
Systematic Review of COVID-19-Related Physical Activity-Based Rehabilitations: Benefits to Be Confirmed by More Robust Methodological Approaches

 , , , , ,
, , , , ,  , and
, and {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Material & Methods
2.1. Literature Search Strategy and Study Eligibility
2.2. General Inclusion Criteria
2.3. General Exclusion Criteria
2.4. Inclusion and Exclusion Criteria Specific to the Programs of PA
2.5. Data Extraction and Synthesis
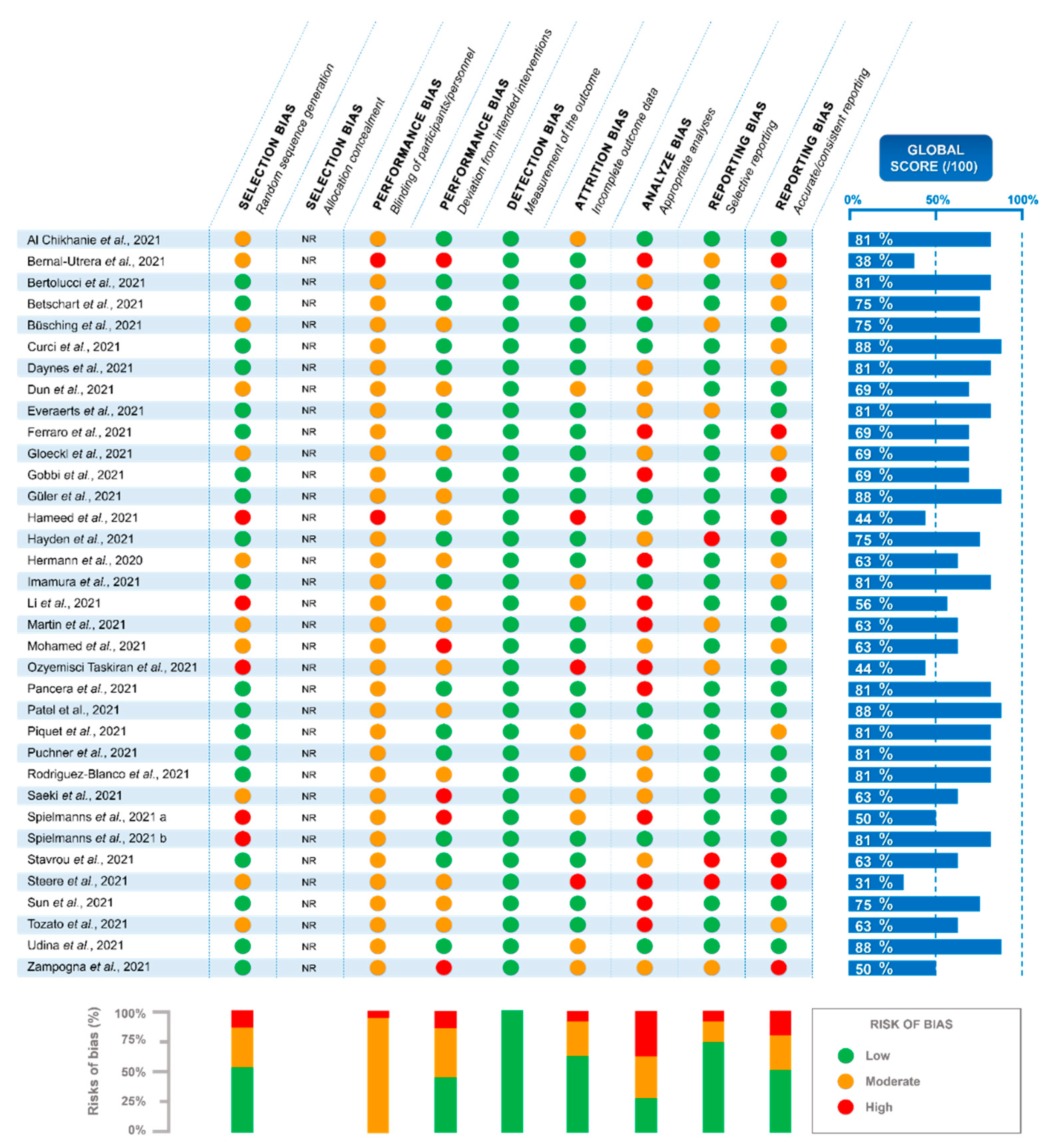
2.6. Criteria for Risks of Bias Assessment
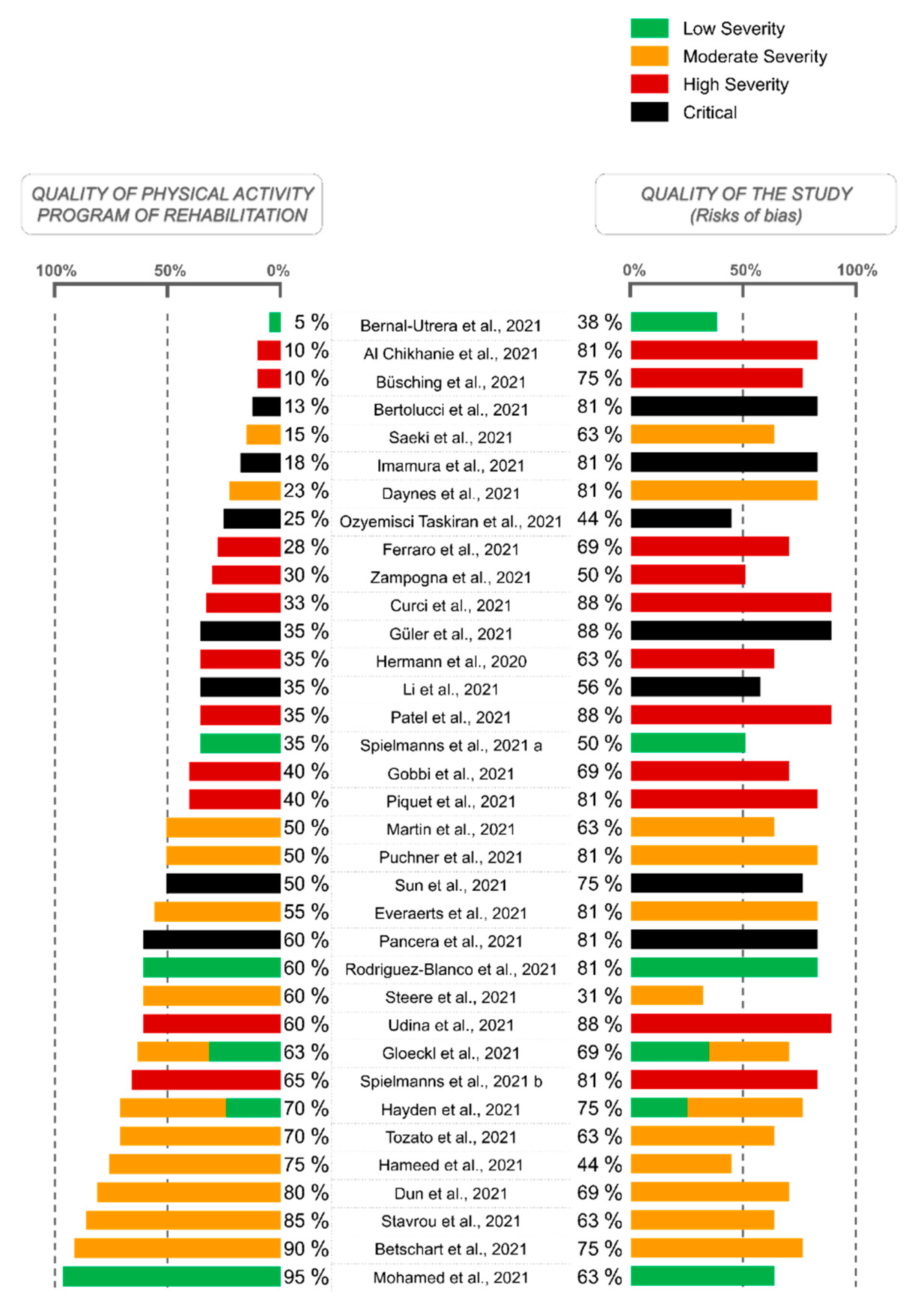
2.7. PA Program Scoring to Assess the Quality of the Description
2.8. Estimation of COVID-19 Severity at the Beginning of Rehabilitation
3. Results
3.1. Selection Process and Risks of Bias
3.2. Experimental Design and Constitutions of Groups
3.3. Characteristics and Severity of the Disease among COV+ Populations Performing the Rehabilitation
3.4. Rehabilitation Interventions
3.5. PA Programs
3.6. Parameters Assessed and Methods Used
3.7. Effects of the RP
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard—25 February 2022 n.d. Available online: https://covid19.who.int (accessed on 28 February 2022).
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Kamal, M.; Abo Omirah, M.; Hussein, A.; Saeed, H. Assessment and characterisation of post-COVID-19 manifestations. Int. J. Clin. Pract. 2021, 75, e13746. [Google Scholar] [CrossRef] [PubMed]
- Garrigues, E.; Janvier, P.; Kherabi, Y.; Le Bot, A.; Hamon, A.; Gouze, H.; Doucet, L.; Berkani, S.; Oliosi, E.; Mallart, E.; et al. Post-discharge persistent symptoms and health-related quality of life after hospitalization for COVID-19. J. Infect. 2020, 81, e4–e6. [Google Scholar] [CrossRef] [PubMed]
- Ried-Larsen, M.; Aarts, H.M.; Joyner, M.J. Effects of strict prolonged bed rest on cardiorespiratory fitness: Systematic review and meta-analysis. J. Appl. Physiol. 2017, 123, 790–799. [Google Scholar] [CrossRef]
- Fernandes, A.; Jaeger, M.S.; Chudow, M. Post-intensive care syndrome: A review of preventive strategies and follow-up care. Am. J. Health-Syst. Pharm. AJHP 2019, 76, 119–122. [Google Scholar] [CrossRef]
- Kashif, A.; Chaudhry, M.; Fayyaz, T.; Abdullah, M.; Malik, A.; Anwer, J.M.A.; Inam, S.H.A.; Fatima, T.; Iqbal, N.; Shoaib, K. Follow-up of COVID-19 recovered patients with mild disease. Sci. Rep. 2021, 11, 13414. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Knight, M.; A’Court, C.; Buxton, M.; Husain, L. Management of post-acute COVID-19 in primary care. BMJ 2020, 370, m3026. [Google Scholar] [CrossRef]
- Raveendran, A.V.; Jayadevan, R.; Sashidharan, S. Long COVID: An overview. Diabetes Metab. Syndr. 2021, 15, 869–875. [Google Scholar] [CrossRef]
- Frota, A.X.; Vieira, M.C.; Soares, C.C.S.; Silva, P.S.D.; Silva, G.M.S.D.; Mendes, F.D.S.N.S.; Mazzoli-Rocha, F.; Veloso, H.H.; Costa, A.D.D.; Lamas, C.D.C.; et al. Functional capacity and rehabilitation strategies in COVID-19 patients: Current knowledge and challenges. Rev. Soc. Bras. Med. Trop. 2021, 54, e07892020. [Google Scholar] [CrossRef]
- Wade, D.T. Rehabilitation after COVID-19: An evidence-based approach. Clin. Med. J. 2020, 20, 359–365. [Google Scholar] [CrossRef]
- Liebl, M.E.; Gutenbrunner, C.; Glaesener, J.J.; Schwarzkopf, S.; Best, N.; Lichti, G.; Kraft, E.; Krischak, G.; Reisshauer, A. Early Rehabilitation in COVID-19—Best Practice Recommendations for the Early Rehabilitation of COVID-19 Patients. Phys. Med. Rehabil. Kurortmed. 2020, 30, 129–134. [Google Scholar] [CrossRef]
- Antonelli, M.; Donelli, D. Respiratory rehabilitation for post-COVID19 patients in spa centers: First steps from theory to practice. Int. J. Biometeorol. 2020, 64, 1811–1813. [Google Scholar] [CrossRef] [PubMed]
- Sun, T.; Guo, L.; Tian, F.; Dai, T.; Xing, X.; Zhao, J.; Li, Q. Rehabilitation of patients with COVID-19. Expert Rev. Respir. Med. 2020, 14, 1249–1256. [Google Scholar] [CrossRef] [PubMed]
- Soares, M.N.; Eggelbusch, M.; Naddaf, E.; Gerrits, K.H.; van der Schaaf, M.; van den Borst, B.; Wiersinga, W.J.; van Vugt, M.; Weijs, P.J.; Murray, A.J.; et al. Skeletal muscle alterations in patients with acute COVID-19 and post-acute sequelae of COVID-19. J. Cachexia Sarcopenia Muscle 2022, 13, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Rebello, C.J.; Axelrod, C.L.; Reynolds, C.F.; Greenway, F.L.; Kirwan, J.P. Exercise as a Moderator of Persistent Neuroendocrine Symptoms of COVID-19. Exerc. Sport Sci. Rev. 2022, 50, 65–72. [Google Scholar] [CrossRef]
- Filgueira, T.O.; Castoldi, A.; Santos, L.E.R.; de Amorim, G.J.; de Sousa Fernandes, M.S.; Anastácio, W.D.L.D.N.; Campos, E.Z.; Santos, T.M.; Souto, F.O. The Relevance of a Physical Active Lifestyle and Physical Fitness on Immune Defense: Mitigating Disease Burden, With Focus on COVID-19 Consequences. Front. Immunol. 2021, 12, 587146. [Google Scholar] [CrossRef]
- Sallis, R.; Young, D.R.; Tartof, S.Y.; Sallis, J.F.; Sall, J.; Li, Q.; Smith, G.N.; Cohen, D.A. Physical inactivity is associated with a higher risk for severe COVID-19 outcomes: A study in 48 440 adult patients. Br. J. Sports Med. 2021, 55, 1099–1105. [Google Scholar] [CrossRef]
- Gil, S.; Jacob Filho, W.; Shinjo, S.K.; Ferriolli, E.; Busse, A.L.; Avelino-Silva, T.J.; Longobardi, I.; de Oliveira Júnior, G.N.; Swinton, P.; Gualano, B.; et al. Muscle strength and muscle mass as predictors of hospital length of stay in patients with moderate to severe COVID-19: A prospective observational study. J. Cachexia Sarcopenia Muscle 2021, 12, 1871–1878. [Google Scholar] [CrossRef]
- Baker, F.L.; Smith, K.A.; Zúñiga, T.M.; Batatinha, H.; Niemiro, G.M.; Pedlar, C.R.; Burgess, S.C.; Katsanis, E.; Simpson, R.J. Acute exercise increases immune responses to SARS-CoV-2 in a previously infected man. Brain Behav. Immun. Health 2021, 18, 100343. [Google Scholar] [CrossRef]
- Curci, C.; Pisano, F.; Bonacci, E.; Camozzi, D.M.; Ceravolo, C.; Bergonzi, R.; De Franceschi, S.; Moro, P.; Guarnieri, R.; Ferrillo, M.; et al. Early rehabilitation in post-acute COVID-19 patients: Data from an Italian COVID-19 Rehabilitation Unit and proposal of a treatment protocol. Eur. J. Phys. Rehabil. Med. 2020, 56, 633–641. [Google Scholar] [CrossRef]
- Pastora-Bernal, J.-M.; Estebanez-Pérez, M.-J.; Molina-Torres, G.; García-López, F.-J.; Sobrino-Sánchez, R.; Martín-Valero, R. Telerehabilitation Intervention in Patients with COVID-19 after Hospital Discharge to Improve Functional Capacity and Quality of Life. Study Protocol for a Multicenter Randomized Clinical Trial. Int. J. Environ. Res. Public Health 2021, 18, 2924. [Google Scholar] [CrossRef] [PubMed]
- Trapé, Á.A.; Camacho-Cardenosa, M.; Camacho-Cardenosa, A.; Merellano-Navarro, E.; Rodrigues, J.A.L.; da Silva Lizzi, E.A.; Sorgi, C.A.; Papoti, M.; Brazo-Sayavera, J. Effects of moderate-intensity intermittent hypoxic training on health outcomes of patients recovered from COVID-19: The AEROBICOVID study protocol for a randomized controlled trial. Trials 2021, 22, 534. [Google Scholar] [CrossRef]
- Li, Z.; Zheng, C.; Duan, C.; Zhang, Y.; Li, Q.; Dou, Z.; Li, J.; Xia, W. Rehabilitation needs of the first cohort of post-acute COVID-19 patients in Hubei, China. Eur. J. Phys. Rehabil. Med. 2020, 56, 339–344. [Google Scholar] [CrossRef]
- Belli, S.; Balbi, B.; Prince, I.; Cattaneo, D.; Masocco, F.; Zaccaria, S.; Bertalli, L.; Cattini, F.; Lomazzo, A.; Dal Negro, F.; et al. Low physical functioning and impaired performance of activities of daily life in COVID-19 patients who survived hospitalisation. Eur. Respir. J. 2020, 56, 2002096. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, A.A.; Alawna, M. Role of increasing the aerobic capacity on improving the function of immune and respiratory systems in patients with coronavirus (COVID-19): A review. Diabetes Metab. Syndr. 2020, 14, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Felten-Barentsz, K.M.; van Oorsouw, R.; Klooster, E.; Koenders, N.; Driehuis, F.; Hulzebos, E.H.; van der Schaaf, M.; Hoogeboom, T.J.; van der Wees, P.J. Recommendations for Hospital-Based Physical Therapists Managing Patients with COVID-19. Phys. Ther. 2020, 100, 1444–1457. [Google Scholar] [CrossRef]
- Wang, T.J.; Chau, B.; Lui, M.; Lam, G.-T.; Lin, N.; Humbert, S. PM&R and Pulmonary Rehabilitation for COVID-19. Am. J. Phys. Med. Rehabil. 2020, 99, 769–774. [Google Scholar] [CrossRef]
- Hekmatikar, A.H.A.; Shamsi, M.M.; Ashkazari, Z.S.Z.; Suzuki, K. Exercise in an Overweight Patient with COVID-19: A Case Study. Int. J. Environ. Res. Public Health 2021, 18, 5882. [Google Scholar] [CrossRef]
- Mayer, K.P.; Steele, A.K.; Soper, M.K.; Branton, J.D.; Lusby, M.L.; Kalema, A.G.; Dupont-Versteegden, E.E.; Montgomery-Yates, A.A. Physical Therapy Management of an Individual With Post-COVID Syndrome: A Case Report. Phys. Ther. 2021, 101, pzab098. [Google Scholar] [CrossRef]
- Serviente, C.; Decker, S.T.; Layec, G. From heart to muscle: Pathophysiological mechanisms underlying long-term physical sequelae from SARS-CoV-2 infection. J. Appl. Physiol. 2022, 132, 581–592. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Physical Activity. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 7 July 2022).
- Higgins, J.P.T.; Savović, J.; Page, M.J.; Elbers, R.G.; Sterne, J.A. Chapter 8: Assessing Risk of Bias in A Randomized Trial. In Cochrane Handbook for Systematic Reviews of Interventions Version 62; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: Hoboken, NJ, USA, 2021; Available online: www.training.cochrane.org/handbook (accessed on 19 January 2022).
- Al Chikhanie, Y.; Veale, D.; Schoeffler, M.; Pépin, J.L.; Verges, S.; Hérengt, F. Effectiveness of pulmonary rehabilitation in COVID-19 respiratory failure patients post-ICU. Respir. Physiol. Neurobiol. 2021, 287, 103639. [Google Scholar] [CrossRef] [PubMed]
- Bernal-Utrera, C.; Anarte-Lazo, E.; De-La-Barrera-Aranda, E.; Fernandez-Bueno, L.; Saavedra-Hernandez, M.; Gonzalez-Gerez, J.J.; Serrera-Figallo, M.A.; Rodriguez-Blanco, C. Perspectives and Attitudes of Patients with COVID-19 toward a Telerehabilitation Programme: A Qualitative Study. Int. J. Environ. Res. Public Health 2021, 18, 7845. [Google Scholar] [CrossRef] [PubMed]
- Bertolucci, F.; Sagliocco, L.; Tolaini, M.; Posteraro, F. Comprehensive rehabilitation treatment for sub-acute COVID-19 patients: An observational study. Eur. J. Phys. Rehabil. Med. 2021, 57, 208–215. [Google Scholar] [CrossRef]
- Betschart, M.; Rezek, S.; Unger, I.; Beyer, S.; Gisi, D.; Shannon, H.; Sieber, C. Feasibility of an Outpatient Training Program after COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 3978. [Google Scholar] [CrossRef]
- Büsching, G.; Zhang, Z.; Schmid, J.-P.; Sigrist, T.; Khatami, R. Effectiveness of Pulmonary Rehabilitation in Severe and Critically Ill COVID-19 Patients: A Controlled Study. Int. J. Environ. Res. Public Health 2021, 18, 8956. [Google Scholar] [CrossRef]
- Curci, C.; Negrini, F.; Ferrillo, M.; Bergonzi, R.; Bonacci, E.; Camozzi, D.M.; Ceravolo, C.; De Franceschi, S.; Guarnieri, R.; Moro, P.; et al. Functional outcome after inpatient rehabilitation in postintensive care unit COVID-19 patients: Findings and clinical implications from a real-practice retrospective study. Eur. J. Phys. Rehabil. Med. 2021, 57, 443–450. [Google Scholar] [CrossRef]
- Daynes, E.; Gerlis, C.; Chaplin, E.; Gardiner, N.; Singh, S.J. Early experiences of rehabilitation for individuals post-COVID to improve fatigue, breathlessness exercise capacity and cognition—A cohort study. Chron. Respir. Dis. 2021, 18, 14799731211015692. [Google Scholar] [CrossRef]
- Dun, Y.; Liu, C.; Ripley-Gonzalez, J.W.; Liu, P.; Zhou, N.; Gong, X.; You, B.; Du, Y.; Liu, J.; Li, B.; et al. Six-month outcomes and effect of pulmonary rehabilitation among patients hospitalized with COVID-19: A retrospective cohort study. Ann. Med. 2021, 53, 2099–2109. [Google Scholar] [CrossRef]
- Everaerts, S.; Heyns, A.; Langer, D.; Beyens, H.; Hermans, G.; Troosters, T.; Gosselink, R.; Lorent, N.; Janssens, W. COVID-19 recovery: Benefits of multidisciplinary respiratory rehabilitation. BMJ Open Respir. Res. 2021, 8, e000837. [Google Scholar] [CrossRef]
- Ferraro, F.; Calafiore, D.; Dambruoso, F.; Guidarini, S.; de Sire, A. COVID-19 related fatigue: Which role for rehabilitation in post-COVID-19 patients? A case series. J. Med. Virol. 2021, 93, 1896–1899. [Google Scholar] [CrossRef] [PubMed]
- Gloeckl, R.; Leitl, D.; Jarosch, I.; Schneeberger, T.; Nell, C.; Stenzel, N.; Vogelmeier, C.F.; Kenn, K.; Koczulla, A.R. Benefits of pulmonary rehabilitation in COVID-19: A prospective observational cohort study. ERJ Open Res. 2021, 7, 00108–02021. [Google Scholar] [CrossRef] [PubMed]
- Gobbi, M.; Bezzoli, E.; Ismelli, F.; Trotti, G.; Cortellezzi, S.; Meneguzzo, F.; Arreghini, M.; Seitanidis, I.; Brunani, A.; Aspesi, V.; et al. Skeletal Muscle Mass, Sarcopenia and Rehabilitation Outcomes in Post-Acute COVID-19 Patients. J. Clin. Med. 2021, 10, 5623. [Google Scholar] [CrossRef] [PubMed]
- Güler, T.; Yurdakul, F.G.; Acar Sivas, F.; Kiliç, Z.; Adigüzel, E.; Yaşar, E.; Bodur, H. Rehabilitative management of post-acute COVID-19: Clinical pictures and outcomes. Rheumatol. Int. 2021, 41, 2167–2175. [Google Scholar] [CrossRef]
- Hameed, F.; Palatulan, E.; Jaywant, A.; Said, R.; Lau, C.; Sood, V.; Layton, A.; Gellhorn, A. Outcomes of a COVID-19 recovery program for patients hospitalized with SARS-CoV-2 infection in New York City: A prospective cohort study. PMR 2021, 13, 609–617. [Google Scholar] [CrossRef]
- Hayden, M.C.; Limbach, M.; Schuler, M.; Merkl, S.; Schwarzl, G.; Jakab, K.; Nowak, D.; Schultz, K. Effectiveness of a Three-Week Inpatient Pulmonary Rehabilitation Program for Patients after COVID-19: A Prospective Observational Study. Int. J. Environ. Res. Public Health 2021, 18, 9001. [Google Scholar] [CrossRef]
- Hermann, M.; Pekacka-Egli, A.M.; Witassek, F.; Baumgaertner, R.; Schoendorf, S.; Spielmanns, M. Feasibility and Efficacy of Cardiopulmonary Rehabilitation After COVID-19. Am. J. Phys. Med. Rehabil. 2020, 99, 865–869. [Google Scholar] [CrossRef]
- Imamura, M.; Mirisola, A.R.; Ribeiro, F.D.Q.; De Pretto, L.R.; Alfieri, F.M.; Delgado, V.R.; Battistella, L.R. Rehabilitation of patients after COVID-19 recovery: An experience at the Physical and Rehabilitation Medicine Institute and Lucy Montoro Rehabilitation Institute. Clinics 2021, 76, e2804. [Google Scholar] [CrossRef]
- Li, L.; Yu, P.; Yang, M.; Xie, W.; Huang, L.; He, C.; Gosselink, R.; Wei, Q.; Jones, A.Y. Physical Therapist Management of COVID-19 in the Intensive Care Unit: The West China Hospital Experience. Phys. Ther. 2021, 101, pzaa198. [Google Scholar] [CrossRef]
- Martin, I.; Braem, F.; Baudet, L.; Poncin, W.; Fizaine, S.; Aboubakar, F.; Froidure, A.; Pilette, C.; Liistro, G.; De Greef, J.; et al. Follow-up of functional exercise capacity in patients with COVID-19: It is improved by telerehabilitation. Respir. Med. 2021, 183, 106438. [Google Scholar] [CrossRef]
- Mohamed, A.A.; Alawna, M. The effect of aerobic exercise on immune biomarkers and symptoms severity and progression in patients with COVID-19: A randomized control trial. J. Bodyw. Mov. Ther. 2021, 28, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Ozyemisci Taskiran, O.; Turan, Z.; Tekin, S.; Senturk, E.; Topaloglu, M.; Yurdakul, F.; Ergonul, O.; Cakar, N. Physical rehabilitation in Intensive Care Unit in acute respiratory distress syndrome patients with COVID-19. Eur. J. Phys. Rehabil. Med. 2021, 57, 434–442. [Google Scholar] [CrossRef] [PubMed]
- Pancera, S.; Bianchi, L.N.; Porta, R.; Galeri, S.; Carrozza, M.C.; Villafañe, J.H. Feasibility of subacute rehabilitation for mechanically ventilated patients with COVID-19 disease: A retrospective case series. Int. J. Rehabil. Res. Int. Z. Rehabil. Rev. Int. Rech. Readapt. 2021, 44, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.; Steinberg, C.; Patel, R.; Chomali, C.; Doulatani, G.; Lindsay, L.; Jaywant, A. Description and Functional Outcomes of a Novel Interdisciplinary Rehabilitation Program for Hospitalized Patients With COVID-19. Am. J. Phys. Med. Rehabil. 2021, 100, 1124–1132. [Google Scholar] [CrossRef]
- Piquet, V.; Luczak, C.; Seiler, F.; Monaury, J.; Martini, A.; Ward, A.B.; Gracies, J.M.; Motavasseli, D.; Lépine, E.; Chambard, L.; et al. Do Patients With COVID-19 Benefit from Rehabilitation? Functional Outcomes of the First 100 Patients in a COVID-19 Rehabilitation Unit. Arch. Phys. Med. Rehabil. 2021, 102, 1067–1074. [Google Scholar] [CrossRef]
- Puchner, B.; Sahanic, S.; Kirchmair, R.; Pizzini, A.; Sonnweber, B.; Wöll, E.; Mühlbacher, A.; Garimorth, K.; Dareb, B.; Ehling, R.; et al. Beneficial effects of multi-disciplinary rehabilitation in postacute COVID-19: An observational cohort study. Eur. J. Phys. Rehabil. Med. 2021, 57, 189–198. [Google Scholar] [CrossRef]
- Rodriguez-Blanco, C.; Gonzalez-Gerez, J.J.; Bernal-Utrera, C.; Anarte-Lazo, E.; Perez-Ale, M.; Saavedra-Hernandez, M. Short-Term Effects of a Conditioning Telerehabilitation Program in Confined Patients Affected by COVID-19 in the Acute Phase. A Pilot Randomized Controlled Trial. Medicina 2021, 57, 684. [Google Scholar] [CrossRef]
- Saeki, T.; Ogawa, F.; Matsumiya, M.; Yamamura, M.; Oritsu, H.; Nonogaki, M.; Uesugi, J.; Takeuchi, I.; Nakamura, T. Long-Term Decreased Exercise Capacity of COVID-19 Patients Who Received Mechanical Ventilation in Japan: A Case Series. Am. J. Phys. Med. Rehabil. 2021, 100, 737–741. [Google Scholar] [CrossRef]
- Spielmanns, M.; Pekacka-Egli, A.M.; Cecon, M.; Witassek, F.; Schoendorf, S.; Lutz, D.; Hermann, M. COVID-19 Outbreak During Inpatient Rehabilitation: Impact on Settings and Clinical Course of Neuromusculoskeletal Rehabilitation Patients. Am. J. Phys. Med. Rehabil. 2021, 100, 203–208. [Google Scholar] [CrossRef]
- Spielmanns, M.; Pekacka-Egli, A.M.; Schoendorf, S.; Windisch, W.; Hermann, M. Effects of a Comprehensive Pulmonary Rehabilitation in Severe Post-COVID-19 Patients. Int. J. Environ. Res. Public Health 2021, 18, 2695. [Google Scholar] [CrossRef]
- Stavrou, V.T.; Tourlakopoulos, K.N.; Vavougios, G.D.; Papayianni, E.; Kiribesi, K.; Maggoutas, S.; Nikolaidis, K.; Fradelos, E.C.; Dimeas, I.; Daniil, Z.; et al. Eight Weeks Unsupervised Pulmonary Rehabilitation in Previously Hospitalized of SARS-CoV-2 Infection. J. Pers. Med. 2021, 11, 806. [Google Scholar] [CrossRef] [PubMed]
- Steere, H.K.; Polich, G.; Silver, J.K.; Hameed, F.; Gellhorn, A.C.; Borg-Stein, J.; Schneider, J.C. Ambulatory Rehabilitation of Patients Hospitalized with SARS-CoV-2 Infections: Early Pandemic Experience in New York City and Boston. PMR 2021, 13, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Liu, J.; Li, H.; Shang, C.; Li, T.; Ji, W.; Wu, J.; Han, X.; Shi, Z. Pulmonary rehabilitation focusing on the regulation of respiratory movement can improve prognosis of severe patients with COVID-19. Ann. Palliat. Med. 2021, 10, 4262–4272. [Google Scholar] [CrossRef]
- Tozato, C.; Ferreira, B.F.C.; Dalavina, J.P.; Molinari, C.V.; Alves, V.L.D.S. Cardiopulmonary rehabilitation in post-COVID-19 patients: Case series. Rev. Bras. Ter. Intensiv. 2021, 33, 167–171. [Google Scholar] [CrossRef] [PubMed]
- Udina, C.; Ars, J.; Morandi, A.; Vilaró, J.; Cáceres, C.; Inzitari, M. Rehabilitation in adult post-COVID-19 patients in post-acute care with Therapeutic Exercise. J. Frailty Aging 2021, 10, 297–300. [Google Scholar] [CrossRef] [PubMed]
- Zampogna, E.; Paneroni, M.; Belli, S.; Aliani, M.; Gandolfo, A.; Visca, D.; Bellanti, M.T.; Ambrosino, N.; Vitacca, M. Pulmonary Rehabilitation in Patients Recovering from COVID-19. Respir. Int. Rev. Thorac. Dis. 2021, 100, 416–422. [Google Scholar] [CrossRef] [PubMed]
- Saeki, T.; Ogawa, F.; Chiba, R.; Nonogaki, M.; Uesugi, J.; Takeuchi, I.; Nakamura, T. Rehabilitation Therapy for A COVID-19 Patient who Received Mechanical Ventilation in Japan: A Case Report. Am. J. Phys. Med. Rehabil. 2020. [Google Scholar] [CrossRef]
- Shan, M.X.; Tran, Y.M.; Vu, K.T.; Eapen, B.C. Postacute inpatient rehabilitation for COVID-19. BMJ Case Rep. 2020, 13, e237406. [Google Scholar] [CrossRef]
- Beom, J.; Jung, J.; Hwang, I.C.; Cho, Y.J.; Kim, E.S.; Kim, H.B.; Lim, J.Y.; Song, K.H. Early rehabilitation in a critically ill inpatient with COVID-19. Eur. J. Phys. Rehabil. Med. 2020, 56, 858–861. [Google Scholar] [CrossRef]
- Bickton, F.M.; Chisati, E.; Rylance, J.; Morton, B. An Improvised Pulmonary Telerehabilitation Program for Postacute COVID-19 Patients Would Be Feasible and Acceptable in a Low-Resource Setting. Am. J. Phys. Med. Rehabil. 2021, 100, 209–212. [Google Scholar] [CrossRef]
- Livingston, T.; Sullivan, E.K.; Wilske, G.; Gustavson, A.M. Innovative Care Delivery of Acute Rehabilitation for Patients With COVID-19: A Case Report. Phys. Ther. 2021, 101, pzaa204. [Google Scholar] [CrossRef] [PubMed]
- Pancera, S.; Galeri, S.; Porta, R.; Pietta, I.; Bianchi, L.N.C.; Carrozza, M.C.; Villafañe, J.H. Feasibility and Efficacy of the Pulmonary Rehabilitation Program in a Rehabilitation Center: Case Report of A Young Patient Developing Severe COVID-19 Acute Respiratory Distress Syndrome. J. Cardiopulm. Rehabil. Prev. 2020, 40, 205–208. [Google Scholar] [CrossRef] [PubMed]
- Ramalingam, M.B.; Huang, Y.; Lim, P.A.C. Rehabilitation of a Post-Intensive Care Unit Patient After Severe COVID-19 Pneumonia. Am. J. Phys. Med. Rehabil. 2020, 99, 1092–1095. [Google Scholar] [CrossRef]
- Torres-Castro, R.; Vasconcello-Castillo, L.; Alsina-Restoy, X.; Solís-Navarro, L.; Burgos, F.; Puppo, H.; Vilaro, J. Respiratory function in patients post-infection by COVID-19: A systematic review and meta-analysis. Pulmonology 2021, 27, 328–337. [Google Scholar] [CrossRef] [PubMed]
- Bailly, M.; Evrard, B.; Coudeyre, E.; Rochette, C.; Meriade, L.; Blavignac, C.; Fournier, A.C.; Bignon, Y.J.; Dutheil, F.; Duclos, M.; et al. Health management of patients with COVID-19: Is there a room for hydrotherapeutic approaches? Int. J. Biometeorol. 2022, 66, 1031–1038. [Google Scholar] [CrossRef]
- Tenforde, M.W.; Self, W.H.; Adams, K.; Gaglani, M.; Ginde, A.A.; McNeal, T.; Ghamande, S.; Douin, D.J.; Talbot, H.K.; Casey, J.D.; et al. Association Between mRNA Vaccination and COVID-19 Hospitalization and Disease Severity. JAMA 2021, 326, 2043–2054. [Google Scholar] [CrossRef]
- Ghram, A.; Moalla, W.; Lavie, C.J. Vaccine and physical activity in the era of COVID-19 pandemic. Prog. Cardiovasc. Dis. 2021, 67, 33–34. [Google Scholar] [CrossRef] [PubMed]
- Valenzuela, P.L.; Simpson, R.J.; Castillo-García, A.; Lucia, A. Physical activity: A coadjuvant treatment to COVID-19 vaccination? Brain Behav. Immun. 2021, 94, 1–3. [Google Scholar] [CrossRef]
- Batatinha, H.; Baker, F.L.; Smith, K.A.; Zúñiga, T.M.; Pedlar, C.R.; Burgess, S.C.; Katsanis, E.; Simpson, R.J. Recent COVID-19 vaccination has minimal effects on the physiological responses to graded exercise in physically active healthy people. J. Appl. Physiol. 2022, 132, 275–282. [Google Scholar] [CrossRef]
- da Silveira, M.P.; da Silva Fagundes, K.K.; Bizuti, M.R.; Starck, É.; Rossi, R.C.; de Resende E Silva, D.T. Physical exercise as a tool to help the immune system against COVID-19: An integrative review of the current literature. Clin. Exp. Med. 2021, 21, 15–28. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bailly, M.; Pélissier, L.; Coudeyre, E.; Evrard, B.; Bingula, R.; Rochette, C.; Mériade, L.; Blavignac, C.; Fournier, A.-C.; Bignon, Y.-J.; et al. Systematic Review of COVID-19-Related Physical Activity-Based Rehabilitations: Benefits to Be Confirmed by More Robust Methodological Approaches. Int. J. Environ. Res. Public Health 2022, 19, 9025. https://doi.org/10.3390/ijerph19159025
Bailly M, Pélissier L, Coudeyre E, Evrard B, Bingula R, Rochette C, Mériade L, Blavignac C, Fournier A-C, Bignon Y-J, et al. Systematic Review of COVID-19-Related Physical Activity-Based Rehabilitations: Benefits to Be Confirmed by More Robust Methodological Approaches. International Journal of Environmental Research and Public Health. 2022; 19(15):9025. https://doi.org/10.3390/ijerph19159025
Chicago/Turabian StyleBailly, Mélina, Léna Pélissier, Emmanuel Coudeyre, Bertrand Evrard, Rea Bingula, Corinne Rochette, Laurent Mériade, Christelle Blavignac, Anne-Cécile Fournier, Yves-Jean Bignon, and et al. 2022. "Systematic Review of COVID-19-Related Physical Activity-Based Rehabilitations: Benefits to Be Confirmed by More Robust Methodological Approaches" International Journal of Environmental Research and Public Health 19, no. 15: 9025. https://doi.org/10.3390/ijerph19159025