
Reducing the Effectiveness of Ward Particulate Matter, Bacteria and Influenza Virus by Combining Two Complementary Air Purifiers

Abstract
:1. Introduction
2. Materials and Methods
2.1. Pollutant and Experimental Equipment
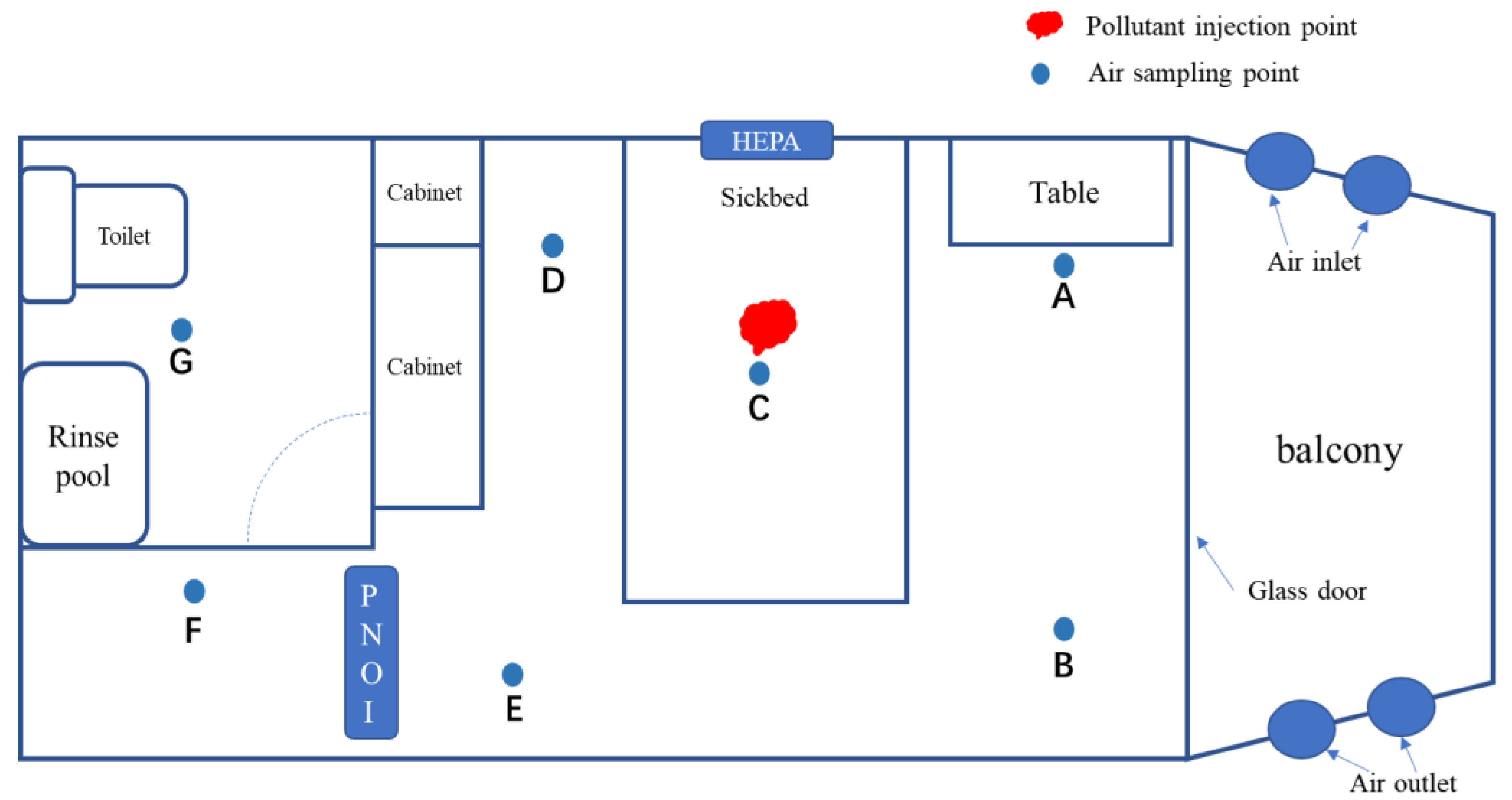
2.2. Experimental Scene
2.3. Air Purifiers
2.4. Formation of Heavily Polluted Environment
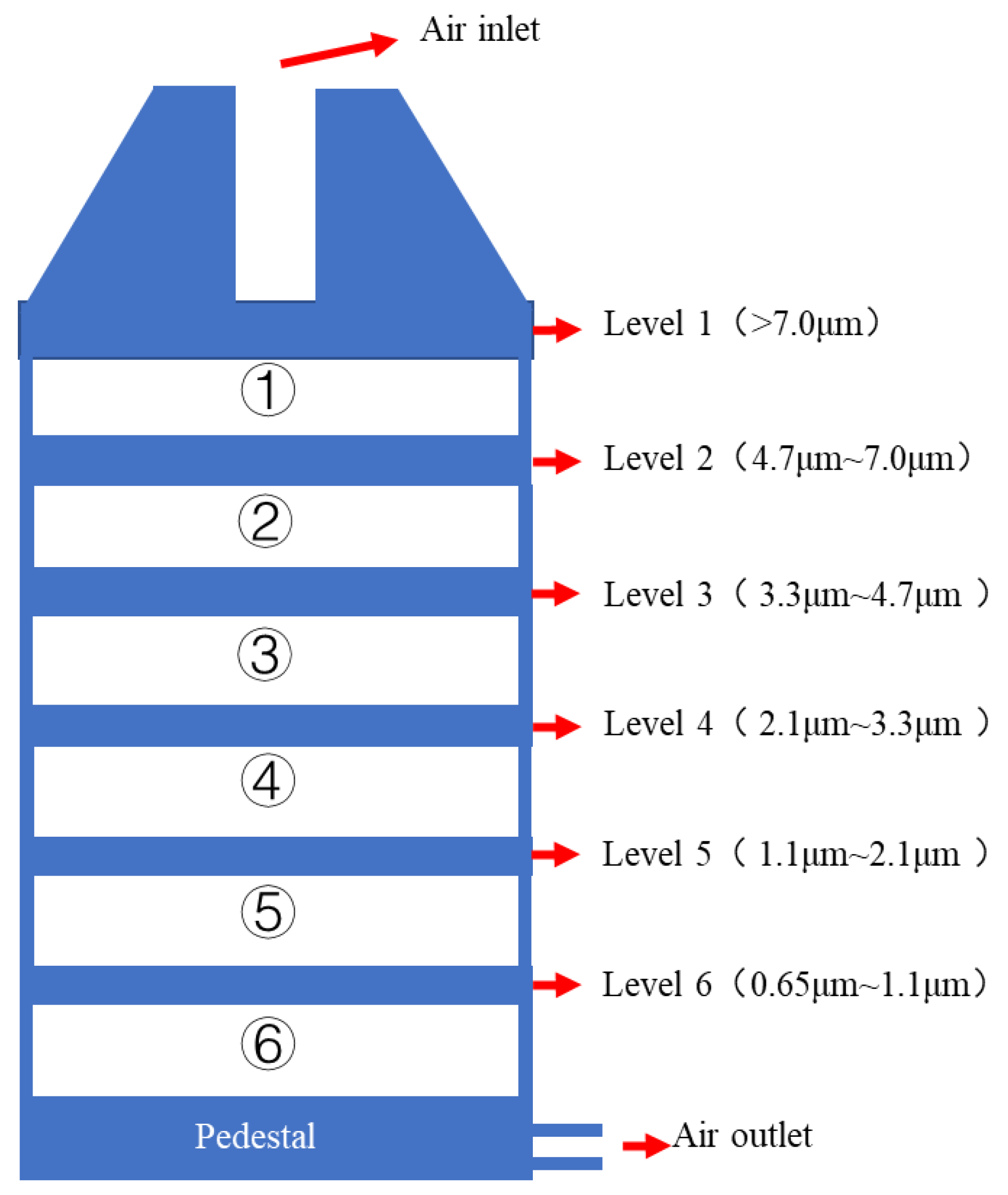
2.5. Collection and Detection of Samples
2.6. Quality Control
2.7. Data Analysis and Calculation Formula
3. Results
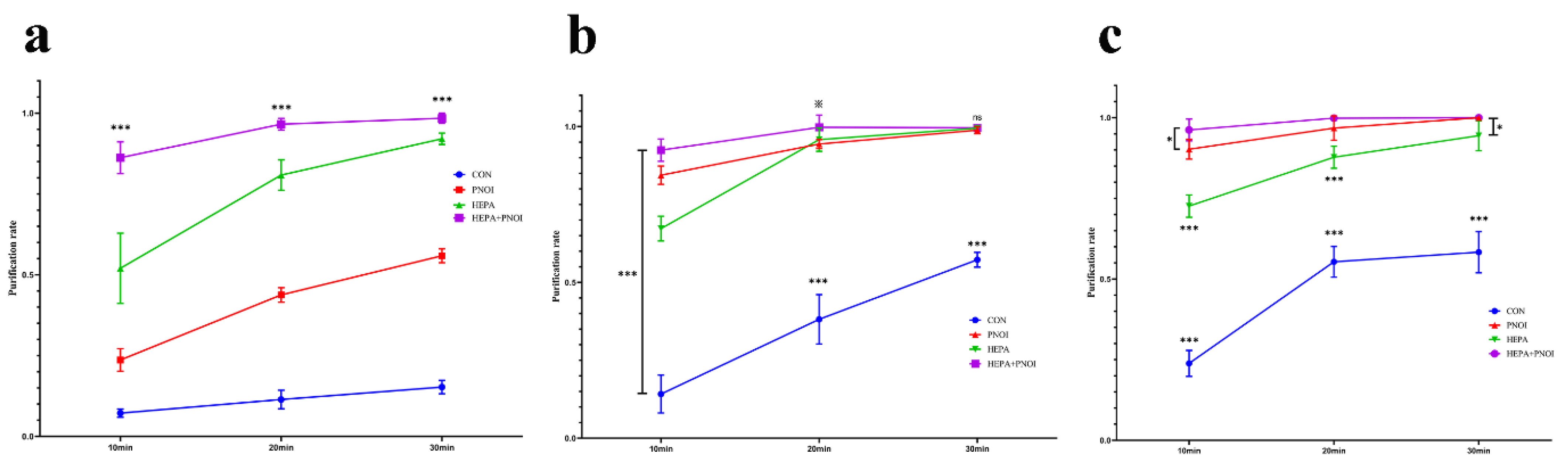
3.1. Preliminary Purification of Three Air Pollutants by Two Purifiers
3.2. Combined Application was Effective for Different Positions and Particle Sizes
3.3. Combination Application Accelerates Influenza Virus Inactivation
3.4. Combination Application Better than Common UV Disinfection
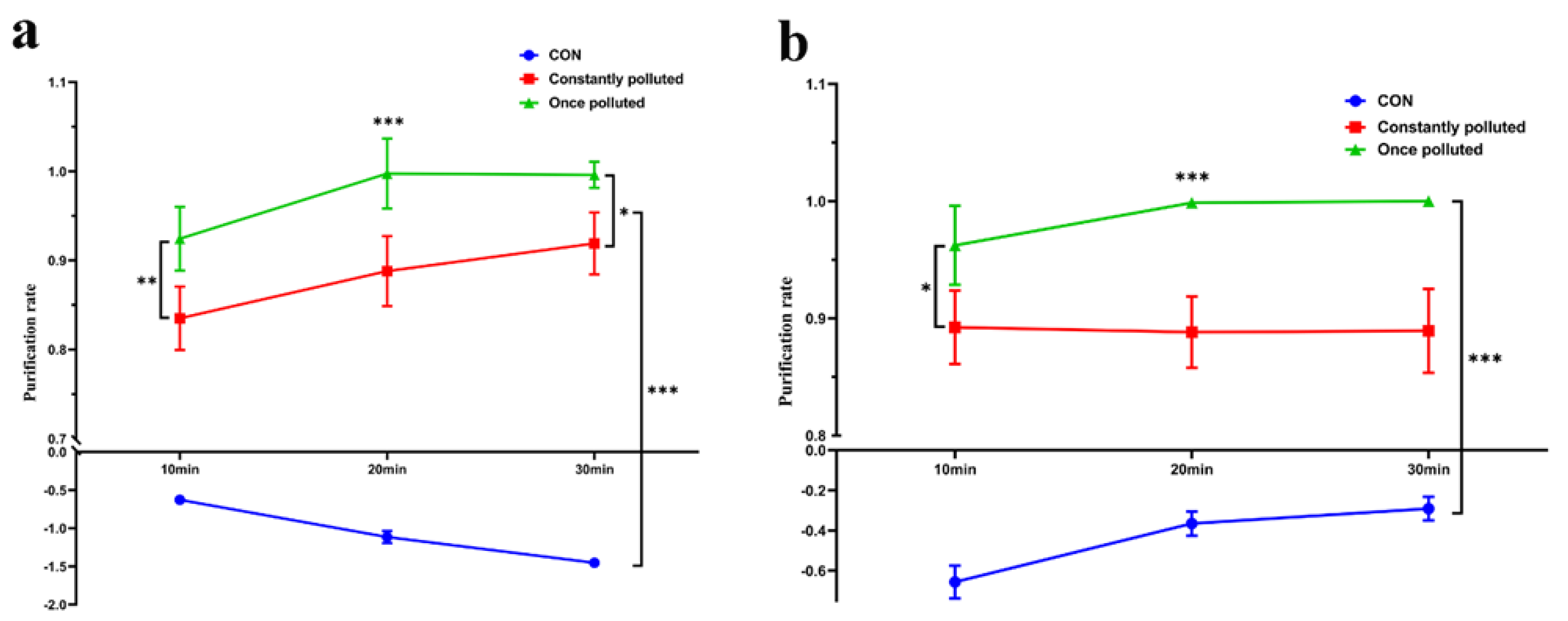
3.5. Combination Applications Still Have Better Effects on Continuously Polluted Environments
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Rickman, H.M.; Rampling, T.; Shaw, K.; Martinez-Garcia, G.; Hail, L.; Coen, P.; Shahmanesh, M.; Shin, G.Y.; Nastouli, E.; Houlihan, C.F. Nosocomial Transmission of Coronavirus Disease 2019: A Retrospective Study of 66 Hospital-acquired Cases in a London Teaching Hospital. Clin. Infect. Dis. 2021, 72, 690–693. [Google Scholar] [CrossRef]
- Tauffer, J.; Konstantyner, T.; de Almeida, M.; Ferreira, D.B.; Antonelli, T.S.; Fram, D.S.; Escudero, D.V.; Ferreira, P.R.A.; Bellei, N.; Colombo, A.L.; et al. Impact of In-Hospital infection with SARS-CoV-2 among Inpatients at a university hospital. Am. J. Infect. Control 2021, 49, 1464–1468. [Google Scholar] [CrossRef] [PubMed]
- Song, Z.; Xu, Y.; Bao, L.; Zhang, L.; Yu, P.; Qu, Y.; Zhu, H.; Zhao, W.; Han, Y.; Qin, C. From SARS to MERS, Thrusting Coronaviruses into the Spotlight. Viruses 2019, 11, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunter, J.C.; Nguyen, D.; Aden, B.; Bandar, Z.A.; Hosani, F.I.A. Transmission of Middle East Respiratory Syndrome Coronavirus Infections in Healthcare Settings, Abu Dhabi. Emerg. Infect. Dis. 2016, 22, 647–656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klevens, R.M.; Edwards, J.R.; Richards, C.J.; Horan, T.C.; Gaynes, R.P.; Pollock, D.A.; Cardo, D.M. Estimating health care-associated infections and deaths in U.S. hospitals, 2002. Public Health Rep. 2007, 122, 160–166. [Google Scholar] [CrossRef]
- Haque, M.; Sartelli, M.; Mckimm, J.; Abu Bakar, M.B. Health care-associated infections-An overview. Infect. Drug Resist. 2018, 11, 2321–2333. [Google Scholar] [CrossRef] [Green Version]
- Zemouri, C.; de Soet, H.; Crielaard, W.; Laheij, A. A scoping review on bio-aerosols in healthcare and the dental environment. PLoS ONE 2017, 12, e0178007. [Google Scholar] [CrossRef]
- Butt, I.A.; Aslam, B.; Rasool, M.H.; Shafiq, H.B.; Khurshid, M.; Aslam, M.A. Distribution of various pathogenic bacteria from pediatric ward settings. Saudi Med. J. 2016, 37, 1268–1271. [Google Scholar] [CrossRef]
- Wang, J.; Liu, F.; Tartari, E.; Huang, J.; Harbarth, S.; Pittet, D.; Zingg, W. The Prevalence of Healthcare-Associated Infections in Mainland China: A Systematic Review and Meta-analysis. Infect Control Hosp. Epidemiol. 2018, 39, 701–709. [Google Scholar] [CrossRef]
- Revelas, A. Healthcare-associated infections: A public health problem. Niger. Med. J. 2012, 53, 59–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cassini, A.; Högberg, L.D.; Plachouras, D.; Quattrocchi, A.; Hoxha, A.; Simonsen, G.S.; Colomb-Cotinat, M.; Kretzschmar, M.E.; Devleesschauwer, B.; Cecchini, M.; et al. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European Economic Area in 2015: A population-level modelling analysis. Lancet Infect Dis. 2019, 19, 56–66. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.C.; Prather, K.A.; Sznitman, J.; Jimenez, J.L.; Lakdawala, S.S.; Tufekci, Z.; Marr, L.C. Airborne transmission of respiratory viruses. Science 2021, 373, eabd9149. [Google Scholar] [CrossRef] [PubMed]
- Mousavi, E.S.; Kananizadeh, N.; Martinello, R.A.; Sherman, J.D. COVID-19 Outbreak and Hospital Air Quality: A Systematic Review of Evidence on Air Filtration and Recirculation. Environ. Sci. Technol. 2021, 55, 4134–4147. [Google Scholar] [CrossRef]
- Mohammadi, A.; Soleimani, A.; Abdolahnejad, A.; Ahmed, M.; Akther, T.; Nemati-Mansour, S.; Raeghi, S.; Rashedi, G.H.; Mirig, M. SARS-CoV-2 detection in hospital indoor environments, NW Iran. Atmos. Pollut. Res. 2022, 13, 101511. [Google Scholar] [CrossRef]
- Limaylla, D.C.; Silva, M.O.; Fortaleza, C. Temperature, humidity, and climate control in hospital units: A clue for understanding the seasonality of healthcare-associated pathogens. Infect. Control Hosp. Epidemiol. 2019, 40, 829–830. [Google Scholar] [CrossRef] [Green Version]
- Drohan, S.E.; Levin, S.A.; Grenfell, B.T.; Laxminarayan, R. Incentivizing hospital infection control. Proc. Natl. Acad. Sci. USA 2019, 116, 6221–6225. [Google Scholar] [CrossRef] [Green Version]
- Schwierzeck, V.; König, J.C.; Kühn, J.; Mellmann, A.; Correa-Martínez, C.L.; Omran, H.; Konrad, M.; Kaiser, T.; Kampmeier, S. First Reported Nosocomial Outbreak of Severe Acute Respiratory Syndrome Coronavirus 2 in a Pediatric Dialysis Unit. Clin. Infect. Dis. 2021, 72, 265–270. [Google Scholar] [CrossRef]
- Stawicki, S.P.; Wolfe, S.; Brisendine, C.; Eid, S.; Zangari, M.; Ford, F.; Snyder, B.; Moyer, W.; Levicoff, L.; Burfeind, W.R. The impact of comprehensive air purification on patient duration of stay, discharge outcomes, and health care economics: A retrospective cohort study. Surgery 2020, 168, 968–974. [Google Scholar] [CrossRef]
- Sharpe, P.A.; Schmidt, M.G. Control and mitigation of healthcare-acquired infections: Designing clinical trials to evaluate new materials and technologies. HERD 2011, 5, 94–115. [Google Scholar] [CrossRef]
- Kim, K.H.; Kabir, E.; Jahan, S.A. Airborne bioaerosols and their impact on human health. J. Environ. Sci. (China) 2018, 67, 23–35. [Google Scholar] [CrossRef]
- Coccia, M. High health expenditures and low exposure of population to air pollution as critical factors that can reduce fatality rate in COVID-19 pandemic crisis: A global analysis. Environ. Res. 2021, 199, 111339. [Google Scholar] [CrossRef] [PubMed]
- Masoumbeigi, H.; Ghanizadeh, G.; Yousefi, A.R.; Heydari, S.; Goodarzi, H.; Dorostkar, S.R.; Tat, M. Investigation of hospital indoor air quality for the presence of SARS-Cov-2. J. Environ. Health Sci. Eng. 2020, 18, 1259–1263. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.H.; Kim, J.H.; Kim, S.; Lee, S.; Lim, D.H. Effects of Indoor Air Purifiers on Children with Asthma. Yonsei Med. J. 2020, 61, 310–316. [Google Scholar] [CrossRef] [PubMed]
- Zacharias, N.; Haag, A.; Brang-Lamprecht, R.; Gebel, J.; Essert, S.M.; Kistemann, T.; Exner, M.; Mutters, N.T.; Engelhart, S. Air filtration as a tool for the reduction of viral aerosols. Sci. Total Environ. 2021, 772, 144956. [Google Scholar] [CrossRef]
- Weiss, C.; Carriere, M.; Fusco, L.; Capua, I.; Regla-Nava, J.A.; Pasquali, M.; Scott, J.A.; Vitale, F.; Unal, M.A.; Mattevi, C.; et al. Toward Nanotechnology-Enabled Approaches against the COVID-19 Pandemic. ACS Nano 2020, 14, 6383–6406. [Google Scholar] [CrossRef]
- Dubey, S.; Rohra, H.; Taneja, A. Assessing effectiveness of air purifiers (HEPA) for controlling indoor particulate pollution. Heliyon 2021, 7, e07976. [Google Scholar] [CrossRef]
- Hashimoto, K.; Kawakami, Y. Effectiveness of Airborne Fungi Removal by using a HEPA Air Purifier Fan in Houses. Biocontrol. Sci. 2018, 23, 215–221. [Google Scholar] [CrossRef] [Green Version]
- Pirkle, S.; Bozarth, S.; Robinson, N.; Hester, W.; Wagner, L.; Broome, S.; Allen, K.; Mannepalli, S. Evaluating and contextualizing the efficacy of portable HEPA filtration units in small exam rooms. Am. J. Infect. Control 2021, 49, 1506–1510. [Google Scholar] [CrossRef]
- Schraufnagel, D.E.; Balmes, J.R.; Cowl, C.T.; De Matteis, S.; Jung, S.H.; Mortimer, K.; Perez-Padilla, R.; Rice, M.B.; Riojas-Rodriguez, H.; Sood, A.; et al. Air Pollution and Noncommunicable Diseases: A Review by the Forum of International Respiratory Societies’ Environmental Committee, Part 1: The Damaging Effects of Air Pollution. Chest 2019, 155, 409–416. [Google Scholar] [CrossRef] [Green Version]
- Fennelly, K.P. Particle sizes of infectious aerosols: Implications for infection control. Lancet Respir. Med. 2020, 8, 914–924. [Google Scholar] [CrossRef]
- Sudharsanam, S.; Swaminathan, S.; Ramalingam, A.; Thangavel, G.; Annamalai, R.; Steinberg, R.; Balakrishnan, K.; Srikanth, P. Characterization of indoor bioaerosols from a hospital ward in a tropical setting. Afr. Health Sci. 2012, 12, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, S. Seasonal variability in size-segregated airborne bacterial particles and their characterization at different source-sites. Environ. Sci. Pollut. Res. Int. 2017, 24, 13519–13527. [Google Scholar] [CrossRef] [PubMed]
- Lindsley, W.G.; Blachere, F.M.; Thewlis, R.E.; Vishnu, A.; Davis, K.A.; Cao, G.; Palmer, J.E.; Clark, K.E.; Fisher, M.A.; Khakoo, R.; et al. Measurements of airborne influenza virus in aerosol particles from human coughs. PLoS ONE 2010, 5, e15100. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Chen, H.; Yao, M.; Li, X. Bacterial pathogens were detected from human exhaled breath using a novel protocol. J. Aerosol. Sci. 2018, 117, 224–234. [Google Scholar] [CrossRef]
- Carpagnano, G.E.; Malerba, M.; Lacedonia, D.; Susca, A.; Logrieco, A.; Carone, M.; Cotugno, G.; Palmiotti, G.A.; Barbaro, M.P.F. Analysis of the fungal microbiome in exhaled breath condensate of patients with asthma. Allergy Asthma Proc. 2016, 37, 41–46. [Google Scholar] [CrossRef] [Green Version]
- Guo, Z.D.; Wang, Z.Y.; Zhang, S.F.; Li, X.; Li, L.; Li, C.; Cui, Y.; Fu, R.-B.; Dong, Y.-Z.; Chi, X.-Y.; et al. Aerosol and Surface Distribution of Severe Acute Respiratory Syndrome Coronavirus 2 in Hospital Wards, Wuhan, China, 2020. Emerg. Infect. Dis. 2020, 26, 1583–1591. [Google Scholar] [CrossRef]
- Jung, M.; Chung, W.J.; Sung, M.; Jo, S.; Hong, J. Analysis of Infection Transmission Routes through Exhaled Breath and Cough Particle Dispersion in a General Hospital. Int. J. Environ. Res. Public Health 2022, 19, 2512. [Google Scholar] [CrossRef]
- Phoon, H.; Hussin, H.; Hussain, B.M.; Lim, S.Y.; Woon, J.J.; Er, Y.X.; Thong, K.L. Distribution, genetic diversity and antimicrobial resistance of clinically important bacteria from the environment of a tertiary hospital in Malaysia. J. Glob. Antimicrob. Resist. 2018, 14, 132–140. [Google Scholar] [CrossRef]
- Protano, C.; Cammalleri, V.; Romano, S.V.; Valeriani, F.; Vitali, M. Hospital environment as a reservoir for cross transmission: Cleaning and disinfection procedures. Ann. Ig. 2019, 31, 436–448. [Google Scholar]
- Correia, G.; Rodrigues, L.; Gameiro, D.S.M.; Gonçalves, T. Airborne route and bad use of ventilation systems as non-negligible factors in SARS-CoV-2 transmission. Med. Hypotheses 2020, 141, 109781. [Google Scholar] [CrossRef] [PubMed]
- Fennelly, M.; O’Connor, D.J.; Hellebust, S.; Murphy, N.; Casey, C.; Eustace, J.; Plant, B.J.; Sodeau, J.; Prentice, M.B. Effectiveness of a plasma treatment device on microbial air quality in a hospital ward, monitored by culture. J. Hosp. Infect. 2021, 108, 109–112. [Google Scholar] [CrossRef] [PubMed]
- Verhougstraete, M.; Reynolds, K. Use of a portable air disinfecting system to remove seeded coliphage in hospital rooms. Am. J. Infect. Control 2016, 44, 714–715. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Index | Actual Level |
|---|---|
| Room volume | 41.62 m3/P |
| Net story height | 2.61 m |
| Coefficient of room depth | 2.21 |
| Daylight factor | ≥1.0% |
| Total viable count | <500 cfu/m3 |
| Fresh air volume | 30–60 m3/(h·P) |
| PM10 | <0.05 mg/m3 |
| Temperature | 18–28 °C |
| Humidity | 50–80% |
| Pollutant | Diameter (μm) | CON | HEPA | PNOI | HEPA + PNOI |
|---|---|---|---|---|---|
| PM | 0.3–0.5 | 6.20 (1.41) | 88.63 (2.71) | 41.68 (2.55) | 97.98 (0.22) |
| 0.5–1.0 | 21.67 (2.18) | 94.40 (1.33) | 64.88 (1.87) | 98.57 (0.74) | |
| 1.0–3.0 | 53.45 (1.97) | 97.52 (0.52) | 84.50 (0.63) | 96.86 (0.52) | |
| 3.0–5.0 | 7.08 (6.11) | 82.74 (3.63) | 65.31 (2.76) | 88.46 (3.16) | |
| 5.0–10.0 | 14.46 (9.76) | 75.75 (4.91) | 67.75 (2.86) | 93.76 (2.62) | |
| >10.0 | 32.80 (7.07) | 67.73 (4.22) | 81.15 (2.75) | 98.16 (2.93) | |
| Bacterial aerosol | 0.65–1.1 | 46.59 (8.76) | 99.52 (0.45) | 97.79 (0.70) | 99.85 (0.19) |
| 1.1–2.1 | 20.97 (5.65) | 99.54 (0.31) | 96.92 (0.80) | 99.85 (0.15) | |
| 2.1–3.3 | 42.69 (3.42) | 99.64 (0.26) | 99.50 (0.28) | 99.91 (0.11) | |
| 3.3–4.7 | 72.17 (9.94) | 99.52 (0.33) | 99.88 (0.16) | 99.93 (0.11) | |
| 4.7–7.0 | 85.81 (4.05) | 99.33 (0.61) | 99.64 (0.42) | 99.47 (0.50) | |
| >7.0 | 75.30 (6.83) | 99.21 (0.75) | 99.50 (0.79) | 98.59 (0.28) |
| Pollutant | Position | CON | HEPA | PNOI | HEPA + PNOI |
|---|---|---|---|---|---|
| PM | A | 30.10 (7.30) | 86.78 (8.18) | 74.32 (6.03) | 91.45 (7.84) |
| B | 32.06 (8.33) | 84.82 (6.82) | 74.91 (6.09) | 95.73 (2.92) | |
| C | 29.26 (5.24) | 91.24 (6.85) | 73.48 (6.06) | 93.13 (5.99) | |
| D | 25.44 (5.07) | 79.13 (7.51) | 76.37 (6.28) | 88.83 (9.38) | |
| E | 26.19 (6.24) | 88.86 (9.09) | 69.12 (6.12) | 95.62 (5.43) | |
| F | 30.32 (6.23) | 83.42 (5.35) | 67.42 (6.40) | 92.04 (6.97) | |
| G | 19.07 (8.59) | 87.51 (6.27) | 72.23 (6.59) | 95.35 (5.04) | |
| Bacterial aerosol | A | 58.04 (4.58) | 99.20 (0.50) | 98.55 (0.75) | 99.92 (0.12) |
| B | 48.98 (5.10) | 99.47 (0.44) | 98.45 (0.4) | 99.62 (0.48) | |
| C | 60.42 (7.68) | 99.30 (0.62) | 99.19 (0.71) | 99.62 (0.64) | |
| D | 58.27 (9.15) | 99.58 (0.35) | 99.21 (0.63) | 99.86 (0.32) | |
| E | 63.50 (5.90) | 99.49 (0.33) | 98.82 (0.75) | 99.75 (0.32) | |
| F | 50.39 (5.08) | 99.86 (0.16) | 99.12 (0.70) | 100.00 (0) | |
| G | 61.13 (5.50) | 99.12 (0.59) | 98.73 (0.73) | 98.43 (0.29) |
| Purifier | Active | Inactive | Total | Activity Ratio (%) |
|---|---|---|---|---|
| CON | 67 | 0 | 67 | 100.00 |
| HEPA | 48 | 0 | 48 | 100.00 |
| PNOI | 23 | 17 | 40 | 57.50 |
| HEPA + PNOI | 12 | 20 | 32 | 37.50 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, B.; Liu, T.; Yi, S.; Huang, Y.; Guo, Y.; Huang, S.; Zhou, C.; Zhou, R.; Cao, H. Reducing the Effectiveness of Ward Particulate Matter, Bacteria and Influenza Virus by Combining Two Complementary Air Purifiers. Int. J. Environ. Res. Public Health 2022, 19, 10446. https://doi.org/10.3390/ijerph191610446
Zhou B, Liu T, Yi S, Huang Y, Guo Y, Huang S, Zhou C, Zhou R, Cao H. Reducing the Effectiveness of Ward Particulate Matter, Bacteria and Influenza Virus by Combining Two Complementary Air Purifiers. International Journal of Environmental Research and Public Health. 2022; 19(16):10446. https://doi.org/10.3390/ijerph191610446
Chicago/Turabian StyleZhou, Bingliang, Tiantian Liu, Siqi Yi, Yuanyuan Huang, Yubing Guo, Si Huang, Chengxing Zhou, Rong Zhou, and Hong Cao. 2022. "Reducing the Effectiveness of Ward Particulate Matter, Bacteria and Influenza Virus by Combining Two Complementary Air Purifiers" International Journal of Environmental Research and Public Health 19, no. 16: 10446. https://doi.org/10.3390/ijerph191610446