

Occupational Safety and Health Staging Framework for Decent Work
 , , ,
, , ,  , , , ,
, , , ,  , , , , , , and
on behalf of the Workgroups on the Future of Decent Work and Demographic Changes and Occupational Healthadd
Show full author list
, , , , , , and
on behalf of the Workgroups on the Future of Decent Work and Demographic Changes and Occupational Healthadd
Show full author list
Abstract
:1. Introduction
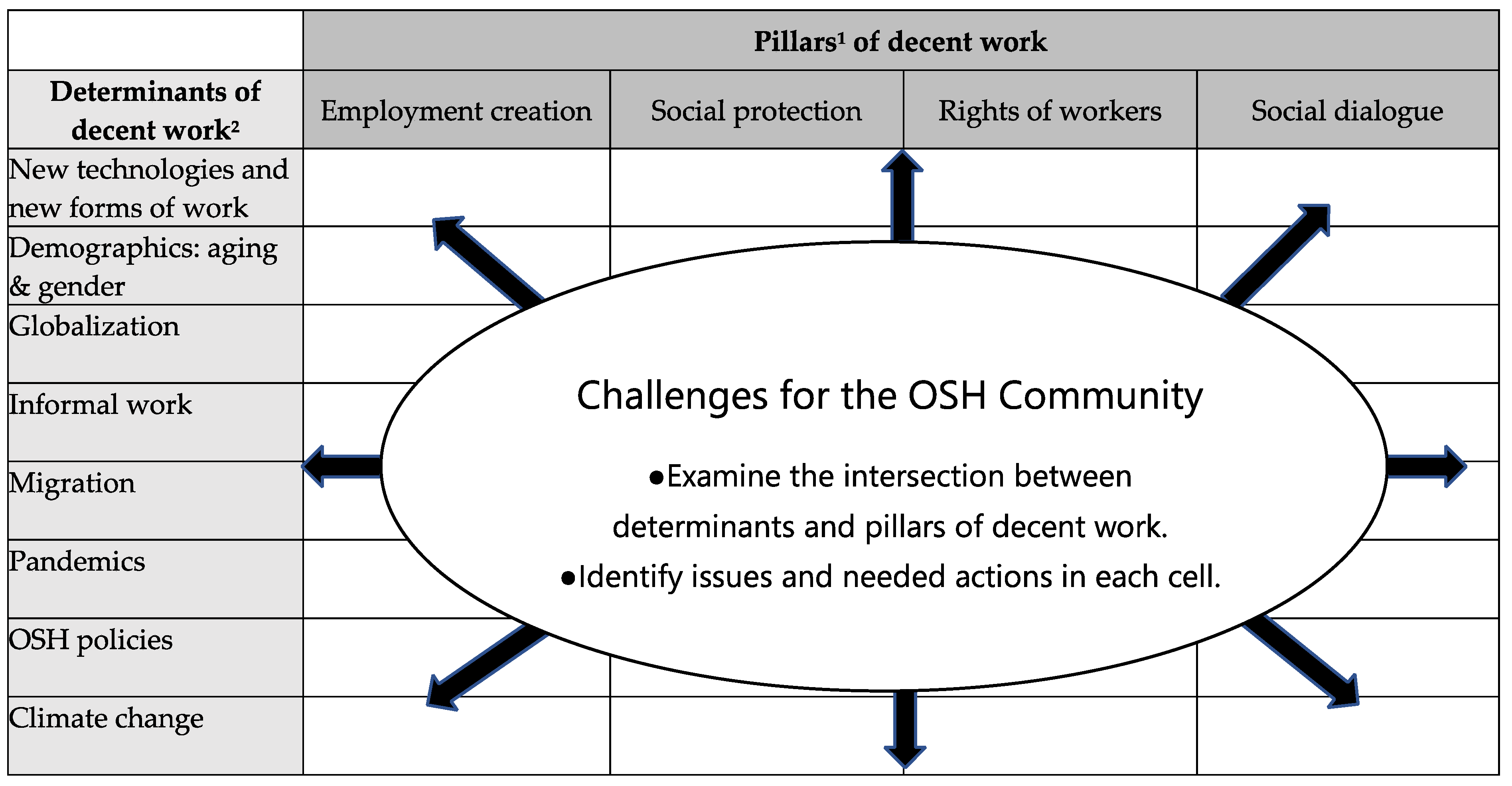
2. Pillars and Determinants of Decent Work
3. Identification of OSH Aspects of Decent Work
3.1. New Technologies and New Forms of Work
3.1.1. New Hazards from Innovative Products and Substances: The Engineered Nanomaterials
3.1.2. New Hazards from Innovative Production Processes and Work Organization: Industry 4.0
3.1.3. Emerging Physical Risks
3.1.4. Emerging Psychosocial Risks
3.2. Demographics
3.2.1. Aging
3.2.2. Gender
3.3. Globalization
3.3.1. Impact of Globalization on Work
3.3.2. Impact of Globalization on Working Conditions and Workers’ Health
3.4. Informal Work
3.5. Migrants
3.5.1. Europe
3.5.2. North America
3.5.3. South America
3.5.4. Africa
3.5.5. Asia
3.6. Pandemics
3.7. Climate Change
3.8. OSH Policies
3.8.1. Hard Law
3.8.2. Soft Law
3.8.3. Finding Balance in Hard and Soft Law Approaches
4. OSH-Related Components of the Pillars of Decent Work
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Disclaimer
References
- World Bank Group. World Development Report 2019: The Changing Nature of Work; World Bank: Washington, DC, USA, 2019. [Google Scholar]
- United Nations. Transforming Our World: The 2030 Agenda for Sustainable Development; Resolution Adopted by General Assembly; United Nations: New York, NY, USA, 2015. [Google Scholar]
- International Labour Organization (ILO). Report of the Director-General: Decent work. In Proceedings of the 87th International Labour Conference, Geneva, Switzerland, 1–17 June 1999; Available online: https://www.ilo.org/public/english/standards/relm/ilc/ilc87/rep-i.htm (accessed on 27 August 2022).
- Schulte, P.A.; Delclos, G.; Felknor, S.A.; Chosewood, L.C. Toward an expanded focus for occupational safety and health. Int. J. Environ. Res. Public Health 2019, 16, 4946. [Google Scholar] [CrossRef] [PubMed]
- Lemke, M.T.L. Is the Total Worker Health Program missing its mark? Integrating complex systems approaches to unify visions. JOEM 2021, 63, e304–e307. [Google Scholar]
- Black, C. Working for a Healthier Tomorrow; The Stationary Office: London, UK, 2008. [Google Scholar]
- Howard, J. Nonstandard work arrangements and worker health and safety. Am. J. Ind. Med. 2017, 60, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Harrison, J.; Dawson, L. Occupational health: Meeting the challenges of the next 20 years. Saf. Health Work 2016, 7, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Peckham, T.T.; Baker, M.G.; Camp, J.E.; Kaufman, J.D.; Sexias, N.S. Creating the Future for Occupational Health. Ann. Work. Expo. Health 2017, 61, 3–15. [Google Scholar] [PubMed]
- Kang, S.K. New Concept for Occupational Health Development: 3 Phases. Ind. Health 2015, 53, 109–111. [Google Scholar] [CrossRef] [PubMed]
- Rantanen, J. Research challenges arising from changes in work life. Scand. J. Work Environ. Health 1999, 25, 473–483. [Google Scholar] [CrossRef]
- Felknor, S.A.; Streit, J.M.K.; Chosewood, L.C.; McDaniel, M.; Schulte, P.A.; Delclos, G.L. How will the future of work shape the OSH professional of the future? A workshop summary. Int. J. Environ. Res. Public Health 2020, 17, 7154. [Google Scholar] [CrossRef]
- Felknor, S.A.; Streit, J.M.H.; McDaniel, M.; Schulte, P.A.; Chosewood, L.C.; Delclos, G.L. How will the future work shape OSH research and practice? A workshop summary. Int. J. Environ. Res. Public Health 2021, 18, 5696. [Google Scholar] [CrossRef]
- Guillemin, M. Lesser Known Aspects of Occupational Healt; L’Harmattan: Paris, France, 2011. (In French) [Google Scholar]
- Naryani, R.J.; Nielson, K.; Daniels, K.; Donaldson-Feilder, E.J.; Lewis, R.C. Out of sight and out of mind P. A. literature review of occupational safety and health leadership and management of distributed workers. Work Stress 2018, 32, 124–146. [Google Scholar] [CrossRef]
- Lerouge, L. (Ed.) Psychosocial Risks in Labour and Social Security Law: A Comparative Legal Overview from Europe, North America, Australia and Japan; Springer International Publishing AG: Paris, France, 2017. [Google Scholar]
- Navarro, V.; Muntaner, C. Political and Economic Determinants of Population Health and Well-Being: Controversies and Developments; Baywood Publishing Co., Inc.: Amityville, NY, USA, 2004; p. 575. [Google Scholar]
- Härma, M.; Kompier, M.A.J.; Vahtera, J. Work—Related stress and health—Risks, mechanisms and couuter measures. Scan. J. Work Environ. Health 2006, 32, 413–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chia, G.; Um, S.M.; Sng, G.K.I.; Hwang, Y.J.; Chia, K.S. Need for a new work place safety and health (WSH) strategy for the Fourth Industrial Revolution. Am. J. Ind. Med. 2017, 62, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Murashov, V.; Hearl, F.; Howard, J. Working safely with robot workers: Recommendations for the new workplace. J. Occup. Environ. Hyg. 2016, 13, 61–71. [Google Scholar] [CrossRef] [PubMed]
- Lucchini, R.G.; London, L. Global occupational health: Current challenges and the need for urgent action. Ann. Glob. Health 2014, 80, 251–256. [Google Scholar] [CrossRef] [PubMed]
- Balliester, T.; Elsheikhi, A. The Future of Works a Literature Review; Working Paper 29; International Labor Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Karasek, R.; Theorell, T. Healthy Work: Stress, Productivity, and the Reconstruction of Working Life; Basic Books: New York, NY, USA, 1990. [Google Scholar]
- Blustein, D.L.; Olle, C.; Connors-Kellgren, A.; Diamonti, A.J. Decent work: A psychological perspective. Front. Psychol. 2016, 7, 407. [Google Scholar] [CrossRef]
- Hudson, H.L.; Nigam, J.A.S.; Sauter, S.L.; Chosewood, L.C.; Schill, A.L.; Howald, J. Total Worker Health; American Psychological Association: Washington, DC, USA, 2019. [Google Scholar] [CrossRef]
- Burton, J. Healthy Workplaces: A Model of Action for Employers, Workers, Policy-Makers and Practitioners; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Jain, A.; Leka, S.; Zwetsloot, G. Managing Health, Safety and Well-Being: Ethics, Responsibility and Sustainability. Part of Aligning Perspectives in Health, Safety and Well-Being; Springer: Dordrecht, The Netherlands, 2018. [Google Scholar]
- Gervais, R.; Buffet, M.-A.; Liddle, M.; Eekelaert, L. Well-Being at Work: Creating a Positive Work Environment; European Agency for Safety and Health at Work: Bilbao, Spain, 2019. [Google Scholar]
- Zwetsloot, G.I.J.M.; van Scheppingen, A.R.; Bos, E.H.; Dijkman, A. The core values that support health, safety, and well-being at work. Saf. Health Work 2013, 4, 187–196. [Google Scholar] [CrossRef]
- Schulte, P.A.; Vainio, H. Well-being at work—Overview and perspective. Scand. J. Work Environ. Health 2010, 36, 422–429. [Google Scholar] [CrossRef]
- Pot, F. Workplace innovation and wellbeing at work. In Workplace Innovation: Theory, Research and Practice. Part of Aligning Perspectives on Health, Safety and Well-Being; Oeij, P.R.A., Rus, D., Pot, F.D., Eds.; Springer: Dordrecht, The Netherlands, 2017; pp. 95–110. [Google Scholar]
- Podgórski, D.; Majchrzycka, K.; Dąbrowska, A.; Gralewicz, G.; Okrasa, M. Towards a conceptual framework of OSH risk management in smart working environments based on smart PPE, ambient intelligence and the Internet of Things technologies. Int. J. Occup. Saf. Ergon. 2017, 23, 1–20. [Google Scholar] [CrossRef]
- Rain, J.S.; Lane, I.M.; Steiner, D.D. A current look at the job satisfaction/life satisfaction relationship: Review and future considerations. Hum. Relat. 1991, 44, 287–307. [Google Scholar] [CrossRef]
- Schulte, P.A.; Murashov, V.; Zumwalde, R.; Kuempel, E.D.; Geraci, C. Occupational exposure limits for nanomaterials: State of the art. J. Nanopart Res. 2010, 12, 1971–1987. [Google Scholar] [CrossRef]
- NPD (Nanotechnology Products Database). StatNano Nanotechnology Database. Available online: https://product.statnano.com/ (accessed on 20 October 2019).
- Iavicoli, I.; Fontana, L.; Pingue, P.; Todea, A.M.; Asbach, C. Assessment of occupational exposure to engineered nanomaterials in research laboratories using personal monitors. Sci. Total Environ. 2018, 627, 689–702. [Google Scholar] [CrossRef] [PubMed]
- Roth, G.A.; Geraci, C.L.; Stefaniack, A.; Murashov, V.; Howard, J. Potential occupational hazards of additive manufacturing. J. Occup. Environ. Hyg. 2019, 16, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Leso, V.; Fontana, L.; Mauriello, M.C.; Iavicoli, I. Occupational risk assessment of engineered nanomaterials: Limits, challenges and opportunities. Curr. Nanosci. 2017, 13, 55–78. [Google Scholar] [CrossRef]
- Fadeel, B.; Pietroiusti, A.; Shvedova, A.A. Adverse Effects of Engineered Nanomaterials: Exposure, Toxicology, and Impact on Human Health, 2nd ed.; Academic Press: London, UK, 2017. [Google Scholar]
- Dobrovolskaia, M.A.; Shurin, M.; Shvedova, A.A. Current understanding of interactions between nanoparticles and the immune system. Toxicol. Appl. Pharmacol. 2016, 299, 78–89. [Google Scholar] [CrossRef]
- Donaldson, K.; Duffin, R.; Langrish, J.P.; Miller, M.R.; Mills, N.L.; Poland, C.A.; Raftis, J.; Shah, A.; Shaw, C.A.; Newby, D.E. Nanoparticles and the cardiovascular system: A critical review. Nanomedicine 2013, 8, 403–423. [Google Scholar] [CrossRef]
- Feng, X.; Chen, A.; Zhang, Y.; Wang, J.; Shao, L.; Wei, L. Central nervous system toxicity of metallic nanoparticles. Int. J. Nanomed. 2015, 10, 4321–4340. [Google Scholar] [CrossRef]
- Iavicoli, I.; Fontana, L.; Leso, V.; Bergamaschi, A. The effects of nanomaterials as endocrine disruptors. Int. J. Mol. Sci. 2013, 14, 16732–16801. [Google Scholar] [CrossRef]
- Iavicoli, I.; Fontana, L.; Nordberg, G. The effects of nanoparticles on the renal system. Crit. Rev. Toxicol. 2016, 46, 490–560. [Google Scholar] [CrossRef]
- Lu, X.; Zhu, T.; Chen, C.; Liu, Y. Right or left: The role of nanoparticles in pulmonary diseases. Int. J. Mol. Sci. 2014, 15, 17577–17600. [Google Scholar] [CrossRef]
- Iavicoli, I.; Leso, V.; Fontana, L.; Bergamaschi, A. Toxicological effects of titanium dioxide nanoparticles: A review of in vitro mammalian studies. Eur. Rev. Med. Pharmacol. Sci. 2011, 15, 481–508. [Google Scholar]
- Iavicoli, I.; Farina, M.; Fontana, L.; Lucchetti, D.; Leso, V.; Fanali, C.; Cufino, V.; Boninsegna, A.; Leopold, K.; Schindl, R.; et al. In vitro evaluation of the potential toxic effects of palladium nanoparticles on fibroblasts and lung epithelial cells. Toxicol. In Vitro 2017, 42, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Leso, V.; Fontana, L.; Iavicoli, I. The occupational health and safety dimension of Industry 4.0 and occupational health. Med. Lav. 2018, 109, 327–338. [Google Scholar]
- Schulte, P.; Leso, V.; Niang, N.; Iavicoli, I. Biological monitoring of workers exposed to engineered nanoparticles. Toxicol. Lett. 2018, 278, 112–124. [Google Scholar] [CrossRef] [PubMed]
- Asbach, C.; Alexander, C.; Clavaguera, S.; Dahmann, D.; Dozol, H.; Faure, B.; Fierz, M.; Fontana, L.; Iavicoli, I.; Kaminski, H.; et al. Review of measurement techniques and methods for assessing personal exposure to airborne nanomaterials in workplaces. Sci. Total. Environ. 2017, 603–604, 793–806. [Google Scholar] [CrossRef]
- ERPS (European Parliamentary Research Service). Industry 4.0: Digitalisation for Productivity and Growth. Available online: http://www.europarl.europa.eu/RegData/etudes/BRIE/2015/568337/EPRS_BRI(2015)568337_EN.pdf (accessed on 27 August 2022).
- Mosconi, F. The New European Industrial Policy: Global Competitiveness and the Manufacturing Renaissance; Routledge: London, UK, 2015. [Google Scholar]
- Pereira, A.C.; Romero, F. A review of the meanings and implications of Industry 4.0 concept. Proc. Manuf. 2017, 13, 1206–1214. [Google Scholar] [CrossRef]
- Lu, Y. Industry 4.0: A survey on technologies, applications and open research issues. J. Ind. Inf. Integr. 2017, 6, 1–10. [Google Scholar] [CrossRef]
- Badri, A.; Boudreau-Trudel, B.; Souissi, A.S. Occupational health and safety in the industry 4.0 era: A cause for major concern? Saf. Sci. 2018, 109, 403–411. [Google Scholar] [CrossRef]
- Fernández, F.B.; Pérez, M.A.S. Analysis and modeling of new and emerging occupational risks in the context of advanced manufacturing processes. Procedia Eng. 2015, 100, 1150–1159. [Google Scholar] [CrossRef]
- Parker, S.K.; Grote, G. Automation, algorithms, and beyond: Why work design matters more than ever in a digital world. Appl. Psychol. 2019, 1–45. [Google Scholar] [CrossRef]
- Acemoglu, D.; Restrepo, P. The Wrong Kind of AI? Artificial Intelligence and the Future of Labor Demand (NBER Working Paper No. 25682); National Bureau of Economic Research: Cambridge, MA, USA, 2019. [Google Scholar]
- Autor, D.; Mindell, D.A.; Reynolds, E.B. The Work of the Future: Shaping Technology and Institutions; Massachusetts Institute of Technology: Cambridge, MA, USA, 2019. [Google Scholar]
- Breque, M.; De Nul, L.; Petridis, A. Industry 5.0. Towards a Sustainable, Human-Centric and Resilient European Industry; European Commission: Brussels, Belgium, 2021. [Google Scholar]
- Oshio, T.; Tsutumi, A.; Inoue, A. The association between job stress and leisure—Time physical inactivity adjusted for individual attributes: Evidence from a Japanese Occupational Cohort Survey. Scan. J. Work Environ. Health 2016, 42, 225–236. [Google Scholar] [CrossRef]
- Trost, S.G.; Owen, N.; Bauman, A.E.; Sallis, J.F.; Brown, W. Correlates of adult participation in physical activity: Review and update. Med. Sci. Sports Exerc. 2002, 34, 1996–2001. [Google Scholar] [CrossRef]
- Department of Health. At Least Five a Week: Evidence on the Impact of Physical Activity and Its Relationship to Health. A Report from the Chief Medical Officer; Department of Health: London, UK, 2004. [Google Scholar]
- EU-OSHA (European Agency for Safety and Health at Work). OSH in Figures: Stress at Work—Facts and Figures; Publications Office of the European Communities: Luxembourg, 2009. [Google Scholar]
- Guduru, R.K.R.; Domeika, A.; Obcarskas, L.; Ylaite, B. The ergonomic association between shoulder, neck/head disorders and sedentary activity: A systematic review. J. Healthc. Eng. 2022, 2022, 5178333. [Google Scholar] [CrossRef] [PubMed]
- Korhonen, T.; Ketola, R.; Toivonen, R.; Luukkonen, R.; Hakkanen, M.; Vii, X.; Juntura, E. Work related and individual predictors for incident neck pain among office employees working with video display units. Occup. Environ. Med. 2003, 60, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; McDonald, J.C.; Cherry, N.M. Incidence and suspected cause of work-related musculoskeletal disorders, United Kingdom, 1996–2001. Occup. Med. 2006, 56, 406–413. [Google Scholar] [CrossRef]
- Steensma, I.A.; Verbeek, J.H.; Heymans, M.W.; Bongers, P.M. Prognostic factors for duration of sick leave in patients sick listed with acute low back pain: A systematic review of the literature. Occup. Environ. Med. 2005, 62, 851–860. [Google Scholar] [CrossRef] [PubMed]
- EU-OSHA (European Agency for Safety and Health at Work). Foresight on New and Emerging Occupational Safety and Health Risks Associated with Digitalisation by 2025. European Risk Observatory Report; Publications Office of the European Union: Luxembourg, 2018. [Google Scholar]
- Yildirim, C. Don’t make me sick: Investigating the incidence of cybersickness in commercial virtual reality headsets. Virtual Real. 2020, 24, 231–239. [Google Scholar] [CrossRef]
- Lager, H.; Virgillito, A.; Buchberger, T.-P. Digitalization of Logistics Work: Ergonomic Improvements Versus Work Intensification. In Digital Supply Chains and the Human Factor; Springer: Berlin/Heidelberg, Germany, 2021; p. 49. [Google Scholar]
- Bongers, P.M.; de Winter, C.V.R.; Kompier, M.A.; Hildebrandt, V.H. Epidemiology of work related neck and upper limb problems: Psychosocial and personal risk factors (part I) and effective interventions from a biobehavioral perspective (part II). J. Occup. Rehab. 2009, 16, 272–295. [Google Scholar] [CrossRef]
- Eatough, E.; Way, J.; Chang, C.H. Understanding the link between psychosocial work-stressors and work-related musculoskeletal complaints. Appl. Ergon. 2012, 43, 554–563. [Google Scholar] [CrossRef]
- European Agency for Safety and Health at Work (EU-OSHA). Priorities for Occupational Safety and Health Research in the EU-25; Publications Office of the European Communities: Luxembourg, 2005. [Google Scholar]
- Oakman, J.; Chan, S. Risk management: Where should we target strategies to reduce work-related musculoskeletal disorders? Saf. Sci. 2015, 73, 99–105. [Google Scholar] [CrossRef]
- Citi GPS. Technology at Work v5.0: A New World of Remote Work. 2020. Available online: https://ir.citi.com/td2TMf%2FvvpzNPqaucEszMhDfq%2Fq%2ByImXWvzH61WVNip7Ecd1v7edrIrz6nCHdxkoR2AmAYyMDa4%3D (accessed on 27 August 2022).
- Litchfield, P.; Cooper, C.; Hancock, C.; Watt, P. Work and wellbeing in the 21st century. Int. J. Environ. Res. Public Health 2016, 13, 1065. [Google Scholar] [CrossRef]
- Benach, J.; Vives, A.; Amable, M.; Vanroelen, C.; Tarafa, G.; Muntaner, C. Precarious employment: Understanding an emerging social determinant of health. Ann. Rev. Public Health 2014, 35, 229–253. [Google Scholar] [CrossRef] [PubMed]
- Rajani, N.B.; Giannakopoulos, G.; Filippidis, F.T. Job insecurity, financial difficulties and mental health in Europe. Occup. Med. 2016, 66, 681–683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ravalier, J.M. Care Worker Wellbeing and Zero-Hours Contracts; Richard Benjamin Trust: London, UK, 2019. [Google Scholar]
- Leka, S. The Future of Working in a Virtual Environment and OSH; EU-OSHA Discussion Paper; European Agency for Safety and Health at Work: Bilbao, Spain, 2021; Available online: https://osha.europa.eu/en/publications/future-working-virtual-environment-and-occupational-safety-and-health (accessed on 27 August 2022).
- Fast-Berglund, Å.; Palmkvist, F.; Nyqvist, P.; Ekered, S.; Åkerman, M. Evaluating cobots for final assembly. Procedia CIRP 2016, 44, 175–180. [Google Scholar] [CrossRef]
- Van de Perre, G.; El Makrini, I.; Van Acker, B.B.; Saldien, J.; Vergara, C.; Pintelon, L.; Chemweno, P.; Weuts, R.; Moons, K.; Dewil, R.; et al. Improving productivity and worker conditions in assembly. Part 1-A: Collaborative architecture and task allocation. In Towards a Robotic Society, Proceedings of the 2018 IEEE/RSJ International Conference on Intelligent Robots and Systems, IROS 2018, Madrid, Spain, 1–5 October 2018; IEEE: Piscataway, NJ, USA, 2018. [Google Scholar]
- Ertel, M.; Pech, E.; Ullsperger, P. Working hours and health in flexible work arrangements. In Occupational Health Psychology: Europe 2001; Weikert, C., Torkelson, E., Pryce, J., Eds.; I-WHO Publications: Nottingham, UK, 2001. [Google Scholar]
- De Cuyper, N.; De Jong, J.; De Witte, H.; Isaksson, K.; Rigotti, T.; Schalk, R. Literature review of theory and research on the psychological impact of temporary employment: Towards a conceptual model. Int. J. Mgmt. Rev. 2008, 10, 25–51. [Google Scholar] [CrossRef]
- Greely, H.; Sahakian, B.; Harris, J.; Kessler, R.C.; Gozzanige, M.; Campbell, P.; Farah, M.J. Towards responsible use of cognitive-enhancing drugs by the healthy. Nature 2008, 456, 702–705. [Google Scholar] [CrossRef] [PubMed]
- Quinlan, M.; Mayhew, C.; Bohle, P. The global expansion of precarious employment, work disorganization, and consequences for occupational health: A review of recent research. Int. J. Health Serv. 2001, 31, 335–414. [Google Scholar] [CrossRef]
- Viale Pereira, G.; Estevez, E.; Cardona, D.; Chesñevar, C.; Collazzo-Yelpo, P.; Cunha, M.A.; Diniz, E.H.; Ferraresi, A.A.; Fischer, F.M.; Cardinelle Oliveira Garcia, F.; et al. South American Expert Roundtable: Increasing Adaptive Governance Capacity for Coping with Unintended Side Effects of Digital Transformation. Sustainability 2020, 12, 718. [Google Scholar] [CrossRef]
- Moore, P. OSH and the Future of Work: Benefits and Risks of Artificial Intelligence Tools in Workplaces; EU-OSHA (European Agency for Safety and Health at Work) Discussion Paper; European Agency for Safety and Health at Work: Bilbao, Spain, 2019; Available online: https://osha.europa.eu/en/publications/osh-and-future-work-benefits-and-risks-artificial-intelligence-tools-workplaces/view (accessed on 27 August 2022).
- Schulte, P.A.; Streit, J.M.K.; Sheriff, F.; Delclos, G.; Felknor, S.A.; Tamers, S.L.; Fendinger, S.; Grosch, J.; Sala, R. Potential scenarios and hazards in the work of the future: A systematic review of the peer-reviewed literature and gray literatures. Ann. Work Exp. Health 2021, 64, 786–816. [Google Scholar] [CrossRef]
- Dollard, M.F.; Nesser, D. The Conundrum of Work Stress; International Labour Organization: Geneva, Switzerland, 2019; Available online: https://www.ilo.org/global/topics/safety-and-health-at-work/events-training/events-meetings/world-day-for-safety/33thinkpieces/WCMS_681594/lang--en/index.htm (accessed on 27 August 2022).
- Niedhammer, I.; Bertrais, S.; Witt, K. Psychosocial work exposures and health outcomes: A meta-review of 72 literature reviews with meta-analysis. Scand. J. Work Environ. Health 2021, 47, 489–508. [Google Scholar] [CrossRef]
- Dhondt, S.; Kraan, K.O.; Bal, M. Organisation, technological change and skills use over time: A longitudinal study on linked employee surveys. New Technol. Work. Employ. 2021, 1–20. [Google Scholar] [CrossRef]
- Dollard, M.F.; Karasek, R. Building psychosocial safety climate. Evaluation of a socially coordinated PAR risk management stress prevention study. In Contemporary Occupational Health Psychology: Global Perspective on Research and Practice; Houdmont, J., Leka, S., Eds.; Wiley-Blackwell: Chichester, UK, 2010; pp. 208–233. [Google Scholar]
- Bailey, T.S.; Dollard, M.F.; Richards, P.A. A national standard for psychological safety climate (PSC): PSC 41 as the benchmark for low risk of job strain and depressive symptoms. J. Occup. Health Psychol. 2015, 20, 15–26. [Google Scholar] [CrossRef]
- Deloitte Access Economics. Occupational Health and Safety (Psychological Health) Regulations Amendment 2022. Regulatory Impact Statement; Deloitte Access Economics: Melbourne, Australia, 2022. [Google Scholar]
- Fischer, F.M.; Martinez, M.C.; Alfredo, C.H.; Silva-Junior, J.S.; Oakman, J.; Cotrim, T.; Fisher, D.; Popkins, S.; Petery, G.A.; Schulte, P.A. Aging and the future of decent work. J. Environ. Res. Public Health 2021, 18, 8898. [Google Scholar] [CrossRef] [PubMed]
- Cedefop. Empowering Adults through Upskilling and Reskilling Pathways. Volume 1: Adult Populations with Potential for Upskilling and Reskilling; Cedefop Reference Series, No. 112; Publication Office of the European Union: Luxembourg, 2020; Available online: http://data.europa.eu/doi/10.2801/691134 (accessed on 27 August 2022).
- Foresight Alliance. The Future of Work; Foresight Alliance LLC: Washington, DC, USA, 2016. [Google Scholar]
- White, M.S.; Burns, C.; Conlon, H.A. The impact of an aging population in the workplace. Workplace Health Saf. 2018, 66, 493–498. [Google Scholar] [CrossRef]
- Schulte, P.A.; Grosch, J.; Scholl, J.C.; Tamers, S.L. Framework for considering productive aging and work. JOEM 2018, 60, 440–448. [Google Scholar] [CrossRef] [PubMed]
- Petery, G.A. Understanding Workplace Ageism. October 2021. Available online: https://blogs.cdc.gov/niosh-science-blog/2021/10/01/ageism/ (accessed on 27 August 2022).
- International Labour Office. 24. Youth Employment (Decent Work for Sustainable Development (DW4SD) Resource Platform). Available online: https://www.ilo.org/global/topics/dw4sd/themes/youth-employment/lang--en/index.htm#:~:text=Youth%20employment%20is%20not%20just%20about%20jobs%3B%20youth,work%20as%20well%3A%20rights%2C%20protection%2C%20voice%20and%20representation (accessed on 30 June 2022).
- World Bank. Female Labor Force Participation. 9 January 2022. Available online: https://genderdata.worldbank.org/data-stories/fffp-data-story/ (accessed on 27 August 2022).
- Trask, B.S. Women, Work and Globalization; Taylor Francis: New York, NY, USA, 2013. [Google Scholar]
- Messing, K.; Mager, S.J. Set gender and women’s occupational health: The importance of considering mechanism. Environ. Res. 2006, 101, 149–162. [Google Scholar] [CrossRef]
- Mourshed, M. The economic impact of ageism. Podcast, 19 November 2021. Available online: https://www.mckinsey.com/about-us/social-responsibility/the-economic-impact-of-ageism (accessed on 27 August 2022).
- Hooftman, W.E.; van Poppel, M.N.; van der Beek, A.J.; Bongers, P.M.; van Mechelen, W. Gender differences in the relations between work-related physical and psychosocial risk factors and musculoskeletal complaints. Scand. J. Work Environ. Health 2004, 30, 261–278. [Google Scholar] [CrossRef]
- Gochfield, M. Framework for gender differences in human and animal toxicology. Environ. Res. 2007, 104, 4–21. [Google Scholar] [CrossRef] [PubMed]
- Habib, R.R.; Hojeij, S.; Elzen, K. Gender in occupational health research of farmworkers: A systematic review. Am. J. Ind. Med. 2014, 57, 1344–1367. [Google Scholar] [CrossRef]
- Brussevich, M.; Dable-Noriss, M.; Kamunge, C.; Karnane, P.; Khalid, S.; Kochhar, K. Gender, Technology and the Future of Work. Report No. SDN 18/07; International Monetary Fund: Washington, DC, USA, 2018. [Google Scholar]
- Scapellato, M.L.; Basso, A.; Bonfiglioli, R.; Foddis, R.; Larese-Filon, F.; Simonini, S.; Spatari, G.; Tomao, P.; Verso, M.G. Health and work in a gender perspective. G. Ital. Med. Lav. Ergon. 2017, 39, 203–210. [Google Scholar]
- Campos-Serna, J.; Ronda-Pérez, E.; Artazcoz, L.; Moen, B.E.; Benavides, F.G. Gender inequalities in occupational health related to the unequal distributions of working and unemployment conditions: A systematic review. Int. J. Equit. Health 2013, 12, 57. [Google Scholar] [CrossRef]
- International Labour Organization (ILO). OSH Practice—Guidelines for Gender Mainstreaming in Occupational Safety and Health; International Labour Organization: Geneva, Switzerland, 2013. [Google Scholar]
- United Nations Conference on Trade and Development (UNCTAD). Development and Globalization: Facts and Figures; UNCTAD’s Division on Globalization and Development Strategies: New York, NY, USA; Geneva, Switzerland, 2004. [Google Scholar]
- Drager, N.; Beaglehole, R. Globalization: Changing the public health landscape. Bull. World Health Organ. 2001, 79, 803. [Google Scholar]
- Lee, K.; Buse, K.; Fustukian, S. Health Policy in a Globalising World; Cambridge University Press: Cambridge, UK, 2002. [Google Scholar]
- Van der Hoeven, R. Globalization of Work; United Nations Development Programme, Human Development Report Office: New York, NY, USA, 2015; Available online: http://hdr.undp.org/en/content/globalization-work (accessed on 27 August 2022).
- United Nations Development Programme (UNDP). Human Development Report 1999; Oxford University Press: New York, NY, USA, 1999. [Google Scholar]
- Cornia, G.A. Globalization and health: Results and options. Bull. World. Health Organ. 2001, 79, 834–841. [Google Scholar] [PubMed]
- Bach, S. Globalization and health. Bull. World Health Organ. 2007, 85, 897. [Google Scholar] [CrossRef]
- International Labour Organization (ILO). World Employment and Social Outlook—Trends 2019. Available online: https://www.ilo.org/wcmsp5/groups/public/---dgreports/---dcomm/---publ/documents/publication/wcms_670542.pdf (accessed on 27 August 2022).
- Crotti, R.; Pal, K.K.; Ratcheva, V.; Zahidi, S. Global Gender Gap Report 2021; Insight Report; World Economic Forum: Geneva, Switzerland, 2021. [Google Scholar]
- International Labour Organization (ILO). Decent Work and Transition to Address Climate Change. 13 October 2015. Available online: https://www.ilo.org/global/topics/green-jobs/news/WCMS_419794/lang--en/index.htm (accessed on 27 August 2022).
- Arnold, D.; Bongiovi, J.R. Precarious, informalizing, and flexible work: Transforming concepts and understandings. Am. Behav. Sci. 2013, 57, 289–308. [Google Scholar] [CrossRef] [Green Version]
- Caldbick, S.; Labonte, R.; Mohindra, K.S.; Ruckert, A. Globalization and the rise of precarious employment: The new frontier for workplace health promotion. Glob. Health Promot. 2014, 21, 23–31. [Google Scholar] [CrossRef]
- Torp, S.; Reierspa, J. Globalization, work and health: A Nordic perspective. Int. J. Environ. Res. Public Health 2020, 17, 7661. [Google Scholar] [CrossRef]
- International Labour Organization (ILO). Globalization and Informal Jobs in Developing Countries; International Labour Organization and World Trade Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Gonzales, F.; Jensen, J.B.; Kim, Y.; Nordås, H.K. Globalisation of Services and Jobs. In Policy Priorities for International Trade and Jobs; Lippoldt, D., Ed.; Organisation for Economic Co-Operation and Development (OECD): Paris, France, 2012; pp. 175–192. [Google Scholar]
- Cowling, K.; Thow, A.M.; Pollack Porter, K. Analyzing the impacts of global trade and investment on non-communicable diseases and risk factors: A critical review of methodological approaches used in quantitative analyses. Glob. Health 2018, 14, 53. [Google Scholar] [CrossRef]
- Loewenson, R. Globalization and occupational health: A perspective from southern Africa. Bull. World Health Organ. 2001, 79, 863–868. [Google Scholar]
- Baram, M. Globalization and workplace hazards in developing nations. Saf. Sci. 2009, 47, 756–766. [Google Scholar] [CrossRef]
- Johnson, J.V. Globalization, workers’ power and the psychosocial work environment: Is the demand-control support model still useful in a neoliberal era? Scand. J. Work Environ. Health 2008, 34, 15–21. [Google Scholar]
- Sauter, S.; Murphy, L. Monitoring the changing organization of work: International practices and new. Soz. Praventivmed. 2003, 48, 341–360. [Google Scholar] [CrossRef]
- NIOH (National Institute for Occupational Health). Informal Economy. Available online: https://www.nioh.ac.za/informal-economy/ (accessed on 27 August 2022).
- Chen, M.A. The Informal Economy: Definitions, Theories and Policies; Women in Informal Employment Globalizing and Organizing (WIEGO): Cambridge, MA, USA, 2012. [Google Scholar]
- Bitran, R. Universal Health Coverage and the Challenge of Informal Employment: Lessons from Developing Countries; Health, Nutrition, and Population (HNP) Discussion Paper; The International Bank for Reconstruction and Development/World Bank: Washington, DC, USA, 2014. [Google Scholar]
- Rockefeller Foundation. Ideo.org: A Human Lens on the Lives of Informal Workers, Supported by the Rockefeller Foundation. Available online: https://www.rockefellerfoundation.org/wp-content/uploads/A-Human-Lens-on-the-Life-of-Informal-Workers.pdf (accessed on 27 August 2022).
- International Labour Organization (ILO). Women and Men in the Informal Economy: A Statistical Picture, 3rd ed.; International Labour Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Ma, R.; Zhong, S.; Morabito, M.; Hajat, S.; Xu, Z.; He, Y.; Bao, J.; Sheng, R.; Li, C.; Fu, C.; et al. Estimation of work-related injury and economic burden attributable to heat stress in Guangzhou, China. Sci. Total Environ. 2019, 666, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Lucas, R.A.; Epstein, Y.; Kjellstrom, T. Excessive occupational heat exposure: A significant ergonomic challenge and health risk for current and future workers. Extrem. Physiol. Med. 2014, 3, 14. [Google Scholar] [CrossRef] [PubMed]
- Boiano, J.M.; Silver, S.R.; Tsai, R.J.; Sanderson, W.T.; Liu, S.; Whitehead, L.W. Development of job exposure matrices to estimate occupational exposure to solar and artificial ultraviolet radiation. Ann. Work Expo. Health 2020, 64, 936–943. [Google Scholar] [CrossRef] [PubMed]
- Machado, T.; Sathyanarayanan, V.; Bhola, P.; Kamath, K. Psychological vulnerability, burnout, and coping among employees of a business process outsourcing organization. Ind. Psychiatry J. 2013, 22, 26–31. [Google Scholar] [CrossRef]
- Rocha, M.R.A.; Marin, M.J.S.; Macias-Seda, J. Living, working conditions and mental health: A study with Brazilian and Spanish workers who work in hospital cleaning services. Cien. Saude Colet. 2020, 25, 3821–3832. [Google Scholar] [CrossRef]
- Shwetha, B.; Sudhakar, H. Influence of shift work on cognitive performance in male business process outsourcing employees. Indian J. Occup. Environ. Med. 2012, 16, 114–118. [Google Scholar] [CrossRef]
- PISAT (Programa Integrado em Saúde Ambiental e do Trabalhador). Boletim Epidemiológico—Ocupação e Suicídio No Brasil, 2007–2015, 14th ed.; PISAT: Salvador, Brazil, 2019; Available online: http://www.ccvisat.ufba.br/wp-content/uploads/2019/08/SUICIDIO_BOLETIM_CCVISATfinalFINAL.pdf (accessed on 27 August 2022). (In Portuguese)
- Klingelschmidt, J.; Milner, A.; Khireddine-Medouni, I.; Witt, K.; Alexopoulos, E.C.; Toivanen, S.; LaMontagne, A.D.; Chastang, J.F.; Niedhammer, I. Suicide among agricultural, forestry, and fishery workers: A systematic literature review and meta-analysis. Scand. J. Work Environ. Health 2018, 44, 3–15. [Google Scholar] [CrossRef]
- Pereira, E.C.; Ferreira, A.P.S.S.; Sato, A.P.S.; Fischer, F.M.; Olympio, K.P.K. Home-based outsourced informal work by children and adolescents impacts sleep and leisure—A preliminary study. Environ. Sci. Pollut. Res. 2020, 27, 32754–32761. [Google Scholar] [CrossRef]
- Santana, V.S.; Kiss, L.; Andermann, A. The scientific knowledge on child labor in Latin America. Cad. Saude Publica 2019, 35, e00105119. [Google Scholar] [CrossRef]
- Skalny, A.V.; Lima, T.R.R.; Ke, T.; Zhou, J.C.; Bornhorst, J.; Alekseenko, S.I.; Aaseth, J.; Anesti, O.; Sarigiannis, D.A.; Tsatsakis, A.; et al. Toxic metal exposure as a possible risk factor for COVID-19 and other respiratory infectious diseases. Food Chem. Toxicol. 2020, 146, 111809, Erratum in 2021, 147, 111999. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, A.P.S.S.; Pereira, E.C.; Salles, F.J.; da Silva, F.F.; Batista, B.L.; Handakas, E.; Olympio, K.P.K. Home-based and informal work exposes the families to high levels of potentially toxic elements. Chemosphere 2019, 218, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Salles, F.; Tavares, D.J.B.; Freire, B.M.; Handakas, E.; Batista, B.L.; Olympio, M.P.K. Home-based informal jewelry production increases exposure of working families to cadmium. Sci. Total Environ. 2021, 785, 147297. [Google Scholar] [CrossRef]
- Pexe, M.E.; Marcante, A.; Luz, M.S.; Fernandes, P.H.M.; Neto, F.C.; Sato, A.P.S.; Olympio, K.P.K. Hairdressers are exposed to high concentrations of formaldehyde during the hair straightening procedure. Environ. Sci. Pollut. Res. 2019, 26, 27319–27329. [Google Scholar] [CrossRef]
- Mathee, A.; Street, R.; Teare, J.; Naicker, N. Lead exposure in the home environment: An overview of risks from cottage industries in Africa. Neurotoxicology 2020, 81, 34–39. [Google Scholar] [CrossRef]
- Rappaport, S.M. Implications of the exposome for exposure science. J. Expo. Sci. Environ. Epidemiol. 2011, 21, 5–9. [Google Scholar] [CrossRef]
- Wild, C.P. Complementing the genome with an “exposome”: The outstanding challenge of environmental exposure measurement in molecular epidemiology. Cancer Epidemiol. Biomark. Prev. 2005, 14, 1847–1850. [Google Scholar] [CrossRef]
- Olympio, K.P.K.; Salles, F.J.; Ferreira, A.P.S.S.; Pereira, E.C.; Oliveira, A.S.; Leroux, I.N.; Vieira, F.B.A. The human exposome unraveling the impact of environment on health. Rev. Saúde Pública 2019, 53, 6. [Google Scholar] [CrossRef]
- Wild, C.P. The exposome: From concept to utility. Int. J. Epidemiol. 2012, 41, 24–32. [Google Scholar] [CrossRef]
- DeBord, D.G.; Carreón, T.; Lentz, T.J.; Middendorf, P.J.; Hoover, M.D.; Schulte, P.A. Use of the “exposome” in the practice of epidemiology: A primer on omic technologies. Am. J. Epidemiol. 2016, 184, 302–314. [Google Scholar] [CrossRef]
- Ceylan, R.F.; Ozkan, B.; Mulazimogullari, E. Historical evidence for economic effects of COVID-19. Eur. J. Health Econ. 2020, 21, 817–823. [Google Scholar] [CrossRef] [PubMed]
- Bambra, C.; Riordan, R.; Ford, J.; Matthews, F. The COVID-19 pandemic and health inequalities. J. Epidemiol. Community Health 2020, 74, 964–968. [Google Scholar] [CrossRef] [PubMed]
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Lotta, G.; Kuhlmann, E. When informal work and poor work conditions backfire and fuel the COVID-19 pandemic: Why we should listen to the lessons from Latin America. Int. J. Health Plan Mgmt. 2021, 36, 976–979. [Google Scholar] [CrossRef]
- Chen, M.A. Informal Economy Monitoring Study Sector Report: Home-Based Workers; Women in Informal Employment Globalizing and Organizing (WIEGO): Cambridge, MA, USA, 2014. [Google Scholar]
- La Porta, R.; Shleifer, A. Informality and development. J. Econ. Perspect. 2014, 28, 109–126. [Google Scholar] [CrossRef]
- International Organization for Migration (IOM). UN Network on Migration. Available online: https://www.iom.int/about-migration (accessed on 27 August 2022).
- United Nations. Department of Economic and Social Affairs: News. September 2019. Available online: https://www.un.org/development/desa/en/news/population/international-migrant-stock-2019.html (accessed on 27 August 2022).
- Salmen-Navarro, A. 4D Jobs-Dirty, dangerous, difficult and discriminatory: An update on the 3D job theory. Saf. Health Work 2022, 22, 880. [Google Scholar] [CrossRef]
- Bermingham, J.R. Immigration: Not a solution for the problems of population decline and aging. Popul. Environ. 2001, 22, 355–363. [Google Scholar] [CrossRef]
- Schenker, M.B. A global perspective of migration and occupational health. Am. J. Ind. Med. 2010, 53, 329–337. [Google Scholar] [CrossRef]
- Krogstad, J.M.; Lopez, M.H. Hispanic immigrants more likely to lack health insurance than U.S.-born. In Health Insurance Coverage in the United States, 2013; Smith, J.C., Medalia, C., Eds.; U.S. Government Printing Office: Washington, DC, USA, 2014. [Google Scholar]
- Eurostat. Migration and Migrant Population Statistics. March 2022. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Migration_and_migrant_population_statistics (accessed on 27 August 2022).
- World Health Organization (WHO). Noncommunicable Diseases. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 27 August 2022).
- Lu, Y.; Kaushal, N.; Denier, N.; Wang, J.S.-H. Health of newly arrived immigrants in Canada in the United States: Differential selection on health. Health Place 2017, 48, 1–10. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Report of the Health of Refugees and Migrants in the WHO European Region; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Artiga, A.; Hamel, L.; Kearney, A.; Stokes, M.; Safarpour, A. Health and Health Care Experiences of Hispanic Adults; Kaiser Family Foundation (KFF): Oakland, CA, USA, 2021; Available online: https://www.kff.org/coronavirus-covid-19/poll-finding/health-and-health-care-experiences-of-hispanic-adults/ (accessed on 27 August 2022).
- International Organization for Migration (IOM). Fatal Journeys, Volume 4, Missing Migrant Children; IOM: Geneva, Switzerland, 2019. [Google Scholar]
- Rees, D.; Murray, J.; Nelson, G.; Sonneberg, P. Oscillating migration and the epidemics of silicosis, tuberculosis, and HIV infection in South African gold miners. Am. J. Ind. Med. 2010, 53, 398–404. [Google Scholar] [CrossRef]
- Kistnasamy, B.; Yassi, A.; Spiegel, S.J.; Fairie, A.; Barher, S.; Speigel, J.N. Tackling injustice of occupational lung diseases acquired in South African mines: Recent developments and ongoing challenges. Glob. Health 2018, 14, 60. [Google Scholar] [CrossRef] [PubMed]
- Hargreaves, S.; Restage, K.; Nellems, L.B.; McAlpina, A.; Pocock, N.; Devakumar, D.; Aldridge, R.W.; Abubaker, I.; Kristensen, K.L.; Hummels, J.L.B.; et al. Occupational health outcomes among international migrant workers: A systematic review and meta-analysis. Lancet Glob. Health 2019, 7, 872–882. [Google Scholar] [CrossRef]
- Swerleh, W.M. Global output of research on the health of international migrant workers from 2000 to 2017. Glob. Health 2015, 14, 105. [Google Scholar] [CrossRef] [PubMed]
- La Dou, J.; London, L.; Watterson, A. Occupational health: A world of false promises. Environ. Health 2008, 17, 81. [Google Scholar] [CrossRef]
- Pratap, P.; Dickson, A.; Love, M.; Zanons, J.; Donoto, C.; Flynn, M.A.; Schulte, P.A. Public health impacts of underemployment and unemployment in the United States: Exploring perceptions, gaps and opportunities. Int. J. Environ. Res. Public Health 2021, 18, 10021. [Google Scholar] [CrossRef]
- Malhotra, R.; Arambepola, C.; Tarun, S.; de Silva, V.; Kishore, J.; Østbye, T. Health issues of female foreign domestic workers: A systematic review of the scientific and gray literature. Int. J. Occup. Environ. Health 2013, 19, 261–277. [Google Scholar] [CrossRef]
- McKinsey Global Institute. The Future of Work in Europe: Automation, Workforce Transitions and the Shifting Geography of Employment. 2020. Available online: https://www.mckinsey.com/featured-insights/future-of-work/the-future-of-work-in-europe (accessed on 27 August 2022).
- Thangavel, P.; Pathak, P.; Chandra, B. COVID-19: Globalization—Will the course change? Vision 2022, 26, 7–10. [Google Scholar] [CrossRef]
- Park, S.E. Epidemiology, virology, and clinical features of severe acute respiratory syndrome -coronavirus-2 (SARS-CoV-2; Coronavirus Disease-19). Clin. Exp. Pediatr. 2020, 63, 119–124. [Google Scholar] [CrossRef]
- Peters, S.E.; Dennerlein, J.T.; Wagner, G.R.; Sorensen, G. Work and health in the post-pandemic world: A public health perspective. Lancet Public Health 2022, 7, e188–e194. [Google Scholar] [CrossRef]
- Schulte, P.A.; Bhattacharya, A.; Butler, C.R.; Chun, H.K.; Jacklitsch, B.; Jacobs, T.; Kiefer, M.; Lincoln, J.; Pendergrass, S.; Shire, J.; et al. Advancing the framework for considering the effects of climate change on worker safety and health. J. Occup. Environ. Hyg. 2016, 13, 847–865. [Google Scholar] [CrossRef]
- Potera, C. Climate change impacts indoor environment. Env. Health Perspect. 2011, 119, a382. [Google Scholar] [CrossRef]
- Institute of Medicine (IOM). Climate Change, the Indoor Environment, and Health; The National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- Kjellstrom, T.; Maitre, N.; Saget, C.; Otto, M.; Karim, T. Working on a Warmer Planet: The impact of Heat Stress on Labor Productivity and Decent Work; International Labor Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Schulte, P.A.; Chun, H. Climate change and occupational safety and health: Establishing a preliminary framework. J. Occup. Environ. Hyg. 2009, 6, 542–554. [Google Scholar] [CrossRef] [PubMed]
- Maitre, N.; Monh, G.; Saget, C. The Employment Impact of Climate Change Adaptation; International Labour Office: Geneva, Switzerland, 2018. [Google Scholar]
- Dunne, J.P.; Stouffer, R.J.; John, J.G. Reductions in labour capacity from heat stress under climate warming. Nat. Clim. Change 2013, 36, 563–566. [Google Scholar] [CrossRef]
- Poschen, P. Decent Work, Green Jobs and Sustainable Economy; Solutions for Climate Change and Sustainable Development; Routledge: London, UK; International Labour Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Patil, M.; Jeffery, K.J. What does climate change mean for occupational health professionals? Occup. Med. 2020, 70, 386–388. [Google Scholar] [CrossRef] [PubMed]
- Barrett, J. Worker Transition and Global Climate Change. Pew Center on Global Climate Change. 2001. Available online: https://www.c2es.org/document/worker-transition-global-climate-change/ (accessed on 27 August 2022).
- Morali, D.; Jehel, L.; Paterniti, S. The August 2003 heat wave in France: Effects on psychiatric disorders and suicidal behavior. Presse Med. 2008, 37, 224–228. [Google Scholar] [CrossRef]
- Clayton, S.; Manning, C.M.; Krygsman, K.; Speiser, M. Mental Health and Our Changing Climate: Impacts, Implications, and Guidance; American Psychological Association, ecoAmerica: Washington, DC, USA, 2017. [Google Scholar]
- Kirton, J.J.; Trebilcock, M.J. (Eds.) Hard Choices, Soft Law: Voluntary Standards in Global Trade, Environment and Social Governance; Ashgate Publishing: Aldershot, UK, 2004. [Google Scholar]
- Abbott, K.W.; Snidal, D. Hard and soft law in international governance. Int. Organ. 2000, 54, 421–456. [Google Scholar] [CrossRef]
- Abbott, K.W.; Keohane, R.O.; Moravcsik, A.; Slaughter, A.M.; Snidal, D. The concept of legalization. Int. Organ. 2000, 54, 401–419. [Google Scholar] [CrossRef]
- Leka, S.; Jain, A.; Iavicoli, S.; Di Tecco, C. An evaluation of the policy context on psychosocial risks and mental health in the workplace in the European Union: Achievements, challenges and the future. BioMed Res. Int. 2015, 2015, 213089. [Google Scholar] [CrossRef]
- Jain, A.; Torres, L.D.; Teoh, K.; Leka, S. The impact of national legislation on psychosocial risks on organisational action plans, psychosocial working conditions, and employee work-related stress in Europe. Soc. Sci. Med. 2022, 302, 114987. [Google Scholar] [CrossRef]
- International Labour Organization (ILO). LEGOSH, Global Database on Occupational Safety and Health Legislation; International Labour Organization: Geneva, Switzerland, 2014; Available online: https://www.ilo.org/dyn/legosh/en/f?p=14100:1:::NO::: (accessed on 27 August 2022).
- Health and Safety Executive (HSE). Tackling Work-Related Stress: A Manager’s Guide to Improving and Maintaining Employee Health and Well-Being; Health and Safety Executive: Sudbury, UK, 2001. [Google Scholar]
- Palassis, J.; Schulte, P.A.; Geraci, C. A new American management systems standard in occupational safety and health. ANST 210. J. Chem. Health Saf. 2006, 13, 20–23. [Google Scholar] [CrossRef]
- EU-OSHA (European Agency for Safety and Health at Work). European Survey of Enterprises and a New and Emerging Right—Managing Safety and Health at Work; Publications Office of the European Communities: Luxembourg, 2010. [Google Scholar]
- Mackay, C.J.; Cousins, R.; Kelly, P.J.; Lee, S.; McCaig, R.H. Management standards and work-related stress in the UK: Policy background and science. Work Stress 2004, 18, 91–112. [Google Scholar] [CrossRef]
- Health and Safety Executive (HSE). Occupational Health and Safety Support Systems for Small and Medium Size Enterprises; HSE Books: Subdbury, UK, 2005. [Google Scholar]
- Joubert, D.M. Occupational health challenges and success in developing countries: A South African perspective. Int. J. Occup. Environ. Health 2002, 8, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Leka, S.; Jain, A.; Widerszal-Bazyl, M.; Żołnierczyk-Zreda, D.; Zwetsloot, G.I.J.M. Developing a standard for psychosocial risk management: PAS1010. Saf. Sci. 2011, 49, 1047–1057. [Google Scholar] [CrossRef]
- McBarnet, D. Corporate Social Responsibility: Beyond Law through Law for Law; Working Paper No. 2009/03; University of Edinburgh School of Law: Edinburgh, UK, 2009. [Google Scholar]
- Potter, R.E.; Dollard, M.F.; Owen, M.S.; O’Keefe, V.; Bailey, T.; Leka, S. Assessing a national health and safety policy intervention using the psychosocial safety climate framework. Saf. Sci. 2017, 100, 91–102. [Google Scholar] [CrossRef]
- Leka, S.; Jain, A. Policy approaches to occupational and organizational health. In Bridging Occupational and Organizational and Publish Health: A transdisciplinary Approach; Bauer, G.F., Hämmig, O., Eds.; Springer: Dordrecht, The Netherlands, 2017; pp. 231–249. [Google Scholar]
- European Trade Union Confederation (ETUC). European Social Partners Framework Agreement on Digitalisation. 2020. Available online: https://www.etuc.org/system/files/document/file2020-06/Final%2022%2006%2020_Agreement%20on%20Digitalisation%202020.pdf (accessed on 27 August 2022).
- Chinkin, C.M. The challenge of soft law: Development and change in international law. Intern. Comp. Law Q. 1989, 38, 850–866. [Google Scholar] [CrossRef]
- Schulte, P.A.; Salamanca–Buentello, F. Ethical and scientific issues of nanotechnology in the workplace. Environ. Health Perspect. 2007, 115, 5–12. [Google Scholar] [CrossRef] [Green Version]
- Sorensen, G.; Dennerlein, J.T.; Peters, S.E.; Sabbath, E.L.; Kelly, E.L.; Wagner, G.R. The future research on work, safety, health and well-being: A guiding conceptual framework. Soc. Sci. Med. 2021, 26, 11359. [Google Scholar]
- Carey, G.; Malbon, E.; Carey, N.; Joyce, A.; Crammond, B. Systems Science and Systems Thinking for Public Health: A Systematic Review of the Field. BMJ Open 2015, 5, e009002. [Google Scholar] [CrossRef]
- Streit, J.M.I.E.; Felknor, S.A.; Edwards, N.T.; Howard, J. Leveraging strategic foresight to advance worker safety, health, and well-being. Int. J. Env. Res. Public Health 2021, 18, 8477. [Google Scholar] [CrossRef]
- Flynn, M.A.; Check, P.; Steege, A.L.; Siven, J.M.; Syron, L.N. Health equity and a paradigm shift in occupational safety and health. Int. J. Env. Res. Public Health 2022, 19, 349. [Google Scholar] [CrossRef]
- Oeij, P.R.A.; Rus, D.; Pot, F.D. (Eds.) Workplace Innovation: Theory, Research and Practice; Series on Aligning Perspectives on Health, Safety and Well-Being; Springer: Berlin/Heidelberg, Germany, 2017. [Google Scholar]
- Bauer, G.F.; Hämmig, O. Bridging Occupational, Organizational, and Public Health: A Transdisciplinary Approach; Springer: Dordrecht, The Netherlands, 2014. [Google Scholar]
- Hammer, L.B.; Zimmerman, K.L. Quality of work life. In APA Handbook of Industrial and Organization Psychology: Maintaining, Expanding, and Contracting the Organization; Zedeck, S., Ed.; American Psychological Association: Washington, DC, USA, 2021; pp. 391–431. [Google Scholar]
- DiRuggiero, E.; Cohen, J.E.; Cole, D.C.; Forman, L. Competing conceptualizations of decent work at the intersection of health, social and economic discourses. Soc. Sci. Med. 2015, 133, 120–127. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization [WHO]. Mental Health: A State of Well-Being. 2014. Available online: http://www.who.int/features/factfiles/mental_health/en/ (accessed on 27 August 2022).
- Swanson, J.L. Work and psychological health. In APA Handbook of Counseling Psychology; Fouad, N.A., Carter, A., Subich, L.M., Eds.; American Psychological Association: Washington, DC, USA, 2012; pp. 3–27. [Google Scholar]
- Duffy, R.D.; Allan, B.; England, J.W.; Blustein, D.L.; Autin, K.L.; Douglass, R.P.; Ferreira, J.; Santos, E.J.R. The development and initial validation of the Decent Work Scale. Couns. Psychol. 2017, 64, 206–221. [Google Scholar] [CrossRef] [PubMed]
- Coggon, D. Occupational medicine at a turning point. Occup. Environ. Med. 2005, 62, 281–283. [Google Scholar] [CrossRef] [PubMed]
- Amick, B.C.; McLeod, C.B.; Bültmann, U. Labor markets and health an integrated life course perspective. Scan. J. Work Environ. Health 2016, 42, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Schulte, P.A.; Pana-Cryan, R.; Schnorr, T.; Schill, A.L.; Guerin, R.; Felknor, S.; Wagner, G.R. An approach to assess the burden of work-related injury, disease, and distress. Am. J. Public Health 2017, 107, 1051–1057. [Google Scholar] [CrossRef]
- Ilmarinen, J.; Tuomi, K.; Klockars, M. Changes in the work ability of active employees over an 11-year period. Scan. J. Work Environ. Health 1997, 23, 49–57. [Google Scholar]
- Laloux, F. Reinventing Organizations: A Guide to Creating Organizations Inspired by the Next Stage of Human Consciousness; Nelson Parker: Brussels, Belgium, 2014. [Google Scholar]
- International Labour Organization. International Labour Conference Adds Safety and Health to Fundamental Principles and Rights at Work. Available online: https://www.ilo.org/global/about-the-ilo/newsroom/news/wcms_848132/lang-en/index.htm (accessed on 10 June 2022).


{kind=link}
| Employment Creation | Social Protection | Rights of Workers | Social Dialogue |
|---|---|---|---|
|
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schulte, P.A.; Iavicoli, I.; Fontana, L.; Leka, S.; Dollard, M.F.; Salmen-Navarro, A.; Salles, F.J.; Olympio, K.P.K.; Lucchini, R.; Fingerhut, M.; et al. Occupational Safety and Health Staging Framework for Decent Work. Int. J. Environ. Res. Public Health 2022, 19, 10842. https://doi.org/10.3390/ijerph191710842
Schulte PA, Iavicoli I, Fontana L, Leka S, Dollard MF, Salmen-Navarro A, Salles FJ, Olympio KPK, Lucchini R, Fingerhut M, et al. Occupational Safety and Health Staging Framework for Decent Work. International Journal of Environmental Research and Public Health. 2022; 19(17):10842. https://doi.org/10.3390/ijerph191710842
Chicago/Turabian StyleSchulte, Paul A., Ivo Iavicoli, Luca Fontana, Stavroula Leka, Maureen F. Dollard, Acran Salmen-Navarro, Fernanda J. Salles, Kelly P. K. Olympio, Roberto Lucchini, Marilyn Fingerhut, and et al. 2022. "Occupational Safety and Health Staging Framework for Decent Work" International Journal of Environmental Research and Public Health 19, no. 17: 10842. https://doi.org/10.3390/ijerph191710842