
A Meta-Analysis of the Effects of Different Exercise Modes on Inflammatory Response in the Elderly


Abstract
:1. Introduction
2. Materials and Methods
2.1. Selection and Exclusion Criteria of Literature
2.2. Searching Strategy
2.3. Data Extraction and Quality Evaluation
2.3.1. Data Extraction and Processing
2.3.2. Literature Quality Evaluation
3. Results
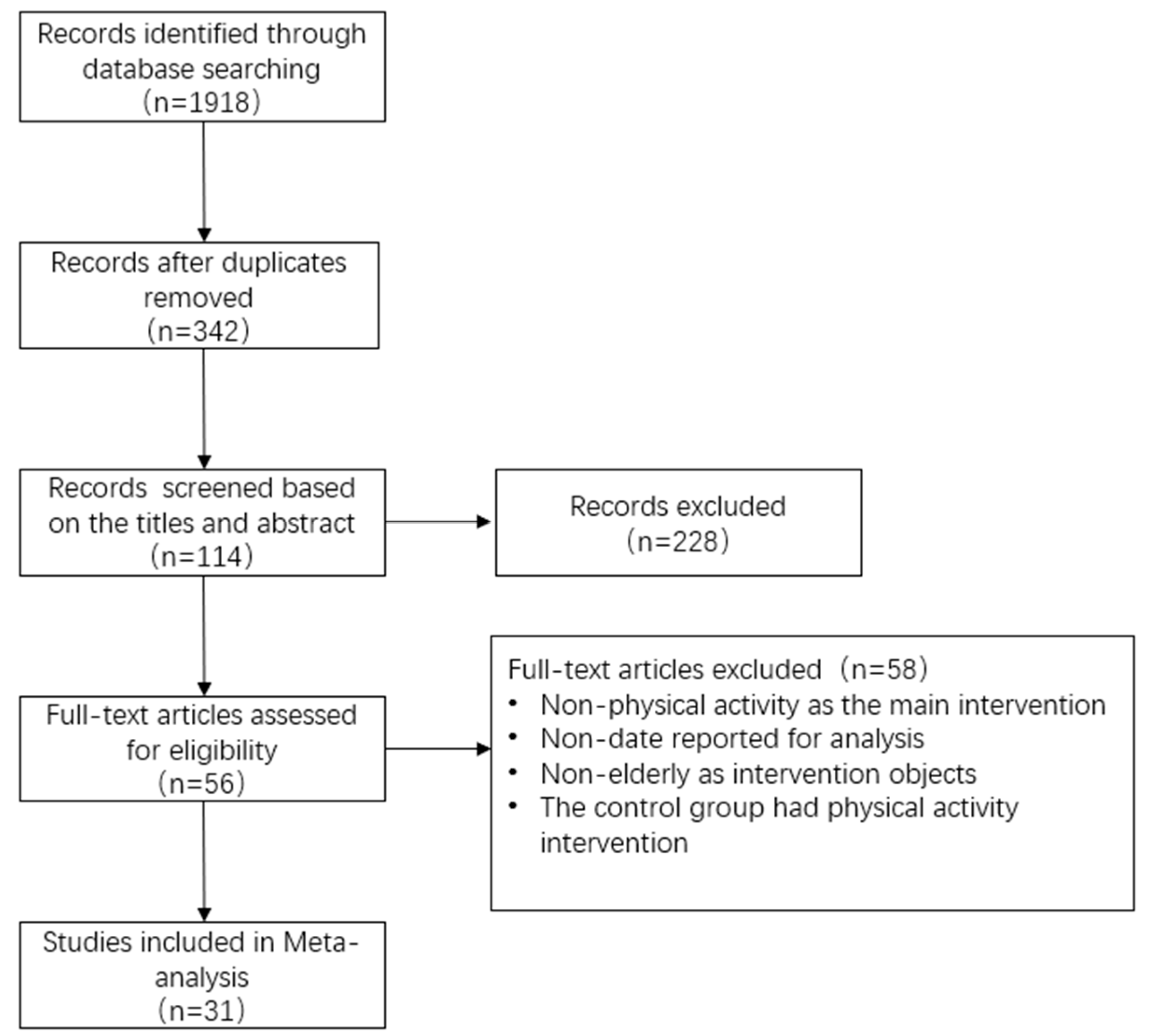
3.1. General Results of Selected Research Literature
3.2. General Features of the Selected Research Literature
3.2.1. General Information of Each Study
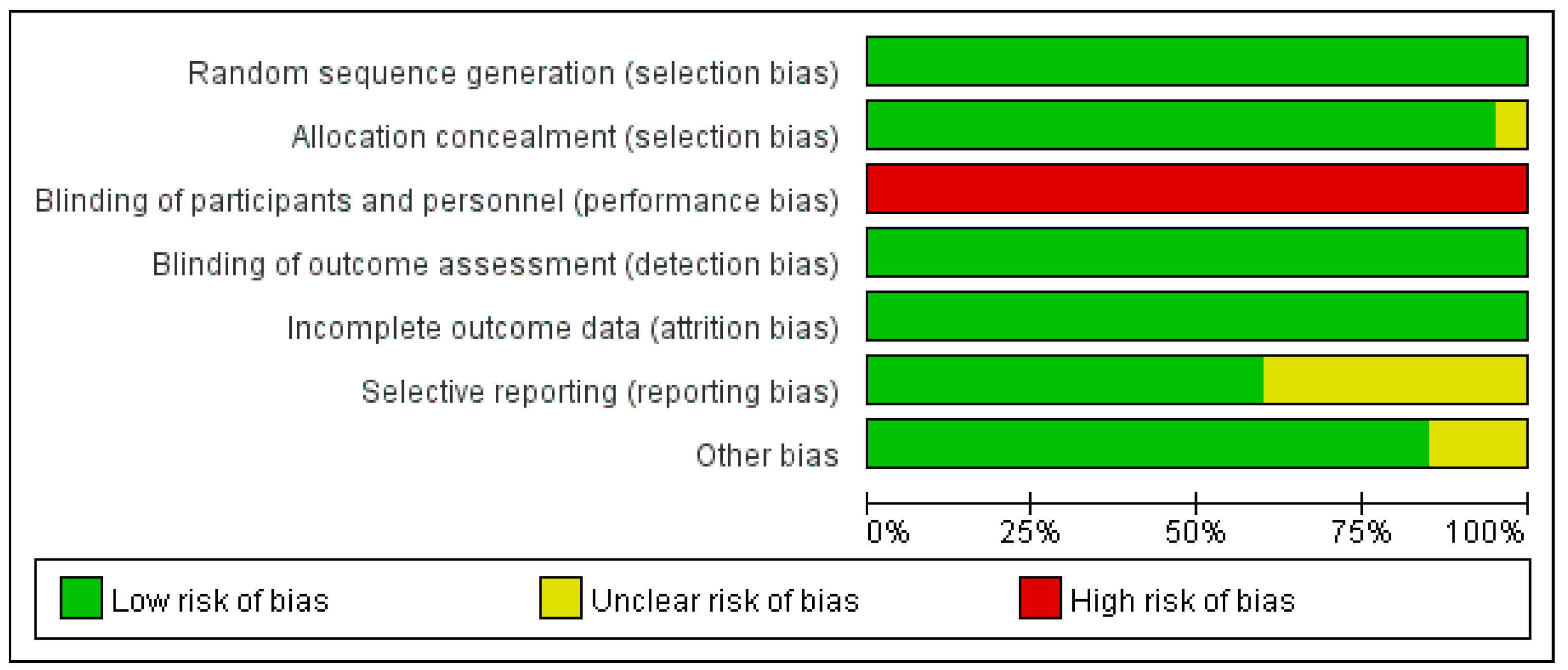
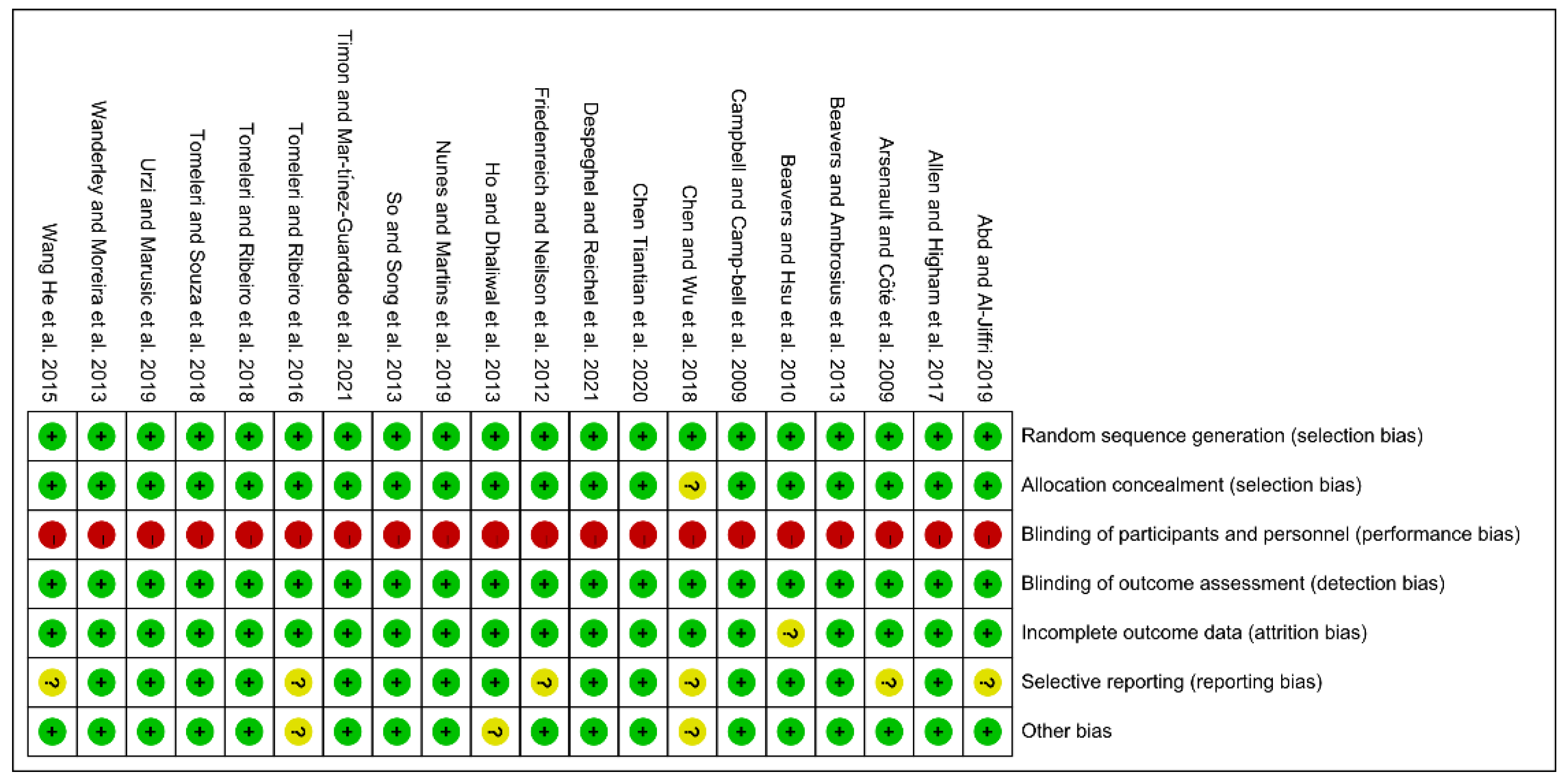
3.2.2. Quality Evaluation of the Selected Literature
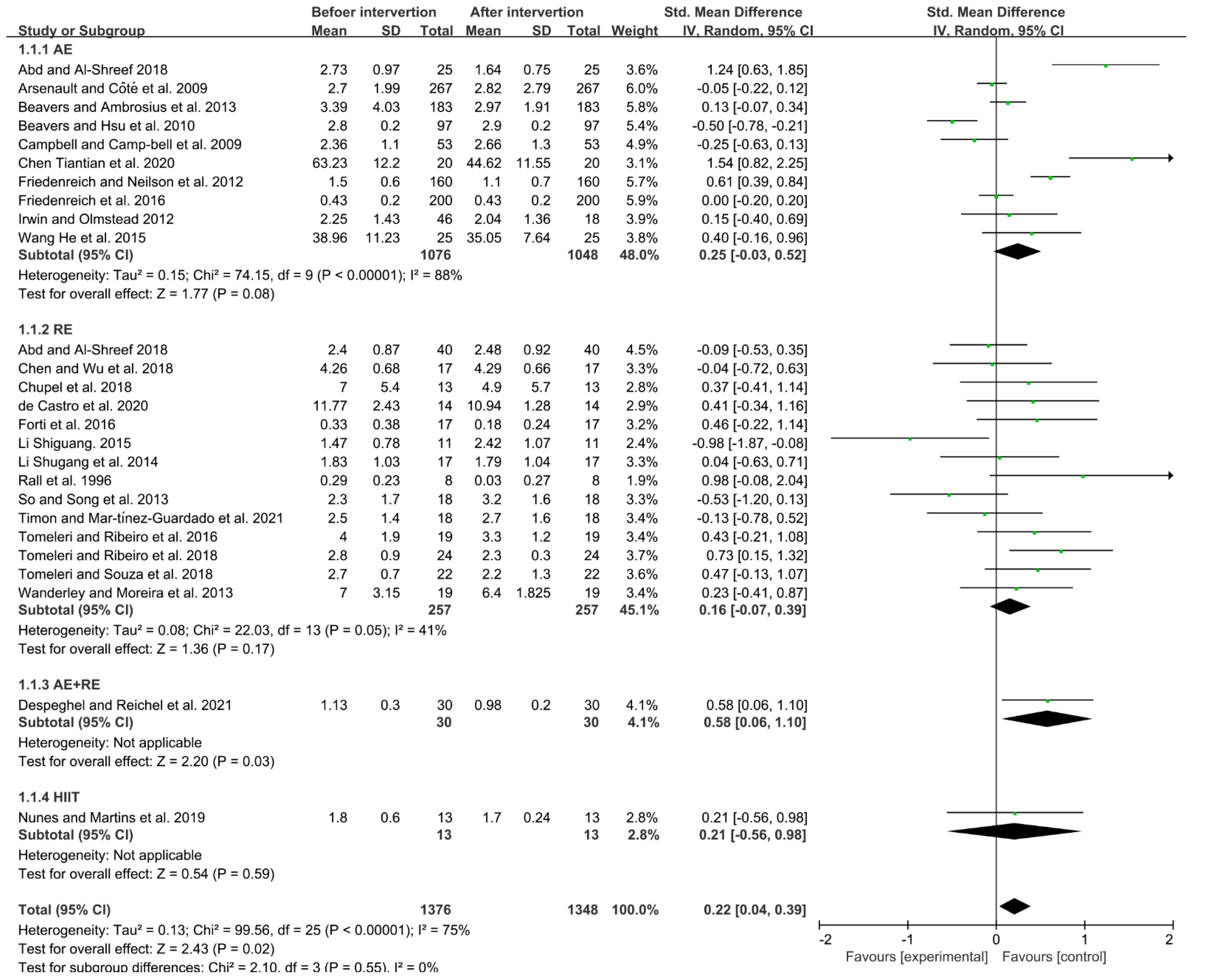
3.3. Effects of Different Exercise Modes on IL-6 in the Elderly
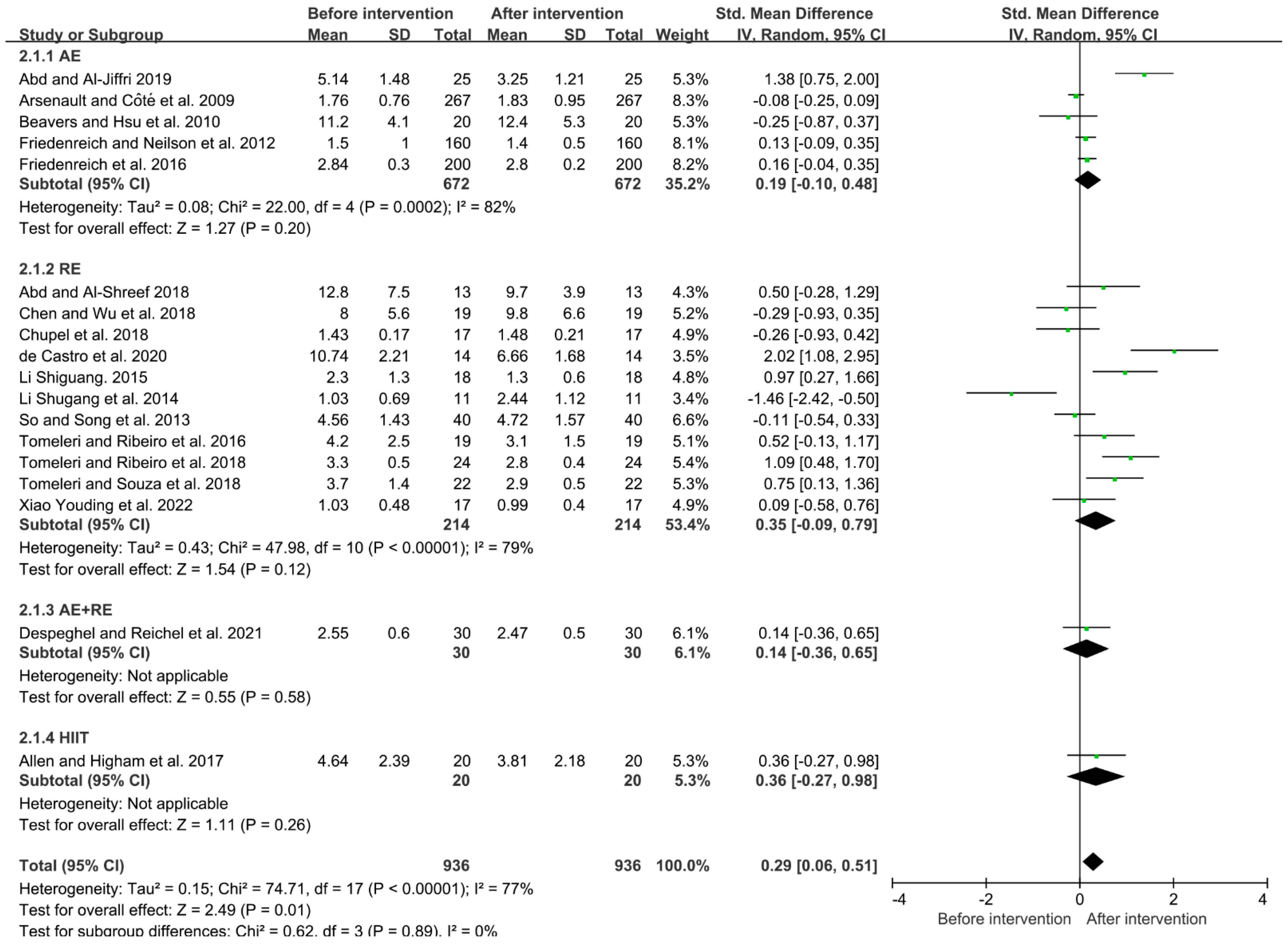
3.4. Effects of Different Exercise Modes on TNF-α in the Elderly
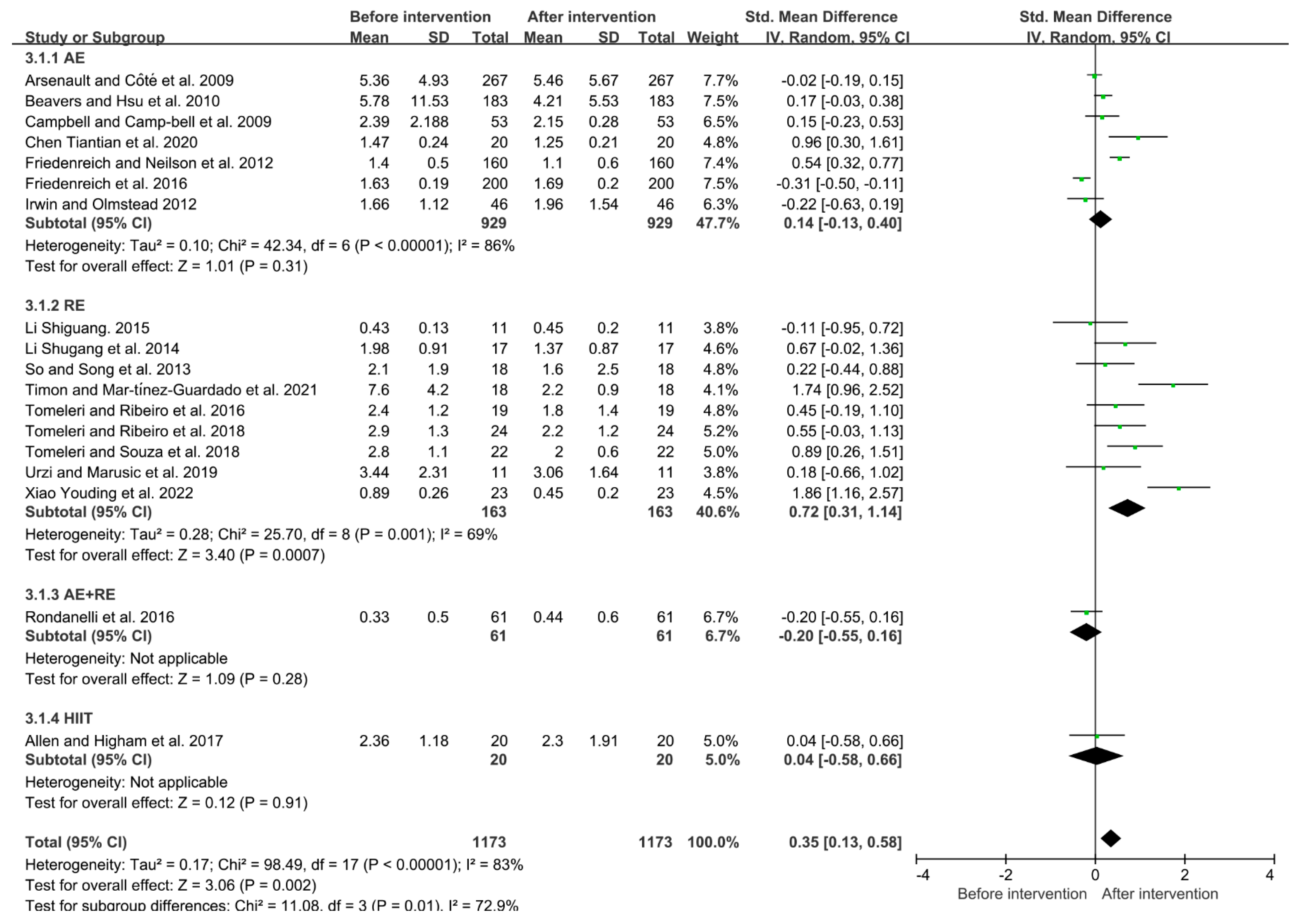
3.5. Effects of Different Exercise Modes on CRP in the Elderly
4. Discussion
5. Limitations of Current Research
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sun, J.Y.; Shuangguan, R.N.; Yan, Y.; Ye, J.P.; Xie, M.H. Research progress on the correlation between cardiopulmonary fitness and inflammatory markers and its mechanism. Chin. J. Rehabil. Med. 2016, 31, 228–234. [Google Scholar]
- Noordam, R.; Oudt, C.H.; Bos, M.M.; Smit, R. High-sensitivity C-reactive protein, low-grade systemic inflammation and type 2 diabetes mellitus: A two-sample Mendelian randomization study. Nutr. Metab. Cardiovasc. Dis. NMCD 2018, 28, 795–802. [Google Scholar] [CrossRef] [PubMed]
- Nuvagah, F.L.; Rose, N.; Ingo, B.; Elke, E.; Romain, M.; Tony, M.; Ivan, B. Strength training reduces circulating interleukin-6 but not brain-derived neurotrophic factor in community-dwelling elderly individuals. Age 2014, 36, 9704. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Chen, P.H.; Xiao, W.H. Obesity leads to skeletal muscle insulin resistance—Mediated by inflammatory factors and ameliorative effects of exercise. Chin. J. Sports Med. 2020, 39, 226–231. [Google Scholar]
- Cong, M.H.; Shi, H.P. Consensus of Chinese experts on exercise therapy for cancer patients. Sci. Sin. Vitae 2022, 52, 587–602. (In Chinese) [Google Scholar] [CrossRef]
- Bruunsgaard, H.; Skinhøj, P.; Pedersen, A.N.; Schroll, M.; Pedersen, B. Ageing, tumour necrosis factor-alpha (TNF-alpha) and atherosclerosis. Clin. Exp. Immunol. 2000, 121, 255–260. [Google Scholar] [CrossRef]
- Abd, E.S.; Al-Shreef, F.M. Inflammatory cytokines and immune system modulation by aerobic versus resisted exercise training for elderly. Afr. Health Sci. 2018, 18, 120–131. [Google Scholar] [CrossRef] [Green Version]
- Monteiro-Junior, R.S.; Maciel-Pinheiro, P.D.; Portugal, E.D.M.; Figueiredo, L.F.D.; Terra, R.; Carneiro, L.S.F.; Rodrigues, V.D.; Nascimento, O.J.M.; Deslandes, A.C.; Laks, J. Effect of Exercise on Inflammatory Profile of Older Persons: Systematic Review and Meta-Analyses. J. Phys. Act. Amp. Health 2018, 15, 64–71. [Google Scholar] [CrossRef]
- Johnson, M.L.; Irving, B.A.; Lanza, I.R.; Vendelbo, M.H.; Konopka, A.R.; Robinson, M.M.; Henderson, G.C.; Klaus, K.A.; Morse, D.M.; Carrie, H. Differential Effect of Endurance Training on Mitochondrial Protein Damage, Degradation, and Acetylation in the Context of Aging. J. Gerontol. 2015, 70, 1386. [Google Scholar] [CrossRef] [Green Version]
- Yousefabadi, H.A.; Niyazi, A.; Alaee, S.; Fathi, M.; Rahimi, G.R.M. Anti-Inflammatory Effects of Exercise on Metabolic Syndrome Patients: A Systematic Review and Meta-Analysis. Biol. Res. Nurs. 2020, 22, 1185452866. [Google Scholar] [CrossRef]
- Kim, S.D.; Yeun, Y.R. Effects of Resistance Training on C-Reactive Protein and Inflammatory Cytokines in Elderly Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2022, 19, 3434. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Sun, Z.; Ya, X.; Zhou, L.; Wang, M.; Wang, X.; Liu, Y. Effect of exercise training on arterial stiffness in obese and overweight children: A meta-analysis. Eur J. Pediatr. 2022, 181, 2633–2642. [Google Scholar] [CrossRef] [PubMed]
- Rall, L.C.; Roubenoff, R.; Cannon, J.G.; Abad, L.W.; Meydani, S.N. Effects of progressive resistance training on immune response in aging and chronic inflammation. Med. Amp. Ence. Sports Amp. Exerc. 1996, 28, 1356–1365. [Google Scholar] [CrossRef]
- Arsenault, B.J.; Côté, M.; Cartier, A.; Lemieux, I.; Després, J.P.; Ross, R.; Earnest, C.P.; Blair, S.N.; Church, T.S. Effect of exercise training on cardiometabolic risk markers among sedentary, but metabolically healthy overweight or obese post-menopausal women with elevated blood pressure. Atherosclerosis 2009, 207, 530–533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, P.T.; Campbell, K.L.; Wener, M.H.; Wood, B.L.; Potter, J.D.; McTiernan, A.; Ulrich, C.M. A yearlong exercise intervention decreases CRP among obese postmenopausal women. Med. Sci. Sports Exerc. 2009, 41, 1533–1539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beavers, K.M.; Hsu, F.C.; Isom, S.; Kritchevsky, S.B.; Church, T.; Goodpaster, B.; Pahor, M.; Nicklas, B.J. Long-term physical activity and inflammatory biomarkers in older adults. Med. Sci. Sports Exerc. 2010, 42, 2189–2196. [Google Scholar] [CrossRef]
- Friedenreich, C.M.; Neilson, H.K.; Woolcott, C.G.; Wang, Q.; Stanczyk, F.Z.; McTiernan, A.; Jones, C.A.; Irwin, M.L.; Yasui, Y.; Courneya, K.S. Inflammatory marker changes in a yearlong randomized exercise intervention trial among postmenopausal women. Cancer Prev. Res. 2012, 5, 98–108. [Google Scholar] [CrossRef] [Green Version]
- Irwin, M.R.; Olmstead, R. Mitigating cellular inflammation in older adults: A randomized controlled trial of Tai Chi Chih. Am. J. Geriatr. Psychiatry 2012, 20, 764–772. [Google Scholar] [CrossRef] [Green Version]
- Beavers, K.M.; Ambrosius, W.T.; Nicklas, B.J.; Rejeski, W.J. Independent and combined effects of physical activity and weight loss on inflammatory biomarkers in overweight and obese older adults. J. Am. Geriatr. Soc. 2013, 61, 1089–1094. [Google Scholar] [CrossRef] [Green Version]
- Ho, S.S.; Dhaliwal, S.S.; Hills, A.P.; Pal, S. Effects of chronic exercise training on inflammatory markers in Australian overweight and obese individuals in a randomized controlled trial. Inflammation 2013, 36, 625–632. [Google Scholar] [CrossRef]
- So, W.Y.; Song, M.; Park, Y.H.; Cho, B.L.; Lim, J.Y.; Kim, S.H.; Song, W. Body composition, fitness level, anabolic hormones, and inflammatory cytokines in the elderly: A randomized controlled trial. Aging Clin. Exp. Res. 2013, 25, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Wanderley, F.A.; Moreira, A.; Sokhatska, O.; Palmares, C.; Moreira, P.; Sandercock, G.; Oliveira, J.; Carvalho, J. Differential responses of adiposity, inflammation and autonomic function to aerobic versus resistance training in older adults. Exp. Gerontol. 2013, 48, 326–333. [Google Scholar] [CrossRef]
- Tomeleri, C.M.; Ribeiro, A.S.; Souza, M.F.; Schiavoni, D.; Schoenfeld, B.J.; Venturini, D.; Barbosa, D.S.; Landucci, K.; Sardinha, L.B.; Cyrino, E.S. Resistance training improves inflammatory level, lipid and glycemic profiles in obese older women: A randomized controlled trial. Exp. Gerontol. 2016, 84, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Li, S.G.; Zhou, Y. Effect of resistance training on muscle content and serum inflammatory factors in the elderly. Chin. J. Gerontol. 2014, 34, 6659–6661. [Google Scholar]
- Wang, H.; Gao, H.N.; Zhao, Z.L. Effects of Long-term Winter Swimming Exercise on Elderly People’s Sex Hormone and Serum Inflammatory Factors. J. Shenyang Sport Univ. 2015, 34, 97–100. [Google Scholar]
- Li, S.G.; Li, W.; Gao, Q.J.; Wang, Y.W. Effects of strength training on aging vascular endothelial function and related mechanisms. Chin. J. Rehabil. Med. 2015, 30, 147–151. [Google Scholar]
- Forti, L.N.; Van Roie, E.; Njemini, R.; Coudyzer, W.; Beyer, I.; Delecluse, C.; Bautmans, I. Load-Specific Inflammation Mediating Effects of Resistance Training in Older Persons. J. Am. Med. Dir. Assoc. 2016, 17, 547–552. [Google Scholar] [CrossRef]
- Friedenreich, C.M.; O’Reilly, R.; Shaw, E.; Stanczyk, F.Z.; Yasui, Y.; Brenner, D.R.; Courneya, K.S. Inflammatory Marker Changes in Postmenopausal Women after a Year-long Exercise Intervention Comparing High Versus Moderate Volumes. Cancer Prev. Res. 2016, 9, 196–203. [Google Scholar] [CrossRef] [Green Version]
- Rondanelli, M.; Klersy, C.; Terracol, G.; Talluri, J.; Maugeri, R.; Guido, D.; Faliva, M.A.; Solerte, B.S.; Fioravanti, M.; Lukaski, H.; et al. Whey protein, amino acids, and vitamin D supplementation with physical activity increases fat-free mass and strength, functionality, and quality of life and decreases inflammation in sarcopenic elderly. Am. J. Clin. Nutr. 2016, 103, 830–840. [Google Scholar] [CrossRef]
- Allen, N.G.; Higham, S.M.; Mendham, A.E.; Kastelein, T.E.; Larsen, P.S.; Duffield, R. The effect of high-intensity aerobic interval training on markers of systemic inflammation in sedentary populations. Eur. J. Appl. Physiol. 2017, 117, 1249–1256. [Google Scholar] [CrossRef]
- Chupel, M.U.; Minuzzi, L.G.; Furtado, G.; Santos, M.L.; Hogervorst, E.; Filaire, E.; Teixeira, A.M. Exercise and taurine in inflammation, cognition, and peripheral markers of blood-brain barrier integrity in older women. Appl. Physiol. Nutr. Metab. 2018, 43, 733–741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.T.; Wu, H.J.; Chen, Y.J.; Ho, S.Y.; Chung, Y.C. Effects of 8-week kettlebell training on body composition, muscle strength, pulmonary function, and chronic low-grade inflammation in elderly women with sarcopenia. Exp. Gerontol. 2018, 112, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Tomeleri, C.M.; Ribeiro, A.S.; Cavaglieri, C.R.; Deminice, R.; Schoenfeld, B.J.; Schiavoni, D.; Dos, S.L.; de Souza, M.F.; Antunes, M.; Venturini, D.; et al. Correlations between resistance training-induced changes on phase angle and biochemical markers in older women. Scand. J. Med. Sci. Sports 2018, 28, 2173–2182. [Google Scholar] [CrossRef] [PubMed]
- Tomeleri, C.M.; Souza, M.F.; Burini, R.C.; Cavaglieri, C.R.; Ribeiro, A.S.; Antunes, M.; Nunes, J.P.; Venturini, D.; Barbosa, D.S.; Sardinha, L.B.; et al. Resistance training reduces metabolic syndrome and inflammatory markers in older women: A randomized controlled trial. J. Diabetes 2018, 10, 328–337. [Google Scholar] [CrossRef] [PubMed]
- Abd, E.S.; Al-Jiffri, O.H. Aerobic exercise modulates cytokine profile and sleep quality in elderly. Afr. Health Sci. 2019, 19, 2198–2207. [Google Scholar] [CrossRef] [Green Version]
- Nunes, P.; Martins, F.M.; Souza, A.P.; Carneiro, M.; Orsatti, C.L.; Michelin, M.A.; Murta, E.; de Oliveira, E.P.; Orsatti, F.L. Effect of high-intensity interval training on body composition and inflammatory markers in obese postmenopausal women: A randomized controlled trial. Menopause 2019, 26, 256–264. [Google Scholar] [CrossRef]
- Urzi, F.; Marusic, U.; Ličen, S.; Buzan, E. Effects of Elastic Resistance Training on Functional Performance and Myokines in Older Women-A Randomized Controlled Trial. J. Am. Med. Dir. Assoc. 2019, 20, 830–834. [Google Scholar] [CrossRef]
- Chen, T.T.; Li, N.C.; Wang, H.W.; He, L.; Li, S.Y.; Hu, Y.L. Effects of Tai-Chi Exercise on Blood Lipids, Inflammatory Factors and BaPWV of Middle-Aged and Elderly People. J. Anhui Sports Sci. 2020, 41, 63–66. [Google Scholar]
- de Castro, D.; Da, C.N.D.; Orsano, V.; de Sousa, N.I.; Beal, F.; Stone, W.; Dos, S.R.T.; Prestes, J. Effect of high-velocity and traditional resistance exercise on serum antioxidants and inflammation biomarkers in older women: A randomized crossover trial. Exp. Gerontol. 2020, 139, 111026. [Google Scholar] [CrossRef]
- Despeghel, M.; Reichel, T.; Zander, J.; Krüger, K.; Weyh, C. Effects of a 6 Week Low-Dose Combined Resistance and Endurance Training on T Cells and Systemic Inflammation in the Elderly. Cells 2021, 10, 843. [Google Scholar] [CrossRef]
- Timon, R.; Martínez-Guardado, I.; Camacho-Cardeñosa, A.; Villa-Andrada, J.M.; Olcina, G.; Camacho-Cardeñosa, M. Effect of intermittent hypoxic conditioning on inflammatory biomarkers in older adults. Exp. Gerontol. 2021, 152, 111478. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Y.D.; Wei, S.M. The effects of resistance training on cardiovascular efficiency in older adults and related mechanisms: A pilot of study. Chin. J. Rehabil. Med. 2022, 37, 202–209. [Google Scholar]
- Rybka, J.; Kupczyk, D.; Kędziora-Kornatowska, K.; Pawluk, H.; Czuczejko, J.; Szewczyk-Golec, K.; Kozakiewicz, M.; Antonioli, M.; Carvalho, L.A.; Kędziora, J. Age-related changes in an antioxidant defense system in elderly patients with essential hypertension compared with healthy controls. Redox Rep. 2011, 16, 71–77. [Google Scholar] [CrossRef]
- Welsh, C.; Celis-Morales, C.A.; Brown, R.; Mackay, D.F.; Lewsey, J.; Mark, P.B.; Gray, S.R.; Ferguson, L.D.; Anderson, J.J.; Lyall, D.M.; et al. Comparison of Conventional Lipoprotein Tests and Apolipoproteins in the Prediction of Cardiovascular Disease. Circulation 2019, 140, 542–552. [Google Scholar] [CrossRef] [PubMed]
- Leggate, M. The IL-6 system and its interaction with chronic low-grade inflammation and high intensity intermittent exercise. Ph.D. Thesis, Loughborough University, Loughborough, UK, 2012. [Google Scholar]
- Liu, J.Q.; Lu, J.D.; Liang, T.Q.; Chen, S.N.; Su, H. Effect of resistance training on interleukin-6 and C-reactive protein in middle-age and elderly people: A Meta-analysis. Chin. J. Tissue Eng. Res. 2022, 43, 45–52. [Google Scholar] [CrossRef]
- Shi, M.L. Effect of Different Modes of Exercise Training on IL-6, TNF-α and hs-CRP. J. Xi’an Phys. Educ. Univ. 2011, 28, 481–488. [Google Scholar]
- Bremer, A.A.; Jialal, I. Adipose Tissue Dysfunction in Nascent Metabolic Syndrome. J. Obes. 2013, 2013, 393192. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author | Year | Type of Study, Health Condition | Age (Years) | Sample Size (n) | Intervention | Frequency | Duration | Outcome | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Control Group | Intervention Group | Control Group | Intervention Group | |||||||
| Rall and Roubenoff et al. [13] | 1996 | SCT, Healthy | 70.3 ± 5.0 | 8 | RE | 1/2W | 12 W | IL-6 | ||
| Arsenault and Côté et al. [14] | 2009 | RCT, Overweight/Obesity | 57.2 ± 6.1 | 57.3 ± 6.6 | 82 | 267 | AE | 3–4/W | 6 M | IL-6, TNF-α, CRP |
| Campbell and Campbell et al. [15] | 2009 | RCT, Overweight | 60.9 ± 6.8 | 60.5 ± 7.0 | 62 | 53 | AE | 12 M | CRP, IL-6 | |
| Beavers and Hsu et al. [16] | 2010 | RCT, Healthy | 77.0 ± 4.4 | 76.4 ± 4.1 | 186 | 183 | AE | 3/W | 12 M | IL-6, CRP |
| Friedenreich and Neilson et al. [17] | 2012 | RCT, Healthy | 60.6 ± 5.7 | 61.2 ± 5.4 | 160 | 160 | AE | 5/W | 12 M | IL-6, TNF-α, CRP |
| Irwin and Olmstead [18] | 2012 | SCT, Healthy | 70.7 ± 5.9 | 46 | AE | 2/W | 25 W | IL-6, CRP | ||
| Beavers and Ambrosius et al. [19] | 2013 | RCT, Overweight/Obesity | 60–79 | 60–79 | 93 | 97 | AE | 5/W | 18 M | IL-6 |
| Ho and Dhaliwal et al. [20] | 2013 | RCT, Overweight/Obesity | 52 (40–66) | 53 (43–64) | 16 | 17 | AE+RE | 3/W | 12 M | IL-6, TNF-α |
| So and Song et al. [21] | 2013 | RCT, Healthy | 68.4 ± 5.8 | 71.6 ± 5.5 | 22 | 18 | RE | 3/W | 12 W | IL-6, TNF-α |
| Wanderley and Moreira et al. [22] | 2013 | RCT, Healthy | 67.8 ± 5.5 | 67.3 ± 4.9 | 11 | 19 | RE | 2/W 8/M | IL-6, TNF-α | |
| 69.9 ± 5.7 | 20 | AE | ||||||||
| Tomeleri and Ribeiro et al. [23] | 2016 | RCT, Healthy | 69.5 ± 4.7 | 66.8 ± 3.2 | 19 | 19 | RE | 3/W | 8 W | IL-6, TNF-α, CRP |
| Li Shugang et al. [24] | 2014 | SCT, Healthy | 65.65 ± 3.14 | 17 | RE | 2/W | 16 W | IL-6, TNF, CRP | ||
| Wang He et al. [25] | 2015 | RCT, Healthy | 63.39 ± 3.43 | 63.53 ± 3.12 | 20 | 25 | AE | 5/W | 6 M | IL-6, TNF |
| Li Shiguang er al. [26] | 2015 | SCT, Healthy | 70.63 ± 3.93 | 11 | RE | 3/W | 12 W | IL-6, TNF, CRP | ||
| Forti and Van Roie et al. [27] | 2016 | SCT, Healthy | 67.86 ± 4.36 | 17 | RE | 3/W | 12 W | IL-6 | ||
| Friedenreich and O’Reilly et al. [28] | 2016 | SCT, Healthy | 59.4 ± 4.8 | 200 | AE | 5/W | 12 M | IL-6, TNF-α, CRP | ||
| Rondanelli and Klersy et al. [29] | 2016 | SCT, Healthy | 80.21 ± 8.54 | 61 | AE + RE | 5/W | 12 W | CRP | ||
| Allen and Higham et al. [30] | 2017 | RCT, Healthy | 49.2 ± 6.1 | 14 | 20 | HIIT | 3/W | 9 W | TNF-α, CRP | |
| Chupel and Minuzzi et al. [31] | 2018 | SCT, Healthy | 83.5 ± 7.3 | 13 | RE | 2/W | 14 W | IL-6, TNF-α | ||
| Chen and Wu et al. [32] | 2018 | RCT, Healthy | 68.3 ± 2.8 | 66.7 ± 5.3 | 16 | 17 | RE | 2/W | 8 W | CRP, IL-6, TNF-α |
| Tomeleri and Ribeiro et al. [33] | 2018 | RCT, Healthy | 68.8 ± 4.6 | 71.0 ± 5.4 | 22 | 24 | RE | 3/W | 12 W | IL-6, TNF-α, CRP |
| Tomeleri and Souza et al. [34] | 2018 | RCT, Healthy | 68.8 ± 4.9 | 72.1 ± 6.3 | 23 | 22 | RE | 3/W | 18 W | IL-6, TNF-α, CRP |
| Abd and Al-Shreef [7] | 2018 | SCT, Healthy | 65.96 ± 3.42 | 40 | RE | 3/W | 6 M | IL-6, TNF-α | ||
| Abd and Al-Jiffri [35] | 2019 | RCT, Healthy | 61–67 | 25 | 25 | AE | 3/W | 6 M | IL-6, TNF-α | |
| Nunes and Martins et al. [36] | 2019 | RCT, Healthy | 62.9 ± 2.25 | 62.3 ± 2.08 | 13 | 13 | HIIT | 3/W | 12 W | IL-6 |
| Urzi and Marusic et al. [37] | 2019 | RCT, Healthy | 88.9 ± 5.3 | 84.4 ± 7.7 | 9 | 11 | RE | 3/W | 12 W | CRP |
| Chen Tiantian et al. [38] | 2020 | RCT, Healthy | 63.59 ± 2.21 | 64.75 ± 2.89 | 10 | 20 | AE | 6/W | 12 M | IL-6, CRP |
| de Castro and Da et al. [39] | 2020 | SCT, Healthy | 67.36 ± 7.13 | 14 | RE | Dis | IL-6, TNF-α | |||
| Despeghel and Reichel et al. [40] | 2021 | RCT, Healthy | 69.8 ± 4.4 | 70.4 ± 5.3 | 10 | 30 | AE + RE | - | 6 W | IL-6, TNF-α |
| Timon and Martínez-Guardado et al. [41] | 2021 | RCT, Healthy | 70.5 ± 4.0 | 70.3 ± 3.3 | 19 | 18 | RE | 3/W | 24 W | IL-6, CRP |
| Xiao Youding et al. [42] | 2022 | SCT, Healthy | 70.79 ± 4.91 | 23 | RE | 3/W | 16 W | TNF-α, CRP | ||
| Study | Bias Due to Confounding | Bias in Selection of Participants into the Study | Bias in Classification of Interventions | Bias Due to Deviations from Intended Interventions | Bias Due to Missing Data | Bias in Measurement of Outcomes | Bias in Selection of the Reported Result |
|---|---|---|---|---|---|---|---|
| Abd and Al-Shreef [7] | Low risk | Low risk | Low risk | High risk | Low risk | Low risk | Low risk |
| Chupel and Minuzzi et al. [31] | Low risk | Low risk | Low risk | High risk | Low risk | Low risk | Low risk |
| de Castro and Da et al. [39] | Low risk | Low risk | Low risk | High risk | Low risk | Low risk | Low risk |
| Forti and Van Roie et al. [27] | Low risk | Low risk | Low risk | High risk | Low risk | Low risk | Low risk |
| Friedenreich and O’Reilly et al. [28] | Low risk | Low risk | Low risk | High risk | Low risk | Low risk | Low risk |
| Irwin and Olmstead [18] | Low risk | Low risk | Low risk | High risk | Low risk | Low risk | Low risk |
| Rall and Roubenoff et al. [13] | Medium risk | Low risk | Low risk | High risk | Low risk | Low risk | Low risk |
| Rondanelli and Klersy et al. [29] | Low risk | Low risk | Low risk | High risk | Low risk | Low risk | Low risk |
| Li Shiguang et al. [26] | Low risk | Low risk | Low risk | High risk | Low risk | Medium risk | Low risk |
| Li Shugang et al. [24] | Low risk | Low risk | Low risk | High risk | Low risk | Medium risk | Low risk |
| Xiao Youding et al. [42] | Medium risk | Low risk | Low risk | High risk | Low risk | Medium risk | Low risk |
| Subgroup | IL-6 | TNF-α | CRP | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Intervention | Effect Size | 95% CI | n | I2 | Effect Size | 95% CI | n | I2 | Effect Size | 95% CI | n | I2 |
| AE | 0.25 | −0.03, 0.52 | 1076 | 88% | 0.19 | −0.10, 0.48 | 672 | 82% | 0.14 | −0.13, 0.40 | 929 | 86% |
| RE | 0.16 | −0.07, 0.39 | 257 | 41% | 0.35 | −0.09, 0.79 | 214 | 79% | 0.72 | 0.31, 1.14 | 163 | 89% |
| AE + RE | 0.58 | 0.06, 1.10 | 30 | — | 0.14 | −0.36, 0.65 | 30 | — | −0.2 | −0.55, 0.16 | 61 | — |
| HIIT | 0.21 | −0.56, 0.98 | 13 | — | 0.36 | −0.27, 0.98 | 20 | — | 0.04 | −0.58, 0.66 | 20 | — |
| Total | 0.22 | 0.04, 0.39 | 1376 | 75% | 0.29 | 0.06, 0.51 | 936 | 77% | 0.35 | 0.13, 0.58 | 1173 | 83% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, H.; He, Z.; Yun, H.; Wang, R.; Liu, C. A Meta-Analysis of the Effects of Different Exercise Modes on Inflammatory Response in the Elderly. Int. J. Environ. Res. Public Health 2022, 19, 10451. https://doi.org/10.3390/ijerph191610451
Zhao H, He Z, Yun H, Wang R, Liu C. A Meta-Analysis of the Effects of Different Exercise Modes on Inflammatory Response in the Elderly. International Journal of Environmental Research and Public Health. 2022; 19(16):10451. https://doi.org/10.3390/ijerph191610451
Chicago/Turabian StyleZhao, Haotian, Zhijian He, Hezhang Yun, Ruifu Wang, and Chang Liu. 2022. "A Meta-Analysis of the Effects of Different Exercise Modes on Inflammatory Response in the Elderly" International Journal of Environmental Research and Public Health 19, no. 16: 10451. https://doi.org/10.3390/ijerph191610451