
The Effects of Eccentric Contraction Execution Time on the Properties of the Patellar Tendon



Abstract
:1. Introduction
2. Materials and Methods
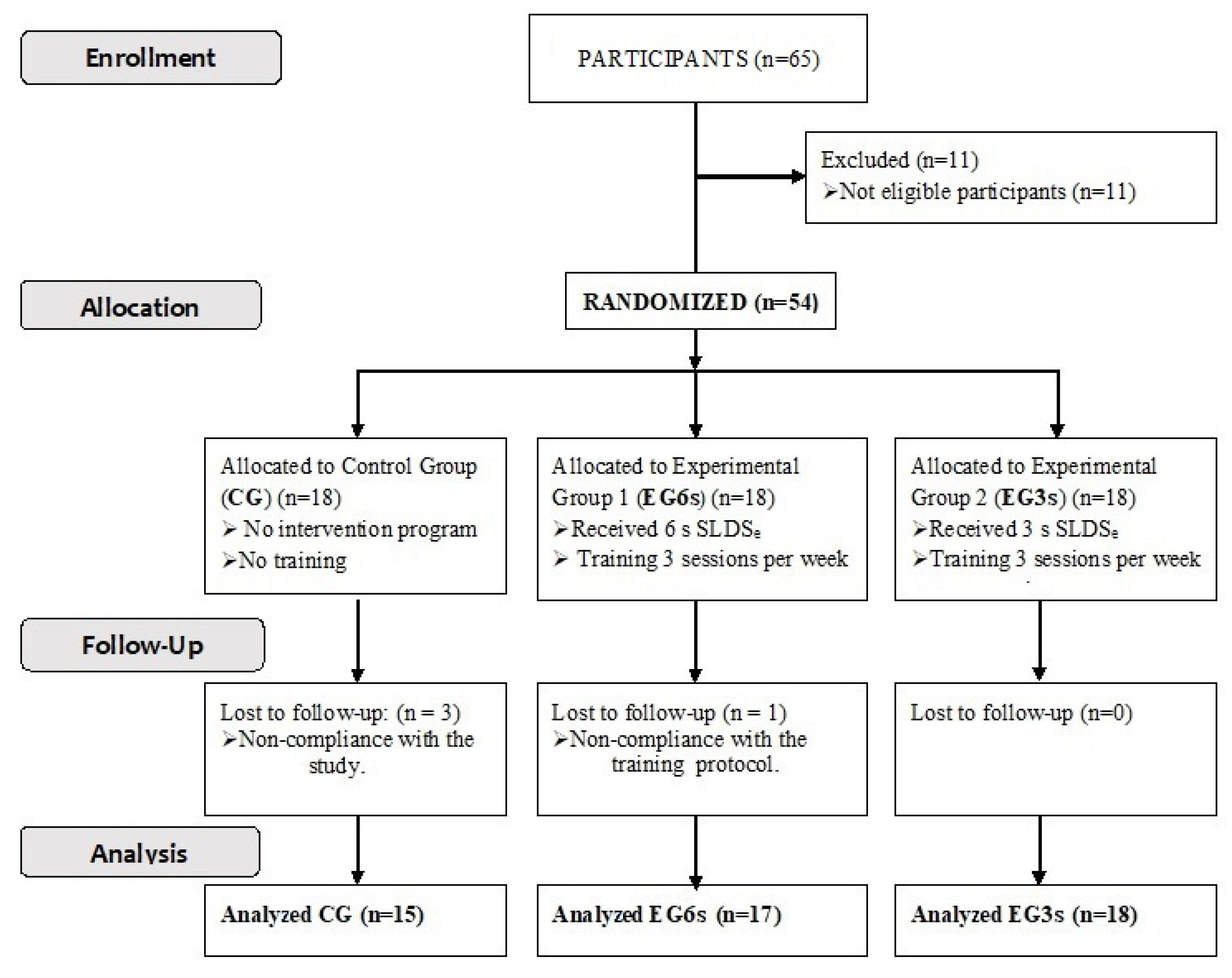
2.1. Participants and General Procedure
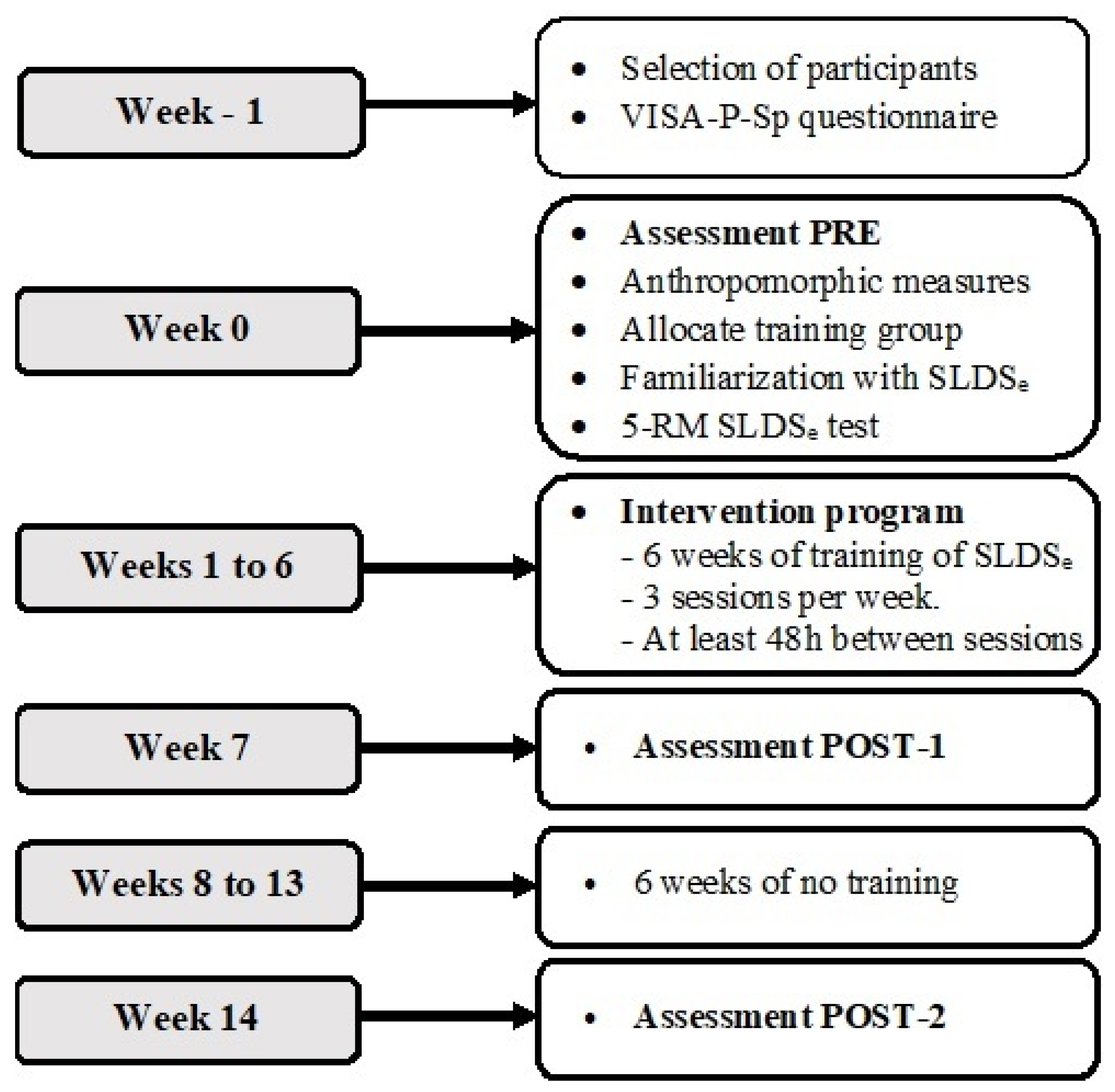
2.2. Experimental Design
2.3. Intervention Program
2.4. 5-RM SLDSe Test
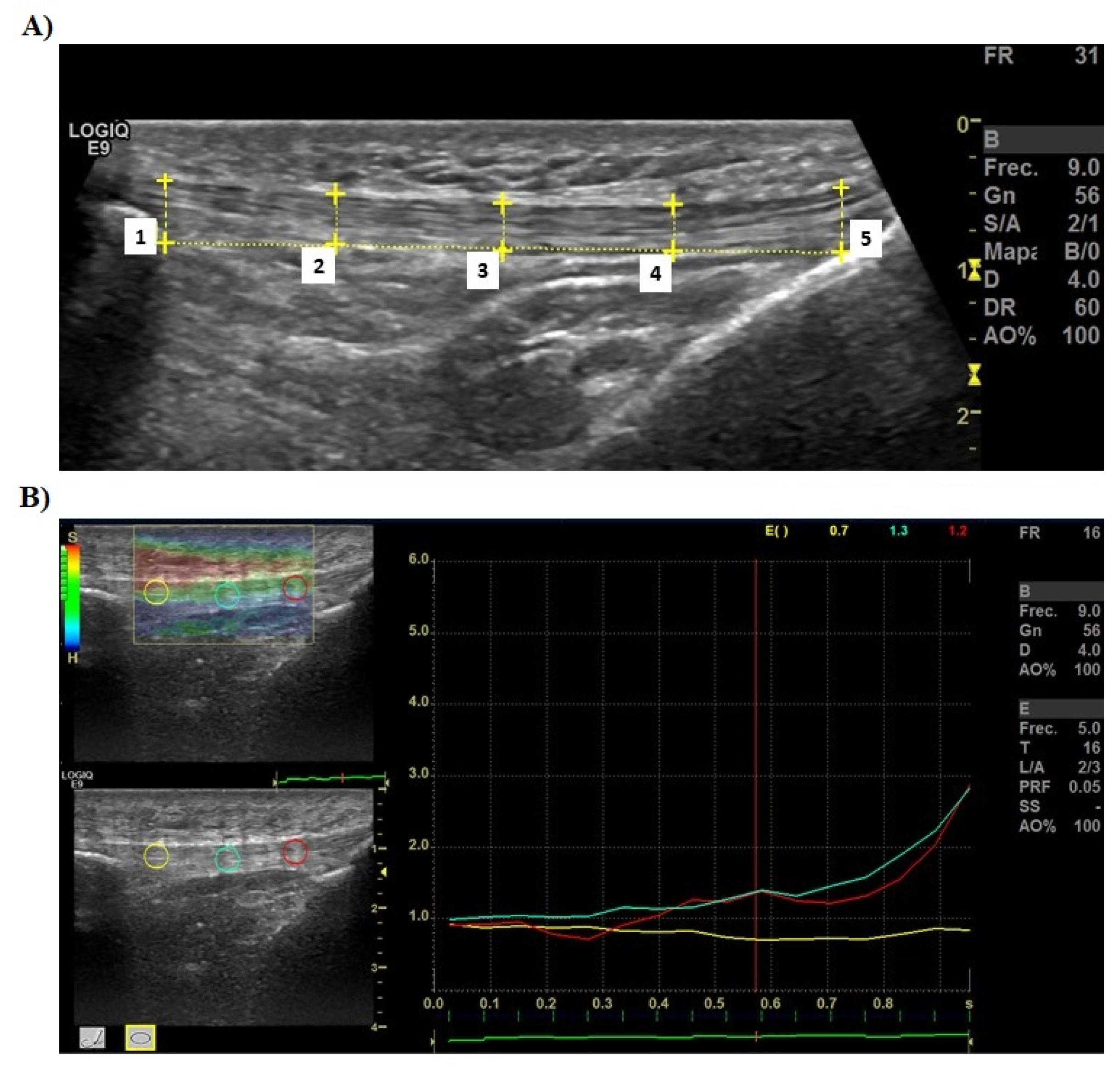
2.5. Thickness of PT Assessment
2.6. Elastic Properties of PT Assessment
2.7. Statistical Analysis
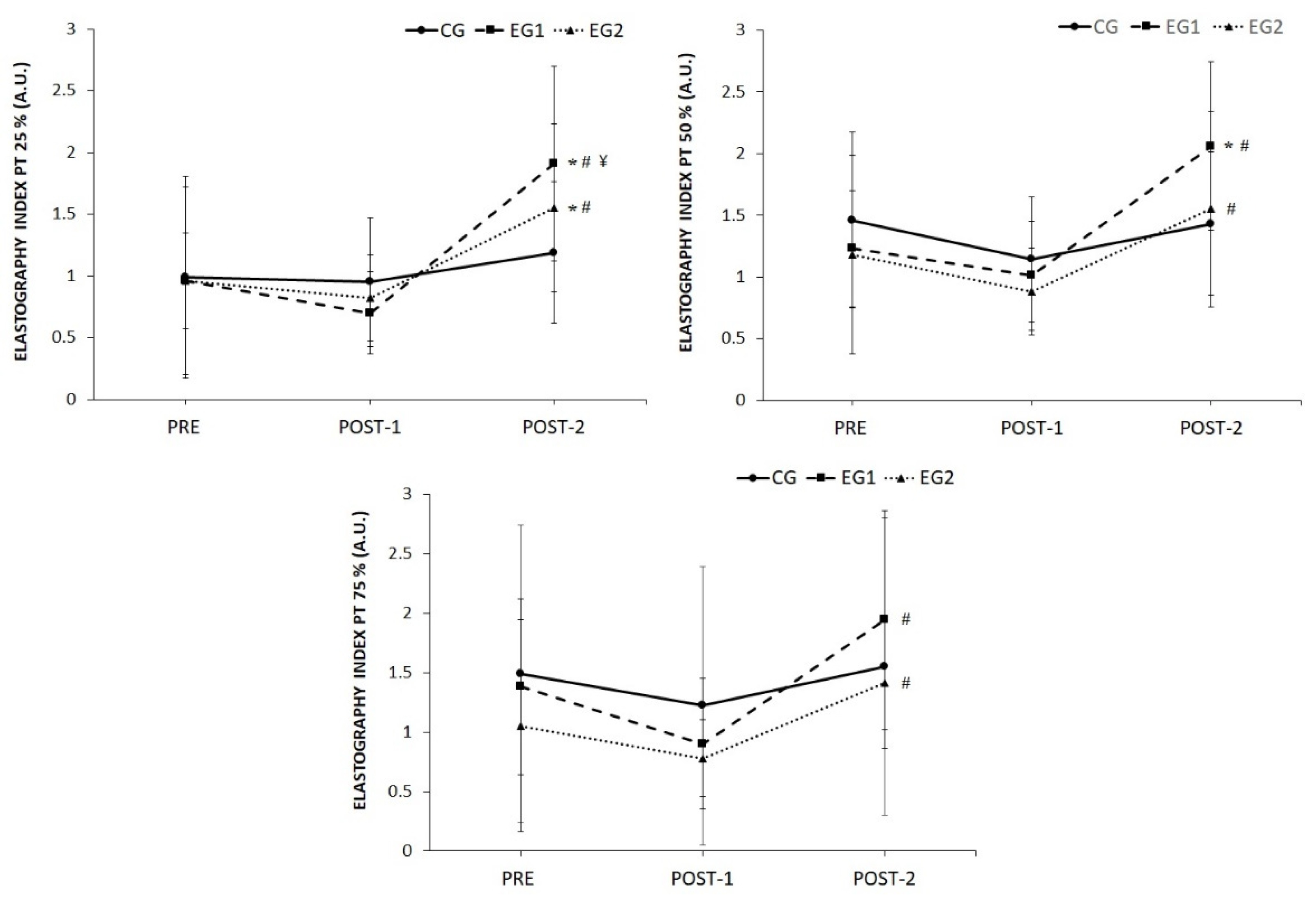
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Andrikoula, S.; Tokis, A.; Vasiliadis, H.S.; Georgoulis, A. The extensor mechanism of the knee joint: An anatomical study. Knee Surg. Sports Traumatol. Arthrosc. 2006, 14, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Glenn, L.L.; Samojla, B.G. A critical reexamination of the morphology, neurovasculature, and fiber architecture of knee extensor muscles in animal models and humans. Biol. Res. Nurs. 2002, 4, 128–141. [Google Scholar] [CrossRef] [PubMed]
- Defrate, L.E.; Nha, K.W.; Papannagari, R.; Moses, J.M.; Gill, T.J.; Li, G. The biomechanical function of the patellar tendon during in-vivo weight-bearing flexion. J. Biomech. 2007, 40, 1716–1722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kubo, K.; Tabata, T.; Ikebukuro, T.; Igarashi, K.; Yata, H.; Tsunoda, N. Effects of mechanical properties of muscle and tendon on performance in long distance runners. Eur. J. Appl. Physiol. 2010, 110, 507–514. [Google Scholar] [CrossRef] [PubMed]
- Hutchison, M.K.; Houck, J.; Cuddeford, T.; Dorociak, R.; Brumitt, J. Prevalence of Patellar Tendinopathy and Patellar Tendon Abnormality in Male Collegiate Basketball Players: A Cross-Sectional Study. J. Athl. Train. 2019, 54, 953–958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janssen, I.; van der Worp, H.; Hensing, S.; Zwerver, J. Investigating Achilles and patellar tendinopathy prevalence in elite athletics. Res. Sports Med. 2018, 26, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Basso, O.; Amis, A.A.; Race, A.; Johnson, D.P. Patellar tendon fiber strains: Their differential responses to quadriceps tension. Clin. Orthop. Relat. Res. 2002, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, A.; Watson, J.N.; Hutchinson, M.R. Patellar Tendinopathy. Sports Health 2015, 7, 415–420. [Google Scholar] [CrossRef] [Green Version]
- Young, M.A.; Cook, J.L.; Purdam, C.R.; Kiss, Z.S.; Alfredson, H. Eccentric decline squat protocol offers superior results at 12 months compared with traditional eccentric protocol for patellar tendinopathy in volleyball players. Br. J. Sports Med. 2005, 39, 102–105. [Google Scholar] [CrossRef] [Green Version]
- Kongsgaard, M.; Reitelseder, S.; Pedersen, T.G.; Holm, L.; Aagaard, P.; Kjaer, M.; Magnusson, S.P. Region specific patellar tendon hypertrophy in humans following resistance training. Acta Physiol. 2007, 191, 111–121. [Google Scholar] [CrossRef]
- Malliaras, P.; Kamal, B.; Nowell, A.; Farley, T.; Dhamu, H.; Simpson, V.; Morrissey, D.; Langberg, H.; Maffulli, N.; Reeves, N.D. Patellar tendon adaptation in relation to load-intensity and contraction type. J. Biomech. 2013, 46, 1893–1899. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.C.; Ng, G.Y.; Zhang, Z.J.; Malliaras, P.; Masci, L.; Fu, S.N. Changes on Tendon Stiffness and Clinical Outcomes in Athletes Are Associated with Patellar Tendinopathy After Eccentric Exercise. Clin. J. Sport Med. 2020, 30, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Kongsgaard, M.; Kovanen, V.; Aagaard, P.; Doessing, S.; Hansen, P.; Laursen, A.H.; Kaldau, N.C.; Kjaer, M.; Magnusson, S.P. Corticosteroid injections, eccentric decline squat training and heavy slow resistance training in patellar tendinopathy. Scand. J. Med. Sci. Sports 2009, 19, 790–802. [Google Scholar] [CrossRef] [PubMed]
- Bohm, S.; Mersmann, F.; Arampatzis, A. Human tendon adaptation in response to mechanical loading: A systematic review and meta-analysis of exercise intervention studies on healthy adults. Sports Med. Open. 2015, 1, 7. [Google Scholar] [CrossRef] [Green Version]
- Lacerda, L.T.; Martins-Costa, H.C.; Diniz, R.C.; Lima, F.V.; Andrade, A.G.; Tourino, F.D.; Bemben, M.G.; Chagas, M.H. Variations in Repetition Duration and Repetition Numbers Influence Muscular Activation and Blood Lactate Response in Protocols Equalized by Time Under Tension. J. Strength Cond. Res. 2016, 30, 251–258. [Google Scholar] [CrossRef] [Green Version]
- Abian, P.; Martinez, F.; Jimenez, F.; Abian-Vicen, J. Effects of Eccentric Single-Leg Decline Squat Exercise on the Morphological and Structural Properties of the Vastus Lateralis and Patellar Tendon. Int. J. Environ. Res. Public Health 2020, 17, 9410. [Google Scholar] [CrossRef]
- Burd, N.A.; Andrews, R.J.; West, D.W.; Little, J.P.; Cochran, A.J.; Hector, A.J.; Cashaback, J.G.; Gibala, M.J.; Potvin, J.R.; Baker, S.K.; et al. Muscle time under tension during resistance exercise stimulates differential muscle protein sub-fractional synthetic responses in men. J. Physiol. 2012, 590, 351–362. [Google Scholar] [CrossRef]
- Farthing, J.P.; Chilibeck, P.D. The effects of eccentric and concentric training at different velocities on muscle hypertrophy. Eur. J. Appl. Physiol. 2003, 89, 578–586. [Google Scholar] [CrossRef]
- Hernandez-Sanchez, S.; Hidalgo, M.D.; Gomez, A. Cross-cultural adaptation of VISA-P score for patellar tendinopathy in Spanish population. J. Orthop. Sports Phys. Ther. 2011, 41, 581–591. [Google Scholar] [CrossRef]
- Purdam, C.R.; Jonsson, P.; Alfredson, H.; Lorentzon, R.; Cook, J.L.; Khan, K.M. A pilot study of the eccentric decline squat in the management of painful chronic patellar tendinopathy. Br. J. Sports Med. 2004, 38, 395–397. [Google Scholar] [CrossRef] [Green Version]
- Brzycki, M. Strength Testing—Predicting a One-Rep Max from Reps-to-Fatigue. J. Phys. Educ. Recreat. Dance 1993, 64, 88–90. [Google Scholar] [CrossRef]
- Bravo-Sánchez, A.; Abián, P.; Jiménez, F.; Abián-Vicén, J. Myotendinous asymmetries derived from the prolonged practice of badminton in professional players. PLoS ONE 2019, 14, e0222190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skow, S.T.; Aalkjaer, J. Ultrasonographic measurement of patellar tendon thickness, a study of intra- and interobserver reliability. Clin. Imag. 2013, 37, 934–937. [Google Scholar] [CrossRef] [PubMed]
- Bravo-Sánchez, A.; Abián, P.; Sánchez-Infante, J.; Esteban-Gacía, P.; Jiménez, F.; Abián-Vicén, J. Objective Assessment of Regional Stiffness in Vastus Lateralis with Different Measurement Methods: A Reliability Study. Sensors 2021, 21, 3213. [Google Scholar] [CrossRef] [PubMed]
- Bravo-Sánchez, A.; Abián, P.; Jimenez, F.; Abián-Vicén, J. Structural and mechanical properties of the Achilles tendon in senior badminton players: Operated vs. non-injured tendons. Clin. Biomech. 2021, 85, 105366. [Google Scholar] [CrossRef] [PubMed]
- Bravo-Sánchez, A.; Abián, P.; Sousa, F.; Jimenez, F.; Abián-Vicén, J. Influence of Badminton Practice on Age-Related Changes in Patellar and Achilles Tendons. J. Aging Phys. Act. 2020, 29, 382–390. [Google Scholar] [CrossRef]
- Klauser, A.S.; Miyamoto, H.; Tamegger, M.; Faschingbauer, R.; Moriggl, B.; Klima, G.; Feuchtner, G.M.; Kastlunger, M.; Jaschke, W.R. Achilles tendon assessed with sonoelastography: Histologic agreement. Radiology 2013, 267, 837–842. [Google Scholar] [CrossRef]
- Tas, S.; Onur, M.R.; Yilmaz, S.; Soylu, A.R.; Korkusuz, F. Shear wave elastography is a reliable and repeatable method for measuring the elastic modulus of the rectus femoris muscle and patellar tendon. J. Ultrasound Med. 2017, 36, 565–570. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Tempfer, H.; Traweger, A. Tendon Vasculature in Health and Disease. Front. Physiol. 2015, 6, 330. [Google Scholar] [CrossRef]
- Arampatzis, A.; Peper, A.; Bierbaum, S.; Albracht, K. Plasticity of human Achilles tendon mechanical and morphological properties in response to cyclic strain. J. Biomech. 2010, 43, 3073–3079. [Google Scholar] [CrossRef]
- Reeves, N.D.; Maganaris, C.N.; Narici, M.V. Effect of strength training on human patella tendon mechanical properties of older individuals. J. Physiol. 2003, 548, 971–981. [Google Scholar] [CrossRef] [PubMed]
- Seynnes, O.R.; Erskine, R.M.; Maganaris, C.N.; Longo, S.; Simoneau, E.M.; Grosset, J.F.; Narici, M.V. Training-induced changes in structural and mechanical properties of the patellar tendon are related to muscle hypertrophy but not to strength gains. J. Appl. Physiol. 2009, 107, 523–530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kongsgaard, M.; Aagaard, P.; Kjaer, M.; Magnusson, S.P. Structural Achilles tendon properties in athletes subjected to different exercise modes and in Achilles tendon rupture patients. J. Appl. Physiol. 2005, 99, 1965–1971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farup, J.; Rahbek, S.K.; Vendelbo, M.H.; Matzon, A.; Hindhede, J.; Bejder, A.; Ringgard, S.; Vissing, K. Whey protein hydrolysate augments tendon and muscle hypertrophy independent of resistance exercise contraction mode. Scand. J. Med. Sci. Sports 2014, 24, 788–798. [Google Scholar] [CrossRef]
- Heinemeier, K.M.; Kjaer, M. In vivo investigation of tendon responses to mechanical loading. J. Musculoskelet Neuronal Interact. 2011, 11, 115–123. [Google Scholar]
- Heinemeier, K.M.; Olesen, J.L.; Schjerling, P.; Haddad, F.; Langberg, H.; Baldwin, K.M.; Kjaer, M. Short-term strength training and the expression of myostatin and IGF-I isoforms in rat muscle and tendon: Differential effects of specific contraction types. J. Appl. Physiol. 2007, 102, 573–581. [Google Scholar] [CrossRef] [Green Version]
- Kaux, J.F.; Drion, P.; Libertiaux, V.; Colige, A.; Hoffmann, A.; Nusgens, B.; Besançon, B.; Forthomme, B.; Le Goff, C.; Franzen, R.; et al. Eccentric training improves tendon biomechanical properties: A rat model. J. Orthop. Res. 2013, 31, 119–124. [Google Scholar] [CrossRef]
- Miller, B.F.; Olesen, J.L.; Hansen, M.; Dossing, S.; Crameri, R.M.; Welling, R.J.; Langberg, H.; Flyvbjerg, A.; Kjaer, M.; Babraj, J.A.; et al. Coordinated collagen and muscle protein synthesis in human patella tendon and quadriceps muscle after exercise. J. Physiol. 2005, 567, 1021–1033. [Google Scholar] [CrossRef]
- Zhang, Z.J.; Ng, G.Y.; Lee, W.C.; Fu, S.N. Changes in morphological and elastic properties of patellar tendon in athletes with unilateral patellar tendinopathy and their relationships with pain and functional disability. PLoS ONE 2014, 9, e108337. [Google Scholar] [CrossRef] [Green Version]
- Shalabi, A.; Kristoffersen-Wiberg, M.; Aspelin, P.; Movin, T. Immediate Achilles tendon response after strength training evaluated by MRI. Med. Sci. Sports Exerc. 2004, 36, 1841–1846. [Google Scholar] [CrossRef] [Green Version]
- Kubo, K.; Kanehisa, H.; Ito, M.; Fukunaga, T. Effects of isometric training on the elasticity of human tendon structures in vivo. J. Appl. Physiol. 2001, 91, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Porta, F.; Damjanov, N.; Galluccio, F.; Iagnocco, A.; Matucci-Cerinic, M. Ultrasound elastography is a reproducible and feasible tool for the evaluation of the patellar tendon in healthy subjects. Int. J. Rheum. Dis. 2014, 17, 762–766. [Google Scholar] [CrossRef]
- Grosse, U.; Syha, R.; Gatidis, S.; Grozinger, G.; Martirosian, P.; Partovi, S.; Nikolaou, K.; Robbin, M.R.; Schick, F.; Springer, F. MR-based in vivo follow-up study of Achilles tendon volume and hydration state after ankle-loading activity. Scand. J. Med. Sci. Sports 2016, 26, 1200–1208. [Google Scholar] [CrossRef] [PubMed]
- Ho, K.Y.; Kulig, K. Changes in water content in response to an acute bout of eccentric loading in a patellar tendon with a history of tendinopathy: A case report. Physiother. Theory Pract. 2016, 32, 566–570. [Google Scholar] [CrossRef] [PubMed]
- Kubo, K.; Ikebukuro, T.; Maki, A.; Yata, H.; Tsunoda, N. Time course of changes in the human Achilles tendon properties and metabolism during training and detraining in vivo. Eur. J. Appl. Physiol. 2012, 112, 2679–2691. [Google Scholar] [CrossRef] [PubMed]
- Kubo, K.; Ikebukuro, T.; Yata, H.; Tsunoda, N.; Kanehisa, H. Time course of changes in muscle and tendon properties during strength training and detraining. J. Strength Cond. Res. 2010, 24, 322–331. [Google Scholar] [CrossRef]
- Michna, H.; Hartmann, G. Adaptation of tendon collagen to exercise. Int. Orthop. 1989, 13, 161–165. [Google Scholar] [CrossRef]
- Magnusson, S.P.; Hansen, P.; Kjaer, M. Tendon properties in relation to muscular activity and physical training. Scand. J. Med. Sci. Sports 2003, 13, 211–223. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PRE | POST-1 | POST-2 | ANOVA Main Effects | F | p-Value | |
|---|---|---|---|---|---|---|
| Length PT (cm) | ||||||
| CG | 4.53 ± 0.42 | 4.45 ± 0.47 | 4.44 ± 0.46 | Time | 0.37 | 0.694 |
| EG6s | 4.49 ± 0.64 | 4.45 ± 0.58 | 4.46 ± 0.55 | Group | 0.36 | 0.702 |
| EG3s | 4.47 ± 0.43 | 4.38 ± 0.39 | 4.47 ± 0.38 | Time × group | 0.60 | 0.667 |
| Thickness PT in patella (cm) | ||||||
| CG | 0.48 ± 0.05 | 0.48 ± 0.06 | 0.47 ± 0.05 | Time | 12.35 | <0.001 |
| EG6s | 0.45 ± 0.10 | 0.47 ± 0.09 | 0.43 ± 0.08 # | Group | 0.48 | 0.621 |
| EG3s | 0.45 ± 0.08 | 0.48 ± 0.09 * | 0.44 ± 0.07 # | Time × group | 2.69 | 0.037 |
| Thickness PT 25% (cm) | ||||||
| CG | 0.41 ± 0.06 | 0.40 ± 0.06 | 0.39 ± 0.06 | Time | 27.67 | <0.001 |
| EG6s | 0.38 ± 0.07 | 0.42 ± 0.07 * | 0.36 ± 0.07 # | Group | 0.26 | 0.773 |
| EG3s | 0.39 ± 0.07 | 0.41 ± 0.08 * | 0.35 ± 0.05 # | Time × group | 8.10 | <0.001 |
| Thickness PT 50% (cm) | ||||||
| CG | 0.39 ± 0.06 | 0.37 ± 0.05 | 0.37 ± 0.04 | Time | 13.17 | <0.001 |
| EG6s | 0.35 ± 0.05 | 0.42 ± 0.07 * | 0.34 ± 0.06 # | Group | 3.58 | 0.037 |
| EG3s | 0.31 ± 0.07 ¥ | 0.34 ± 0.07 *,† | 0.33 ± 0.07 | Time × group | 7.80 | <0.001 |
| Thickness PT 75% (cm) | ||||||
| CG | 0.40 ± 0.05 | 0.39 ± 0.04 | 0.40 ± 0.04 | Time | 11.89 | <0.001 |
| EG6s | 0.38 ± 0.06 | 0.44 ± 0.07 * | 0.37 ± 0.07 # | Group | 1.51 | 0.232 |
| EG3s | 0.36 ± 0.07 | 0.39 ± 0.07 * | 0.35 ± 0.07 # | Time × group | 3.91 | 0.006 |
| Thickness PT in tibia(cm) | ||||||
| CG | 0.51 ± 0.07 | 0.49 ± 0.08 | 0.50 ± 0.07 | Time | 6.23 | 0.004 |
| EG6s | 0.51 ± 0.09 | 0.56 ± 0.10 * | 0.48 ± 0.08 # | Group | 1.20 | 0.310 |
| EG3s | 0.46 ± 0.10 | 0.48 ± 0.09 | 0.47 ± 0.07 | Time × group | 7.14 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez, F.; Abián, P.; Jiménez, F.; Abián-Vicén, J. The Effects of Eccentric Contraction Execution Time on the Properties of the Patellar Tendon. Int. J. Environ. Res. Public Health 2022, 19, 9296. https://doi.org/10.3390/ijerph19159296
Martínez F, Abián P, Jiménez F, Abián-Vicén J. The Effects of Eccentric Contraction Execution Time on the Properties of the Patellar Tendon. International Journal of Environmental Research and Public Health. 2022; 19(15):9296. https://doi.org/10.3390/ijerph19159296
Chicago/Turabian StyleMartínez, Fernando, Pablo Abián, Fernando Jiménez, and Javier Abián-Vicén. 2022. "The Effects of Eccentric Contraction Execution Time on the Properties of the Patellar Tendon" International Journal of Environmental Research and Public Health 19, no. 15: 9296. https://doi.org/10.3390/ijerph19159296