
Association between Pre-Pregnancy Overweightness/Obesity and Pregnancy Outcomes in Women with Polycystic Ovary Syndrome: A Systematic Review and Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction and Risk of Bias Assessment
2.4. Statistical Analysis
3. Results
3.1. Study Selection
3.2. Study Characteristics

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study [Reference], Year (Country) | Study Design | Study Population | Outcome | PCOS Criteria | Con Method | Detail of Con Method | NOS Score | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| BMI (kg/m2) | Sample Size | Age(y) | Miscarriage A: Definition of Miscarriage B: Definition of Miscarriage (M) Rate | Live Birth A: Definition of Live Birth B: Definition of Live Birth (L) Rate | Preterm Birth A: Definition of Preterm Birth B: Definition of Preterm Birth (P) Rate | ||||||
| Hamilton-Fairley et al. [40]. 1992 (UK) | RC | ≧25.0, <28 | 25 | 30.9 ± 3.7 | A: not mentioned B: M/positive pregnancy test | Adams (US) | OI | Gonadotrophin | 9 | ||
| ≧19, <25 | 75 | 29.8 ± 4.3 | |||||||||
| McCormick et al. [15]. 2008 (USA) | RC | ≧30 | 10 | 31.5 ± 5.0 | A: GA < 20 weeks B: M/positive pregnancy test | A: alive newborn B: L/egg retrievals | Rot | IVF | GnRH agonist protocol (97.9%); GnRH-anta protocol (2.1%) | 9 | |
| ≧18.5, <30 | 6 | 31.5 ± 3.0 | |||||||||
| Ozgun et al. [19]. 2011 (Turkey) | PC | ≧30 | 18 | 26.7 ± 2.9 | A: GA < 20 weeks B: M/clinical pregnancy | A: not mentioned B: L/all patients | Rot | ICSI | Long protocol | 8 | |
| <30 | 26 | 26.8 ± 4.5 | |||||||||
| Shalom-Paz et al. [13]. 2011 (Canada) | RC | ≧35, | 13 | 29.6 ± 1.0 | A: not mentioned B: M/clinical pregnancy | A: not mentioned B: L/clinical pregnancy | Rot | IVF | Not mentioned | 7 | |
| ≧30, <35 | 12 | 31.0 ± 0.9 | |||||||||
| ≧25, <30 | 24 | 31.2 ± 0.7 | |||||||||
| ≧20, <25 | 50 | 30.8 ± 0.4 | |||||||||
| <20 | 17 | 31.3 ± 0.8 | |||||||||
| De Frène et al. [34]. 2014 (Belgium) | RC | >25 | 93 | 29.0 ± 4.2 | A: GA < 25 weeks B: M/positive hCG at GA 4 weeks | A: GA < 37 weeks B: P/live birth | Rot | Any | Not mentioned | 8 | |
| ≦25 | 107 | 28.4 ± 3.1 | |||||||||
| Huang et al. [21]. 2014 (China) | RC | ≧24 | 49 | 30.5 ± 4.1 | A: not mentioned B: M/clinical pregnancy | A: alive and survived > 1 month B: L/all patients | Rot | IVF/ICSI | Not mentioned | 7 | |
| <24 | 79 | 29.4 ± 3.4 | |||||||||
| Bailey et al. [35]. 2014 (USA) | RC | ≧30 | 31 | 32.4 ± 3.2 | A: GA < 20 weeks B: M/FET cycles | A: alive newborn B: L/FET cycles | Rot | IVF/ICSI | Not mentioned | 8 | |
| ≧25, <30 | 19 | 32.6 ± 2.9 | |||||||||
| ≧18.7, <25 | 51 | 32.0 ± 3.5 | |||||||||
| Cui et al. [20]. 2016 (China) | RC | ≧28 | 88 | 27.50 ± 3.4 | A: GA < 20 weeks B: M/clinical pregnancy | A: not mentioned B: P/clinical pregnancy | Rot | IVF/ICSI | Long protocol | 6 | |
| ≧24, <28 | 125 | 27.50 ± 3.1 | |||||||||
| ≧18.5, <24 | 183 | 26.99 ± 2.9 | |||||||||
| <18.5 | 12 | 27.33 ± 3.3 | |||||||||
| Sheng et al. [12]. 2017 (China) | PC | ≧28 | 63 | 28.7 ± 2.7 | A: <1 st trimester B: M/clinical pregnancy | Rot | IVF/ICSI | Long protocol | 7 | ||
| ≧24, <28 | 211 | 28.5 ± 3.1 | |||||||||
| ≧18.5, <24 | 449 | 27.7 ± 3.1 | |||||||||
| <18.5 | 51 | 26.3 ± 3.1 | |||||||||
| Pan et al. [14]. 2018 (China) | RC | ≧28 | 102 | 29.77 ± 3.5 | A: GA < 28 weeks B: M/ET | A: alive newborn B: L/ET | A: GA 28~37 weeks B: P/ET | Rot | IVF | Long protocol | 6 |
| ≧24, <28 | 315 | 29.45 ± 3.5 | |||||||||
| ≧18.5, <24 | 606 | 29.08 ± 3.2 | |||||||||
| <18.5 | 51 | 27.78 ± 3.1 | |||||||||
| Yang et al. [36]. 2018 (China) | RC | ≥25 | 213 | 29.5 | A: not mentioned B: M/clinical pregnancy | A: not mentioned B: not mentioned | A: not mentioned B: P/clinical pregnancy | Rot | IVF | GnRH-anta protocol | 7 |
| <25 | 370 | 29.1 | |||||||||
| Chen et al. [39]. 2018 (China) | RC | ≥24 | 138 | 28.9 ± 3.0 | A: GA < 12 weeks B: M/clinical pregnancy | A: not mentioned B: L/all patients | A: not mentioned B: P/live birth | Rot | IVF | GnRH-anta protocol | 7 |
| <24 | 260 | 28.8 ± 2.7 | |||||||||
| Lin et al. [16]. 2019 (China) | RC | ≧30 | 228 | 33.27 ± 3.6 | A: not mentioned B: M/clinical pregnancy | A: alive at GA ≥ 24 weeks B: L/FET cycles | A: <37 weeks B: P/FET cycles | Rot | IVF/ICSI | GnRH-anta protocol; mild stimulation; PPOS (Percentage not mentioned) | 7 |
| ≧25.0, <30 | 480 | 33.09 ± 3.8 | |||||||||
| ≧18.5, <25 | 972 | 32.82 ± 3.4 | |||||||||
| Qiu et al. [18]. 2019 (China) | RC | ≧30 | 204 | 30.05 ± 3.6 | A: <1 st trimester B: M/clinical pregnancy | A: alive at GA ≥24 weeks B: L/FET cycles | Rot | IVF/ICSI with freeze all | GnRH-anta protocol | 6 | |
| ≧25, <30 | 780 | 30.48 ± 3.9 | |||||||||
| ≧18.5, <25 | 1911 | 29.97 ± 3.3 | |||||||||
| <18.5 | 184 | 28.91 ± 3.2 | |||||||||
| Zhou et al. [17]. 2020 (China) | RC | ≧30 | 198 | 27.97 ± 3.0 | A: not mentioned B: M/clinical pregnancy | A: not mentioned B: not mentioned | A: not mentioned B: not mentioned | Rot | IVF/ICSI | Ultra-long protocol | 7 |
| ≧25, <30 | 742 | 28.19 ± 3.1 | |||||||||
| ≧18.5, <25 | 800 | 28.13 ± 3.1 | |||||||||
| <18.5 | 42 | 27.76 ± 2.5 | |||||||||
| Guan et al. [38]. 2021 (China) | RC | ≧28 | 194 | not mentioned | A: not mentioned B: M/clinical pregnancy | A: not mentioned B: L/clinical pregnancy | Rot | OI with IUI | CC (3.9%); LE (18.1%); hMG (11.3%); hMG + CC(17.8%); hMG + LE (48.9%) | 7 | |
| ≧24, <28 | 321 | ||||||||||
| ≧18.5, <24 | 299 | ||||||||||
| <18.5 | 17 | ||||||||||
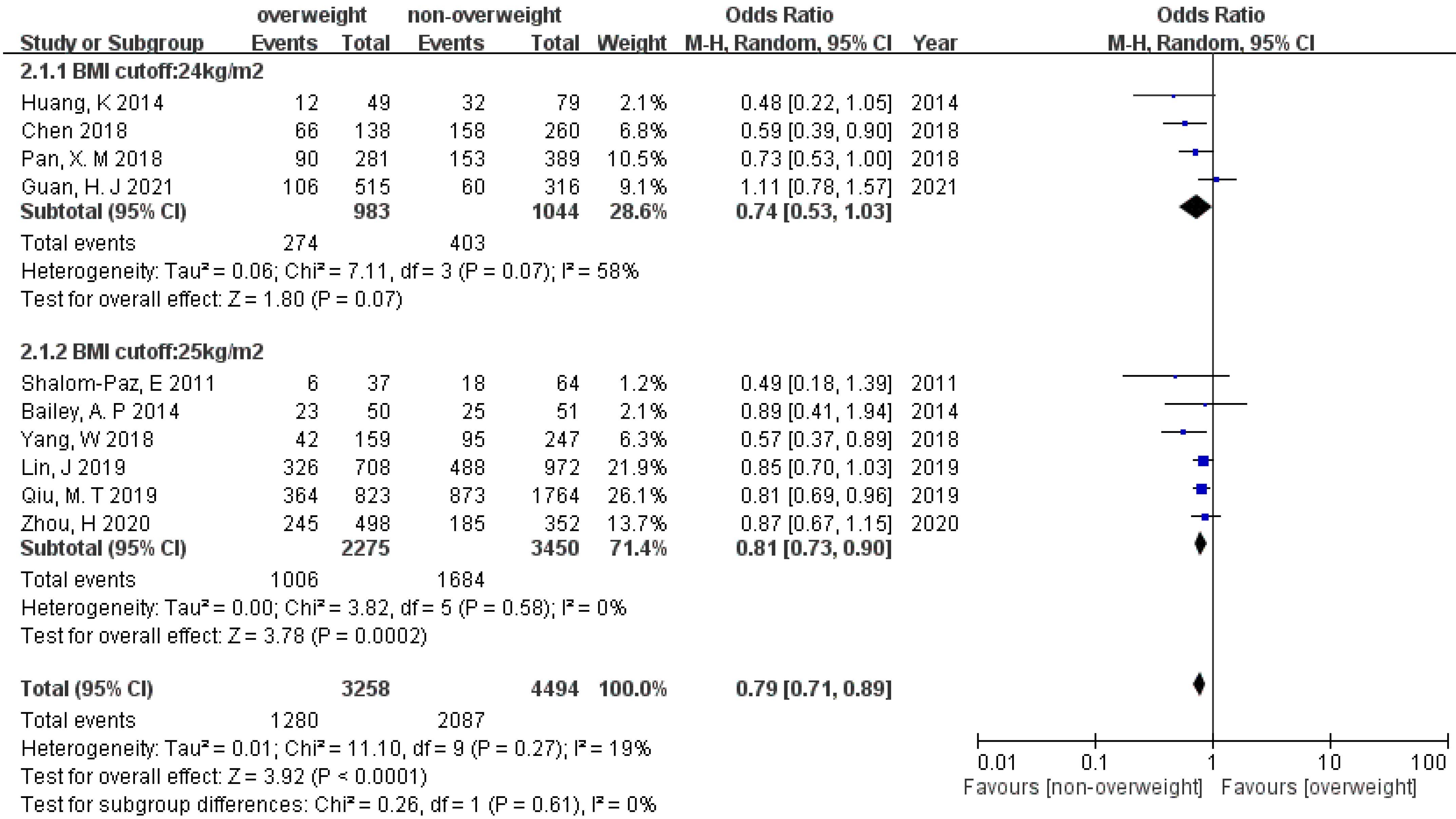
3.3. Miscarriage
3.4. Live Birth
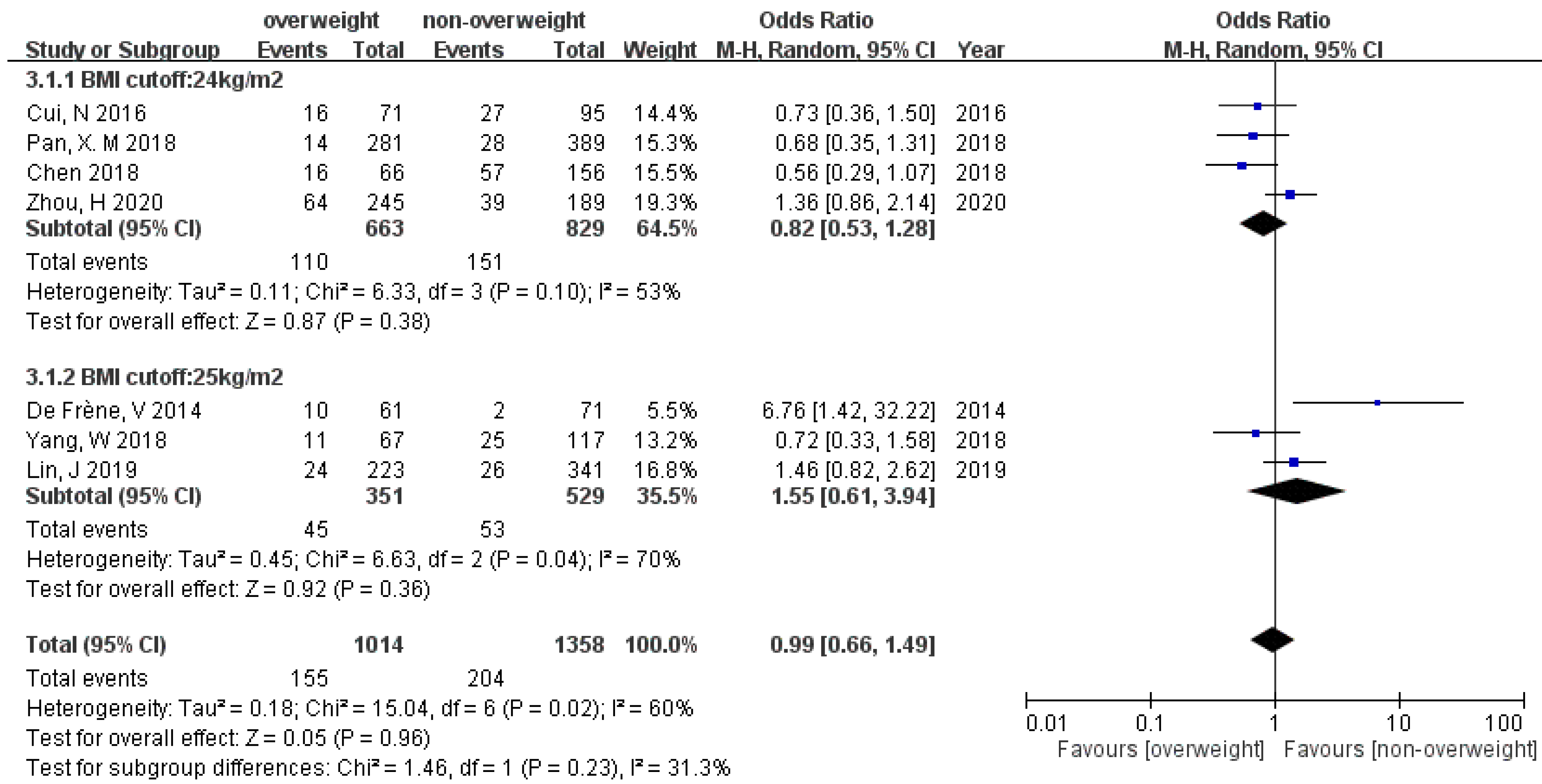
3.5. Preterm Birth (PB)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- McCartney, C.R.; Marshall, J.C. Polycystic Ovary Syndrome. N. Engl. J. Med. 2016, 375, 54–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armanini, D.; Boscaro, M.; Bordin, L.; Sabbadin, C. Controversies in the Pathogenesis, Diagnosis and Treatment of PCOS: Focus on Insulin Resistance, Inflammation, and Hyperandrogenism. Int. J. Mol. Sci. 2022, 23, 4110. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi, H.M.; Adeli, I.; Calina, D.; Docea, A.O.; Mousavi, T.; Daniali, M.; Nikfar, S.; Tsatsakis, A.; Abdollahi, M. Polycystic Ovary Syndrome: A Comprehensive Review of Pathogenesis, Management, and Drug Repurposing. Int. J. Mol. Sci. 2022, 23, 583. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Zheng, B.; Du, S.; Lin, Y. Explore the potential molecular mechanism of polycystic ovarian syndrome by protein-protein interaction network analysis. Taiwan. J. Obstet. Gynecol. 2021, 60, 807–815. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.H.; Sun, K.C.; Wang, P.H. Does the observation of lower ratio of anterior anogenital distance and posterior anogenital distance appear in adolescent and remain constant in women diagnosed with polycystic ovary syndrome? J. Chin. Med. Assoc. 2020, 83, 211–212. [Google Scholar] [CrossRef] [PubMed]
- Dennett, C.C.; Simon, J. The role of polycystic ovary syndrome in reproductive and metabolic health: Overview and approaches for treatment. Diabetes Spectr. 2015, 28, 116–120. [Google Scholar] [CrossRef] [Green Version]
- Seow, K.M.; Chang, Y.W.; Chen, K.H.; Juan, C.C.; Huang, C.Y.; Lin, L.T.; Tsui, K.H.; Chen, Y.J.; Lee, W.L.; Wang, P.H. Molecular Mechanisms of Laparoscopic Ovarian Drilling and Its Therapeutic Effects in Polycystic Ovary Syndrome. Int. J. Mol. Sci. 2020, 21, 8147. [Google Scholar] [CrossRef]
- Yu, H.F.; Chen, H.S.; Rao, D.P.; Gong, J. Association between polycystic ovary syndrome and the risk of pregnancy complications: A PRISMA-compliant systematic review and meta-analysis. Medicine 2016, 95, e4863. [Google Scholar] [CrossRef]
- Toosy, S.; Sodi, R.; Pappachan, J.M. Lean polycystic ovary syndrome (PCOS): An evidence-based practical approach. J. Diabetes Metab. Disord. 2018, 17, 277–285. [Google Scholar] [CrossRef]
- Sebire, N.J.; Jolly, M.; Harris, J.P.; Wadsworth, J.; Joffe, M.; Beard, R.W.; Regan, L.; Robinson, S. Maternal obesity and pregnancy outcome: A study of 287,213 pregnancies in London. Int. J. Obes. Relat. Metab. Disord. 2001, 25, 1175–1182. [Google Scholar] [CrossRef] [Green Version]
- Valent, A.M.; Barbour, L.A. Management of Women with Polycystic Ovary Syndrome during Pregnancy. Endocrinol. Metab. Clin. N. Am. 2021, 50, 57–69. [Google Scholar] [CrossRef] [PubMed]
- Sheng, Y.; Lu, G.; Liu, J.; Liang, X.; Ma, Y.; Zhang, X.; Zhang, S.; Sun, Y.; Sun, Y.; Chen, W.; et al. Effect of body mass index on the outcomes of controlled ovarian hyperstimulation in Chinese women with polycystic ovary syndrome: A multicenter, prospective, observational study. J. Assist. Reprod. Genet. 2017, 34, 61–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shalom-Paz, E.; Marzal, A.; Wiser, A.; Almog, B.; Reinblatt, S.; Tulandi, T.; Holzer, H. Effects of different body mass indices on in vitro maturation in women with polycystic ovaries. Fertil. Steril. 2011, 96, 336–339. [Google Scholar] [CrossRef]
- Pan, X.-M.; Lin, Z.; Li, N.; Wu, J.-Q.; Chen, D.-Q.; Zhu, Y.-M.; Qu, F. Effects of body mass index on the outcomes of in vitro fertilization in Chinese patients with polycystic ovary syndrome: A retrospective cohort study. J. Zhejiang Univ. Sci. B 2018, 19, 490–496. [Google Scholar] [CrossRef]
- McCormick, B.; Thomas, M.; Maxwell, R.; Williams, D.; Aubuchon, M. Effects of polycystic ovarian syndrome on in vitro fertilization-embryo transfer outcomes are influenced by body mass index. Fertil. Steril. 2008, 90, 2304–2309. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Huang, J.; Wang, N.; Kuang, Y.; Cai, R. Effects of pre-pregnancy body mass index on pregnancy and perinatal outcomes in women with PCOS undergoing frozen embryo transfer. BMC Pregnancy Childbirth 2019, 19, 487. [Google Scholar] [CrossRef] [Green Version]
- Zhou, H.; Zhang, D.; Luo, Z.; Yang, A.; Cui, N.; Hao, G.; Wang, W. Association between Body Mass Index and Reproductive Outcome in Women with Polycystic Ovary Syndrome Receiving IVF/ICSI-ET. Biomed. Res. Int. 2020, 2020, 6434080. [Google Scholar] [CrossRef]
- Qiu, M.; Tao, Y.; Kuang, Y.; Wang, Y. Effect of body mass index on pregnancy outcomes with the freeze-all strategy in women with polycystic ovarian syndrome. Fertil. Steril. 2019, 112, 1172–1179. [Google Scholar] [CrossRef]
- Ozgun, M.T.; Uludag, S.; Oner, G.; Batukan, C.; Aygen, E.M.; Sahin, Y. The influence of obesity on ICSI outcomes in women with polycystic ovary syndrome. J. Obstet. Gynaecol. 2011, 31, 245–249. [Google Scholar] [CrossRef]
- Cui, N.; Wang, H.; Wang, W.; Zhang, J.; Xu, Y.; Jiang, L.; Yang, A.; Hao, G. Impact of Body Mass Index on Outcomes of In Vitro Fertilization/Intracytoplasmic Sperm Injection among Polycystic Ovarian Syndrome Patients. Cell. Physiol. Biochem. 2016, 39, 1723–1734. [Google Scholar] [CrossRef]
- Huang, K.; Liao, X.; Dong, X.; Zhang, H. Effect of overweight/obesity on IVF-ET outcomes in chinese patients with polycystic ovary syndrome. Int. J. Clin. Exp. Med. 2014, 7, 5872–5876. [Google Scholar] [PubMed]
- Lee, W.L.; Lee, F.K.; Wang, P.H. Pre-pregnancy body mass index is a determined risk factor for the development of gestational diabetes, regardless of singleton or twin pregnancy. Taiwan. J. Obstet. Gynecol. 2022, 61, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Song, X.; Shu, J.; Zhang, S.; Chen, L.; Diao, J.; Li, J.; Li, Y.; Wei, J.; Liu, Y.; Sun, M.; et al. Pre-Pregnancy Body Mass Index and Risk of Macrosomia and Large for Gestational Age Births with Gestational Diabetes Mellitus as a Mediator: A Prospective Cohort Study in Central China. Nutrients 2022, 14, 1072. [Google Scholar] [CrossRef] [PubMed]
- Kuo, S.C.; Lee, W.L.; Wang, P.H. The effects of maternal body weight and gestational diabetes mellitus on the risk of the delivery of large-for-gestational age babies: Synergistic or additive? Taiwan. J. Obstet. Gynecol. 2022, 61, 413–414. [Google Scholar] [CrossRef] [PubMed]
- Fakhraei, R.; Denize, K.; Simon, A.; Sharif, A.; Zhu-Pawlowsky, J.; Dingwall-Harvey, A.L.J.; Hutton, B.; Pratt, M.; Skidmore, B.; Ahmadzai, N.; et al. Predictors of Adverse Pregnancy Outcomes in Pregnant Women Living with Obesity: A Systematic Review. Int. Environ. Res. Public Health 2022, 19, 2063. [Google Scholar] [CrossRef]
- Chang, W.H.; Lee, W.L.; Wang, P.H. Gestational weight gain and birth weight of newborn. Taiwan. J. Obstet. Gynecol. 2021, 60, 979–980. [Google Scholar] [CrossRef]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Latina, R.; Iacorossi, L.; Fauci, A.J.; Biffi, A.; Castellini, G.; Coclite, D.; D’Angelo, D.; Gianola, S.; Mari, V.; Napoletano, A.; et al. On Behalf of Inih-Major Trauma. Effectiveness of Pre-Hospital Tourniquet in Emergency Patients with Major Trauma and Uncontrolled Haemorrhage: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 12861. [Google Scholar] [CrossRef]
- Magrini, M.; Curzio, O.; Tampucci, M.; Donzelli, G.; Cori, L.; Imiotti, M.C.; Maestro, S.; Moroni, D. Anorexia Nervosa, Body Image Perception and Virtual Reality Therapeutic Applications: State of the Art and Operational Proposal. Int. J. Environ. Res. Public Health 2022, 19, 2533. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alam, M.K.; Alfawzan, A.A.; Shrivastava, D.; Srivastava, K.C.; Alswairki, H.J.; Mussallam, S.; Abutayyem, H.; Ahmed, N. Oral Health Status in Marfan Syndrome: A Systematic Review and Meta-Analysis of 353 Cases. Int. J. Environ. Res. Public Health 2022, 19, 5048. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic; Report of a WHO consultation; World Health Organization: Geneva, Switzerland, 2000; Volume 894, pp. 1–253. [Google Scholar]
- De Frene, V.; Vansteelandt, S.; T’Sjoen, G.; Gerris, J.; Somers, S.; Vercruysse, L.; De Sutter, P. A retrospective study of the pregnancy, delivery and neonatal outcome in overweight versus normal weight women with polycystic ovary syndrome. Hum. Reprod. 2014, 29, 2333–2338. [Google Scholar] [CrossRef] [PubMed]
- Bailey, A.P.; Hawkins, L.K.; Missmer, S.A.; Correia, K.F.; Yanushpolsky, E.H. Effect of body mass index on in vitro fertilization outcomes in women with polycystic ovary syndrome. Am. J. Obstet. Gynecol. 2014, 211, 163.e161–166. [Google Scholar] [CrossRef]
- Yang, W.; Yang, R.; Lin, M.M.; Yang, Y.; Song, X.L.; Zhang, J.J.; Yang, S.; Song, Y.; Li, J.; Pang, T.S.; et al. Body mass index and basal androstenedione are independent risk factors for miscarriage in polycystic ovary syndrome. Reprod. Biol. Endocrinol. 2018, 16, 119. [Google Scholar] [CrossRef]
- Chen, C.M. Overview of obesity in Mainland China. Obes. Rev. 2008, 9 (Suppl. S1), 14–21. [Google Scholar] [CrossRef]
- Guan, H.J.; Pan, L.Q.; Song, H.; Tang, H.Y.; Tang, L.S. Predictors of pregnancy after intrauterine insemination in women with polycystic ovary syndrome. J. Int. Med. Res. 2021, 49, 3000605211018600. [Google Scholar] [CrossRef]
- Chen, R.; Chen, S.; Liu, M.; He, H.; Xu, H.; Liu, H.; Du, H.; Wang, W.; Xia, X.; Liu, J. Pregnancy outcomes of PCOS overweight/obese patients after controlled ovarian stimulation with the GnRH antagonist protocol and frozen embryo transfer. Reprod. Biol. Endocrinol. 2018, 16, 36. [Google Scholar] [CrossRef] [Green Version]
- Hamilton-Fairley, D.; Kiddy, D.; Watson, H.; Paterson, C.; Franks, S. Association of moderate obesity with a poor pregnancy outcome in women with polycystic ovary syndrome treated with low dose gonadotrophin. Br. J. Obstet. Gynaecol. 1992, 99, 128–131. [Google Scholar] [CrossRef]
- Maryam, K.; Bouzari, Z.; Basirat, Z.; Kashifard, M.; Zadeh, M.Z. The comparison of insulin resistance frequency in patients with recurrent early pregnancy loss to normal individuals. BMC Res. Notes 2012, 5, 133. [Google Scholar] [CrossRef] [Green Version]
- Bahri Khomami, M.; Joham, A.E.; Boyle, J.A.; Piltonen, T.; Silagy, M.; Arora, C.; Misso, M.L.; Teede, H.J.; Moran, L.J. Increased maternal pregnancy complications in polycystic ovary syndrome appear to be independent of obesity—A systematic review, meta-analysis, and meta-regression. Obes. Rev. 2019, 20, 659–674. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.F.; Zhang, J.; Xu, Y.M.; Cao, Z.Y.; Wang, Y.Z.; Hao, G.M.; Gao, B.L. High BMI and Insulin Resistance Are Risk Factors for Spontaneous Abortion in Patients with Polycystic Ovary Syndrome Undergoing Assisted Reproductive Treatment: A Systematic Review and Meta-Analysis. Front. Endocrinol. 2020, 11, 592495. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.H.; Lee, I.T.; Ho, L.T.; Sheu, W.H.; Hwu, C.M. Combined Lipid Goal Attainment in Patients with Type 2 Diabetes and Dyslipidemia: A Head-to-Head Comparative Trial of Statins. J. Chin. Med. Assoc. 2022, 85, 832–839. [Google Scholar] [CrossRef]
- Zhang, S.; Sun, D.; Qian, X.; Li, L.; Wu, W. Combined Effects of Obesity and Dyslipidaemia on the Prevalence of Diabetes Amongst Adults Aged ≥45 Years: Evidence from a Nationally Representative Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 8036. [Google Scholar] [CrossRef] [PubMed]
- Chuang, W.C.; Chu, C.H.; Hsu, Y.H.; Yao, C.S. Effect of socioeconomic status on survival in patients on the Diabetes Shared Care Program: Finding from a Taiwan nationwide cohort. J. Chin. Med. Assoc. 2022, 85, 311–316. [Google Scholar] [CrossRef]
- Sheehan, C.M.; Gotlieb, E.E.; Ayers, S.L.; Tong, D.; Oesterle, S.; Vega-López, S.; Wolfersteig, W.; Ruelas, D.M.; Shaibi, G.Q. Neighborhood Conditions and Type 2 Diabetes Risk among Latino Adolescents with Obesity in Phoenix. Int. J. Environ. Res. Public Health 2022, 19, 7920. [Google Scholar] [CrossRef]
- Lo, W.J.; Lin, Y.C.; Chang, H.Y.; Chen, M.J. Risk factors for ocular neovascularization after central retinal artery occlusion. J. Chin. Med. Assoc. 2022, 85, 881–886. [Google Scholar] [CrossRef]
- Zhao, J.; Chen, Q.; Xue, X. An Update on the Progress of Endometrial Receptivity in Women with Polycystic Ovary Syndrome. Reprod. Sci. 2021. [Google Scholar] [CrossRef]
- Bellver, J.; Martinez-Conejero, J.A.; Labarta, E.; Alama, P.; Melo, M.A.; Remohi, J.; Pellicer, A.; Horcajadas, J.A. Endometrial gene expression in the window of implantation is altered in obese women especially in association with polycystic ovary syndrome. Fertil. Steril. 2011, 95, 2335–2341, 2341.e1–2341.e8. [Google Scholar] [CrossRef]
- Oróstica, L.; Astorga, I.; Plaza-Parrochia, F.; Vera, C.; Garcia, V.; Carvajal, R.; Gabler, F.; Romero, C.; Vega, M. Proinflammatory environment and role of TNF-alpha in endometrial function of obese women having polycystic ovarian syndrome. Int. J. Obes. 2016, 40, 1715–1722. [Google Scholar] [CrossRef]
- Xue, Z.; Li, J.; Feng, J.; Han, H.; Zhao, J.; Zhang, J.; Han, Y.; Wu, X.; Zhang, Y. Research Progress on the Mechanism between Polycystic Ovary Syndrome and Abnormal Endometrium. Front. Physiol. 2021, 12, 788772. [Google Scholar] [CrossRef] [PubMed]
- Snider, A.P.; Wood, J.R. Obesity induces ovarian inflammation and reduces oocyte quality. Reproduction 2019, 158, R79–R90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, C.C.; Liao, P.H.; Cheng, Y.H.; Chien, C.Y.; Cheng, K.H.; Chien, C.T. Diabetes associated with hypertension exacerbated oxidative stress-mediated inflammation, apoptosis and autophagy leading to erectile dysfunction in rats. J. Chin. Med. Assoc. 2022, 85, 346–357. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; He, Y.; Wu, Y.; Zhang, D.; Huang, H. Association between abnormal body mass index and pregnancy outcomes in patients following frozen embryo transfer: A systematic review and meta-analysis. Reprod. Biol. Endocrinol. 2021, 19, 140. [Google Scholar] [CrossRef]
- Jiang, X.; Liu, R.; Liao, T.; He, Y.; Li, C.; Guo, P.; Zhou, P.; Cao, Y.; Wei, Z. A Predictive Model of Live Birth Based on Obesity and Metabolic Parameters in Patients with PCOS Undergoing Frozen-Thawed Embryo Transfer. Front. Endocrinol. 2021, 12, 799871. [Google Scholar] [CrossRef]
- Bednarz, K.; Kowalczyk, K.; Cwynar, M.; Czapla, D.; Czarkowski, W.; Kmita, D.; Nowak, A.; Madej, P. The Role of Glp-1 Receptor Agonists in Insulin Resistance with Concomitant Obesity Treatment in Polycystic Ovary Syndrome. Int. J. Mol. Sci. 2022, 23, 4334. [Google Scholar] [CrossRef]
- Liu, T.; Liu, D.; Song, X.; Qu, J.; Zheng, X.; Li, J.; Yang, R.; Yang, S.; Zhang, X.; Wang, H.; et al. Lipid Metabolism Was Associated with Oocyte in vitro Maturation in Women with Polycystic Ovarian Syndrome Undergoing Unstimulated Natural Cycle. Front. Cell. Dev. Biol. 2021, 9, 719173. [Google Scholar] [CrossRef]
- Santos, S.; Voerman, E.; Amiano, P.; Barros, H.; Beilin, L.J.; Bergstrom, A.; Charles, M.A.; Chatzi, L.; Chevrier, C.; Chrousos, G.P.; et al. Impact of maternal body mass index and gestational weight gain on pregnancy complications: An individual participant data meta-analysis of European, North American and Australian cohorts. BJOG 2019, 126, 984–995. [Google Scholar] [CrossRef]
- Rahman, M.M.; Abe, S.K.; Kanda, M.; Narita, S.; Rahman, M.S.; Bilano, V.; Ota, E.; Gilmour, S.; Shibuya, K. Maternal body mass index and risk of birth and maternal health outcomes in low- and middle-income countries: A systematic review and meta-analysis. Obes. Rev. 2015, 16, 758–770. [Google Scholar] [CrossRef]
- Bahri Khomami, M.; Joham, A.E.; Boyle, J.A.; Piltonen, T.; Arora, C.; Silagy, M.; Misso, M.L.; Teede, H.J.; Moran, L.J. The role of maternal obesity in infant outcomes in polycystic ovary syndrome-A systematic review, meta-analysis, and meta-regression. Obes. Rev. 2019, 20, 842–858. [Google Scholar] [CrossRef]
- Wang, R.; Mol, B.W. The Rotterdam criteria for polycystic ovary syndrome: Evidence-based criteria? Hum. Reprod. 2017, 32, 261–264. [Google Scholar] [CrossRef] [PubMed]
- Teede, H.J.; Misso, M.L.; Costello, M.F.; Dokras, A.; Laven, J.; Moran, L.; Piltonen, T.; Norman, R.J.; International PCOS Network. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Fertil. Steril. 2018, 110, 364–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Wu, L.; Li, T.C.; Wang, C.C.; Zhang, T.; Chung, J.P.W. Systematic review update and meta-analysis of randomized and non-randomized controlled trials of ovarian stimulation versus artificial cycle for endometrial preparation prior to frozen embryo transfer in women with polycystic ovary syndrome. Reprod. Biol. Endocrinol. 2022, 20, 62. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.H.; Li, Y.H.; Wang, Y.Y.; Chang, W.D. Higher Neutrophil-To-Lymphocyte Ratio Was Associated with Increased Risk of Chronic Kidney Disease in Overweight/Obese but Not Normal-Weight Individuals. Int. J. Environ. Res. Public Health 2022, 19, 8077. [Google Scholar] [CrossRef]
- Hung, K.Y.; Chen, S.T.; Chu, Y.Y.; Ho, G.; Liu, W.L. Nutrition support for acute kidney injury 2020-consensus of the Taiwan AKI task force. J. Chin. Med. Assoc. 2022, 85, 252–258. [Google Scholar] [CrossRef]
- Cooke, M.B.; Deasy, W.; Ritenis, E.J.; Wilson, R.A.; Stathis, C.G. Effects of Intermittent Energy Restriction Alone and in Combination with Sprint Interval Training on Body Composition and Cardiometabolic Biomarkers in Individuals with Overweight and Obesity. Int. J. Environ. Res. Public Health 2022, 19, 7969. [Google Scholar] [CrossRef]
- Abdul Basir, S.M.; Abdul Manaf, Z.; Mohd Noor, N.; Mat Ludin, A.F.; Shahar, S.; Abdul Manaf, M.R. The Challenges and Strategies towards Healthy Eating during COVID-19 Home Confinement Period among Working Adults with BMI ≥ 25 kg/m2 Enrolled in a Weight Loss Program: Qualitative Findings. Int. J. Environ. Res. Public Health 2022, 19, 6656. [Google Scholar] [CrossRef]
- Lin, B.Z.; Lin, T.J.; Lin, C.L.; Liao, L.Y.; Chang, T.A.; Lu, B.J.; Chen, K.Y. Differentiation of clinical patterns and survival outcomes of hepatocellular carcinoma on hepatitis B and nonalcoholic fatty liver disease. J. Chin. Med. Assoc. 2021, 84, 606–613. [Google Scholar] [CrossRef]
- Chen, C.T.; Lin, M.C.; Lee, Y.J.; Li, L.H.; Chen, Y.J.; Chuanyi Hou, P.; How, C.K. Association between body mass index and clinical outcomes in out-of-hospital cardiac arrest survivors treated with targeted temperature management. J. Chin. Med. Assoc. 2021, 84, 504–509. [Google Scholar] [CrossRef]
- Ellahi, B.; Aitken, A.; Dikmen, D.; Seyhan-Erdoğan, B.; Makda, M.; Razaq, R. Acceptability, Usability and Weight Loss Outcomes in a Randomized Cross-Over Study of Commercially Available Portion Size Tools in an Overweight South Asian Community. Int. J. Environ. Res. Public Health 2022, 19, 7714. [Google Scholar] [CrossRef]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, S.-T.; Liu, C.-H.; Ma, S.-H.; Chang, W.-H.; Chen, Y.-J.; Lee, W.-L.; Wang, P.-H. Association between Pre-Pregnancy Overweightness/Obesity and Pregnancy Outcomes in Women with Polycystic Ovary Syndrome: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 9094. https://doi.org/10.3390/ijerph19159094
Yang S-T, Liu C-H, Ma S-H, Chang W-H, Chen Y-J, Lee W-L, Wang P-H. Association between Pre-Pregnancy Overweightness/Obesity and Pregnancy Outcomes in Women with Polycystic Ovary Syndrome: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2022; 19(15):9094. https://doi.org/10.3390/ijerph19159094
Chicago/Turabian StyleYang, Szu-Ting, Chia-Hao Liu, Sheng-Hsiang Ma, Wen-Hsun Chang, Yi-Jen Chen, Wen-Ling Lee, and Peng-Hui Wang. 2022. "Association between Pre-Pregnancy Overweightness/Obesity and Pregnancy Outcomes in Women with Polycystic Ovary Syndrome: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 19, no. 15: 9094. https://doi.org/10.3390/ijerph19159094