

Arterial Stiffness and HbA1c: Association Mediated by Insulin Resistance in Hispanic Adults
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Dependent Variable: Arterial Stiffness
2.2. Independent Variable: HbA1c
2.3. Mediator and Potential Confounding Variables
2.4. Statistical Analysis
2.4.1. Descriptive Analysis
2.4.2. Association Assessment
2.4.3. Mediation Analysis
2.4.4. Modifiers of the Effect of HbA1c on PWV
3. Results
3.1. Descriptive Analysis
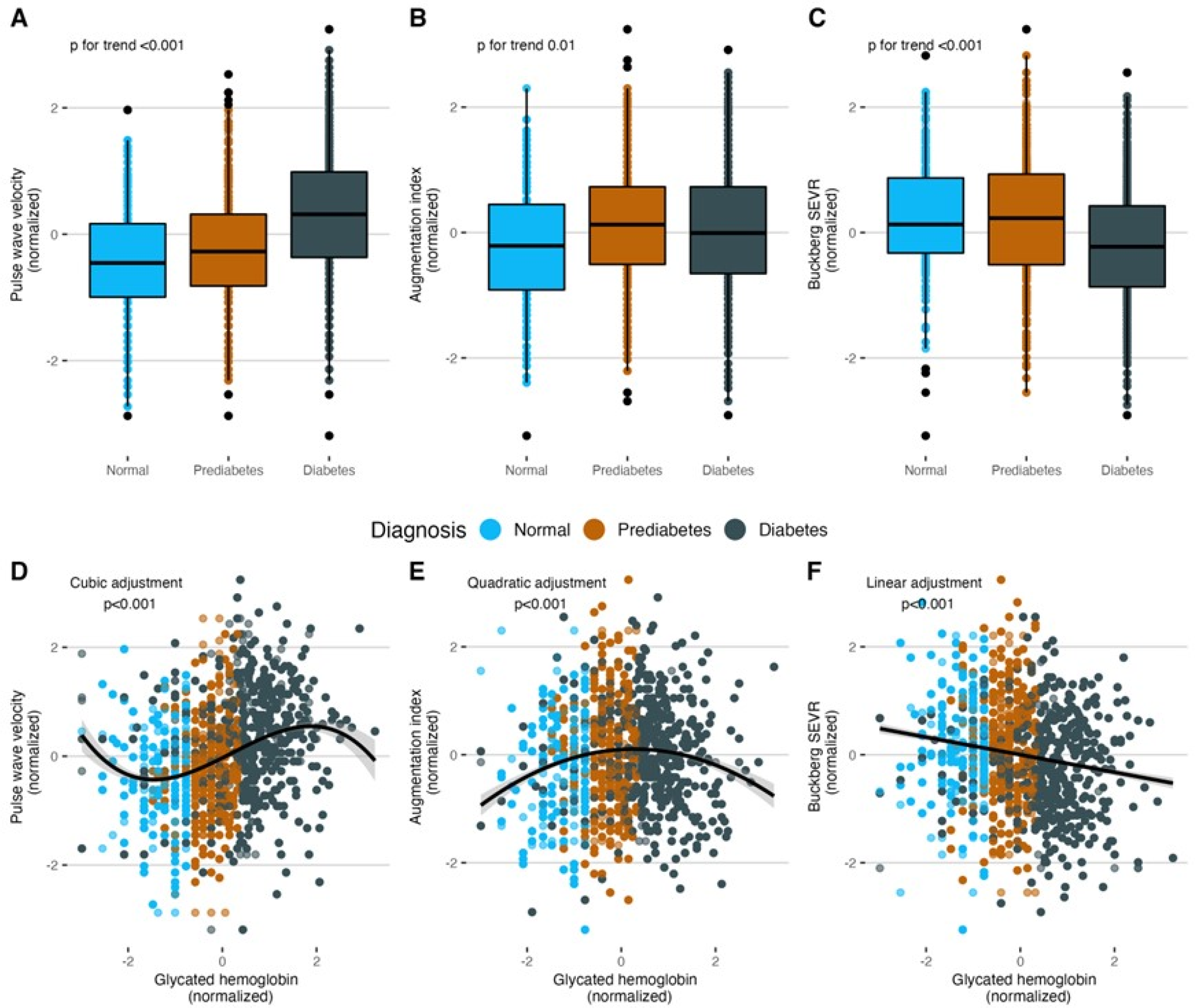
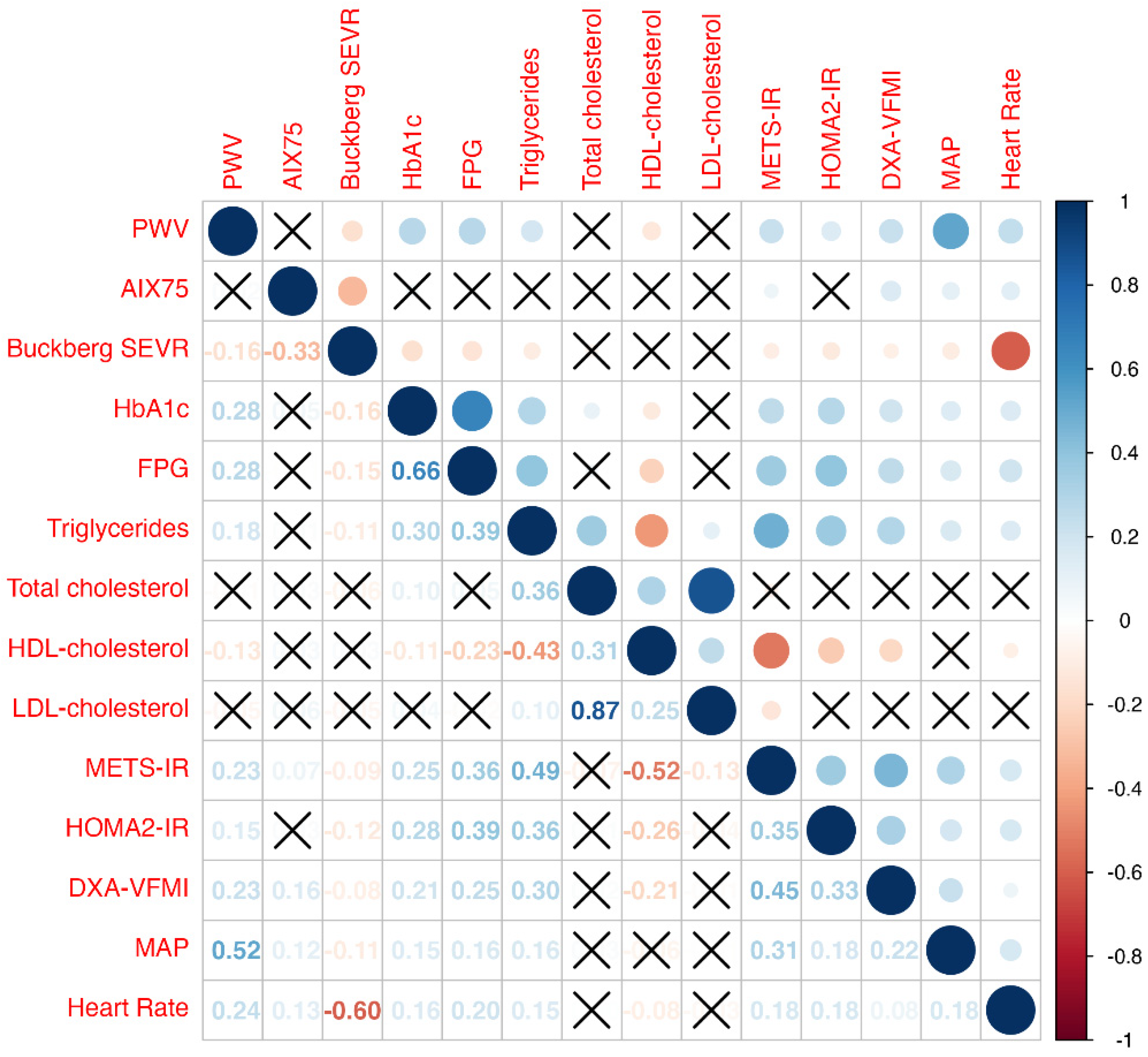
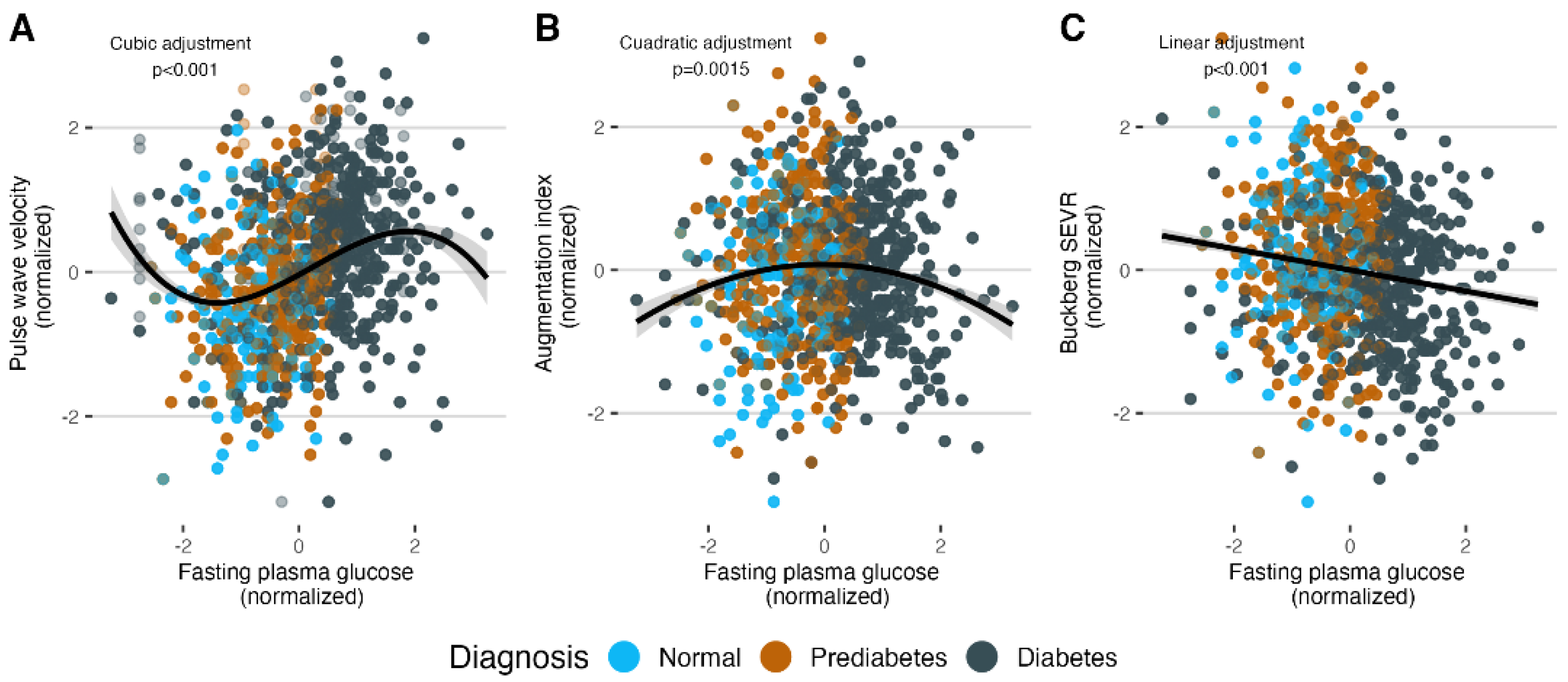
3.2. Association Assessment
3.3. Mediation Analysis
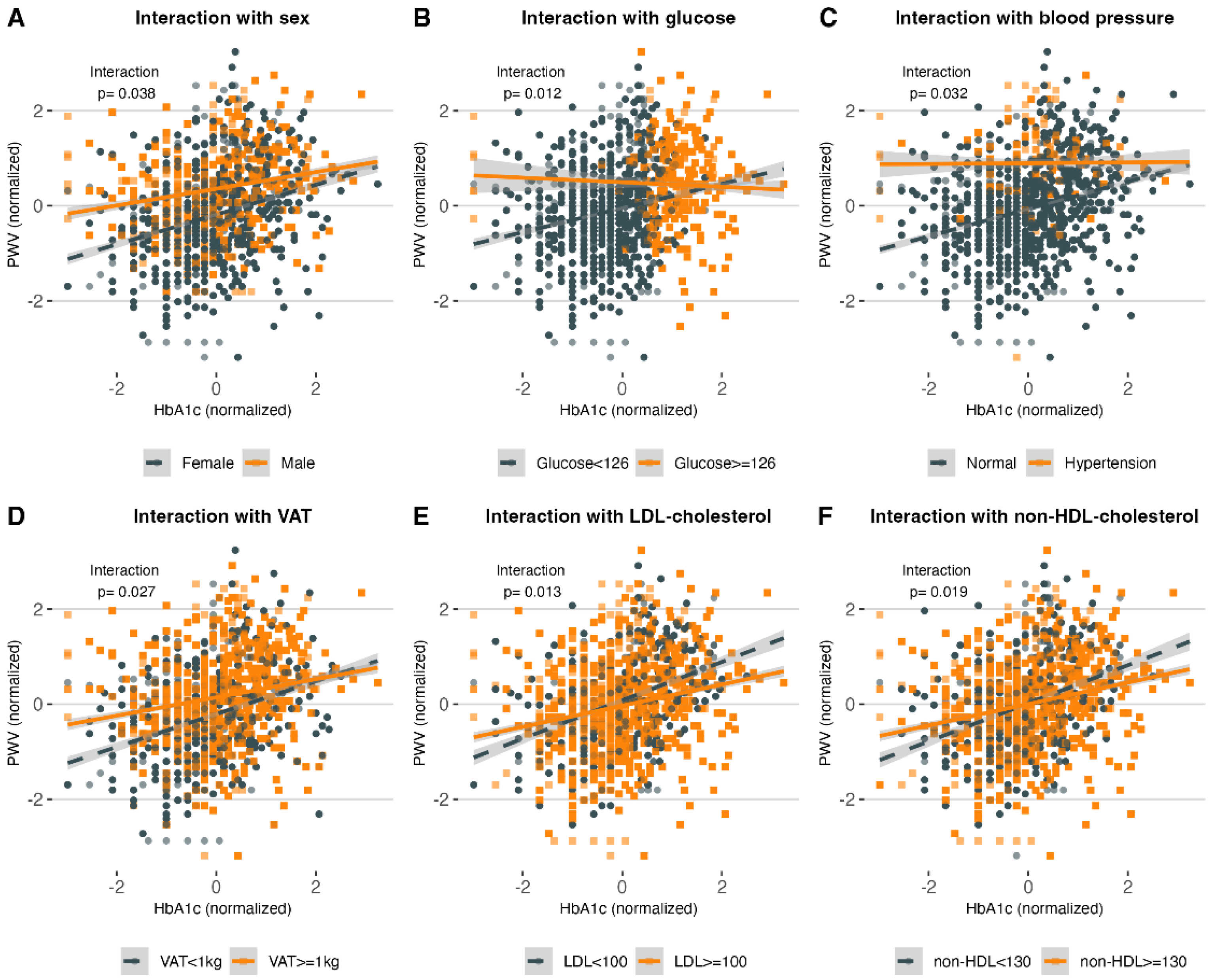
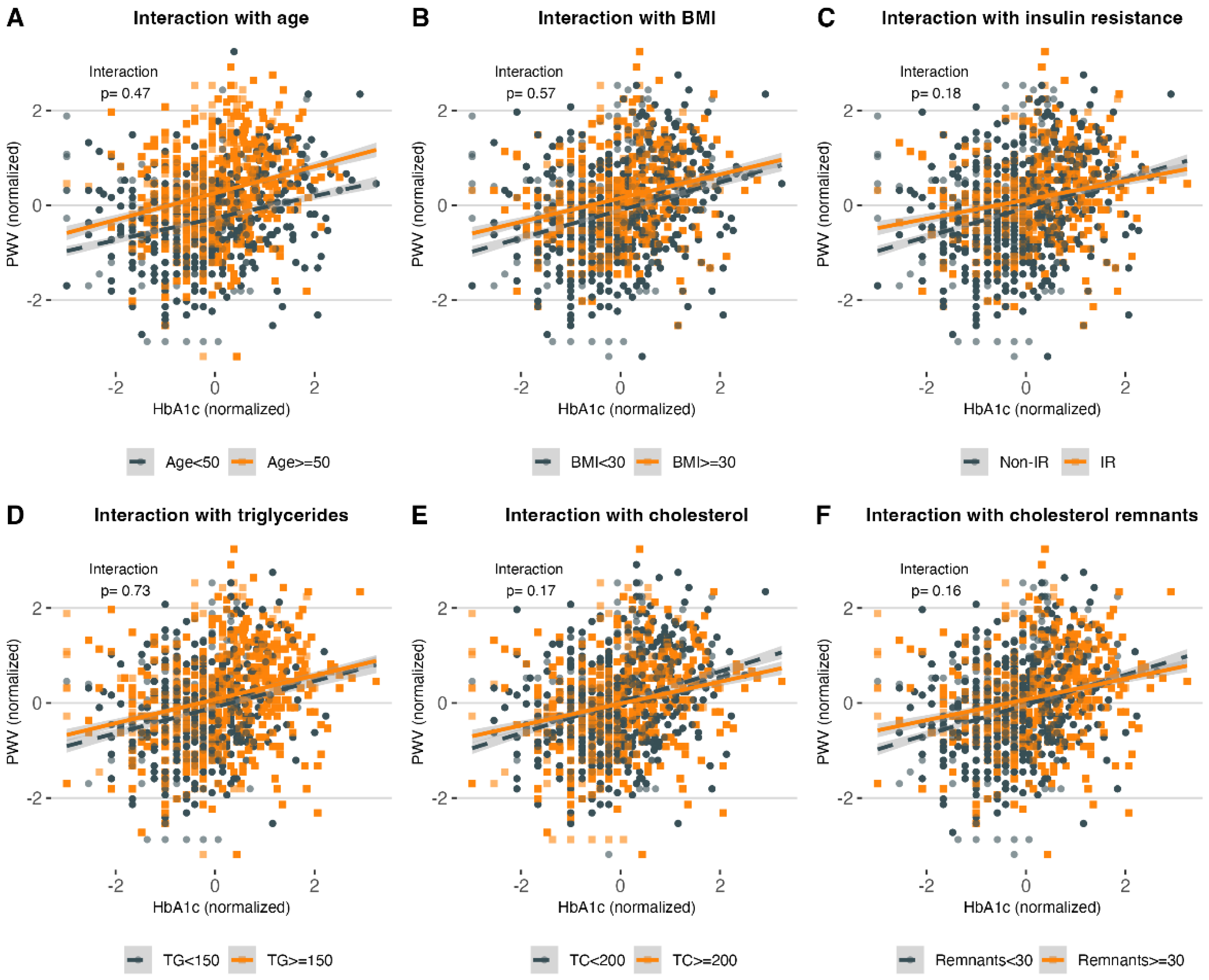
3.4. Modifiers of the Effect of HbA1c on PWV
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

Appendix B

Appendix C

Appendix D

References
- Vlachopoulos, C.; Aznaouridis, K.; Stefanadis, C. Prediction of Cardiovascular Events and All-Cause Mortality with Arterial Stiffness. J. Am. Coll. Cardiol. 2010, 55, 1318–1327. [Google Scholar] [CrossRef]
- Cavalcante, J.; Lima, J.A.; Redheuil, A.; Al-Mallah, M. Aortic Stiffness. J. Am. Coll. Cardiol. 2011, 57, 1511–1522. [Google Scholar] [CrossRef] [PubMed]
- Schutte, A.E.; Kruger, R.; Gafane-Matemane, L.F.; Breet, Y.; Strauss-Kruger, M.; Cruickshank, J.K. Ethnicity and Arterial Stiffness. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 1044–1054. [Google Scholar] [CrossRef] [PubMed]
- DuPont, J.J.; Kenney, R.M.; Patel, A.R.; Jaffe, I.Z. Sex Differences in Mechanisms of Arterial Stiffness. Br. J. Pharmacol. 2019, 176, 4208–4225. [Google Scholar] [CrossRef] [PubMed]
- The Reference Values for Arterial Stiffness’ Collaboration. Determinants of Pulse Wave Velocity in Healthy People and in the Presence of Cardiovascular Risk Factors: ‘Establishing Normal and Reference Values’. Eur. Heart J. 2010, 31, 2338–2350. [Google Scholar] [CrossRef]
- Johansen, N.B.; Vistisen, D.; Brunner, E.J.; Tabák, A.G.; Shipley, M.J.; Wilkinson, I.B.; McEniery, C.M.; Roden, M.; Herder, C.; Kivimäki, M.; et al. Determinants of Aortic Stiffness: 16-Year Follow-Up of the Whitehall II Study. PLoS ONE 2012, 7, e37165. [Google Scholar] [CrossRef]
- Cruickshank, J.K.; Silva, M.J.; Molaodi, O.R.; Enayat, Z.E.; Cassidy, A.; Karamanos, A.; Read, U.M.; Faconti, L.; Dall, P.; Stansfield, B.; et al. Ethnic Differences in and Childhood Influences on Early Adult Pulse Wave Velocity. Hypertension 2016, 67, 1133–1141. [Google Scholar] [CrossRef]
- Ashraf, A.P.; Fisher, G.; Alvarez, J.; Dudenbostel, T.; Calhoun, D.A.; Szalai, A.J.; Gower, B.A. Associations of C-Reactive Protein to Indices of Vascular Health and the Influence of Serum 25(OH)D Status in Healthy Adults. J. Nutr. Metab. 2012, 2012, 475975. [Google Scholar] [CrossRef]
- Schram, M.T.; Kostense, P.J.; van Dijk, R.A.J.M.; Dekker, J.M.; Nijpels, G.; Bouter, L.M.; Heine, R.J.; Stehouwer, C.D.A. Diabetes, Pulse Pressure and Cardiovascular Mortality: The Hoorn Study. J. Hypertens. 2002, 20, 1743–1751. [Google Scholar] [CrossRef]
- Henry, R.M.A.; Kostense, P.J.; Spijkerman, A.M.W.; Dekker, J.M.; Nijpels, G.; Heine, R.J.; Kamp, O.; Westerhof, N.; Bouter, L.M.; Stehouwer, C.D.A. Arterial Stiffness Increases with Deteriorating Glucose Tolerance Status. Circulation 2003, 107, 2089–2095. [Google Scholar] [CrossRef]
- Stakos, D.A.; Schuster, D.P.; Sparks, E.A.; Meis, S.B.; Wooley, C.F.; Osei, K.; Boudoulas, H. Association between Glycosylated Hemoglobin, Left Ventricular Mass and Aortic Function in Nondiabetic Individuals with Insulin Resistance. Eur. J. Endocrinol. 2007, 157, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Sun, H.; Shang, F.; Wu, H.; Shi, H.; Ren, L.; He, Y.; Zhang, M.; Peng, H. Association between Glucose Metabolism and Vascular Aging in Chinese Adults: A Cross-Sectional Analysis in the Tianning Cohort Study. Clin. Interv. Aging 2019, 14, 1937–1946. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.; Kim, J.; Sohn, T.; Son, H.; Lee, J. Effects of Glucose Control on Arterial Stiffness in Patients with Type 2 Diabetes Mellitus and Hypertension: An Observational Study. J. Int. Med. Res. 2018, 46, 284–292. [Google Scholar] [CrossRef]
- Nuamchit, T.; Siriwittayawan, D.; Thitiwuthikiat, P. The Relationship Between Glycemic Control and Concomitant Hypertension on Arterial Stiffness in Type II Diabetes. Vasc. Health Risk Manag. 2020, 16, 343–352. [Google Scholar] [CrossRef]
- Moreno, B.; de Faria, A.P.; Ritter, A.M.V.; Yugar, L.B.T.; Ferreira-Melo, S.E.; Amorim, R.; Modolo, R.; Fattori, A.; Yugar-Toledo, J.C.; Coca, A.; et al. Glycated Hemoglobin Correlates with Arterial Stiffness and Endothelial Dysfunction in Patients with Resistant Hypertension and Uncontrolled Diabetes Mellitus. J. Clin. Hypertens. 2018, 20, 910–917. [Google Scholar] [CrossRef] [PubMed]
- Noh, J.-W.; Kim, E.-J.; Seo, H.-J.; Kim, S.G. Independent Association between Glycated Hemoglobin and Arterial Stiffness in Healthy Men. J. Diabetes Investig. 2016, 7, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Kulecki, M.; Uruska, A.; Naskret, D.; Zozulinska-Ziolkiewicz, D. Arterial Stiffness and Type 1 Diabetes: The Current State of Knowledge. Curr. Diabetes Rev. 2021, 18, 41–51. [Google Scholar] [CrossRef]
- Shah, A.S.; Isom, S.; D’Agostino, R., Jr.; Dolan, L.M.; Dabelea, D.; Imperatore, G.; Mottl, A.; Lustigova, E.; Pihoker, C.; Marcovina, S.; et al. Longitudinal Changes in Arterial Stiffness and Heart Rate Variability in Youth-Onset Type 1 versus Type 2 Diabetes: The SEARCH for Diabetes in Youth Study. Diabetes Care 2022, 45, 1647–1656. [Google Scholar] [CrossRef]
- Taimour, S.; Gottsäter, A.; Jujic, A.; Nilsson, P.M. Hyperglycemia and Arterial Stiffness across Two Generations. J. Hypertens. 2021, 39, 471–475. [Google Scholar] [CrossRef]
- Wilkinson, I.B.; MacCallum, H.; Flint, L.; Cockcroft, J.R.; Newby, D.E.; Webb, D.J. The Influence of Heart Rate on Augmentation Index and Central Arterial Pressure in Humans. J. Physiol. 2000, 1, 263–270. [Google Scholar] [CrossRef]
- Bello-Chavolla, O.Y.; Almeda-Valdes, P.; Gomez-Velasco, D.; Viveros-Ruiz, T.; Cruz-Bautista, I.; Romo-Romo, A.; Sánchez-Lázaro, D.; Meza-Oviedo, D.; Vargas-Vázquez, A.; Campos, O.A.; et al. METS-IR, a Novel Score to Evaluate Insulin Sensitivity, Is Predictive of Visceral Adiposity and Incident Type 2 Diabetes. Eur. J. Endocrinol. 2018, 178, 533–544. [Google Scholar] [CrossRef] [PubMed]
- Martin, S.S.; Blaha, M.J.; Elshazly, M.B.; Brinton, E.A.; Toth, P.P.; McEvoy, J.W.; Joshi, P.H.; Kulkarni, K.R.; Mize, P.D.; Kwiterovich, P.O.; et al. Friedewald-Estimated versus Directly Measured Low-Density Lipoprotein Cholesterol and Treatment Implications. J. Am. Coll. Cardiol. 2013, 62, 732–739. [Google Scholar] [CrossRef] [PubMed]
- McEniery, C.M.; Wilkinson, I.B.; Johansen, N.B.; Witte, D.R.; Singh-Manoux, A.; Kivimaki, M.; Tabak, A.G.; Brunner, E.J.; Shipley, M.J. Nondiabetic Glucometabolic Status and Progression of Aortic Stiffness: The Whitehall II Study. Diabetes Care 2017, 40, 599–606. [Google Scholar] [CrossRef] [PubMed]
- Cavero-Redondo, I.; Martínez-Vizcaíno, V.; Álvarez-Bueno, C.; Recio-Rodríguez, J.I.; Gómez-Marcos, M.Á.; García-Ortiz, L. Relationship between Glycaemic Levels and Arterial Stiffness in Non-Diabetic Adults. Med. Clínica 2018, 150, 56–60. [Google Scholar] [CrossRef]
- De Oliveira Alvim, R.; Mourao-Junior, C.A.; de Oliveira, C.M.; de Faria Lima, R.; Horimoto, A.R.V.R.; Hong, V.A.C.; Bortolotto, L.A.; Krieger, J.E.; Pereira, A.C. Glycemic Control and Arterial Stiffness in a Brazilian Rural Population: Baependi Heart Study. Diabetol. Metab. Syndr. 2015, 7, 86. [Google Scholar] [CrossRef]
- Liang, J.; Zhou, N.; Teng, F.; Zou, C.; Xue, Y.; Yang, M.; Song, H.; Qi, L. Hemoglobin A1c Levels and Aortic Arterial Stiffness: The Cardiometabolic Risk in Chinese (CRC) Study. PLoS ONE 2012, 7, e38485. [Google Scholar] [CrossRef] [PubMed]
- Antonio-Villa, N.E.; Bello-Chavolla, O.Y.; Vargas-Vázquez, A.; Mehta, R.; Fermín-Martínez, C.A.; Martagón-Rosado, A.J.; Barquera-Guevara, D.A.; Aguilar-Salinas, C.A.; Arellano-Campos, O.; Gómez-Velasco, D.V.; et al. Increased Visceral Fat Accumulation Modifies the Effect of Insulin Resistance on Arterial Stiffness and Hypertension Risk. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 506–517. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
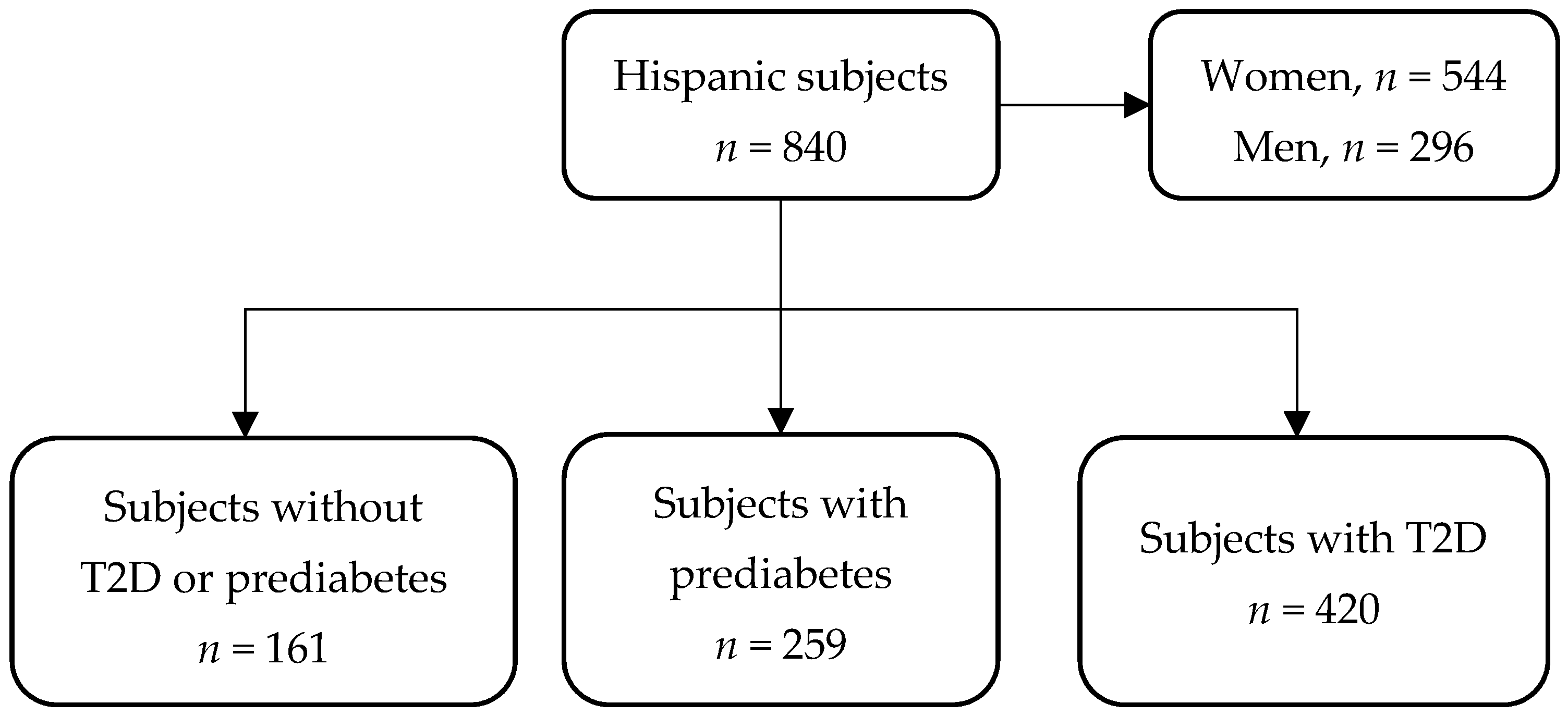
| Variables | Overall n = 840 | Without T2D or Prediabetes n = 161 | Prediabetes n = 259 | T2D n = 420 | p-Value |
|---|---|---|---|---|---|
| Age, (years) | 51 (41–59) | 44 (32–54) | 51 (41–57) | 53.5 (43–62) | <0.001 |
| Female sex, n (%) | 544 (64.8) | 110 (68.3) | 182 (70.3) | 252 (60) | 0.014 |
| HbA1c, (%) | 6.1 (5.7–7.6) | 5.4 (5.1–5.6) | 5.9 (5.7–6.1) | 7.5 (6.3–10) | <0.001 |
| FPG, (mg/dL) | 102.5 (93–127) | 92 (86–96) | 97 (91–104) | 127 (104–194.75) | <0.001 |
| TG, (mg/dL) | 161 (106.8–232.3) | 116 (78–165) | 145 (98.5–206.5) | 190 (133.5–258.8) | <0.001 |
| TC, (mg/dL) | 191 (165–223) | 186 (161–224) | 189 (167.5–217.5) | 195 (165–226) | 0.556 |
| HDL-C, (mg/dL) | 42 (36–51) | 46 (39–54) | 43 (36–52) | 42 (35–49) | <0.001 |
| LDL-C, (mg/dL) | 117.7 (96.7–140.5) | 113.8 (95.7–140.1) | 119.2 (100.3–139) | 117.5 (95.4–142.2) | 0.715 |
| non-HDL-C, (mg/dL) | 148 (123–176) | 145 (119–168) | 145 (124.5–172.5) | 151 (123.8–181.3) | 0.057 |
| RM, (mg/dL) | 27.5 (20.7–36.8) | 22.9 (16.9–29.6) | 25.4 (20–34.1) | 30.9 (23.6–39.7) | <0.001 |
| Creatinine, (mg/dL) | 0.7 (0.6–0.9) | 0.7 (0.6–0.9) | 0.7 (0.6–0.8) | 0.7 (0.6–0.9) | 0.093 |
| BMI, (kg/m2) | 28.9 (26.1–32.3) | 27.8 (24.4–31.7) | 29.5 (27.1–32.5) | 28.9 (25.9–32.4) | <0.001 |
| VFMI, (kg/m2) | 0.5 (0.3–0.6) | 0.3 (0.2–0.5) | 0.5 (0.3–0.6) | 0.5 (0.4–0.7) | <0.001 |
| METS-IR | 46.9 (40.8–53.5) | 41.6 (35.4–48.7) | 47.0 (40.7–52.6) | 48.6 (42.7–55.2) | <0.001 |
| SBP, (mmHg) | 112 (104–122) | 110 (101–116) | 112 (103–120) | 114 (106–124.5) | <0.001 |
| DBP, (mmHg) | 73 (67–80) | 71 (65–76) | 74 (67–80) | 74 (68–81) | <0.001 |
| PWV, (m/s) | 6.4 (5.6–7.3) | 5.9 (5.3–6.6) | 6.1 (5.5–6.8) | 6.8 (6–7.8) | <0.001 |
| AIX75, (%) | 34 (25–43) | 31 (21–40) | 36 (27–45) | 34 (25–44) | 0.002 |
| Buckberg SEVR | 148 (132–165) | 151 (139–170) | 153 (136.25–172) | 143 (128–158) | <0.001 |
| Outcome | β-Coefficient | 95% CI | Std Error | p-Value |
|---|---|---|---|---|
| PWV | ||||
| Model 1 | 0.179 | 0.107 to 0.252 | 0.037 | <0.001 |
| Model 2 | 0.090 | 0.034 to 0.146 | 0.028 | 0.002 |
| Model 3 | 0.077 | 0.019 to 0.134 | 0.029 | 0.009 |
| AIX75 | ||||
| Model 1 | 0.865 | −1.299 to 3.03 | 1.102 | 0.433 |
| Model 2 | −0.449 | −2.305 to 1.408 | 0.946 | 0.635 |
| Model 3 | −0.785 | −2.696 to 1.127 | 0.974 | 0.421 |
| Buckberg SEVR | ||||
| Model 1 | −0.103 | −0.179 to −0.028 | 0.038 | 0.007 |
| Model 2 | −0.035 | −0.093 to 0.023 | 0.029 | 0.234 |
| Model 3 | −0.036 | −0.096 to 0.025 | 0.031 | 0.245 |
| Outcome | ACME | ADE | Total Effect | Proportion Mediated | p-Value |
|---|---|---|---|---|---|
| PWV | 0.016 (0.004 to 0.031) | 0.07 (0.009 to 0.127) | 0.086 (0.028 to 0.14) | 0.179 (0.04 to 0.66) | 0.012 |
| MAP | 0.049 (0.03 to 0.072) | −0.027 (−0.094 to 0.036) | 0.023 (−0.041 to 0.085) | 1.114 (−16.477 to 16.505) | 0.49 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martagón, A.J.; Fermín-Martínez, C.A.; Antonio-Villa, N.E.; Mehta, R.; Almeda-Valdés, P.; Vargas-Vázquez, A.; Muñoz-Hernández, L.; Gómez-Velasco, D.V.; Elías-López, D.; Galán-Ramírez, G.A.; et al. Arterial Stiffness and HbA1c: Association Mediated by Insulin Resistance in Hispanic Adults. Int. J. Environ. Res. Public Health 2022, 19, 11017. https://doi.org/10.3390/ijerph191711017
Martagón AJ, Fermín-Martínez CA, Antonio-Villa NE, Mehta R, Almeda-Valdés P, Vargas-Vázquez A, Muñoz-Hernández L, Gómez-Velasco DV, Elías-López D, Galán-Ramírez GA, et al. Arterial Stiffness and HbA1c: Association Mediated by Insulin Resistance in Hispanic Adults. International Journal of Environmental Research and Public Health. 2022; 19(17):11017. https://doi.org/10.3390/ijerph191711017
Chicago/Turabian StyleMartagón, Alexandro J., Carlos A. Fermín-Martínez, Neftali Eduardo Antonio-Villa, Roopa Mehta, Paloma Almeda-Valdés, Arsenio Vargas-Vázquez, Liliana Muñoz-Hernández, Donají V. Gómez-Velasco, Daniel Elías-López, Gabriela A. Galán-Ramírez, and et al. 2022. "Arterial Stiffness and HbA1c: Association Mediated by Insulin Resistance in Hispanic Adults" International Journal of Environmental Research and Public Health 19, no. 17: 11017. https://doi.org/10.3390/ijerph191711017