Google Scholar]
- Drewnowski, J. Poverty: Its Meaning and Measurement. Dev. Chang. 1977, 8, 183–208. [Google Scholar] [CrossRef]
- Nielsen, L. Global Relative Poverty; International Monetary Fund: Washington, DC, USA, 2009. [Google Scholar]
- Wang, C.; Yao, Y. Empirical Study on the Dynamic Evolution of Urban and Rural Poverty in China: 1990–2005. Quant. Econ. Technol. Econ. Res. 2010, 27, 3–15. [Google Scholar]
- Liu, H. Study on the Relationship between Migrant Workers, the Characteristics of the Elderly and Rural Family Poverty. Popul. Econ. 2017, 1, 63–74. [Google Scholar]
- Ravallion, M.; Chen, S. Global Poverty Measurement when Relative Income Matters. J. Public Econ. 2019, 177, 104046. [Google Scholar] [CrossRef]
- Hu, L.; Yao, S.; Song, X. Evaluation of Weak Relative Poverty in China and its Implications for Poverty Reduction Strategy after 2020. China Rural. Econ. 2021, 1, 72–90. [Google Scholar]
- Chakravarty, S.R. Measuring Vulnerability to Poverty: An Expected Poverty Index. In Themes in Economic Analysis; Routledge: London, UK, 2015. [Google Scholar]
- Qin, J.; Rong, A. Analysis of the Impact of Fiscal Expenditure Structure on Rural Relative Poverty. Econ. Issues 2012, 11, 95–98. [Google Scholar]
- Sen, A. Development as Freedom; Oxford University Press: Oxford, UK, 1999. [Google Scholar]
- Wang, X.; Feng, H. China’s Multidimensional Relative Poverty Standard after 2020: International Experience and Policy Orientation. China Rural. Econ. 2020, 3, 2–21. [Google Scholar]
- Zhang, N.; Kou, X.; Liu, R. Rural poverty reduction effect and efficiency of financial instruments—Based on the analysis of three relative poverty lines. China Rural. Econ. 2021, 1, 49–71. [Google Scholar]
- Wang, S.; Sun, J. China’s Relative Poverty Standard, Measurement and Targeting after Building A Well-off Society in An All-round Way—Analysis Based on China’s Household Survey Data in 2018. China Rural. Econ. 2021, 3, 2–23. [Google Scholar]
- Wang, W.; Luo, X.; Zhang, C.; Song, J.; Xu, D. Can Land Transfer Alleviate the Poverty of the Elderly? Evidence from Rural China. Int. J. Environ. Res. Public Health 2021, 18, 11288. [Google Scholar] [CrossRef]
- Wang, W.; Zhang, C.; Guo, Y.; Xu, D. Impact of Environmental and Health Risks on Rural Households’ Sustainable Livelihoods: Evidence from China. Int. J. Environ. Res. Public Health 2021, 18, 10955. [Google Scholar] [CrossRef]
- Zhang, Z.; Song, J.; Yan, C.; Xu, D.; Wang, W. Rural Household Differentiation and Poverty Vulnerability: An Empirical Analysis Based on the Field Survey in Hubei, China. Int. J. Environ. Res. Public Health 2022, 19, 4878. [Google Scholar] [CrossRef]
- Ballantine, J.; Brignall, S.; Modell, S. Performance Measurement and Management in Public Health Services: A Comparison of U.K. and Swedish Practice. Manag. Account. Res. 1998, 3, 71–94. [Google Scholar] [CrossRef]
- Almeida, C.; Travassos, C.; Porto, S.; Labra, M.E. Health Sector Reform in Brazil: A Case Study of Inequity. Int. J. Health Serv. 2000, 30, 129–162. [Google Scholar] [CrossRef]
- Callaghan, G.; Wistow, G. Governance and Public Involvement in the British National Health Service: Understanding Difficulties and Developments. Soc. Sci. Med. 2006, 63, 2289–2300. [Google Scholar] [CrossRef]
- Zhao, Z.G.; Cheng, J.Q.; Xu, S.L.; Hou, W.L.; Richardus, J.H. A Quality Assessment Index Framework for Public Health Services: A Delphi Study. Public Health 2015, 129, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D. Public Health Services in Shenzhen: A Case Study. Public Health 2011, 125, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Vellakkal, S. Impact of Public Health Programs on Maternal and Child Health Services and Health Outcomes in India: A Systematic Review. Soc. Sci. Med. 2021, 274, 113795. [Google Scholar] [CrossRef] [PubMed]
- Abbott, A.; Jones, P. Government Response to Increased Demand for Public Services: The Cyclicality of Government Health Expenditures in the OECD. Eur. J. Political Econ. 2021, 6, 101988. [Google Scholar] [CrossRef]
- Chen, S.; Li, J.; Lu, S.; Xiong, B. Escaping from poverty trap: A choice between government transfer payments and public services. Glob. Health Res. Policy 2017, 2, 15. [Google Scholar] [CrossRef]
- Wan, G.; Hu, X.; Liu, W. China’s Poverty Reduction Miracle and Relative Poverty: Focusing on the Roles of Growth and Inequality. China Econ. Rev. 2021, 68, 101643. [Google Scholar] [CrossRef]
- Liu, C. Rural Public Investment, Public Services and China’s Pro Poor Growth. Agric. Econ. Issues 2012, 6, 49–54. [Google Scholar]
- Zeng, F.; Zeng, X. An Empirical Study on Poverty Reduction through Basic Public Services—A Case Study of Hunan Province. Agric. Technol. Econ. 2013, 8, 4–11. [Google Scholar]
- Xu, J.; Fang, W. Government Assistance or Public Services: A Study on the Efficiency of Poverty Reduction Policies for Urban and Rural Floating Population. Sci. Res. Manag. 2017, 6, 152–160. [Google Scholar]
- Zhu, L. Grass Roots Public Service Supply and Poverty Reduction in Agricultural and Pastoral Areas of Tibet. Manag. World 2004, 4, 41–50. [Google Scholar]
- Wang, Y.; Liu, L. The Impact of New Rural Cooperative Medical Insurance and Health Human Capital on Rural Residents’ Labor Participation. China Rural. Econ. 2016, 11, 68–81. [Google Scholar]
- Wu, B. The Role of the New Rural Cooperative Medical System in Poverty Alleviation—A Comparative Analysis Based on the Income and Heat Poverty Line. Soc. Secur. Rev. 2018, 2, 55–70. [Google Scholar]
- Liu, Y.; Nie, R. An Empirical Study on Income Gap, Medical Insurance and Health poverty—Evidence Based on CFPS Data. J. Liaoning Univ. (Philos. Soc. Sci.) 2019, 4, 55–63. [Google Scholar]
- Zhou, J.; Zhou, Z.; He, M. Has the Basic Medical Insurance Reduced the Poverty of the Rural Elderly Population—From the New Rural Cooperative Medical System to the Medical Insurance for Urban and Rural Residents. Soc. Secur. Res. 2019, 3, 33–45. [Google Scholar]
- Castro-Leal, F.; Dayton, J.; Demery, L.; Mehra, K. Public Social Spending in Africa: Do the Poor Benefit? World Bank Res. Obs. 1999, 14, 49–72. [Google Scholar] [CrossRef]
- Sen, A. Inequality Reexamined; Philosophical Books; Harvard University Press: Cambridge, MA, USA, 1994; Volume 1, pp. 65–67. [Google Scholar]
- Mushkin, S.J. Health as An Investment. J. Political Econ. 1962, 70, 129–157. [Google Scholar] [CrossRef]
- Grossman, M. On the Concept of Health Capital and the Demand for Health. J. Political Econ. 1972, 80, 223–255. [Google Scholar] [CrossRef]
- Becker, G.S. A Theory of the Allocation of Time. Econ. J. 1965, 299, 493–517. [Google Scholar] [CrossRef]
- Schultz, T.P. On Human Capital Investment; Beijing Institute of Economics Press: Beijing, China, 1990. [Google Scholar]
- Wang, Y.; Yin, Z. Healthy Human Capital accumulation and Farmers’ Income Growth. China Rural. Econ. 2009, 12, 24–31. [Google Scholar]
- Gyimah-Brempong, K.; Wilson, M. Health Human Capital and Economic Growth in Sub-Saharan African and OECD Countries. Q. Rev. Econ. Financ. 2004, 2, 296–320. [Google Scholar] [CrossRef]
- Weil, D.N. Accounting for the Effect of Health on Economic Growth. Q. J. Econ. 2007, 3, 1265–1306. [Google Scholar] [CrossRef]
- Yang, Y.; Wang, W. Research on the Poverty Reduction Effect of equalization of Basic Public Services in Urban and Rural Areas. J. Huazhong Univ. Sci. Technol. (Soc. Sci. Ed.) 2020, 2, 75–82. [Google Scholar]
- Mayer, E.; Sarin, A. Some Mechanisms Linking Economic in Equality and Infant Mortality. Soc. Sci. Med. 2005, 3, 439–455. [Google Scholar] [CrossRef] [PubMed]
- Farahani, M.; Subramanian, S.V.; Canning, D. Effects of State-level Public Spending on Health on the Mortality Probability in India. Health Econ. 2010, 19, 1361–1376. [Google Scholar] [CrossRef] [PubMed]
- Mcintyre, D.; Meheus, F.; Røttingen, J.A. What Level of Domestic Government Health Expenditure Should We Aspire to for Universal Health Coverage? Health Econ. Policy Law 2017, 12, 125–137. [Google Scholar] [CrossRef]
- Gupta, S.; Verhoeven, M. The Efficiency of Government Expenditure: Experiences from Africa. J. Policy Model. 2001, 23, 7–15. [Google Scholar] [CrossRef]
- Zheng, D.; Gong, J.; Zhang, C. Efficiency of Medical Service Systems in the Rural areas of Mainland China: A Comparative Study from 2013 to 2017. Public Health 2019, 171, 139–147. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable Name | Variable Description | Mean | SD a | MIN | MAX |
|---|---|---|---|---|---|
| Family relative poverty (Pov) | 1 = Poverty 0 = Non-poverty | 0.21072 | 0.40783 | 0 | 1 |
| Public health services (Pubmed) | Per capita financial medical and health expenditure (CNY) | 637.08610 | 268.54480 | 199.83100 | 1704.61700 |
| Age of householder (Age) | Year | 47.65101 | 16.75277 | 10 | 99 |
| Education level of householder (Aedu) | Year | 5.89187 | 4.40064 | 0 | 22 |
| Family health human capital (Heapop) | Family self-rated healthy population/total family population | 0.81935 | 0.26627 | 0 | 1 |
| Time spent by the family away from the nearest business street (Cdis) | minute | 36.60226 | 59.45423 | 1 | 1440 |
| Whether the family is farming (Farm) | 1 = Engage in agricultural work, 0 = not engaged in agricultural work | 0.81585 | 0.38762 | 0 | 1 |
| Family health expenditure (Afmedcost) | Per capita health care expenditure of households (CNY) | 1273.3460 | 4303.7340 | 0 | 246,666.70 |
| Family burden coefficient (Bur) | Family non-working age population/working age population | 0.36143 | 0.59995 | 0 | 10 |
| Geographical location of the village (Cdistance) | Distance between village and county (LI) | 44.11037 | 37.13605 | 0 | 280 |
| Industrial structure (Third) | Proportion of tertiary industry in the province (%) | 41.90452 | 6.79345 | 29.30 | 69.17880 |
| Independent Variable | Coefficient | Odds Ratio | |
|---|---|---|---|
| Pubmed | −0.00210 *** (0.00026) | 0.99791 *** (0.00026) | −0.00027 *** (0.00003) |
| Age | −0.04382 *** (0.00708) | 0.95713 *** (0.00678) | −0.00558 *** (0.00090) |
| Age2 | 0.00063 *** (0.00007) | 1.00063 *** (0.00007) | 0.00008 *** (0.00001) |
| Aedu | −0.05400 *** (0.00627) | 0.94743*** (0.00594) | −0.00688 *** (0.00080) |
| Lnafmedcost | −0.02146 *** (0.00553) | 0.97877 *** (0.00541) | −0.00273 *** (0.00070) |
| Cdis | 0.00214 *** (0.00045) | 1.00214 *** (0.00045) | 0.00027 *** (0.00006) |
| Farm | −0.27129 *** (0.06154) | 0.76240 *** (0.04692) | −0.03456 *** (0.00781) |
| Bur | 0.23207 *** (0.03927) | 1.26121 *** (0.04953) | 0.02956 *** (0.00499) |
| Cdistance | 0.00392 *** (0.00076) | 1.00393 *** (0.00076) | 0.00050 *** (0.00010) |
| Third | −0.00835 (0.00553) | 0.99168 (0.00548) | −0.00317 (0.00070) |
| Constant term | −0.34084 (0.29349) | 0.71117 (0.20872) | _ |
| Observations | 19,890 | 19,890 | 19,890 |
| Independent Variable | (1) | (2) | |
|---|---|---|---|
| Heapop | Pov | ||
| Coefficient | Odds ratio | ||
| Pubmed | 0.00007 *** (0.00002) | 0.99797 *** (0.00026) | −0.00026 *** (0.00003) |
| Heapop | 0.35703 *** (0.03058) | −0.13132 *** (0.01088) | |
| Lnafmedcost | −0.00722 *** (0.00043) | 0.96972 *** (0.00537) | −0.00392 *** (0.00071) |
| Age | 0.00030 (0.00053) | 0.95569 *** (0.00673) | −0.00578 *** (0.00090) |
| Age2 | −0.00002 *** (0.00001) | 1.00062 *** (0.00007) | 0.00008 *** (0.00001) |
| Cdis | −0.00008 * (0.00005) | 1.00206 *** (0.00044) | 0.00026 *** (0.00006) |
| Cdistance | −0.00008 (0.00007) | 1.00379 *** (0.00075) | 0.00048 *** (0.00009) |
| Farm | 0.02003 *** (0.00486) | 0.78939 *** (0.04845) | −0.03015 *** (0.00780) |
| Bur | 0.05296 *** (0.00310) | 1.34931 *** (0.05289) | 0.03820 *** (0.00499) |
| Aedu | 0.00412 *** (0.00048) | 0.95211 *** (0.00594) | −0.00626 *** (0.00080) |
| Third | −0.00095 ** (0.00045) | 0.99091 * (0.00542) | −0.00116 *** (0.00070) |
| Constant term | 0.86184 *** (0.02320) | 1.78025 * (0.53466) | — |
| Observations | 19,890 | 19,890 | |
| Core Explanatory Variables | Intermediary Variable | Dependent Variable (POV) | |
|---|---|---|---|
| Pubmed | Heapop | Total effect | −0.00028 ** |
| (0.00012) | |||
| Direct effect | −0.00023 * | ||
| (0.00012) | |||
| Indirect effect | −0.00005 *** | ||
| (0.00001) | |||
| Indirect effect/Total effect | 18.56% | ||
| Estimation Method | Probit | Logit | Probit |
|---|---|---|---|
| Dependent Variable | Pov | Pov1 | Pov1 |
| Model Number | (1) | (2) | (3) |
| Pubmed | −0.00025 *** (0.00003) | −0.00030 *** (0.00004) | −0.00028 *** (0.00004) |
| Heapop | −0.13364 *** (0.01104) | −0.16094 *** (0.01215) | −0.16899 *** (0.01231) |
| Other control variables | Yes | Yes | Yes |
| Observations | 19,890 | 19,890 | 19,890 |
| Total effect | −0.00017 ** (0.00007) | −0.00024 ** (0.00011) | −0.00014 ** (0.00007) |
| Direct effect | −0.00014 ** (0.00007) | −0.00020 * (0.00011) | −0.00011 * (0.00007) |
| Indirect effect | −0.00003 *** (0.00001) | −0.00004 *** (0.00001) | −0.00003 *** (0.00001) |
| Indirect effect/Total effect | 17.56% | 16.58% | 23.55% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, Y.; Zhou, L.; Zhang, C.; Luo, X.; Luo, Y.; Wang, W. Public Health Services, Health Human Capital, and Relative Poverty of Rural Families. Int. J. Environ. Res. Public Health 2022, 19, 11089. https://doi.org/10.3390/ijerph191711089
Yang Y, Zhou L, Zhang C, Luo X, Luo Y, Wang W. Public Health Services, Health Human Capital, and Relative Poverty of Rural Families. International Journal of Environmental Research and Public Health. 2022; 19(17):11089. https://doi.org/10.3390/ijerph191711089
Chicago/Turabian StyleYang, Yingya, Liangliang Zhou, Chongmei Zhang, Xin Luo, Yihan Luo, and Wei Wang. 2022. "Public Health Services, Health Human Capital, and Relative Poverty of Rural Families" International Journal of Environmental Research and Public Health 19, no. 17: 11089. https://doi.org/10.3390/ijerph191711089