
Intravascular Lithotripsy as a Novel Treatment Method for Calcified Unprotected Left Main Diseases—Comparison to Rotational Atherectomy—Short-Term Outcomes

 , , , , , and
, , , , , and
Abstract
:1. Introduction
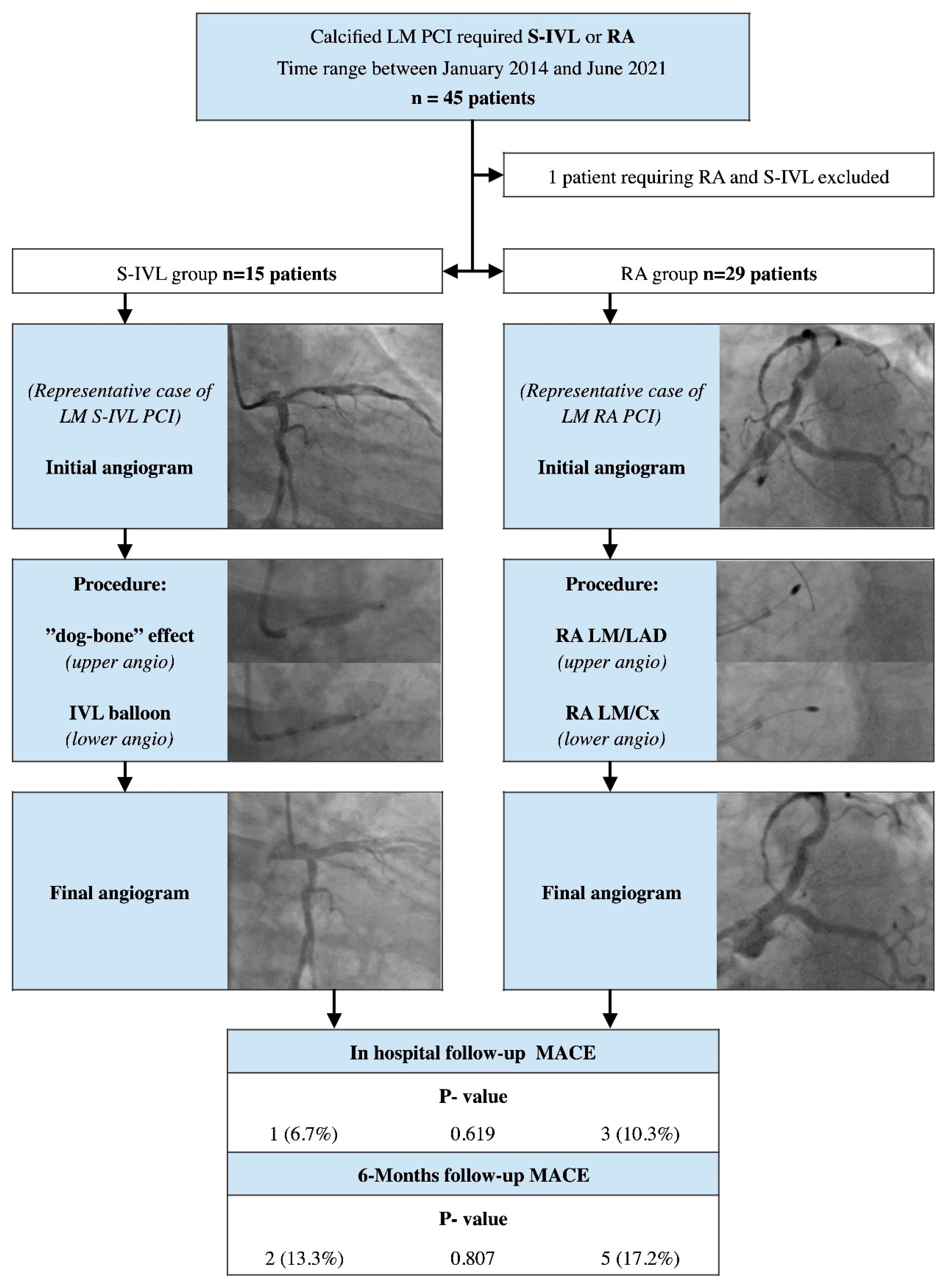
2. Materials and Methods
3. Results
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Kuramitsu, S.; Ohya, M.; Shinozaki, T.; Otake, H.; Horie, K.; Kawamoto, H.; Yamanaka, F.; Natsuaki, M.; Shiomi, H.; Nakazawa, G.; et al. Risk factors and long-term clinical outcomes of second-generation drug-eluting stent thrombosis. Circ. Cardiovasc. Interv. 2019, 12, e007822. [Google Scholar] [CrossRef]
- D’Ascenzo, F.; Elia, E.; Marengo, G.; Wańha, W.; Ferreiro, R.G.; Truffa, A.; Trabattoni, D.; Figini, F.; Verardi, R.; Di Palma, G.; et al. Long-term (≥15 years) follow-up of percutaneous coronary intervention of unprotected left main (from the GRAVITY registry). Am. J. Cardiol. 2021, 156, 72–78. [Google Scholar] [CrossRef]
- Uva, M.S.; Neumann, F.-J.; Ahlsson, A.; Alfonso, F.; Banning, A.; Benedetto, U.; Byrne, R.A.; Collet, J.-P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS guidelines on myocardial revascularization. Eur. J. Cardio-Thorac. Surg. 2019, 55, 4–90. [Google Scholar] [CrossRef] [Green Version]
- Copeland-Halperin, R.S.; Baber, U.; Aquino, M.; Rajamanickam, A.; Roy, S.; Hasan, C.; Barman, N.; Kovacic, J.C.; Moreno, P.; Krishnan, P.; et al. Prevalence, correlates, and impact of coronary calcification on adverse events following PCI with newer-generation DES: Findings from a large multiethnic registry. Catheter. Cardiovasc. Interv. 2018, 91, 859–866. [Google Scholar] [CrossRef]
- Rozenbaum, Z.; Takahashi, T.; Kobayashi, Y.; Bliagos, D.; Menegus, M.; Colombo, A.; Latib, A. Contemporary technologies to modify calcified plaque in coronary artery disease. Prog. Cardiovasc. Dis. 2021, 69, 18–26. [Google Scholar] [CrossRef]
- Rola, P.; Włodarczak, A.; Jastrzębski, A.; Barycki, M.; Turkiewicz, K.; Kulczycki, J.J.; Szudrowicz, M.; Pęcherzewski, M.; Doroszko, A.; Lesiak, M. Impella protected percutaneous coronary intervention on the last remaining highly calcified coronary artery facil-itated by shockwave intravascular lithotripsy and levosimendan infusion. Kardiol Pol. 2021, 79, 1145–1146. [Google Scholar] [CrossRef]
- Rola, P.; Włodarczak, A.; Barycki, M.; Kulczycki, J.J.; Engel, B.; Doroszko, A. “All hands on deck”—Rota-lithotripsy—A combination of rotational atherectomy and intravascular lithotripsy (shockwave) with additional use of a Turnpike Gold microcatheter and guide extension as a novel approach for calcified lesions. Postepy Kardiol Interwencyjnej 2021, 17, 214–217. [Google Scholar] [CrossRef]
- Lee, K.; Jung, J.H.; Lee, M.; Kim, D.W.; Park, M.W.; Choi, I.J.; Lee, J.H.; Lee, J.H.; Lee, S.R.; Lee, P.H.; et al. Clinical outcome of rotational atherectomy in calcified lesions in Korea-ROCK registry. Medicina 2021, 57, 694. [Google Scholar] [CrossRef]
- Januszek, R.; Siudak, Z.; Dziewierz, A.; Rakowski, T.; Legutko, J.; Dudek, D.; Bartuś, S. Bailout rotational atherectomy in patients with myocardial infarction is not associated with an increased periprocedural complication rate or poorer angiographic out-comes in comparison to elective procedures (from the ORPKI Polish National Registry 2015–2016). Postepy Kardiol Interwencyjnej 2018, 14, 135–143. [Google Scholar]
- Iannaccone, M.; Barbero, U.; D’Ascenzo, F.; Latib, A.; Pennacchi, M.; Rossi, M.L.; Ugo, F.; Meliga, E.; Kawamoto, H.; Moretti, C.; et al. Rotational atherectomy in very long lesions: Results for the ROTATE registry. Catheter. Cardiovasc. Interv. 2016, 88, E164–E172. [Google Scholar] [CrossRef]
- Sharma, S.K.; Tomey, M.I.; Teirstein, P.S.; Kini, A.S.; Reitman, A.B.; Lee, A.C.; Généreux, P.; Chambers, J.W.; Grines, C.L.; Himmelstein, S.I.; et al. North American expert review of rotational atherectomy. Circ. Cardiovasc. Interv. 2019, 12, e007448. [Google Scholar] [CrossRef]
- Sabatowski, K.; Malinowski, K.P.; Siudak, Z.; Reczuch, K.; Dobrzycki, S.; Lesiak, M.; Hawranek, M.; Gil, R.J.; Witkowski, A.; Wojakowski, W.; et al. Sex-related differences and rotational atherectomy: Analysis of 5 177 percutaneous coronary interventions based on a large national registry from 2014 to 2020. Kardiol. Polska 2021, 79, 1320–1327. [Google Scholar] [CrossRef] [PubMed]
- Adams, G.; Shammas, N.; Mangalmurti, S.; Bernardo, N.L.; Miller, W.E.; Soukas, P.A.; Parikh, S.A.; Armstrong, E.J.; Tepe, G.; Lansky, A.; et al. Intravascular lithotripsy for treatment of calcified lower extremity arterial stenosis: Initial analysis of the disrupt PAD III study. J. Endovasc. Ther. 2020, 27, 473–480. [Google Scholar] [CrossRef] [PubMed]
- Hill, J.M.; Kereiakes, D.J.; Shlofmitz, R.A.; Klein, A.J.; Riley, R.F.; Price, M.J.; Herrmann, H.C.; Bachinsky, W.; Waksman, R.; Stone, G.W. Disrupt CAD III investigators. Intravascular lithotripsy for treatment of severely calcified coronary artery disease. J. Am. Coll. Cardiol. 2020, 76, 2635–2646. [Google Scholar] [CrossRef]
- Rola, P.; Włodarczak, A.; Kulczycki, J.J.; Barycki, M.; Furtan, Ł.; Pęcherzewski, M.; Szudrowicz, M.; Włodarczak, S.; Doroszko, A.; Lesiak, M. Efficacy and safety of shockwave intravascular lithotripsy (S-IVL) in calcified unprotected left main percutaneous coronary intervention—Short-term outcomes. Postepy Kardiol Interwencyjnej 2021, 17, 344–348. [Google Scholar] [CrossRef]
- Nowak, A.; Ratajczak, J.; Kasprzak, M.; Sukiennik, A.; Fabiszak, T.; Wojakowski, W.; Ochała, A.; Wańha, W.; Kuczmik, W.; Navarese, E.P.; et al. Long-term outcome of rotational atherectomy according to burr-to-artery ratio and changes in coronary artery blood flow: Observational analysis. Cardiol. J. 2021. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D. Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction. Fourth universal definition of myocardial infarction. J. Am. Coll Cardiol. 2018, 72, 2231–2264. [Google Scholar]
- Garcia-Garcia, H.M.; McFadden, E.P.; Farb, A.; Mehran, R.; Stone, G.W.; Spertus, J.; Onuma, Y.; Morel, M.-A.; Van Es, G.-A.; Zuckerman, B.; et al. Standardized end point definitions for coronary intervention trials: The academic research consortium-2 consensus document. Circulation 2018, 137, 2635–2650. [Google Scholar] [CrossRef]
- R Development Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://www.R-project.org/ (accessed on 16 June 2022).
- Neumann, F.-J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.-P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS guidelines on myocardial revascularization. EuroIntervention 2019, 14, 1435–1534. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.S.; Yang, T.; Lasala, J.; Cox, D. Impact of coronary artery calcification in percutaneous coronary intervention with paclitaxel-eluting stents: Two-year clinical outcomes of paclitaxel-eluting stents in patients from the ARRIVE program. Catheter. Cardiovasc. Interv. 2016, 88, 891e–897e. [Google Scholar] [CrossRef]
- Yabushita, H.; Takagi, K.; Tahara, S.; Fujino, Y.; Warisawa, T.; Kawamoto, H.; Watanabe, Y.; Mitomo, S.; Karube, K.; Matsumoto, T.; et al. Impact of rota-tional atherectomy on heavily calcified, unprotected left main disease. Circ. J. 2014, 78, 1867–1872. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Lara, J.; Pinar, E.; Valdesuso, R.; Lacunza, J.; Gimeno, J.R.; Hurtado, J.A.; Valdés-Chávarri, M. Percutaneous coronary inter-vention with rotational atherectomy for severely calcified unprotected left main: Immediate and two-years follow-up re-sults. Catheter. Cardiovasc. Interv. 2012, 80, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Ielasi, A.; Kawamoto, H.; Latib, A.; Boccuzzi, G.G.; Sardella, G.; Garbo, R.; Meliga, E.; D’Ascenzo, F.; Presbitero, P.; Nakamura, S.; et al. In-hospital and 1-year outcomes of rotational atherectomy and stent implantation in patients with severely calcified unprotected left main narrowings (from the multicenter ROTATE registry). Am. J. Cardiol. 2017, 119, 1331–1337. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, D.L.; Lopes, R.D.; Harrington, R.A. Diagnosis and treatment of acute coronary syndromes: An analysis from the british cardiovascular intervention society database. JAMA 2022, 327, 662–675, Erratum in: JAMA, 2022, 327, 1710. [Google Scholar] [CrossRef] [PubMed]
- Jakubiak, G.K.; Pawlas, N.; Cieślar, G.; Stanek, A. Pathogenesis and clinical significance of in-stent restenosis in patients with diabetes. Int. J. Environ. Res. Public Health 2021, 18, 11970. [Google Scholar] [CrossRef]
- Ocaranza-Sánchez, R.; Abellás-Sequeiros, R.A.; Santás-Álvarez, M.; Bayón-Lorenzo, J.; Gonzalez-Juanatey, C. First-in-man report-ed 12-months follow-up after intravascular lithotripsy in left main percutaneous revascularization. Coron. Artery Dis. 2021, 32, 586–587. [Google Scholar] [CrossRef]
- Cosgrove, C.S.; Wilson, S.J.; Bogle, R.; Hanratty, C.G.; Williams, R.; Walsh, S.J.; McEntegart, M.; Spratt, J.C. Intravascular lithotripsy for lesion preparation in patients with calcific distal left main disease. EuroIntervention 2020, 16, 76–79. [Google Scholar] [CrossRef]
- Salazar, C.H.; Gonzalo, N.; Aksoy, A.; Forero, M.N.T.; Nef, H.; Van Mieghem, N.M.; Latib, A.; Sanchez, R.O.; Werner, N.; Escaned, J. Feasibility, safety, and efficacy of intravascular lithotripsy in severely calcified left main coronary stenosis. JACC Cardiovasc. Interv. 2020, 13, 1727–1729. [Google Scholar] [CrossRef]
- Wańha, W.; Tomaniak, M.; Wańczura, P.; Bil, J.; Januszek, R.; Wolny, R.; Opolski, M.P.; Kuźma, Ł.; Janas, A.; Figatowski, T.; et al. Intravascular lithotripsy for the treatment of stent underexpansion: The multicenter IVL-DRAGON registry. J. Clin. Med. 2022, 11, 1779. [Google Scholar] [CrossRef]
- Rola, P.; Włodarczak, A.; Kulczycki, J.J.; Barycki, M.; Furtan, Ł.; Szudrowicz, M.; Jastrzębski, A.; Pęcherzewski, M.; Doroszko, A.; Lesiak, M. Feasibility of the intravascular lithotripsy in coronary artery disease. Short-term outcomes of the Lower-Silesia shockwave registry. Kardiol. Polska 2021, 79, 1133–1135. [Google Scholar] [CrossRef]
- Sattar, Y.; Ullah, W.; Mir, T.; Biswas, S.; Titus, A.; Darmoch, F.; Pacha, H.M.; Mohamed, M.O.; Kwok, C.S.; Fischman, D.L.; et al. Safety and efficacy of coronary intravascular lithotripsy for calcified coronary arteries– a systematic review and meta-analysis. Expert Rev. Cardiovasc. Ther. 2020, 19, 89–98. [Google Scholar] [CrossRef] [PubMed]
- Rola, P.; Włodarczak, A.; Barycki, M.; Pęcherzewski, M.; Kulczycki, J.J.; Szudrowicz, M.; Jastrzębski, A.; Furtan, Ł.; Doroszko, A.; Lesiak, M. Shockwave intravascular lithotripsy as a novel strategy for balloon undilatable heavily calcified chronic total occlusion lesions. Cardiol. J. 2021. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, M.B.; Arujuna, A.; Ilsley, C.; Archbold, A.; Crake, T.; Firoozi, S.; Kalra, S.; Knight, C.; Lim, P.; Malik, I.S.; et al. Radial versus femoral access is associated with reduced complications and mortality in patients with non-ST-segment-elevation myocardial infarction: An observational cohort study of 10,095 patients. Circ. Cardiovasc. Interv. 2014, 7, 456–464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vranckx, P.; Frigoli, E.; Rothenbühler, M.; Tomassini, F.; Garducci, S.; Andò, G.; Picchi, A.; Sganzerla, P.; Paggi, A.; Ugo, F.; et al. Radial versus femoral access in patients with acute coronary syndromes with or without ST-segment elevation. Eur. Heart J. 2017, 38, 1069–1080. [Google Scholar] [CrossRef]
- Olinic, D.-M.; Stanek, A.; Tătaru, D.-A.; Homorodean, C.; Olinic, M. Acute limb ischemia: An update on diagnosis and management. J. Clin. Med. 2019, 8, 1215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Włodarczak, A.; Rola, P.; Barycki, M.; Kulczycki, J.J.; Szudrowicz, M.; Lesiak, M.; Doroszko, A. Rota-lithotripsy-a novel bail-out strategy for calcified coronary lesions in acute coronary syndrome. The first-in-man experience. J. Clin. Med. 2021, 10, 1872. [Google Scholar] [CrossRef]
- Mentias, A.; Sarrazin, M.V.; Saad, M.; Panaich, S.; Kapadia, S.; Horwitz, P.A.; Girotra, S. Long-term outcomes of coronary stenting with and without use of intravascular ultrasound. JACC Cardiovasc. Interv. 2020, 13, 1880–1890. [Google Scholar] [CrossRef]
- Pawłowski, T.; Legutko, J.; Kochman, J.; Roleder, T.; Pręgowski, J.; Chmielak, Z.; Kubica, J.; Ochała, A.; Parma, R.; Grygier, M.; et al. Clinical use of intracoronary imaging modalities in Poland. Expert opinion of the Association of Cardiovascular Interventions of the Polish Cardiac Society. Kardiol. Polska 2022, 80, 509–519. [Google Scholar] [CrossRef]
- Kinnaird, T.; Johnson, T.; Anderson, R.; Gallagher, S.; Sirker, A.; Ludman, P.; de Belder, M.; Copt, S.; Oldroyd, K.; Banning, A.; et al. Intravascular imaging and 12-month mortality after unprotected left main stem PCI: An analysis from the British cardiovascular intervention society database. JACC Cardiovasc. Interv. 2020, 13, 346–357. [Google Scholar] [CrossRef]
- Gue, Y.X.; Jeong, Y.-H.; Farag, M.; Spinthakis, N.; Gorog, D.A. Precision treatment in ACS–Role of assessing fibrinolysis. J. Clin. Med. 2021, 10, 929. [Google Scholar] [CrossRef]
- Jakubiak, G.K.; Cieślar, G.; Stanek, A. Nitrotyrosine, nitrated lipoproteins, and cardiovascular dysfunction in patients with type 2 diabetes: What do we know and what remains to be explained? Antioxidants 2022, 11, 856. [Google Scholar] [CrossRef] [PubMed]
- Tomaniak, M.; Katagiri, Y.; Modolo, R.; De Silva, R.; Khamis, R.Y.; Bourantas, C.V.; Torii, R.; Wentzel, J.J.; Gijsen, F.J.H.; Van Soest, G.; et al. Vulnerable plaques and patients: State-of-the-art. Eur. Heart. J. 2020, 41, 2997–3004. [Google Scholar] [CrossRef] [PubMed]
- Ochijewicz, D.; Tomaniak, M.; Koltowski, L.; Rdzanek, A.; Pietrasik, A.; Kochman, J. Intravascular imaging of coronary artery disease: Recent progress and future directions. J. Cardiovasc. Med. 2017, 18, 733–741. [Google Scholar] [CrossRef] [PubMed]
- Ahn, J.-M.; Kang, S.-J.; Yoon, S.-H.; Park, H.W.; Kang, S.M.; Lee, J.-Y.; Lee, S.-W.; Kim, Y.-H.; Lee, C.W.; Park, S.-W.; et al. Meta-analysis of outcomes after intravascular ultrasound–guided versus angiography-guided drug-eluting stent implantation in 26,503 patients enrolled in three randomized trials and 14 observational studies. Am. J. Cardiol. 2014, 113, 1338–1347. [Google Scholar] [CrossRef] [PubMed]
- Van Zandvoort, L.J.; Tomaniak, M.; Forero, M.N.T.; Masdjedi, K.; Visseren, L.; Witberg, K.; Ligthart, J.; Kardys, I.; Lemmert, M.E.; Diletti, R.; et al. Predictors for clinical outcome of untreated stent edge dissections as detected by optical coherence tomography. Circ. Cardiovasc. Interv. 2020, 13, e008685. [Google Scholar] [CrossRef]
- Gupta, T.; Weinreich, M.; Greenberg, M.; Colombo, A.; Latib, A. Rotational atherectomy: A contemporary appraisal. Interv. Cardiol. Rev. Res. Resour. 2019, 14, 182–189. [Google Scholar] [CrossRef]
- Zieliński, K.; Kołtowski, Ł.; Kalińczuk, Ł.; Mintz, G.S.; Kochman, J.; Witkowski, A.; Pręgowski, J.; Motyl, D.; Lorusso, R.; Suwalski, P.; et al. In-hospital outcomes of rotational versus orbital atherectomy during percutaneous coronary intervention: A meta-analysis. Kardiol. Polska 2019, 77, 846–852. [Google Scholar] [CrossRef] [Green Version]
- Rola, P.; Włodarczak, A.; Barycki, M.; Doroszko, A. Use of the shock wave therapy in basic research and clinical applications—From bench to bedsite. Biomedicines 2022, 10, 568. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Rotational Atherectomy (RA) N-29 | Shockwave Intravascular (S-IVL) N-15 | p-Value | |
|---|---|---|---|
| Age | 70.3 ± 9.1 | 72.1 ± 6.1 | 0.478 |
| Gender male (ratio) | 21 (72.4%) | 12 (80.0%) | 0.532 |
| Stable angina | 13 (44.8%) | 6 (40.0%) | 0.591 |
| Unstable angina | 6 (20.7%) | 2 (13.3%) | 0.511 |
| NSTEMI | 9 (31.0%) | 6 (40.0%) | 0.535 |
| STEMI | 1 (3.4%) | 1 (6.7%) | 0.561 |
| Diabetes mellitus | 16 (55.2%) | 10 (66.7%) | 0.487 |
| Chronic heart failure | 9 (31.0%) | 6 (40.0%) | 0.412 |
| Hypertension | 25 (86.2%) | 13 (86.7%) | 0.591 |
| Hyperlipidemia | 20 (68.9%) | 15 (100%) | 0.293 |
| Atrial Fibrillation | 5 (17.2%) | 5 (33.3%) | 0.248 |
| History of PCI | 16 (55.2%) | 7 (46.7%) | 0.544 |
| History of MI | 13 (44.8%) | 5 (33.3%) | 0.360 |
| History of CABG | 6 (20.7%) | 1 (6.7%) | 0.311 |
| COPD | 6 (20.7%) | 2 (13.3%) | 0.511 |
| Chronic kidney diseases | 13 (44.8%) | 6 (40.0%) | 0.519 |
| Rotational Atherectomy N-29 | Shockwave Intravascular N-15 | p-Value | |
|---|---|---|---|
| Syntax I score | 28.0 ± 7.5; | 23.3 ± 13.0 | 0.038 |
| Syntax II—PCI score | 35.8 ± 8.4 | 38.7 ± 14.8 | 0.489 |
| Syntax II PCI four year mortality | 9.6 [7.7–15.2] | 10.1 [5–34] | 0.876 |
| Syntax II—CABG score | 34.5 ± 9.0 | 38.3 ± 10.5 | 0.175 |
| Syntax II CABG year mortality | 11.5 [6.8–28.9] | 10.3 [6–20.1] | 0.414 |
| Radial Access | 15 (51.7%) | 12 (80.0%) | 0.287 |
| 6F Guide Catheter | 3 (10.3%) | 4 (26.7%) | 0.115 |
| 7F or larger Guide Catheter | 26 (89.6%) | 11 (73.3%) | 0.263 |
| Predilatation | 26 (89.6%) | 15 (100%) | 0.498 |
| Predilatation balloon diameter (mm) | 2.78 [2.5–3.0] | 3.24 [3–3.5] | 0.002 |
| Predilatation pressure (atm) | 21.2 ± 1.4 | 19.2 ± 1.4 | 0.031 |
| Single stent technique | 21 (72.4%) | 11 (73.3%) | 0.458 |
| Two stent bifurcation technique | 8 (27.6%) | 3 (20.0%) | 0.357 |
| Postdilatation—POT | 26 (89.6%) | 14 (93.3%) | 0.558 |
| Intravascular Guidance | 3 (10.3%) | 3 (20.0%) | 0.420 |
| Perforation | 3 (10.3%) | 0 (0%) | 0.327 |
| No-flow phenomenon | 1 (3.4%) | 0 (0%) | 0.561 |
| Administration of catecholamines | 2 (6.9%) | 2 (13.3%) | 0.420 |
| Acetylsalicylic Acid | 29 (100%) | 15 (100%) | 1 |
| Clopidogrel | 19 (65.6%) | 9 (60%) | 0.552 |
| Ticagrelol | 10 (34.4%) | 6 (40%) | 0.552 |
| Rotational Atherectomy N-29 | Shockwave Intravascular N-15 | p-Value | |
|---|---|---|---|
| In hospital follow-up | |||
| MACE | 3 (10.3%) | 1 (6.7%) | 0.619 |
| Death | 3 (10.3%) | 1 (6.7%) | 0.619 |
| Myocardial infarction | 0 (0%) | 1 (6.7%) | 0.341 |
| Target vessel revascularization | 0 (0%) | 1 (6.7%) | 0.341 |
| Stent thrombosis | 0 (0%) | 1 (6.7%) | 0.341 |
| Cerebrovascular episodes | 0 (0%) | 0 (0%) | – |
| Stent restenosis | 0 (0%) | 0 (0%) | – |
| Any revascularization | 0 (0%) | 0 (0%) | – |
| Six Month follow-up | |||
| MACE | 5 (17.2%) | 2 (13.3%) | 0.807 |
| Death | 4 (13.7%) | 2 (13.3%) | 0.965 |
| Myocardial infarction | 1 (3.4%) | 1 (6.7%) | 0.619 |
| Target vessel revascularization | 0 (0%) | 1 (6.7%) | 0.151 |
| Stent thrombosis | 0 (0%) | 1 (6.7%) | 0.151 |
| Cerebrovascular episodes | 0 (0%) | 0 (0%) | – |
| Stent restenosis | 0 (0%) | 0 (0%) | – |
| Any revascularization | 2 (6.9%) | 0 (0%) | 0.413 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rola, P.; Kulczycki, J.J.; Włodarczak, A.; Barycki, M.; Włodarczak, S.; Szudrowicz, M.; Furtan, Ł.; Jastrzębski, A.; Pęcherzewski, M.; Lesiak, M.; et al. Intravascular Lithotripsy as a Novel Treatment Method for Calcified Unprotected Left Main Diseases—Comparison to Rotational Atherectomy—Short-Term Outcomes. Int. J. Environ. Res. Public Health 2022, 19, 9011. https://doi.org/10.3390/ijerph19159011
Rola P, Kulczycki JJ, Włodarczak A, Barycki M, Włodarczak S, Szudrowicz M, Furtan Ł, Jastrzębski A, Pęcherzewski M, Lesiak M, et al. Intravascular Lithotripsy as a Novel Treatment Method for Calcified Unprotected Left Main Diseases—Comparison to Rotational Atherectomy—Short-Term Outcomes. International Journal of Environmental Research and Public Health. 2022; 19(15):9011. https://doi.org/10.3390/ijerph19159011
Chicago/Turabian StyleRola, Piotr, Jan Jakub Kulczycki, Adrian Włodarczak, Mateusz Barycki, Szymon Włodarczak, Marek Szudrowicz, Łukasz Furtan, Artur Jastrzębski, Maciej Pęcherzewski, Maciej Lesiak, and et al. 2022. "Intravascular Lithotripsy as a Novel Treatment Method for Calcified Unprotected Left Main Diseases—Comparison to Rotational Atherectomy—Short-Term Outcomes" International Journal of Environmental Research and Public Health 19, no. 15: 9011. https://doi.org/10.3390/ijerph19159011