
Association of Diet, Body Mass Index, and Lifestyle on the Gastrointestinal Health Risk in a Sample of Adults

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Sociodemographic, Habits, and Lifestyle Data
2.3. Gastrointestinal Health
2.4. Functional Gastrointestinal Disorders
2.5. Body Mass Index (BMI)
2.6. Statistical Analysis
3. Results
3.1. Frequency of Intestinal Symptoms
3.2. Differences between Sexes
3.3. Risks to Intestinal Health
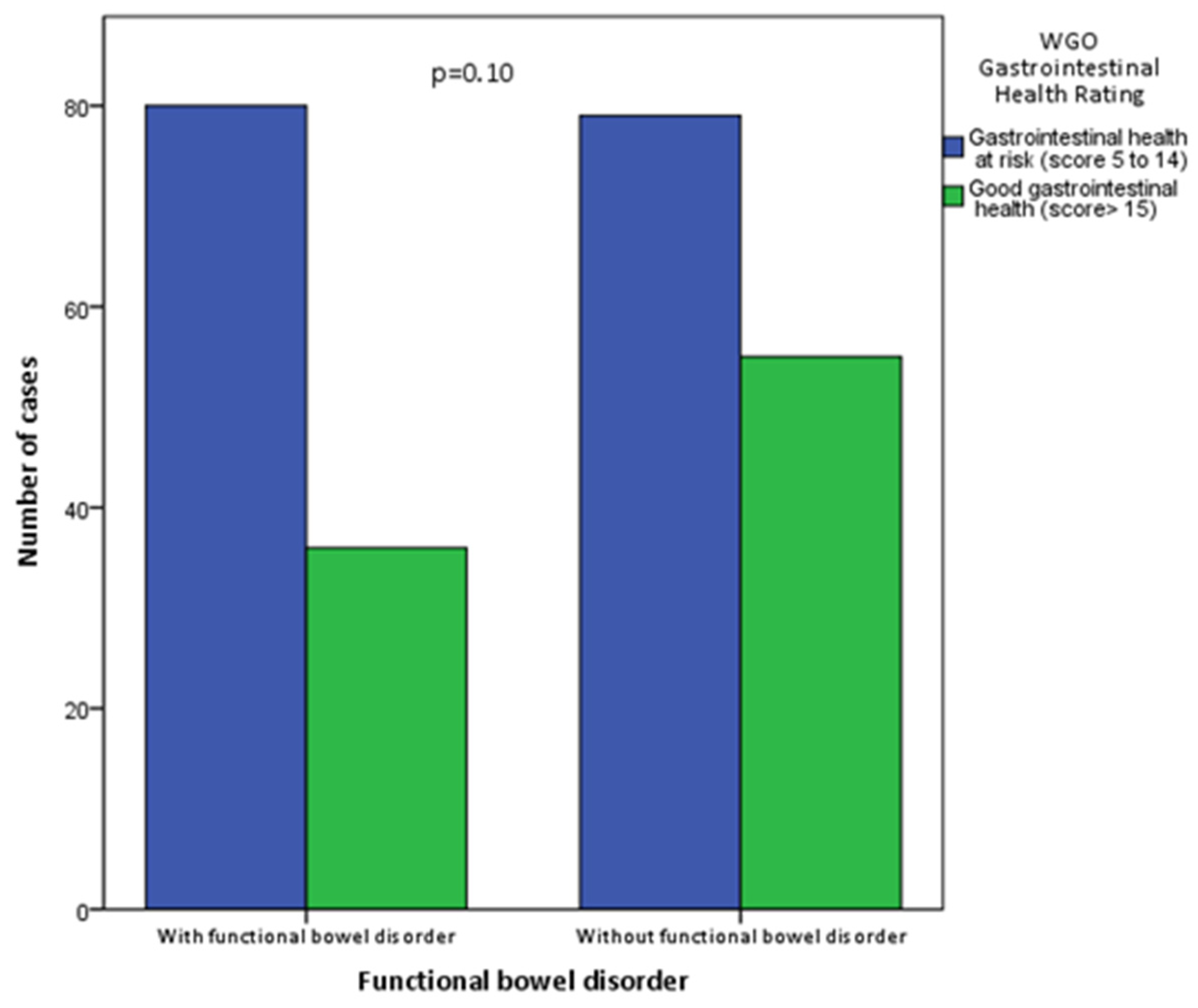
3.4. Rome IV Criteria
4. Discussion
4.1. Functional Bowel Disorder (Irritable Bowel Syndrome)
4.2. Role of Diet on Intestinal Disease
4.2.1. Alcohol
4.2.2. Fruits and Vegetables
4.2.3. Beverages and Water Intake
4.3. Body Mass Index
4.4. Physical Activity
4.5. Food Schedule
4.6. Educational Level and Sociodemographic Characteristics
4.7. Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| GI | Gastrointestinal |
| GIH | Gastrointestinal health |
| FGID | Functional gastrointestinal disorders |
| IBS | Irritable bowel syndrome |
| BMI | Body mass index |
| WGO | World Gastroenterology Organization |
| LRA | Logistic regression analysis |
| FODMAP | Fermentable oligosaccharides, disaccharides, monosaccharides, and polyols |
References
- Moonen, P.-J.; Blaser, A.R.; Starkopf, J.; Straaten, H.M.O.-V.; Van Der Mullen, J.; Vermeulen, G.; Malbrain, M.L. The Black Box Revelation: Monitoring Gastrointestinal Function. Anaesthesiol. Intensiv. Ther. 2018, 50, 72–81. [Google Scholar] [CrossRef] [PubMed]
- Halder, S.L.S.; Locke, G.R.; Talley, N.J.; Fett, S.L.; Zinsmeister, A.R.; Melton, L.J. Impact of Functional Gastrointestinal Disorders on Health-Related Quality of Life: A Population-Based Case-Control Study. Aliment. Pharmacol. Ther. 2004, 19, 233–242. [Google Scholar] [CrossRef] [PubMed]
- Foxx-Orenstein, A.E. New and Emerging Therapies for the Treatment of Irritable Bowel Syndrome: An Update for Gastroenterologists. Ther. Adv. Gastroenterol. 2016, 9, 354–375. [Google Scholar] [CrossRef] [PubMed]
- Richardson, D.P.; Ansell, J.; Drummond, L.N. The Nutritional and Health Attributes of Kiwifruit: A Review. Eur. J. Nutr. 2018, 57, 2659–2676. [Google Scholar] [CrossRef]
- Holtmann, G.; Shah, A.; Morrison, M. Pathophysiology of Functional Gastrointestinal Disorders: A Holistic Overview. Dig. Dis. 2017, 35, 5–13. [Google Scholar] [CrossRef]
- Emerenziani, S.; Guarino, M.P.L.; Asensio, L.M.T.; Altomare, A.; Ribolsi, M.; Balestrieri, P.; Cicala, M. Role of Overweight and Obesity in Gastrointestinal Disease. Nutrients 2019, 12, 111. [Google Scholar] [CrossRef]
- Hongo, M. Epidemiology of FGID Symptoms in Japanese General Population with Reference to Lifestyle. J. Gastroenterol. Hepatol. 2011, 26, 19–22. [Google Scholar] [CrossRef]
- Gonlachanvit, S. Are Rice and Spicy Diet Good for Functional Gastrointestinal Disorders? J. Neurogastroenterol. Motil. 2010, 16, 131–138. [Google Scholar] [CrossRef]
- Miwa, H. Lifestyle in Persons with Functional Gastrointestinal Disorders-Large-Scale Internet Survey of Lifestyle in Japan. Neurogastroenterol. Motil. 2012, 24, 464–471. [Google Scholar] [CrossRef]
- López, N.P.Y.; Torres-López, E.; Zamarripa-Dorsey, F. Respuesta Clínica En Pacientes Mexicanos Con Síndrome De Intestino Irritable Tratados Con Dieta Baja En Carbohidratos Fermentables (FODMAP). Rev. Gastroenterol. Mex. 2015, 80, 180–185. [Google Scholar] [CrossRef] [Green Version]
- Catálogo Maestro de Guías de Práctica Clínica*IMSS 042-08. Diagnóstico y Tratamiento del Intestino Irritable en el Adulto. Available online: https://www.imss.gob.mx/sites/all/statics/guiasclinicas/042GRR.pdf (accessed on 19 August 2022).
- World Gastroenterology Organisation. Global Guardian of Digestive Health. Serving the World. 2022. Available online: https://www.worldgastroenterology.org/forms/health-test.php (accessed on 19 August 2022).
- De La Salud, P. Reglamento de la ley general de salud en materia de investigación para la salud. Diario Oficial de la Federación 1987. Available online: https://www.diputados.gob.mx/LeyesBiblio/regley/Reg_LGS_MIS.pdf (accessed on 19 August 2022).
- Mearin, F.; Lacy, B.E.; Chang, L.; Chey, W.D.; Lembo, A.J.; Simren, M.; Spiller, R. Bowel Disorders. Gastroenterology 2016, 150, 1393–1407. [Google Scholar] [CrossRef]
- Mearin, F.; Ciriza, C.; Mínguez, M.; Rey, E.; Mascort, J.J.; Peña, E.; Cañones, P.; Júdez, J. Clinical Practice Guideline: Irritable Bowel Syndrome with Constipation and Functional Constipation in the Adult. Rev. Esp. Enfermedades Dig. 2016, 108, 332–363. [Google Scholar] [CrossRef] [PubMed]
- Lohman, T.J.; Roache, A.F.; Martorell, R. Anthropometric Standardization Reference Manual; Human Kinetics Books: Champaign, IL, USA, 1988. [Google Scholar]
- World Health Organization Obesity and Overweight. Factsheet. Updated 2020. Available online: www.who.int/mediacentre/factsheets/fs311/en/ (accessed on 19 August 2022).
- Drossman, D.A. The Functional Gastrointestinal Disorders and the Rome III Process. Gastroenterology 2006, 130, 1377–1390. [Google Scholar] [CrossRef] [PubMed]
- Sperber, A.D.; Bangdiwala, S.I.; Drossman, D.A.; Ghoshal, U.C.; Simren, M.; Tack, J.; Whitehead, W.E.; Dumitrascu, D.L.; Fang, X.; Fukudo, S.; et al. Worldwide Prevalence and Burden of Functional Gastrointestinal Disorders, Results of Rome Foundation Global Study. Gastroenterology 2021, 160, 99–114.e3. [Google Scholar] [CrossRef]
- Nellesen, D.; Yee, K.; Chawla, A.; Lewis, B.E.; Carson, R.T. A Systematic Review of the Economic and Humanistic Burden of Illness in Irritable Bowel Syndrome and Chronic Constipation. J. Manag. Care Pharm. 2013, 19, 755–764. [Google Scholar] [CrossRef]
- Guilera, M.; Balboa, A.; Mearin, F. Bowel Habit Subtypes and Temporal Patterns in Irritable Bowel Syndrome: Systematic Review. Am. J. Gastroenterol. 2005, 100, 1174–1184. [Google Scholar] [CrossRef]
- Adeyemo, M.A.; Spiegel, B.M.R.; Chang, L. Meta-Analysis: Do Irritable Bowel Syndrome Symptoms Vary between Men and Women? Aliment. Pharmacol. Ther. 2010, 32, 738–755. [Google Scholar] [CrossRef]
- World Gastroenterology Organization. Global Guidelines. Síndrome de Intestino Irritable. 2015. Available online: https://www.worldgastroenterology.org/guidelines/global-guidelines/irritable-bowel-syndrome-ibs/irritable-bowel-syndrome-ibs-spanish (accessed on 19 August 2022).
- Lovell, R.M.; Ford, A.C. Global Prevalence of and Risk Factors for Irritable Bowel Syndrome: A Meta-analysis. Clin. Gastroenterol. Hepatol. 2012, 10, 712–721.e4. [Google Scholar] [CrossRef]
- Arce, A.D.; Ermocilla, C.A.; Costa, H. Evaluation of Constipation. Am. Fam. Physician 2002, 65, 2283–2290. [Google Scholar]
- Bellini, M.; Gambaccini, D.; Usai-Satta, P.; De Bortoli, N.; Bertani, L.; Marchi, S.; Stasi, C. Irritable Bowel Syndrome and Chronic Constipation: Fact and Fiction. World J. Gastroenterol. 2015, 21, 11362–11370. [Google Scholar] [CrossRef]
- Tollenaar, M.S.; Overgaauw, S. Empathy and Mentalizing Abilities in Relation to Psychosocial Stress in Healthy Adult Men and Women. Heliyon 2020, 6, e04488. [Google Scholar] [CrossRef] [PubMed]
- Monsbakken, K.W.; Vandvik, P.O.; Farup, P.G. Perceived Food Intolerance in Subjects with Irritable Bowel Syndrome–Etiology, Prevalence and Consequences. Eur. J. Clin. Nutr. 2005, 60, 667–672. [Google Scholar] [CrossRef] [PubMed]
- Anbazhagan, A.N.; Priyamvada, S.; Alrefai, W.A.; Dudeja, P.K. Pathophysiology of IBD Associated Diarrhea. Tissue Barriers 2018, 6, e1463897. [Google Scholar] [CrossRef] [PubMed]
- El-Salhy, M.; Patcharatrakul, T.; Gonlachanvit, S. The Role of Diet in the Pathophysiology and Management of Irritable Bowel Syndrome. Indian J. Gastroenterol. 2021, 40, 111–119. [Google Scholar] [CrossRef]
- Gros, M.; Gros, B.; Mesonero, J.; Latorre, E. Neurotransmitter Dysfunction in Irritable Bowel Syndrome: Emerging Approaches for Management. J. Clin. Med. 2021, 10, 3429. [Google Scholar] [CrossRef]
- Heeney, A.; Rogers, A.; Mohan, H.; Mc Dermott, F.; Baird, A.; Winter, D. Prostaglandin E2 Receptors and Their Role in Gastrointestinal Motility–Potential Therapeutic Targets. Prostaglandins Other Lipid Mediat. 2020, 152, 106499. [Google Scholar] [CrossRef]
- Mesa, M.D.; Loureiro, B.; Iglesia, I.; Fernandez Gonzalez, S.; Llurba Olivé, E.; García Algar, O.; Solana, M.J.; Cabero Perez, M.J.; Sainz, T.; Martinez, L.; et al. The Evolving Microbiome from Pregnancy to Early Infancy: A Comprehensive Review. Nutrients 2020, 12, 133. [Google Scholar] [CrossRef]
- Gibson, P.R.; Shepherd, S.J. Evidence-Based Dietary Management of Functional Gastrointestinal Symptoms: The FODMAP approach. J. Gastroenterol. Hepatol. 2010, 25, 252–258. [Google Scholar] [CrossRef]
- Ibrahim, F.; Stribling, P. A 5Ad Dietary Protocol for Functional Bowel Disorders. Nutrients 2019, 11, 1938. [Google Scholar] [CrossRef]
- Reding, K.W.; Cain, K.C.; E Jarrett, M.; Eugenio, M.D.; Heitkemper, M.M. Relationship Between Patterns of Alcohol Consumption and Gastrointestinal Symptoms Among Patients with Irritable Bowel Syndrome. Am. J. Gastroenterol. 2013, 108, 270–276. [Google Scholar] [CrossRef]
- Rozich, J.J.; Holmer, A.; Singh, S. Effect of Lifestyle Factors on Outcomes in Patients with Inflammatory Bowel Diseases. Am. J. Gastroenterol. 2020, 115, 832–840. [Google Scholar] [CrossRef] [PubMed]
- Bergmann, M.M.; Hernandez, V.; Bernigau, W.; Boeing, H.; Chan, S.S.; Luben, R.; Khaw, K.T.; van Schaik, F.; Oldenburg, B.; Bueno-de-Mesquita, B.; et al. No Association of Alcohol Use and the Risk of Ulcerative Colitis or Crohn’s Disease: Data from A European Prospective Cohort Study (EPIC). Eur. J. Clin. Nutr. 2017, 71, 512–518. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Xiang, L.; He, J. Beverage Intake and Risk of Crohn Disease: A Meta-Analysis of 16 Epidemiological Studies. Medicine 2019, 98, e15795. [Google Scholar] [CrossRef]
- Scientific Advisory Committee on Nutrition 2015. Carbohydrates and Health. Available online: https://assets.publishing.ser-vice.gov.uk/government/uploads/system/uploads/attachment_data/file/445503/SACN_Carbohydrates_and_Health.pdf (accessed on 19 May 2021).
- Gill, S.K.; Rossi, M.; Bajka, B.; Whelan, K. Dietary Fibre in Gastrointestinal Health and Disease. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 101–116. [Google Scholar] [CrossRef]
- El-Salhy, M. Irritable Bowel Syndrome: Diagnosis and Pathogenesis. World J. Gastroenterol. 2012, 18, 5151–5163. [Google Scholar] [CrossRef] [PubMed]
- Eswaran, S.; Muir, J.; Chey, W.D. Fiber and Functional Gastrointestinal Disorders. Am. J. Gastroenterol. 2013, 108, 718–727. [Google Scholar] [CrossRef] [PubMed]
- Defrees, D.N.; Bailey, J. Irritable Bowel Syndrome: Epidemiology, Pathophysiology, Diagnosis, and Treatment. Prim. Care: Clin. Off. Pract. 2017, 44, 655–671. [Google Scholar] [CrossRef]
- Dionne, J.; Ford, A.C.; Yuan, Y.; Chey, W.D.; Lacy, B.E.; Saito, Y.A.; Quigley, E.M.M.; Moayyedi, P. A Systematic Review and Meta-Analysis Evaluating the Efficacy of a Gluten-Free Diet and a Low FODMAPS Diet in Treating Symptoms of Irritable Bowel Syndrome. Am. J. Gastroenterol. 2018, 113, 1290–1300. [Google Scholar] [CrossRef]
- Baker, A.H.; Wardle, J. Sex Differences in Fruit and Vegetable Intake in Older Adults. Appetite 2003, 40, 269–275. [Google Scholar] [CrossRef]
- Guo, Y.-B.; Zhuang, K.-M.; Kuang, L.; Zhan, Q.; Wang, X.-F.; Liu, S.-D. Association between Diet and Lifestyle Habits and Irritable Bowel Syndrome: A Case-Control Study. Gut Liver 2015, 9, 649–656. [Google Scholar] [CrossRef]
- Alharbi, S.H.; Alateeq, F.A.; Alshammari, K.I.; Alshammri, A.S.S.; Alabdali, N.A.N.; Alsulaiman, M.A.S.; Algothi, S.M.I.; Altoraifi, A.S.; Almutairi, M.Q.; Ahmed, H.G. Irritable Bowel Syndrome and Dietary Habits in Northern Saudi Arabia. Health 2019, 11, 289–297. [Google Scholar] [CrossRef] [Green Version]
- Salari-Moghaddam, A.; Keshteli, A.H.; Esmaillzadeh, A.; Adibi, P. Water Consumption and Prevalence of Irritable Bowel Syndrome Among Adults. PLoS ONE 2020, 15, e0228205. [Google Scholar] [CrossRef]
- Zaribaf, F.; Keshteli, A.H.; Esmaillzadeh, A.; Saneei, P.; Feizi, A.; Daghaghzadeh, H.; Feinle-Bisset, C.; Adibi, P. Empirically Derived Dietary Habits Are Associated with Irritable Bowel Syndrome. Eur. J. Clin. Nutr. 2018, 72, 1537–1547. [Google Scholar] [CrossRef] [PubMed]
- Sadik, R.; Björnsson, E.; Simrén, M. The Relationship Between Symptoms, Body Mass Index, Gastrointestinal Transit and Stool Frequency in Patients with Irritable Bowel Syndrome. Eur. J. Gastroenterol. Hepatol. 2010, 22, 102–108. [Google Scholar] [CrossRef]
- Akhondi, N.; Montazerin, S.M.; Soltani, S.; Saneei, P.; Keshteli, A.H.; Esmaillzadeh, A.; Adibi, P. General and Abdominal Obesity in Relation to the Prevalence of Irritable Bowel Syndrome. Neurogastroenterol. Motil. 2019, 31, e13549. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.G.; Lee, J.K.; Kang, Y.-S.; Shin, S.; Kim, J.H.; Lim, Y.J.; Koh, M.-S.; Lee, J.H.; Kang, H.W. Visceral Abdominal Obesity Is Associated with an Increased Risk of Irritable Bowel Syndrome. Am. J. Gastroenterol. 2015, 110, 310–319. [Google Scholar] [CrossRef] [PubMed]
- Sezgin, O.; Akpinar, H.; Ozer, B.; Toruner, M.; Bal, K.; Bor, S. Population-Based Assessment of Gastrointestinal Symptoms and Diseases: Cappadocia Cohort, Turkey. Turk. J. Gastroenterol. 2020, 30, 1009–1020. [Google Scholar] [CrossRef] [PubMed]
- Simrén, M.; Månsson, A.; Langkilde, A.M.; Svedlund, J.; Abrahamsson, H.; Bengtsson, U.; Björnsson, E.S. Food-Related Gastrointestinal Symptoms in the Irritable Bowel Syndrome. Digestion 2001, 63, 108–115. [Google Scholar] [CrossRef]
- Nam, S.Y. Obesity-Related Digestive Diseases and Their Pathophysiology. Gut Liver 2017, 11, 323–334. [Google Scholar] [CrossRef]
- Shamah-Levy, T.; Romero-Martínez, M.; Barrientos-Gutiérrez, T.; Cuevas-Nasu, L.; Bautista-Arredondo, S.; Colchero, M.A.; Gaona-Pineda, E.B.; Lazcano-Ponce, E.; Martínez-Barnetche, J.; Alpuche-Arana, C.; et al. Encuesta Nacional de Salud y Nutrición 2021 sobre COVID-19; Resultados nacionales; Instituto Nacional de Salud Pública: Cuernavaca, México, 2022; Available online: https://www.insp.mx/resources/images/stories/2022/docs/220801_Ensa21_digital_29julio.pdf (accessed on 19 August 2022).
- Estébanez, B.; Huang, C.-J.; Rivera-Viloria, M.; González-Gallego, J.; Cuevas, M.J. Exercise Outcomes in Childhood Obesity-Related Inflammation and Oxidative Status. Front. Nutr. 2022, 9, 886291. [Google Scholar] [CrossRef]
- Motiani, K.K.; Savolainen, A.M.; Eskelinen, J.-J.; Toivanen, J.; Ishizu, T.; Yli-Karjanmaa, M.; Virtanen, K.A.; Parkkola, R.; Kapanen, J.; Grönroos, T.J.; et al. Two Weeks of Moderate-Intensity Continuous Training, But Not High-Intensity Interval Training, Increases Insulin-Stimulated Intestinal Glucose Uptake. J. Appl. Physiol. 2017, 122, 1188–1197. [Google Scholar] [CrossRef] [PubMed]
- Motiani, K.K.; Collado, M.C.; Eskelinen, J.J.; Virtanen, K.A.; Löyttyniemi, E.; Salminen, S.; Nuutila, P.; Kalliokoski, K.K.; Hannukainen, J.C. Exercise Training Modulates Gut Microbiota Profile and Improves Endotoxemia. Med. Sci. Sports Exerc. 2020, 52, 94–104. [Google Scholar] [CrossRef] [PubMed]
- Koh, H.-C.E.; van Vliet, S.; Pietka, T.A.; Meyer, G.A.; Razani, B.; Laforest, R.; Gropler, R.J.; Mittendorfer, B. Subcutaneous Adipose Tissue Metabolic Function and Insulin Sensitivity in People with Obesity. Diabetes 2021, 70, 2225–2236. [Google Scholar] [CrossRef] [PubMed]
- Konturek, P.C.; Brzozowski, T.; Konturek, S.J. Gut clock: Implication of Circadian Rhythms in the Gastrointestinal Tract. J. Physiol. Pharmacol. 2011, 62, 139–150. [Google Scholar] [PubMed]
- Latif, A.; Memon, F.A.; Asad, M. Irritable Bowel Syndrome in a Population of a Developing Country: Prevalence and Association. Cureus 2020, 12, e8112. [Google Scholar] [CrossRef]
- Chung, W.; Kim, J.; Lim, S.-J.; Lee, S. Sex-Specific Role of Education on the Associations of Socioeconomic Status Indicators with Obesity Risk: A Population-Based Study in South Korea. PLoS ONE 2018, 13, e0190499. [Google Scholar] [CrossRef]
- Ogden, C.L.; Fakhouri, T.H.; Carroll, M.D.; Hales, C.; Fryar, C.D.; Li, X.; Freedman, D.S. Prevalence of Obesity Among Adults, by Household Income and Education—United States, 2011–2014. MMWR. Morb. Mortal. Wkly. Rep. 2017, 66, 1369–1373. [Google Scholar] [CrossRef]
- Mansouri, A.; Rarani, M.A.; Fallahi, M.; Alvandi, I. Irritable Bowel Syndrome Is Concentrated in People with Higher Educations in Iran: An Inequality Analysis. Epidemiol. Health 2017, 39, e2017005. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Median | Percentile (25, 75) | Range (min, max) | |
|---|---|---|---|
| Age (years) | 38.5 | 25, 47 | 18, 63 |
| Weight (kg) | 70.5 | 61.0, 79.2 | 42, 120 |
| Height (cm) | 160 | 155.0, 165.2 | 142, 184 |
| BMI (kg/m2) | 27 | 24, 30 | 18, 50 |
| Frequency (%) | |||
| Body Mass Index | |||
| Underweight | 1 | 0.4 | |
| Normal weight | 75 | 30 | |
| Overweight | 106 | 42.4 | |
| Obesity | 68 | 27.2 | |
| Sociodemographic Data | |||
| Marital status | |||
| Single | 131 | 52.4 | |
| With couple | 119 | 47.6 | |
| Occupation | |||
| Paid | 104 | 41.6 | |
| Unpaid | 146 | 58.4 | |
| Scholarship | |||
| Elementary | 4 | 1.6 | |
| Middle school | 11 | 4.4 | |
| High school | 68 | 27.2 | |
| Bachelor | 158 | 63.2 | |
| Other | 9 | 3.6 | |
| Socioeconomic level | |||
| High | 7 | 2.8 | |
| Medium | 234 | 93.6 | |
| Low | 9 | 3.6 | |
| Symptom | Total | Women (n = 199) | Men (n = 51) | p-Value |
|---|---|---|---|---|
| Diarrhea | 40 (16) | 36 (18.1) | 4 (7.8) | 0.75 |
| Constipation | 77 (30.8) | 68 (34.2) | 9 (17.6) | 0.02 |
| Flatulence | 151 (60.4) | 118 (59.3) | 33 (64.7) | 0.48 |
| Abdominal distension | 162 (64.8) | 130 (65.3) | 32 (62.7) | 0.73 |
| Abdominal heaviness | 87 (34.8) | 73 (36.7) | 14 (27.5) | 0.21 |
| Abdominal pain | 78 (31.2) | 66 (33.2) | 12 (23.5) | 0.18 |
| Exposure Variable | Mean Differences | CI 95% | ETA2 | p Value | |
|---|---|---|---|---|---|
| Water consumption per day * (reference group: less than one liter) | Between one and two liters Between two and three liters | −2.15 −2.91 | −3.90, −0.41 −4.71, −1.10 | 0.046 | 0.010 <0.001 |
| Consumption of 2 or more chocolate/week | Yes vs. No | 0.06 | −1.29, 1.41 | 0.001 | 0.931 |
| Consumption of 2 or more cupcakes/week | Yes vs. No | −6.77 | −2.00, 0.67 | 0.005 | 0.324 |
| Alcoholic beverages intake, at least once a week | Yes vs. No | 1.21 | 0.05, 2.37 | 0.017 | 0.041 |
| Smoking, more than two times a week | Yes vs. No | −0.32 | −1.48, 0.83 | 0.001 | 0.584 |
| Irritating or spicy foods, at least once a week | Yes vs. No | 0.99 | −0.97, 2.96 | 0.005 | 0.319 |
| Carbonated Drinks, at least once a week | Yes vs. No | −0.61 | −1.97, 0.73 | 0.004 | 0.368 |
| Coffe at least once a day | Yes vs. No | 0.70 | −0.70, 2.12 | 0.005 | 0.325 |
| Eat Out | Yes vs. No | 0.93 | −0.49, 3.18 | 0.009 | 0.149 |
| A usual morning snack | Yes vs. No | −0.513 | −2.46, 1.43 | 0.001 | 0.605 |
| A usual evening snack | Yes vs. No | −1.93 | −4.07, 0.20 | 0.014 | 0.076 |
| Consumption vegetables * (reference group: less than once a week) | One time a week Every 3 or 4 days Every 1 or 2 days Daily | −1.96 −3.57 −5.09 −6.02 | −4.35, 0.44 −5.74, −1.39 −7.50, −2.67 −8.23, −3.81 | 0.268 | 0.215 <0.001 <0.001 <0.001 |
| Weekly exercise | Once Every 3 or 4 days Every 1 or 2 days Daily | −1.35 −3.00 −4.71 −6.60 | −2−28, −0.42 −4.68, −2.51 −5.75, −3.67 −7.70, −5.50 | 0.400 | 0.001 <0.001 <0.001 <0.001 |
| Body mass index (kg/m2) * (reference group: 24.9 or less) | 40 or more 35 to 39.9 30 to 34.9 25 to 29.9 | −5.40 −4.47 −2.58 −1.12 | −9.37, −1.44 −6.87, −2.08 −4.33, −0.84 −2.53, 0.30 | 0.169 | 0.002 <0.001 <0.001 0.203 |
| Symptomatic medication use * (reference group: no medication) | Daily Every 3–4 days Every 1–2 days 1 per week | −4.70 −4.13 −5.74 −2.46 | −6.09, −3.30 −5.64, −2.62 −7.61, −3.87 3.31, −1.62 | 0.279 | <0.001 <0.001 <0.001 <0.001 |
| With Functional Bowel Disorder | Without Functional Bowel Disorder | |||
|---|---|---|---|---|
| n | % | n | % | |
| With constipation | 65 | 56.0 | 52 | 38.8 |
| With diarrhea | 4 | 3.40 | 9 | 6.7 |
| Mixed | 15 | 13.0 | 10 | 7.4 |
| Indeterminate | 32 | 27.6 | 0 | 0 |
| Asymptomatic | 0 | 0 | 63 | 47.0 |
| Total | 116 | 100 | 134 | 100 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sámano, R.; Esparza-Juárez, F.; Chico-Barba, G.; González-Medina, E.; Sánchez-Jiménez, B.; Hernández-Trejo, M. Association of Diet, Body Mass Index, and Lifestyle on the Gastrointestinal Health Risk in a Sample of Adults. Int. J. Environ. Res. Public Health 2022, 19, 10569. https://doi.org/10.3390/ijerph191710569
Sámano R, Esparza-Juárez F, Chico-Barba G, González-Medina E, Sánchez-Jiménez B, Hernández-Trejo M. Association of Diet, Body Mass Index, and Lifestyle on the Gastrointestinal Health Risk in a Sample of Adults. International Journal of Environmental Research and Public Health. 2022; 19(17):10569. https://doi.org/10.3390/ijerph191710569
Chicago/Turabian StyleSámano, Reyna, Fernanda Esparza-Juárez, Gabriela Chico-Barba, Erika González-Medina, Bernarda Sánchez-Jiménez, and María Hernández-Trejo. 2022. "Association of Diet, Body Mass Index, and Lifestyle on the Gastrointestinal Health Risk in a Sample of Adults" International Journal of Environmental Research and Public Health 19, no. 17: 10569. https://doi.org/10.3390/ijerph191710569