
Changes in the Color and Brightness of White Spots Associated with Orthodontic Treatment 6 Months after the Application of Infiltrative Resins: Systematic Review and Meta-Analysis

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Data Sources
2.2. Eligibility. Inclusion and Exclusion Criteria
2.3. Study Selections and Data Extraction
2.4. Risk of Bias Assessment
2.5. Data Analysis
3. Results
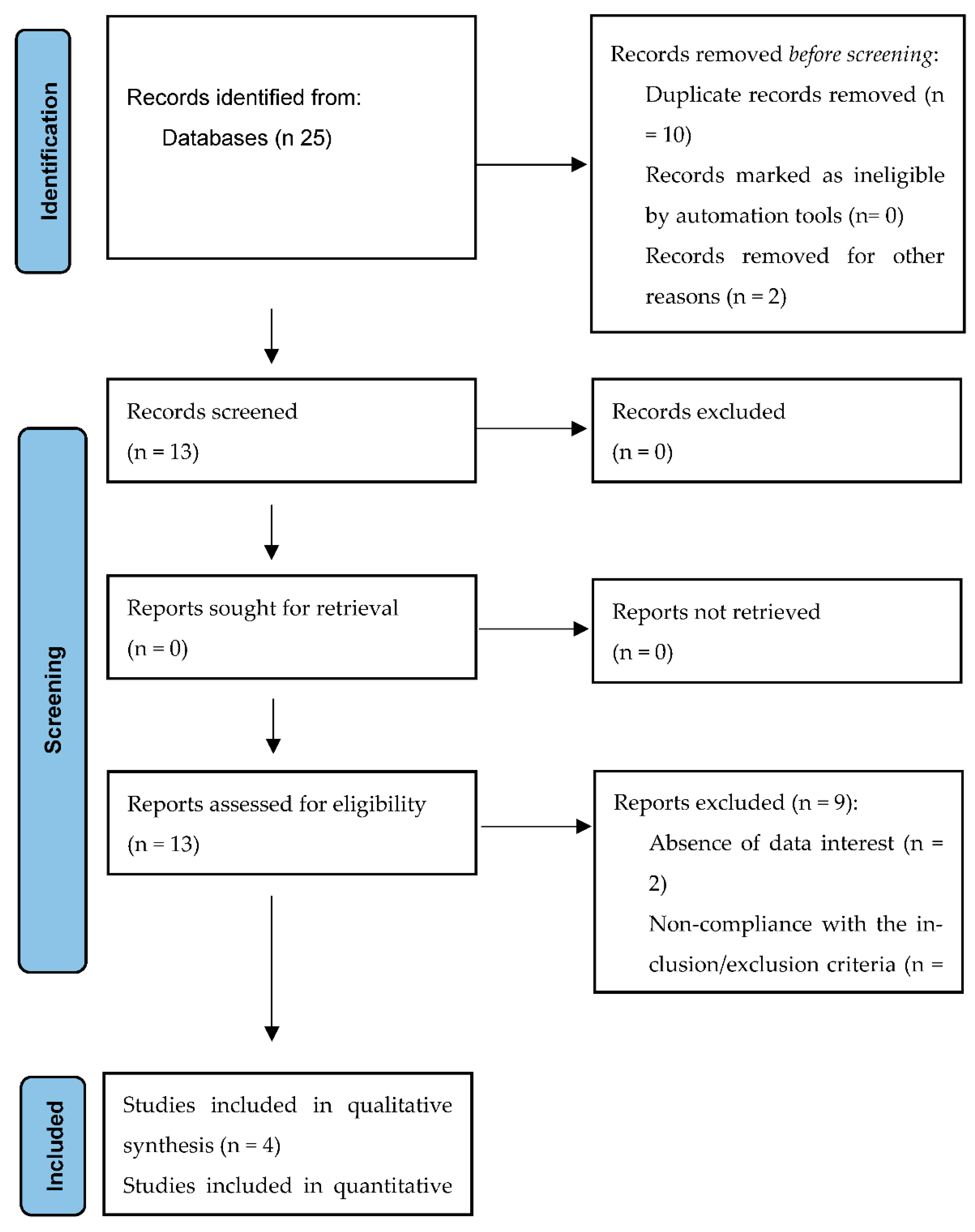
3.1. Article Selections
3.2. Study Characteristics
3.3. Results of Meta-Analysis
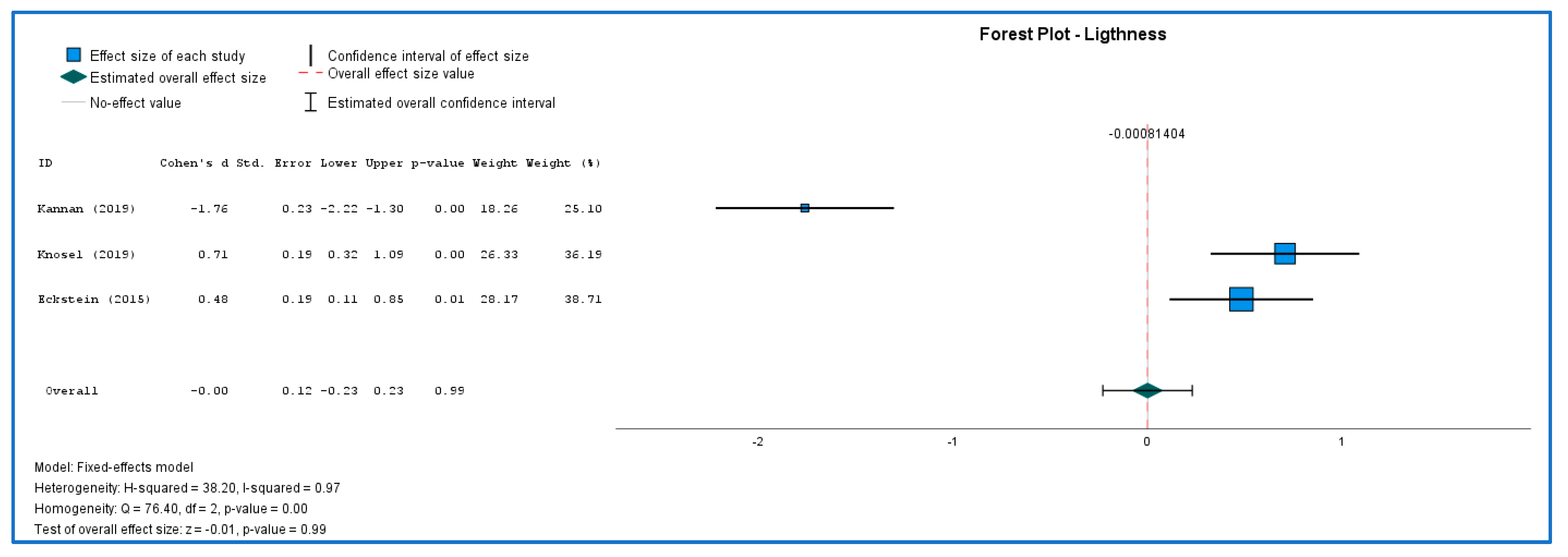
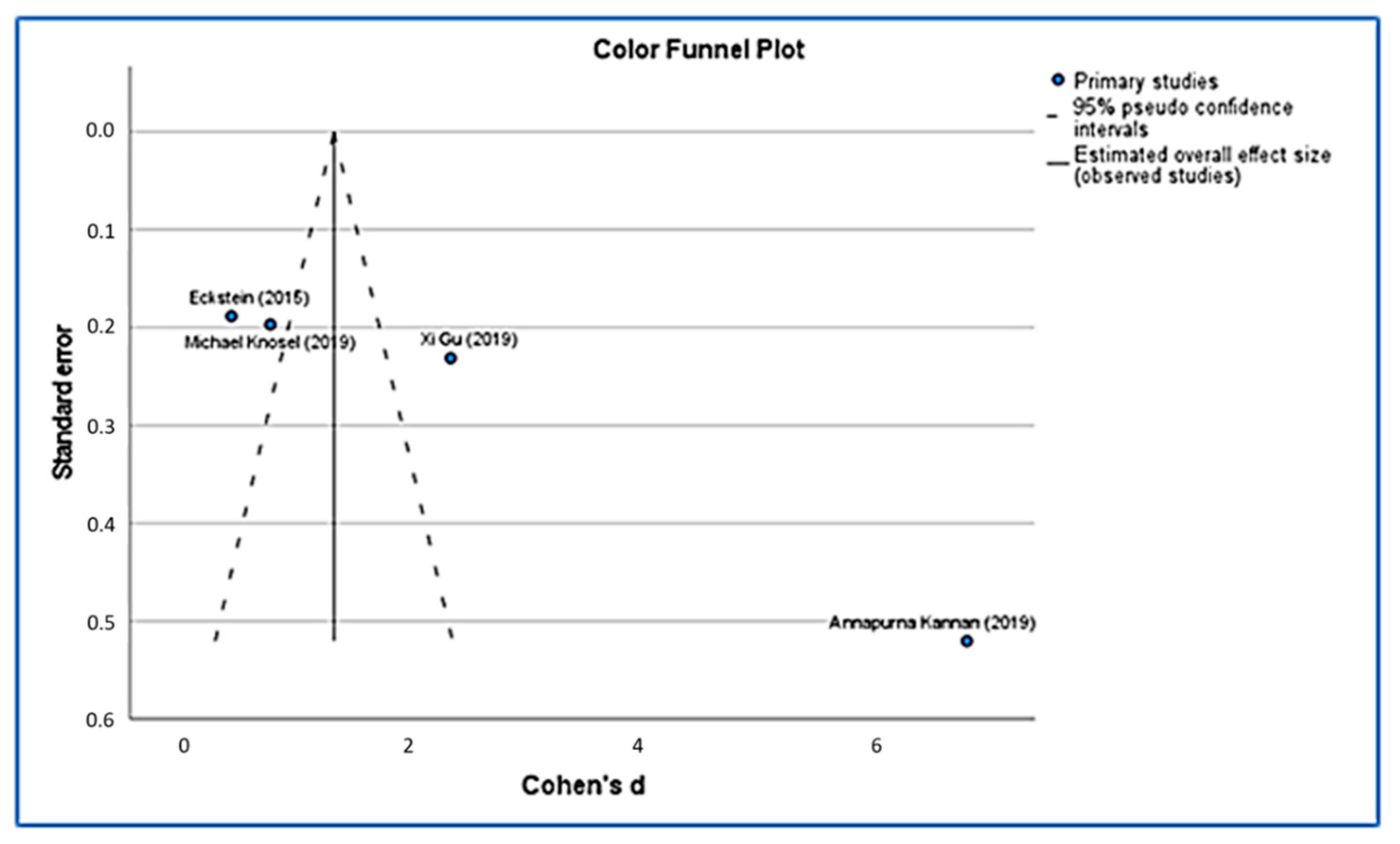
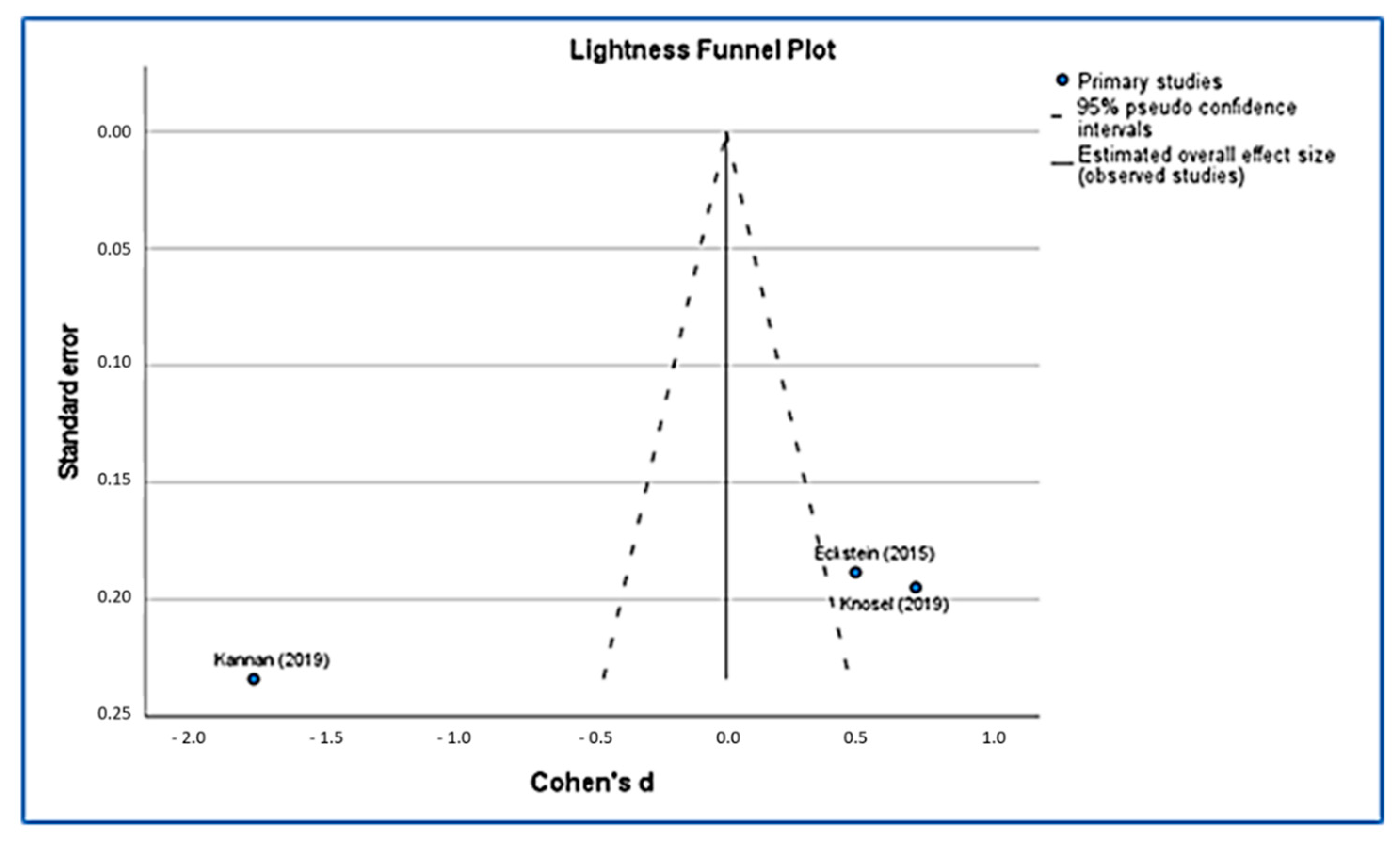
3.3.1. Color and Lightness Evaluation
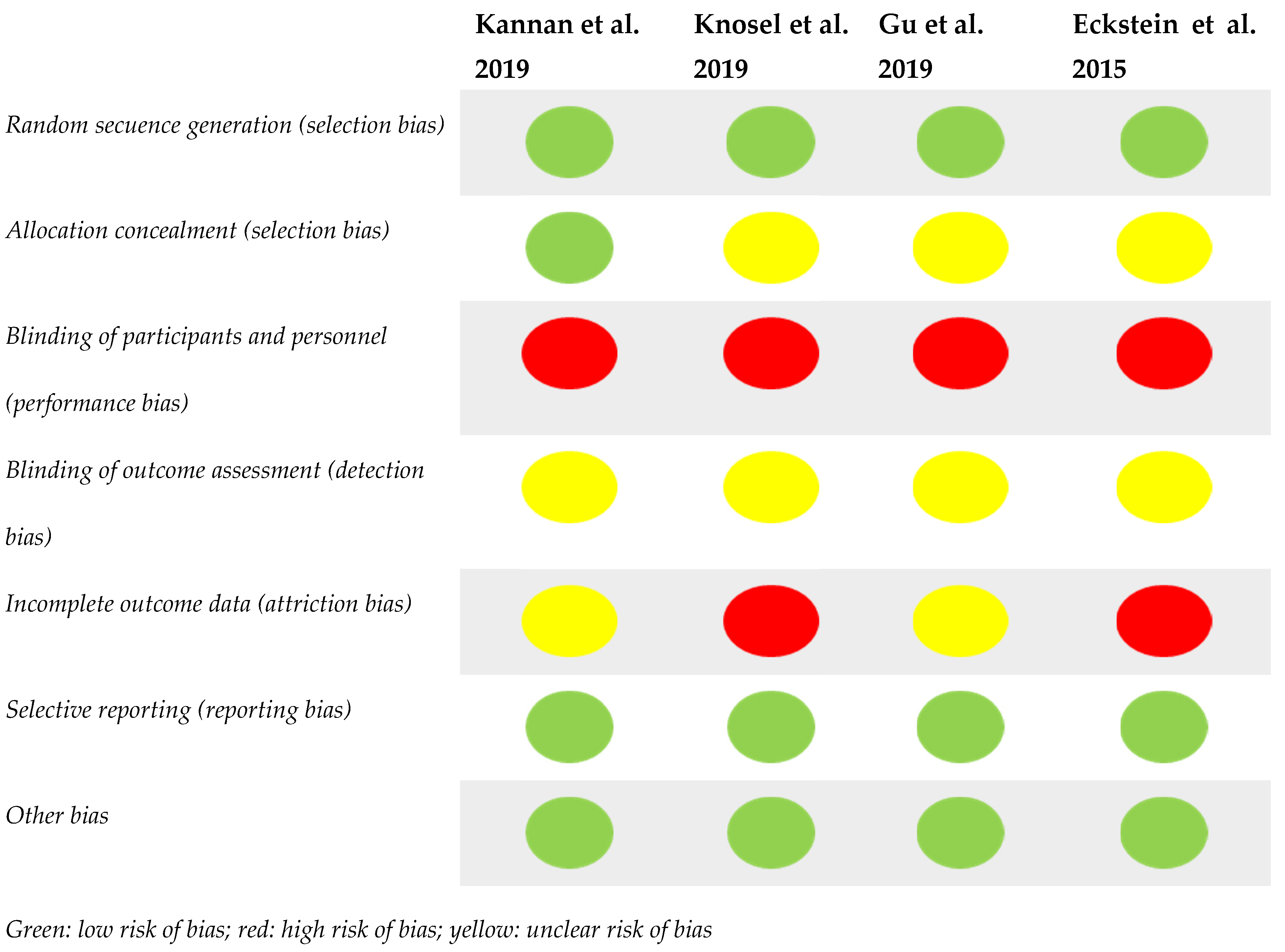
3.3.2. Risk of Bias
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alshammari, F.M.; Sanea, J.A. Efficacy of amorphous calcium phosphate (ACP) containing adhesive in preventing demineralization during orthodontic treatment, a triple blinded randomized clinical trial (RCT). J. Contemp. Dent. Pract. 2019, 20, 727–731. [Google Scholar] [CrossRef] [PubMed]
- Derks, A.; Katsaros, C.; Frenckenet, J.E.; Van’t Hof, M.A.; Kujipers-Jagtman, A.M. Caries-inhibiting effect of preventive measures during orthodontic treatment with fixed appliances. A systematic review. Caries Res. 2004, 38, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Poornima, P.; Krithikadatta, J.; Ponraj, R.R.; Velmurugan, N.; Kishen, A. Biofilm formation following chitosan-based varnish or chlorhexidine-fluoride varnish application in patients undergoing fixed orthodontic treatment: A double blinded randomised controlled trial. BMC Oral Health 2021, 21, 465. [Google Scholar] [CrossRef] [PubMed]
- Heymann, G.C.; Grauer, D. A contemporary review of white spot lesions in orthodontics. J. Esthet. Restor. Dent. 2013, 25, 85–95. [Google Scholar] [CrossRef]
- Kamber, R.; Meyer-Lueckel, H.; Kloukos, D.; Tennert, C.; Wierichs, R.J. Efficacy of sealants and bonding materials during fixed orthodontic treatment to prevent enamel demineralization: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 16556. [Google Scholar]
- Tufekci, E.; Dixon, J.S.; Gunsolley, J.C.; Lindauer, S.J. Prevalence of white spot lesions during orthodontic treatment with fixed appliances. Angle Orthod. 2011, 81, 206–210. [Google Scholar] [CrossRef] [Green Version]
- Boersma, J.G.; Van der Veen, M.H.; Lagerweij, M.D.; Bokhout, B.; Prahl-Andersen, B. Caries prevalence measured with QLF after treatment with fixed orthodontic appliances: Influencing factors. Caries Res. 2005, 39, 41–47. [Google Scholar] [CrossRef]
- Gorelick, L.; Geiger, A.M.; Gwinnet, A.J. Incidence of white spot formation after bonding and banding. Am. J. Orthod. 1982, 81, 93–98. [Google Scholar]
- Julien, K.C.; Buschang, P.H.; Campbell, P.M. Prevalence of white spot lesion formation during orthodontic treatment. Angle Orthod. 2013, 83, 641–647. [Google Scholar] [CrossRef]
- Sundararaj, D.; Venkatachalapathy, S.; Tandon, A.; Pereira, A. Critical evaluation of incidence and prevalence of white spot lesions during fixed orthodontic appliance treatment: A meta-analysis. J. Int. Soc. Prev. Community Dent. 2015, 5, 433–439. [Google Scholar]
- Buschang, P.H.; Chastain, D.; Keylor, C.L.; Crosby, D.; Julien, K.C. Incidence of white spot lesions among patients treated with clear aligners and traditional braces. Angle Orthod. 2019, 89, 359–364. [Google Scholar]
- Khalaf, K. Factors affecting the formation, severity and location of white spot lesions during orthodontic treatment with fixed appliances. J. Oral Maxillofac. Res. 2014, 5, 1–10. [Google Scholar]
- Lovrov, S.; Hertrich, K.; Hirschfelderet, U. Enamel demineralization during fixed orthodontic treatment-incidence and correlation to various oral-hygiene parameters. J. Orofac. Orthop. 2007, 68, 353–363. [Google Scholar]
- Lucchese, A.; Gherlone, E. Prevalence of white-spot lesions before and during orthodontic treatment with fixed appliances. Eur. J. Orthod. 2013, 35, 664–668. [Google Scholar]
- Ata-Ali, F.; Ata-Ali, J.; Ferrer-Molina, M.; Cobo, T.; De Carlos, F.; Cobo, J. Adverse effects of lingual and buccal orthodontic techniques. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 820–829. [Google Scholar] [CrossRef]
- Derks, A.; Kuijpers-Jagtman, A.M.; Frencken, J.E.; Van’t Hof, M.A.; Katsaros, C. Caries preventive measures used in orthodontic practices: An evidence-based decision? Am. J. Orthod. Dentofac. Orthop. 2007, 132, 165–170. [Google Scholar]
- Opsahl-Vital, S.; Haignere-Rubinstein, C.; Lasfargues, J.J.; Chaussain, C. Caries risk and orthodontic treatment. Int. Orthod. 2010, 8, 28–45. [Google Scholar]
- Enerbäck, H.; Lingström, P.; Möller, M.; Nylén, C.; Bresin, C.Ö.; Ros, I.Ö.; Westerlund, A. Validation of caries risk assessment methods in orthodontic patients. Am. J. Orthod. Dentofac. Orthop. 2020, 58, 92–101. [Google Scholar]
- Wang, Y.; Qin, D.; Guo, F.; Levey, C.; Huang, G.; Ngan, P.; Hua, F.; He, H. Outcomes used in trials regarding the prevention and treatment of orthodontically induced white spot lesions: A scoping review. Am. J. Orthod. Dentofac. Orthop. 2021, 160, 659–670. [Google Scholar]
- Govindaraj, A.; Dinesh, S. Effect of Chlorhexidine Varnish and Fluoride Varnish on White Spot Lesions in Orthodontic Patients-a Systematic Review. Open Dent. J. 2021, 15, 151–159. [Google Scholar]
- Perrini, F.; Lombardo, L.; Arreghini, A.; Medori, S.; Siciliani, G. Caries prevention during orthodontic treatment: In-vivo assessment of high-fluoride varnish to prevent white spot lesions. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Firzok, H.; Zahid, S.; Asad, S.; Manzoor, F.; Khan, A.S.; Shah, A.T. Sol-gel derived fluoridated and non-fluoridated bioactive glass ceramics-based dental adhesives: Compositional effect on re-mineralization around orthodontic brackets. J. Non-Cryst. Solids 2019, 521, 1–8. [Google Scholar] [CrossRef]
- Ali, A.; Ismail, H.; Amin, K. Effect of nanosilver mouthwash on prevention of white spot lesions in patients undergoing fixed orthodontic treatment—A randomized double-blind clinical trial. J. Dent. Sci. 2021, 17, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Kamran, M.A.; Alnazeh, A.A.; Hameed, M.S.; Yassin, S.M.; Mannakandath, M.L.; Alshahrani, I. Formulation and clinical performance of nanosilver loaded poly-l-glycolic acid modified orthodontic adhesive for orthodontic bonding. J. Mol. Struct. 2022, 1249, 131490. [Google Scholar] [CrossRef]
- Khursheed-Alam, M.J.; Alsuwailem, R.; Ali-Alfawzan, A. Antibacterial activity and bond strength of silver nanoparticles modified orthodontic bracket adhesive: A systematic review and meta-analysis of in-vitro and in-vivo studies. Int. J. Adhes. Adhes. 2021, 113, 103040. [Google Scholar] [CrossRef]
- Amaechi, B.T.; McGarrell, B.; Luong, M.N.; Okoye, L.N.; Gakunga, P.T. Prevention of white spot lesions around orthodontic brackets using organoselenium-containing antimicrobial enamel surface sealant. Heliyon 2021, 7, e06490. [Google Scholar] [CrossRef]
- Bishara, S.E.; Ostby, A.W. White spot lesions: Formation, prevention, and treatment. Semin. Orthod. 2008, 30, 174–182. [Google Scholar] [CrossRef]
- Lopatiene, K.; Borisovaite, M.; Lapenaite, E. Prevention and treatment of white spot lesions during and after treatment with fixed orthodontic appliances: A systematic literature review. J. Oral Maxillofac. Res. 2016, 7, e1. [Google Scholar] [CrossRef] [Green Version]
- Munjal, D.; Garg, S.; Dhindsa, A.; Sidhu, G.K.; Sethi, H.S. Assessment of White Spot Lesions and In-Vivo Evaluation of the Effect of CPP-ACP on White Spot Lesions in Permanent Molars of Children. J. Clin. Diagn. Res. 2016, 10, 149–154. [Google Scholar] [CrossRef]
- Ebrahimi, M.; Mehrabkhani, M.; Ahrari, F.; Parisay, I.; Jahantigh, M. The effects of three remineralizing agents on regression of white spot lesions in children: A two-week, single-blind, randomized clinical trial. J. Clin. Exp. Dent. 2017, 9, 641–648. [Google Scholar] [CrossRef] [Green Version]
- Singh, S.; Singh, S.P.; Utreja, A.K.; Jena, A.K. Effects of various remineralizing agents onthe outcome of post-orthodontic white spot lesions (WSLs): A clinical trial. Prog. Orthop. 2016, 17, 25. [Google Scholar] [CrossRef] [Green Version]
- Bröchner, A.; Christensen, C.; Kristensen, B.; Tranæus, S.; Karlsson, L.; Sonnesen, L. Treatment of post-orthodontic white spot lesions with casein phosphopeptide-stabilised amorphous calcium phosphate. Clin. Oral Investig. 2011, 15, 369–373. [Google Scholar] [CrossRef]
- Sonesson, M.; Bergstrand, F.; Gizani, S.; Twetman, S. Management of postorthodontic white spot lesions: An updated systematic review. Eur. J. Orthod. 2016, 39, 116–121. [Google Scholar]
- Yetkiner, E.; Wegehaupt, F.; Wiegand, A.; Attin, R.; Attin, T. Colour improvement and stability of white spot lesions following infiltration, micro-abrasion, or fluoride treatments in vitro. Eur. J. Orthod. 2014, 36, 595–602. [Google Scholar] [CrossRef] [Green Version]
- Kobbe, C.; Fritz, U.; Wierichs, R.J.; Meyer-Lueckela, H. Evaluation of the value of re-wetting prior to resin infiltration of post-orthodontic caries lesions. J. Dent. 2019, 19, 103243. [Google Scholar] [CrossRef]
- Eckstein, A.; Helms, H.J.; Knösel, M. Camouflage effects following resin infiltration of postorthodontic white-spot lesions in vivo: One-year follow-up. Angle Orthod. 2015, 85, 374–380. [Google Scholar] [CrossRef] [Green Version]
- Paris, S.; Meyer-Lueckel, H.; Kielbassa, A.M. Resin infiltration of natural caries lesions. J. Dent. Res. 2007, 86, 662–666. [Google Scholar] [CrossRef]
- Paris, S.; Hopfenmuller, W.; Meyer-Lueckel, H. Resin infiltration of caries lesions: An efficacy randomized trial. J. Dent. Res. 2010, 89, 823–826. [Google Scholar] [CrossRef]
- Doméjean, S.; Ducamp, R.; Léger, S.; Holmgren, C. Resin infiltration of non-cavitated caries lesions: A systematic review. Med. Princ. Pract. 2015, 24, 216–221. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. Ann. Intern. Med. 2009, 151, 65–94. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.; Higgins, J.; Reeves, B. A Cochrane risk of bias assessment tool: For non-randomized studies of interventions (ACROBAT-NRSI). Version 2014, 1, 24. [Google Scholar]
- Kannan, A.; Padmanabhan, S. Comparative evaluation of Icon® resin infiltration and Clinpro™ XT varnish on colour and fluorescence changes of white spot lesions: A randomized controlled trial. Prog. Orthod. 2019, 20, 23. [Google Scholar] [CrossRef] [PubMed]
- Knosel, M.; Ecksteinb, A.; Helmsc, H.J. Long-term follow-up of camouflage effects following resin infiltration of post orthodontic white-spot lesions in vivo. Angle Orthod. 2019, 89, 33–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gu, X.; Yang, L.; Yang, D.; Gao, Y.; Duane, X.; Zhue, X.; Yuan, H.; Lig, J. Esthetic improvements of postorthodontic white-spot lesions treated with resin infiltration and microabrasion: A split-mouth, randomized clinical trial. Angle Orthod. 2019, 89, 372–377. [Google Scholar] [CrossRef] [Green Version]
- Huedo-Medina, T.B.; Sánchez-Meca, J.; Marin-Martinez, F.; Botella, J. Assessing heterogeneity in meta-analysis: Q statistic or I2 index? Psychol. Methods 2006, 11, 193. [Google Scholar] [CrossRef] [Green Version]
- Heravi, F.; Ahrari, F.; Tanbakuchi, B. Effectiveness of MI Paste Plus and Remin Pro on remineralization and color improvement of postorthodontic white spot lesions. Dent. Res. J. 2018, 15, 95–103. [Google Scholar]
- Agarwal, A.; Pandey, H.; Pandey, L.; Choudhary, G. Effect of Fluoridated Toothpaste on White Spot Lesions in Postorthodontic Patients. Int. J. Clin. Pediatr. Dent. 2013, 6, 85–88. [Google Scholar]
- Badiee, M.; Jafari, N.; Fatemi, S.; Ameli, N.; Kasraei, S.; Ebadifar, A. Comparison of the effects of toothpastes containing nanohydroxyapatite and fluoride on white spot lesions in orthodontic patients: A randomized clinical trial. Dent. Res. J. 2020, 17, 354–359. [Google Scholar]
- Benson, P. Evaluation of white spot lesions on teeth with orthodontic brackets. Semin. Orthod. 2008, 14, 200–208. [Google Scholar] [CrossRef]
- Fondriest, J. Shade matching in restorative dentistry: The science and strategies. Int. J. Periodontics Restor. Dent. 2003, 23, 467–479. [Google Scholar] [CrossRef]
- Darling, C.L.; Huynh, G.D.; Fried, D. Light scattering properties of natural and artificially demineralized dental enamel at 1310 nm. J. Biomed. Opt. 2006, 11, 34023. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author and Year | Journal | Study Type | Type of Treatment | Tooth Type | Sample (Teeth) | Assessment Criterion | Follow-Up | Results |
|---|---|---|---|---|---|---|---|---|
| Kannan (2019) [43] | Prog. Orthod | RCT | Icon® resin infiltration Clinpro xt Varnish® | Incisor, canine, premolars, first molar | 102 | Color, Brightness | 3, 6 months | The immediate results were better with resin infiltration, but at 3/6 months the situation was reversed. |
| Knosel (2019) [44] | Angle Orthod. | RCT | Icon® resin infiltration Control Group | Permanent teeth. | 111 | Color, Brightness | 6, 12, 24, 45 months | Improved long-term WLS with stable results. |
| Gu (2019) [45] | Angle Orthod. | RCT | Icon® resin infiltration Microabrasion | Permanent anterior teeth. | 128 | Color | 1 week, 6, 12 months | Similar results in both methods, slightly superior with resin infiltration. |
| Eckstein (2015) [36]) | Angle Orthod. | RCT | Icon® resin infiltration | Permanent teeth | 117 | Color, Brightness | 1, 6, 12 months | Color and brightness improve after resin infiltration and results are stable in the long run. |
| Group | Teeth | Lightness | Colour | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T0 (before Intervetion) | T1 (6 Month after Intervetion) | T0 (before Intervetion) | T1 (6 Month after Intervetion) | Change t0–t1 | ||||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | |||
| Kannan (2019) [43] | Icon resin infiltration | 102 | 74 | 0.8 | 81.88 | 6.27 | 9.66 | 1.42 | ||||
| Knosel (2019) [44] | Icon resin infilltration | 111 | 73.9 | 4.84 | 70.96 | 3.36 | 9.12 | 5.63 | 5.5 | 2.76 | 3.61 | |
| Gu (2019) [45] | Icon resin infiltration | 128 | 6.57 | 2.48 | 2.20 | 0.82 | ||||||
| Eckstein (2015) [36] | Icon resin infiltration | 117 | 72.55 | 3.45 | 70.88 | 3.49 | 8.15 | 3.74 | 6.33 | 3.81 | 1.81 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baptista-Sánchez, H.; Antonio-Zancajo, L.; Albaladejo-Martínez, A.; Colino Gallardo, P.; Garcovich, D.; Alvarado-Lorenzo, M.; Alvarado-Lorenzo, A. Changes in the Color and Brightness of White Spots Associated with Orthodontic Treatment 6 Months after the Application of Infiltrative Resins: Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 9277. https://doi.org/10.3390/ijerph19159277
Baptista-Sánchez H, Antonio-Zancajo L, Albaladejo-Martínez A, Colino Gallardo P, Garcovich D, Alvarado-Lorenzo M, Alvarado-Lorenzo A. Changes in the Color and Brightness of White Spots Associated with Orthodontic Treatment 6 Months after the Application of Infiltrative Resins: Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2022; 19(15):9277. https://doi.org/10.3390/ijerph19159277
Chicago/Turabian StyleBaptista-Sánchez, Hugo, Laura Antonio-Zancajo, Alberto Albaladejo-Martínez, Pedro Colino Gallardo, Daniele Garcovich, Mario Alvarado-Lorenzo, and Alfonso Alvarado-Lorenzo. 2022. "Changes in the Color and Brightness of White Spots Associated with Orthodontic Treatment 6 Months after the Application of Infiltrative Resins: Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 19, no. 15: 9277. https://doi.org/10.3390/ijerph19159277