
Quality of Life and Mental Health Benefits of Public Participation in Forest Conservation Activities in Urban Areas



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
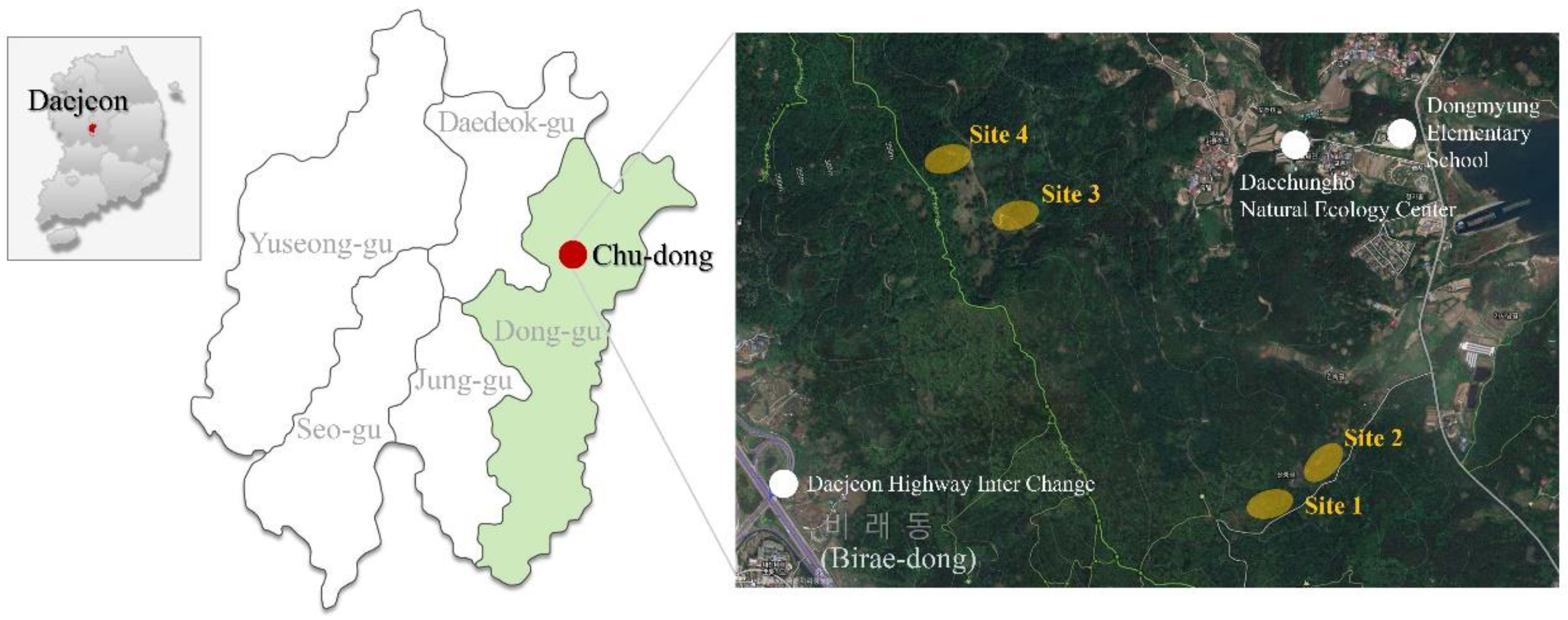
2.2. Research Sites
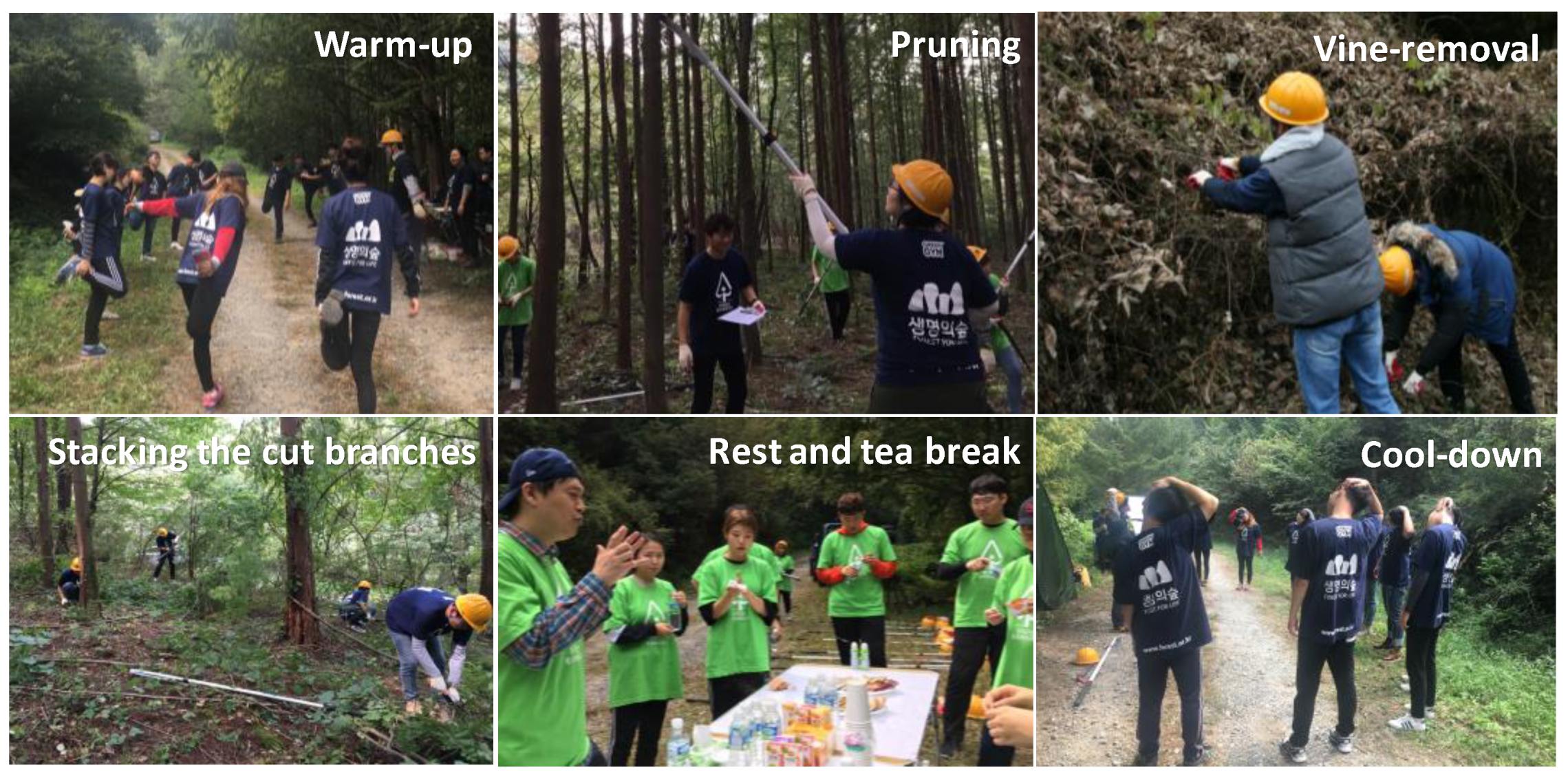
2.3. Forest Conservation Activity Program
2.3.1. Warm-Up Exercise
2.3.2. Expert Demonstration and Safety Training
2.3.3. First FCA Session
2.3.4. Break Time
2.3.5. Second FCA Session
2.3.6. Cool-Down and Finish
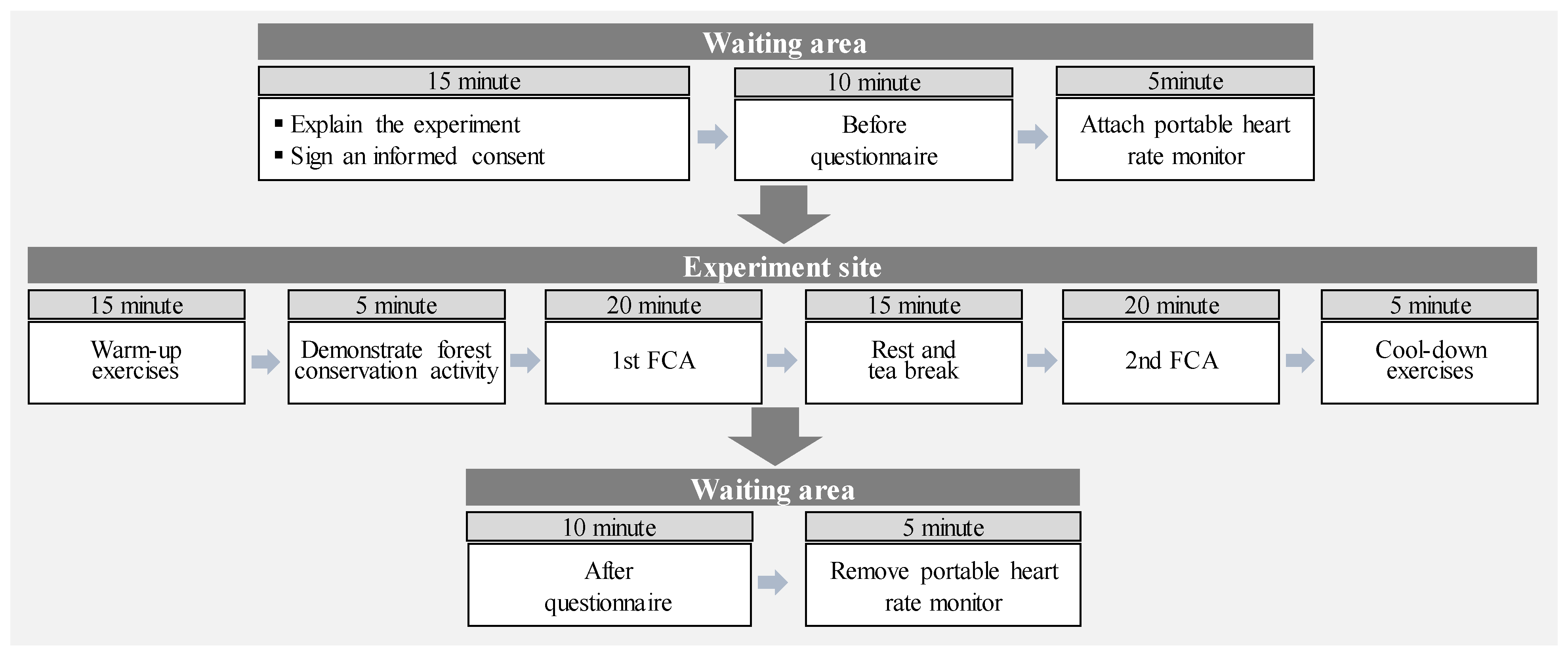
2.4. Procedures
2.5. Physical Activity Measurement Indicators
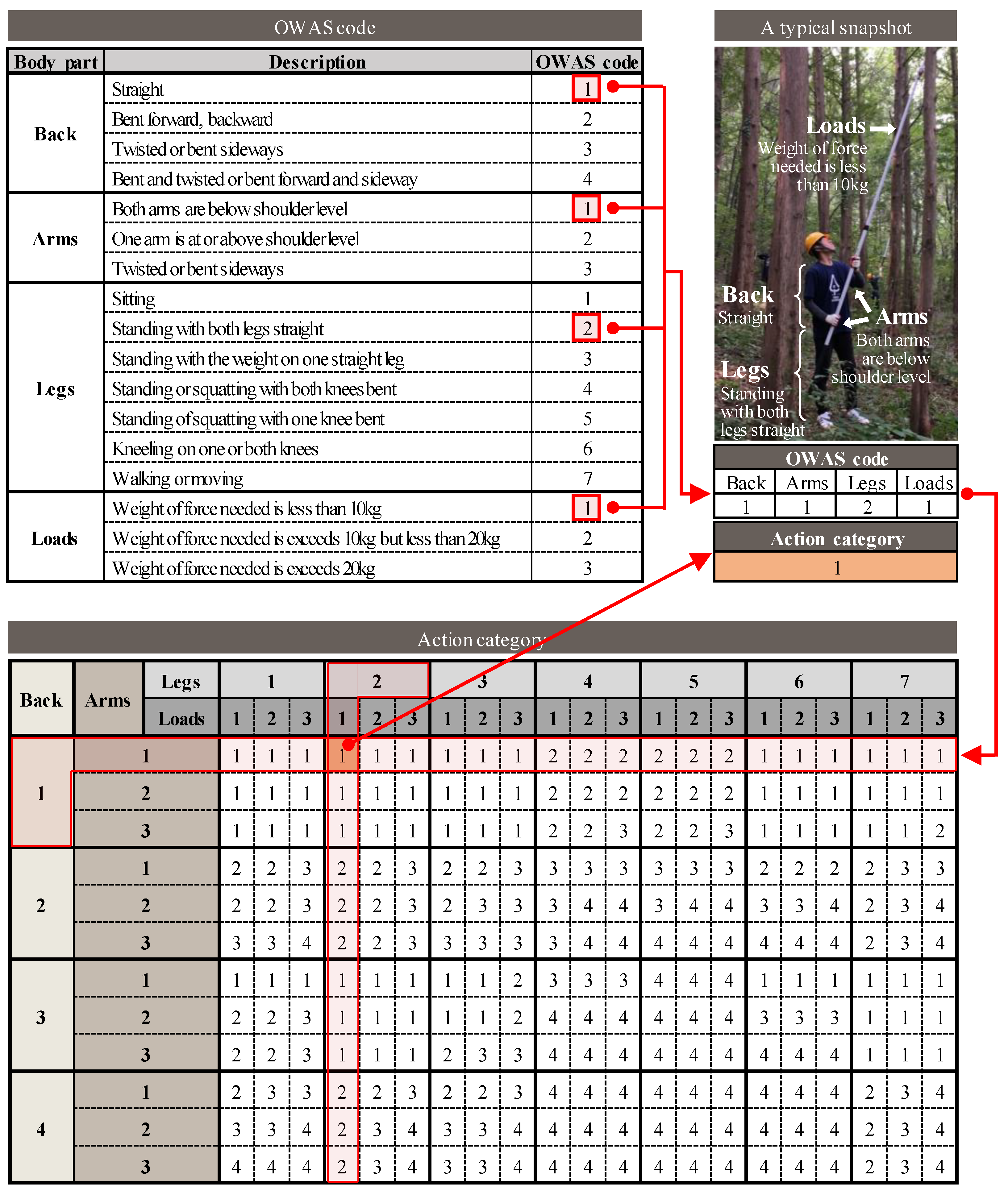
2.5.1. Musculoskeletal System Load
2.5.2. Physical Activity Intensity
2.6. Mental Health Measurement Indicators
2.6.1. Quality of Life
2.6.2. Rosenberg Self-Esteem Scale (RES)
2.6.3. Positive and Negative Affect Schedule (PANAS)
2.6.4. Perceived Restorativeness Scale (PRS)
2.7. Statistical Analysis
3. Results
3.1. Musculoskeletal System Load
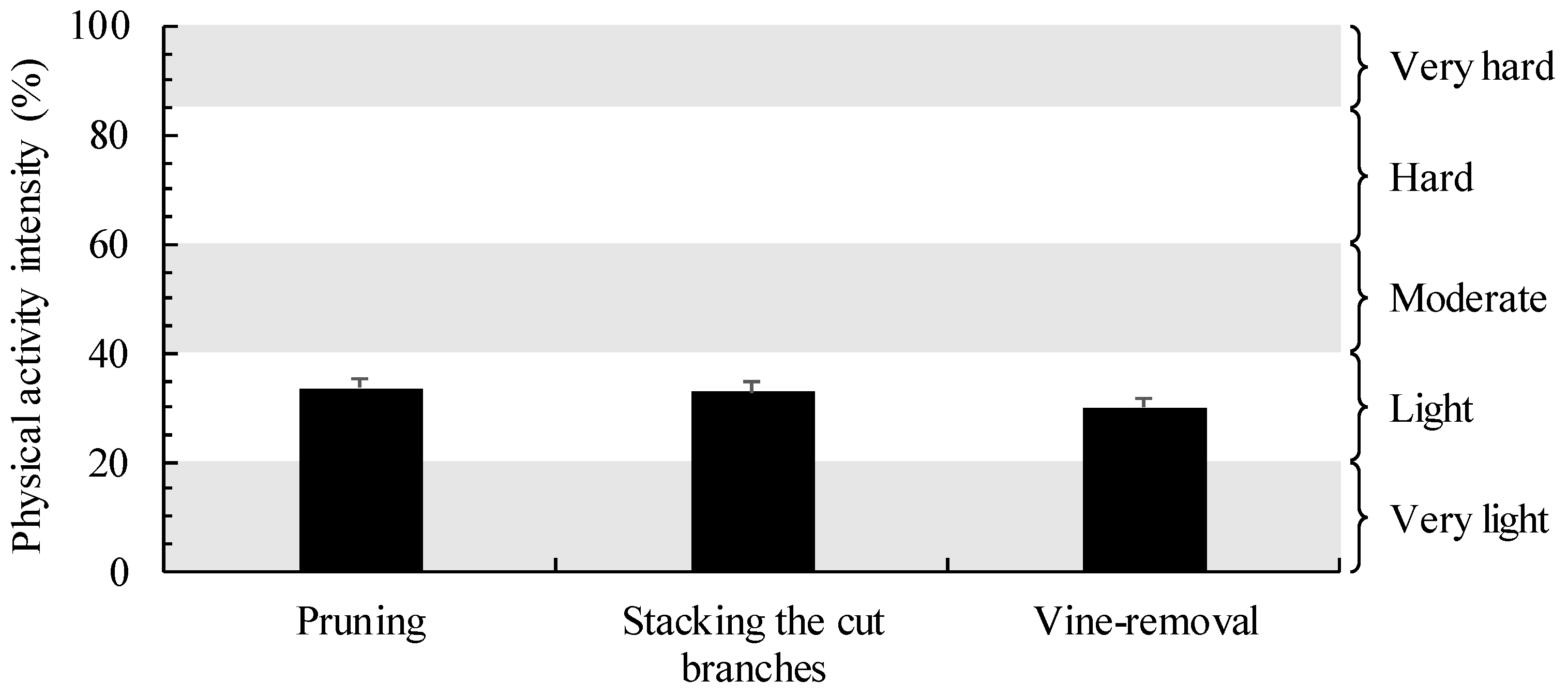
3.2. Physical Activity Intensity (PAI)
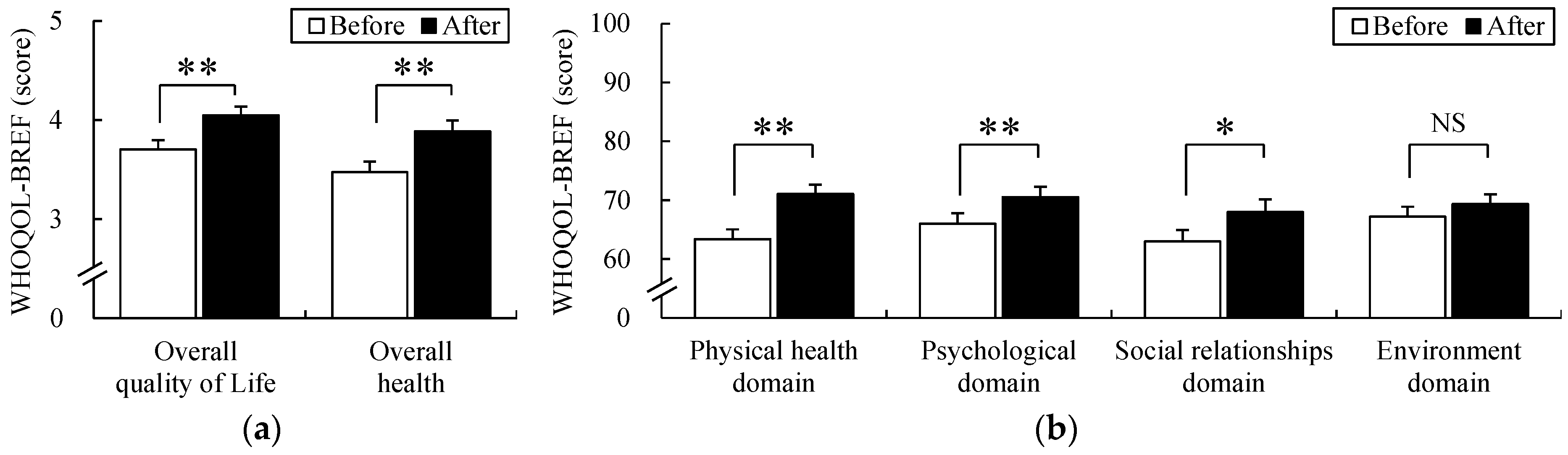
3.3. Quality of Life
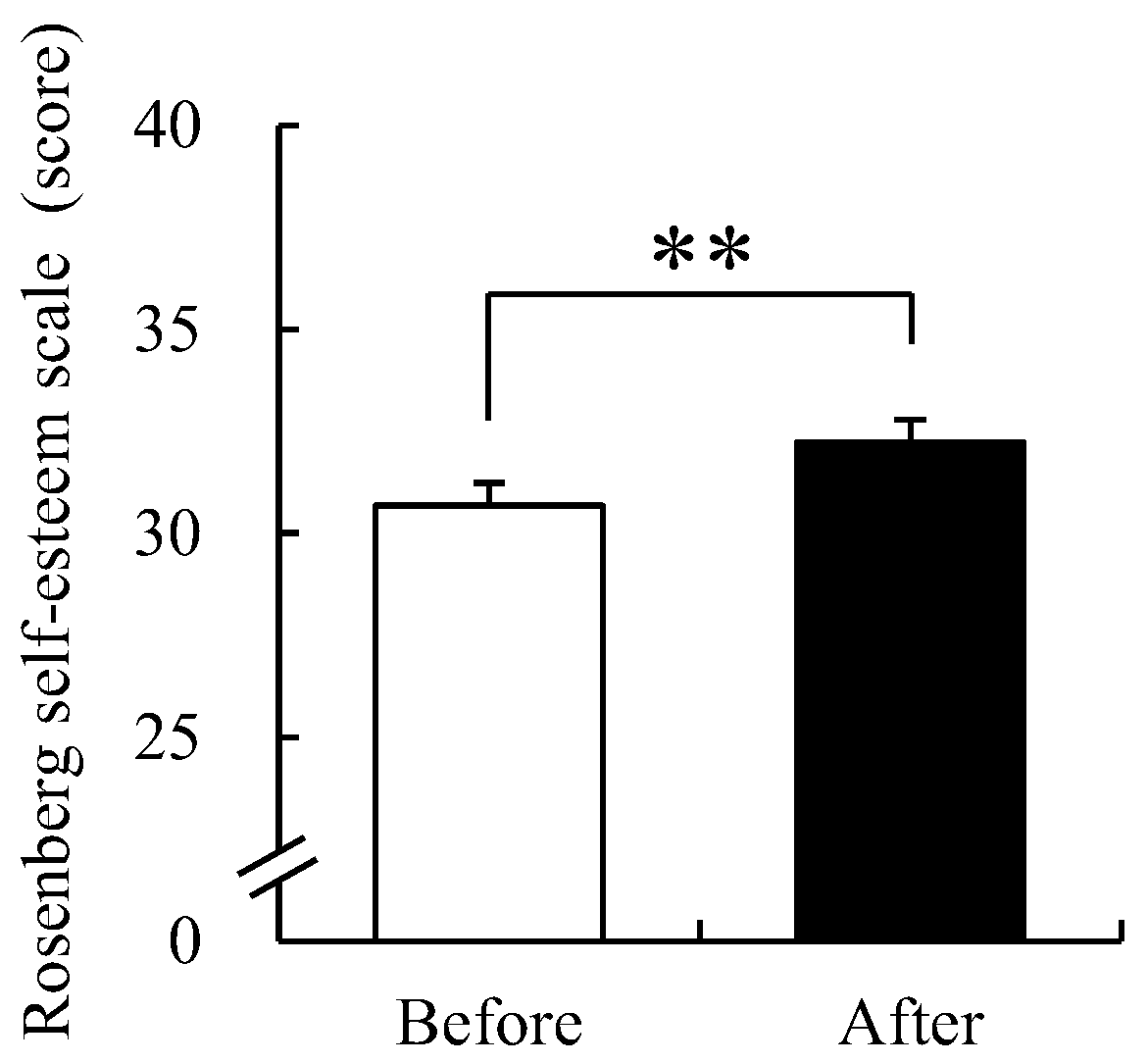
3.4. Rosenberg Self-Esteem Scale
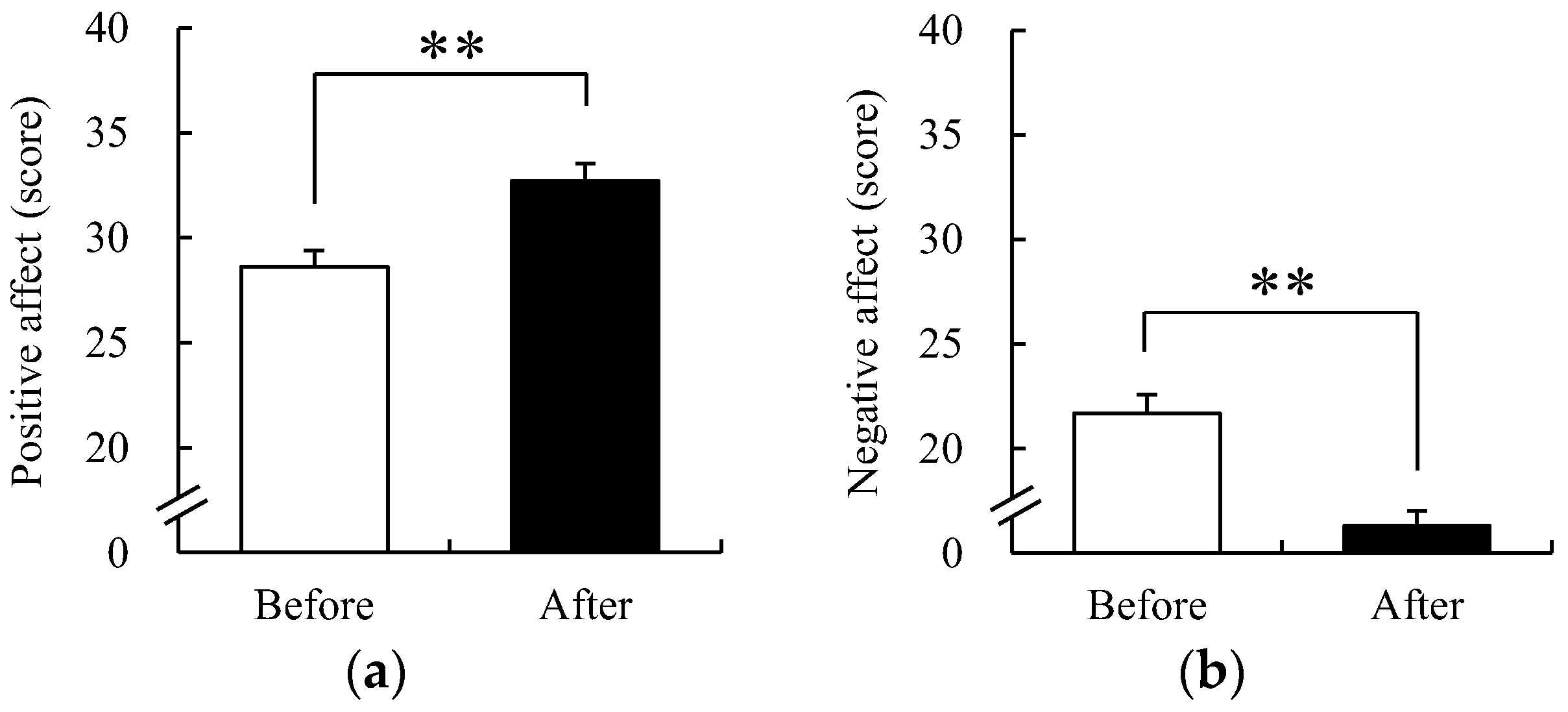
3.5. Positive and Negative Affect Schedule
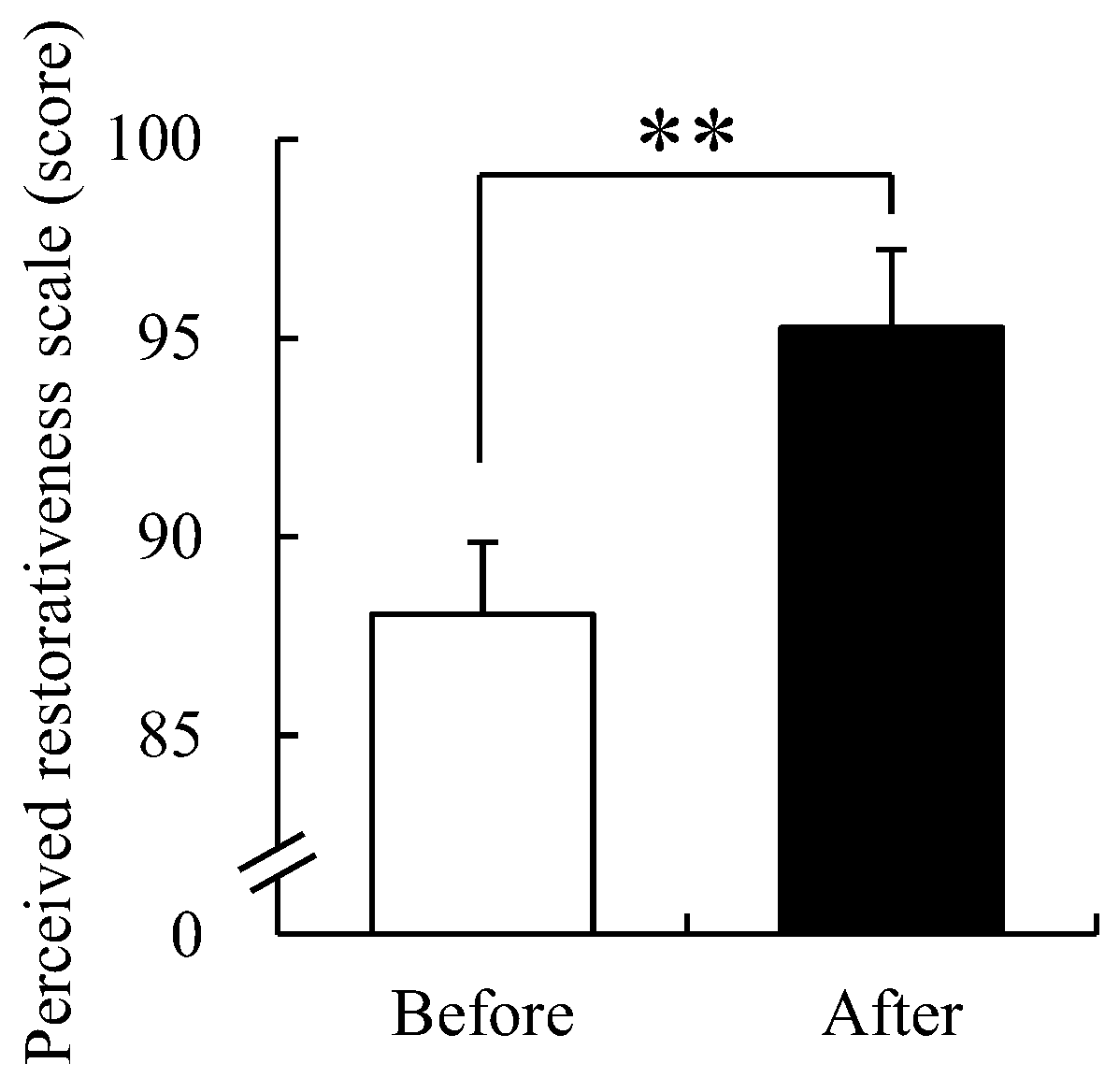
3.6. Perceived Restorativeness Scale
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tombari, B. Rapid Urbanisation: Theories, Causes, Consequences and Coping Strategies. Ann. Geogr. Stud. 2019, 2, 32–45. [Google Scholar]
- United Nations. 2018 Revision of World Urbanization Prospects; UN: New York, NY, USA, 2018. [Google Scholar]
- Keleş, S.; Sivrikaya, F.; Çakir, G.; Köse, S. Urbanization and forest cover change in regional directorate of Trabzon forestry from 1975 to 2000 using landsat data. Environ. Monit. Assess. 2008, 140, 1–14. [Google Scholar] [CrossRef]
- Byomkesh, T.; Nakagoshi, N.; Dewan, A.M. Urbanization and green space dynamics in Greater Dhaka, Bangladesh. Landsc. Ecol. Eng. 2012, 8, 45–58. [Google Scholar] [CrossRef]
- Li, G.; Fang, C.; Wang, S.; Sun, S. The Effect of Economic Growth, Urbanization, and Industrialization on Fine Particulate Matter (PM2.5) Concentrations in China. Environ. Sci. Technol. 2016, 50, 11452–11459. [Google Scholar] [CrossRef] [PubMed]
- Xiong, Y.; Huang, S.; Chen, F.; Ye, H.; Wang, C.; Zhu, C. The Impacts of Rapid Urbanization on the Thermal Environment: A Remote Sensing Study of Guangzhou, South China. Remote Sens. 2012, 4, 2033–2056. [Google Scholar] [CrossRef] [Green Version]
- Brunekreef, B.; Holgate, S.T. Air pollution and health. Lancet 2002, 360, 1233–1242. [Google Scholar] [CrossRef]
- Kampa, M.; Castanas, E. Human health effects of air pollution. Environ. Pollut. 2008, 151, 362–367. [Google Scholar] [CrossRef]
- Dominski, F.H.; Lorenzetti Branco, J.H.; Buonanno, G.; Stabile, L.; da Silva, M.G.; Andrade, A. Effects of air pollution on health: A mapping review of systematic reviews and meta-analyses. Environ. Res. 2021, 201, 111487. [Google Scholar] [CrossRef]
- Nowak, D.J.; Hirabayashi, S.; Bodine, A.; Greenfield, E. Tree and forest effects on air quality and human health in the United States. Environ. Pollut. 2014, 193, 119–129. [Google Scholar] [CrossRef] [Green Version]
- Nowak, D.J.; Hirabayashi, S.; Doyle, M.; McGovern, M.; Pasher, J. Air pollution removal by urban forests in Canada and its effect on air quality and human health. Urban For. Urban Green. 2018, 29, 40–48. [Google Scholar] [CrossRef]
- Aram, F.; Higueras García, E.; Solgi, E.; Mansournia, S. Urban green space cooling effect in cities. Heliyon 2019, 5, e01339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gladwell, V.F.; Brown, D.K.; Wood, C.; Sandercock, G.R.; Barton, J.L. The great outdoors: How a green exercise environment can benefit all. Extrem. Physiol. Med. 2013, 2, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mytton, O.T.; Townsend, N.; Rutter, H.; Foster, C. Green space and physical activity: An observational study using Health Survey for England data. Health Place 2012, 18, 1034–1041. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Dai, X.; Wu, J.; Wu, X.; Nie, X. Influence of urban green open space on residents’ physical activity in China. BMC Public Health 2019, 19, 1093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, C.; Joung, D.; Ikei, H.; Igarashi, M.; Aga, M.; Park, B.-J.; Miwa, M.; Takagaki, M.; Miyazaki, Y. Physiological and psychological effects of walking on young males in urban parks in winter. J. Physiol. Anthropol. 2013, 32, 18. [Google Scholar] [CrossRef] [Green Version]
- Joung, D.; Kim, G.; Choi, Y.; Lim, H.; Park, S.; Woo, J.-M.; Park, B.-J. The prefrontal cortex activity and psychological effects of viewing forest landscapes in autumn season. Int. J. Environ. Res. Public Health 2015, 12, 7235–7243. [Google Scholar] [CrossRef] [Green Version]
- Joung, D.; Lee, B.; Lee, J.; Lee, C.; Koo, S.; Park, C.; Kim, S.; Kagawa, T.; Park, B.-J. Measures to Promote Rural Healthcare Tourism with a Scientific Evidence-Based Approach. Int. J. Environ. Res. Public Health 2020, 17, 3266. [Google Scholar] [CrossRef]
- Krasny, M.E.; Tidball, K.G. Civic ecology: A pathway for Earth Stewardship in cities. Front. Ecol. Environ. 2012, 10, 267–273. [Google Scholar] [CrossRef]
- Tidball, K.G.; Krasny, M.E. Urban environmental education from a social-ecological perspective: Conceptual framework for civic ecology education. Cities Environ. 2010, 3, 11. [Google Scholar] [CrossRef]
- Sakurai, R.; Kobori, H.; Nakamura, M.; Kikuchi, T. Factors influencing public participation in conservation activities in urban areas: A case study in Yokohama, Japan. Biol. Conserv. 2015, 184, 424–430. [Google Scholar] [CrossRef]
- Birch, M. Cultivating wildness: Three conservation volunteers’ experiences of participation in the Green Gym scheme. Br. J. Occup. Ther. 2005, 68, 244–252. [Google Scholar] [CrossRef]
- Reynolds, V. The green gym. Volunt. Action 2000, 2, 15–26. [Google Scholar]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Pate, R.R.; Pratt, M.; Blair, S.N.; Haskell, W.L.; Macera, C.A.; Bouchard, C.; Buchner, D.; Ettinger, W.; Heath, G.W.; King, A.C.; et al. Physical Activity and Public Health: A Recommendation From the Centers for Disease Control and Prevention and the American College of Sports Medicine. J. Am. Med. Assoc. 1995, 273, 402–407. [Google Scholar] [CrossRef]
- Karhu, O.; Kansi, P.; Kuorinka, I. Correcting working postures in industry: A practical method for analysis. Appl. Ergon. 1977, 8, 199–201. [Google Scholar] [CrossRef]
- Howley, E.T. Type of activity: Resistance, aerobic and leisure versus occupational physical activity. Med. Sci. Sports Exerc. 2001, 33, S364–S369; discussion S419–S420. [Google Scholar] [CrossRef]
- Fox, S.M., III; Naughton, J.P.; Haskell, W.L. Physical activity and the prevention of coronary heart disease. Ann. Clin. Res. 1971, 3, 404–432. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Programme on Mental Health: WHOQOL User Manual, 2012 Revis; World Health Organization: Geneva, Switzerland, 1998. [Google Scholar]
- Rosenberg, M. Society and the adolescent self-image. In Society and the Adolescent Self-Image; Princeton University Press: Princeton, NJ, USA, 2015. [Google Scholar]
- Lee, J.-Y.; Nam, S.-K.; Lee, M.-K.; Lee, J.-H.; Lee, S. Rosenberg’self-esteem scale: Analysis of item-level validity. Korean J. Couns. Psychother. 2009, 21, 173–189. [Google Scholar]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Pers. Soc. Psychol. 1988, 54, 1063. [Google Scholar] [CrossRef]
- Park, H.S.; Lee, J.M. A Validation Study of Korean Version of PANAS-Revised. Korean J. Psychol. Gen. 2016, 35, 617–641. [Google Scholar] [CrossRef]
- Hartig, T.; Korpela, K.; Evans, G.W.; Gärling, T. A measure of restorative quality in environments. Scand. Hous. Plan. Res. 1997, 14, 175–194. [Google Scholar] [CrossRef]
- Lee, S.-H.; Hyun, M.-H. The factor structure of the Korean version of the Perceived Restorativeness Scale(PRS). Korean J. Health Psychol. 2003, 8, 229–241. [Google Scholar]
- Gallis, C. Work-related prevalence of musculoskeletal symptoms among Greek forest workers. Int. J. Ind. Ergon. 2006, 36, 731–736. [Google Scholar] [CrossRef]
- Dimou, V.; Malesios, C.; Pispa, S. Monitoring self-reported musculoskeletal symptoms in forestry operations. Int. J. For. Eng. 2020, 31, 106–113. [Google Scholar] [CrossRef]
- Kurumatani, N.; Yamaguchi, B.; Dejima, M.; Enomoto, Y.; Moriyama, T. Aerobic capacity of forestry workers and physical demands of forestry operations. Eur. J. Appl. Physiol. Occup. Physiol. 1992, 64, 546–551. [Google Scholar] [CrossRef]
- Abell, J.E.; Hootman, J.M.; Zack, M.M.; Moriarty, D.; Helmick, C.G. Physical activity and health related quality of life among people with arthritis. J. Epidemiol. Community Health 2005, 59, 380. [Google Scholar] [CrossRef] [Green Version]
- Bratman, G.N.; Daily, G.C.; Levy, B.J.; Gross, J.J. The benefits of nature experience: Improved affect and cognition. Landsc. Urban Plan. 2015, 138, 41–50. [Google Scholar] [CrossRef]
- Pretty, J.; Peacock, J.; Sellens, M.; Griffin, M. The mental and physical health outcomes of green exercise. Int. J. Environ. Health Res. 2005, 15, 319–337. [Google Scholar] [CrossRef]
- Kaplan, R.; Kaplan, S. The Experience of Nature: A Psychological Perspective; Cambridge University Press: Cambridge, UK, 1989. [Google Scholar]
- Lilley, R.; Feyer, A.-M.; Kirk, P.; Gander, P. A survey of forest workers in New Zealand: Do hours of work, rest, and recovery play a role in accidents and injury? J. Saf. Res. 2002, 33, 53–71. [Google Scholar] [CrossRef]
- Wilson, E.O. Biophilia; Harvard Universiy Press: Cambridge, MA, USA, 1984. [Google Scholar]
- Ulrich, R.S. Visual landscapes and psychological well-being. Landsc. Res. 1979, 4, 17–23. [Google Scholar] [CrossRef]
- Yerrell, P. National Evaluation of BTCV’s Green Gym; School of Health and Social Care, Oxford Brookes University: Oxford, UK, 2008. [Google Scholar]
- Smyth, N.; Thorn, L.; Wood, C.; Hall, D.; Lister, C. Increased Wellbeing following Engagement in a Group Nature-Based Programme: The Green Gym Programme Delivered by the Conservation Volunteers. Healthcare 2022, 10, 978. [Google Scholar] [CrossRef] [PubMed]
- Uehara, I.; Itoh, S. Importance of multiple outdoor Activities for persons with developmental disabilities. J. Ther. Hortic. 1999, 10, 22–27. [Google Scholar]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Site 1 | Site 2 | Site 3 | Site 4 | |
|---|---|---|---|---|
| Forest type | Conifers | Conifers | Non-stocked forest land 1 | Non-stocked forest land |
| Tree species | Metasequoia glyptostroboides | Picea abies (L.) H. Karst. | - | - |
| Type of FCA 2 | Pruning Stacking the cut branches | Pruning Stacking the cut branches | Vine-removal | Vine-removal |
| Slope (°) | 10 | 10 | 15 | 15 |
| Height (m) | 15 | 20 | ||
| DBH (cm) | 16 | 14 |
| OWAS Categories | Action Category Description |
|---|---|
| Action Category 1 |
|
| Action Category 2 |
|
| Action Category 3 |
|
| Action Category 4 |
|
| %HRR | ||||||
|---|---|---|---|---|---|---|
| <20 | 20–39 | 40–59 | 60–84 | ≥85 | 100 | |
| PAI | Very light | Light | Moderate | Hard | Very hard | Maximal |
| FCA | Action Categories (%) | Average Action Category | ||||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | Total | ||
| Pruning | 58.75 | 26.25 | 2.50 | 12.50 | 100.00 | 1.69 ± 0.11 |
| Stacking the cut branches | 45.00 | 27.50 | 25.00 | 2.50 | 100.00 | 1.85 ± 0.14 |
| Vine-removal | 35.00 | 20.00 | 33.75 | 11.25 | 100.00 | 2.21 ± 0.12 |
| FCA | HRmax | HRr | HRw | PAI |
|---|---|---|---|---|
| Pruning | 197.8 ± 0.2 | 78.9 ± 1.5 | 119.4 ± 1.6 | 33.6 ± 1.6 |
| Stacking the cut branches | 197.7 ± 0.2 | 78.8 ± 1.7 | 118.6 ± 1.9 | 32.8 ± 1.8 |
| Vine-removal | 196.6 ± 0.3 | 81.9 ± 1.9 | 116.2 ± 2.6 | 29.9 ± 1.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Joung, D.; Park, B.-J.; Kang, S. Quality of Life and Mental Health Benefits of Public Participation in Forest Conservation Activities in Urban Areas. Int. J. Environ. Res. Public Health 2022, 19, 9768. https://doi.org/10.3390/ijerph19159768
Joung D, Park B-J, Kang S. Quality of Life and Mental Health Benefits of Public Participation in Forest Conservation Activities in Urban Areas. International Journal of Environmental Research and Public Health. 2022; 19(15):9768. https://doi.org/10.3390/ijerph19159768
Chicago/Turabian StyleJoung, Dawou, Bum-Jin Park, and Shinkwang Kang. 2022. "Quality of Life and Mental Health Benefits of Public Participation in Forest Conservation Activities in Urban Areas" International Journal of Environmental Research and Public Health 19, no. 15: 9768. https://doi.org/10.3390/ijerph19159768