
The Identification of Subphenotypes and Associations with Health Outcomes in Patients with Opioid-Related Emergency Department Encounters Using Latent Class Analysis

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Population
2.3. Variables and Covariates
2.4. Statistical Analyses
3. Results
3.1. Model Selection
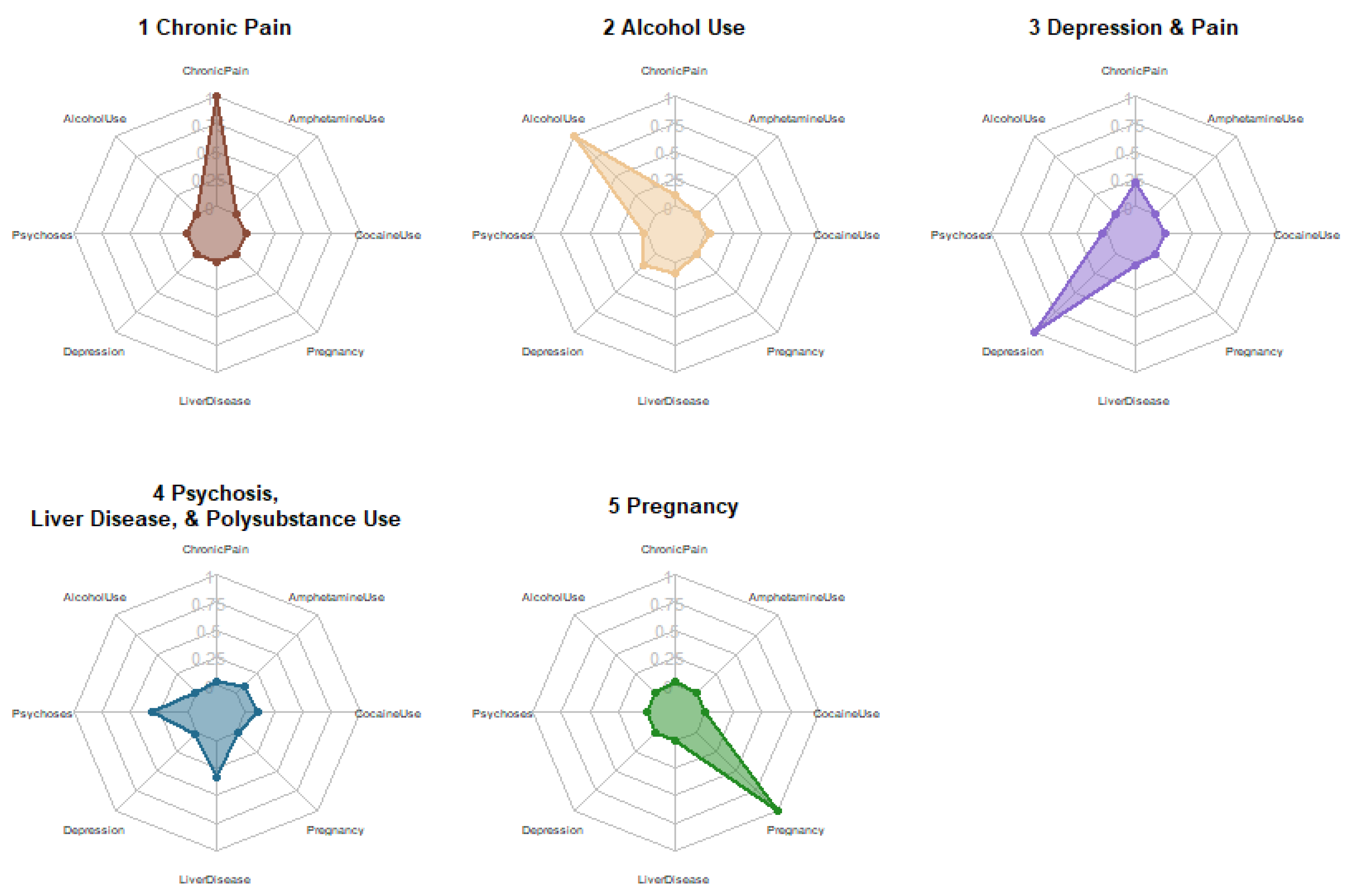
3.2. Subphenotype Characteristics
3.3. Outcomes and Cost Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Centers for Disease Control and Prevention, National Center for Health Statistics. Multiple Cause of Death 1999–2017 on CDC WONDER Online Database, Released January 2020. Available online: https://wonder.cdc.gov/wonder/help/mcd.html (accessed on 3 March 2021).
- CDC Health Alert Network Increase in Fatal Drug Overdoses Across the United States Driven by Synthetic Opioids Before and During the COVID-19 Pandemic 2020. Available online: https://emergency.cdc.gov/han/2020/han00438.asp (accessed on 3 March 2021).
- National Institute on Drug Abuse. Overdose Death Rates. 2021. Available online: https://nida.nih.gov/research-topics/trends-statistics/overdose-death-rates (accessed on 3 March 2021).
- Langabeer, J.R.; Stotts, A.L.; Bobrow, B.J.; Wang, H.E.; Chambers, K.A.; Yatsco, A.J.; Cardenas-Turanzas, M.; Champagne-Langabeer, T. Prevalence and Charges of Opioid-Related Visits to U.S. Emergency Departments. Drug Alcohol Depend. 2021, 221, 108568. [Google Scholar] [CrossRef] [PubMed]
- Abbasi, A.B.; Salisbury-Afshar, E.; Jovanov, D.; Berberet, C.; Arunkumar, P.; Aks, S.E.; Layden, J.E.; Pho, M.T. Health Care Utilization of Opioid Overdose Decedents with No Opioid Analgesic Prescription History. J. Urban Health 2019, 96, 38–48. [Google Scholar] [CrossRef] [PubMed]
- Balio, C.P.; Wiley, K.K.; Greene, M.S.; Vest, J.R. Opioid-Related Emergency Department Encounters: Patient, Encounter, and Community Characteristics Associated With Repeated Encounters. Ann. Emerg. Med. 2020, 75, 568–575. [Google Scholar] [CrossRef] [PubMed]
- O’Grady, M.A.; Kapoor, S.; Kwon, N.; Morley, J.; Auerbach, M.; Neighbors, C.J.; Conigliaro, J.; Morgenstern, J. Substance Use Screening and Brief Intervention: Evaluation of Patient and Implementation Differences between Primary Care and Emergency Department Settings. J. Eval. Clin. Pract. 2019, 25, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Weiner, S.G.; Baker, O.; Bernson, D.; Schuur, J.D. One-Year Mortality of Patients After Emergency Department Treatment for Nonfatal Opioid Overdose. Ann. Emerg. Med. 2020, 75, 13–17. [Google Scholar] [CrossRef] [Green Version]
- Leece, P.; Chen, C.; Manson, H.; Orkin, A.M.; Schwartz, B.; Juurlink, D.N.; Gomes, T. One-Year Mortality After Emergency Department Visit for Nonfatal Opioid Poisoning: A Population-Based Analysis. Ann. Emerg. Med. 2020, 75, 20–28. [Google Scholar] [CrossRef] [Green Version]
- D’Onofrio, G.; McCormack, R.P.; Hawk, K. Emergency Departments-A 24/7/365 Option for Combating the Opioid Crisis. N. Engl. J. Med. 2018, 379, 2487–2490. [Google Scholar] [CrossRef] [Green Version]
- D’Onofrio, G.; Chawarski, M.C.; O’Connor, P.G.; Pantalon, M.V.; Busch, S.H.; Owens, P.H.; Hawk, K.; Bernstein, S.L.; Fiellin, D.A. Emergency Department-Initiated Buprenorphine for Opioid Dependence with Continuation in Primary Care: Outcomes During and After Intervention. J. Gen. Intern. Med. 2017, 32, 660–666. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.S.; Aks, S.E. Take-Home Naloxone and the Need for a Publicly Funded Naloxone Supply. J. Addict. Med. 2021, 16, 1–3. [Google Scholar] [CrossRef]
- Waye, K.M.; Goyer, J.; Dettor, D.; Mahoney, L.; Samuels, E.A.; Yedinak, J.L.; Marshall, B.D.L. Implementing Peer Recovery Services for Overdose Prevention in Rhode Island: An Examination of Two Outreach-Based Approaches. Addict. Behav. 2019, 89, 85–91. [Google Scholar] [CrossRef]
- Kaczorowski, J.; Bilodeau, J.; Orkin, A.M.; Dong, K.; Daoust, R.; Kestler, A. Emergency Department-Initiated Interventions for Patients with Opioid Use Disorder: A Systematic Review. Acad. Emerg. Med. 2020, 27, 1173–1182. [Google Scholar] [CrossRef] [PubMed]
- Gunn, A.H.; Smothers, Z.P.W.; Schramm-Sapyta, N.; Freiermuth, C.E.; MacEachern, M.; Muzyk, A.J. The Emergency Department as an Opportunity for Naloxone Distribution. West. J. Emerg. Med. 2018, 19, 1036–1042. [Google Scholar] [CrossRef] [PubMed]
- Kaucher, K.A.; Caruso, E.H.; Sungar, G.; Gawenus, L.; Hurlbut, K.; Sanchez, D.C.; Broderick, K. Evaluation of an Emergency Department Buprenorphine Induction and Medication-Assisted Treatment Referral Program. Am. J. Emerg. Med. 2020, 38, 300–304. [Google Scholar] [CrossRef] [PubMed]
- Chan, G.; Gelernter, J.; Oslin, D.; Farrer, L.; Kranzler, H.R. Empirically Derived Subtypes of Opioid Use and Related Behaviors. Addiction 2011, 106, 1146–1154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, S.; Biello, K.B.; Bazzi, A.R.; Drainoni, M.-L. Age Differences in Emergency Department Utilization and Repeat Visits among Patients with Opioid Use Disorder at an Urban Safety-Net Hospital: A Focus on Young Adults. Drug Alcohol Depend. 2019, 200, 14–18. [Google Scholar] [CrossRef]
- Weiss, R.D.; Rao, V. The Prescription Opioid Addiction Treatment Study: What Have We Learned. Drug Alcohol Depend. 2017, 173 (Suppl. S1), S48–S54. [Google Scholar] [CrossRef]
- Afshar, M.; Joyce, C.; Dligach, D.; Sharma, B.; Kania, R.; Xie, M.; Swope, K.; Salisbury-Afshar, E.; Karnik, N.S. Subtypes in Patients with Opioid Misuse: A Prognostic Enrichment Strategy Using Electronic Health Record Data in Hospitalized Patients. PLoS ONE 2019, 14, e0219717. [Google Scholar] [CrossRef]
- Liu, S.J.; Mair, C.; Songer, T.J.; Krans, E.E.; Wahed, A.; Talbott, E. Opioid-Related Hospitalizations in Pennsylvania: A Latent Class Analysis. Drug Alcohol Depend. 2019, 202, 185–190. [Google Scholar] [CrossRef]
- Barton, A.W.; Reinhart, C.A.; Campbell, C.C.; Smith, D.C.; Albarracin, D. Opioid Use at the Transition to Emerging Adulthood: A Latent Class Analysis of Non-Medical Use of Prescription Opioids and Heroin Use. Addict. Behav. 2021, 114, 106757. [Google Scholar] [CrossRef]
- Mori, M.; Krumholz, H.M.; Allore, H.G. Using Latent Class Analysis to Identify Hidden Clinical Phenotypes. JAMA 2020, 324, 700. [Google Scholar] [CrossRef]
- Grant, R.W.; McCloskey, J.; Hatfield, M.; Uratsu, C.; Ralston, J.D.; Bayliss, E.; Kennedy, C.J. Use of Latent Class Analysis and K-Means Clustering to Identify Complex Patient Profiles. JAMA Netw. Open 2020, 3, e2029068. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.O.; Morgan-Lopez, A.A.; Nonnemaker, J.M.; Pepper, J.K.; Hensel, E.C.; Robinson, R.J. Latent Class Analysis of E-Cigarette Use Sessions in Their Natural Environments. Nicotine Tob. Res. 2019, 21, 1408–1413. [Google Scholar] [CrossRef] [PubMed]
- Calfee, C.S.; Delucchi, K.; Parsons, P.E.; Thompson, B.T.; Ware, L.B.; Matthay, M.A. NHLBI ARDS Network Subphenotypes in Acute Respiratory Distress Syndrome: Latent Class Analysis of Data from Two Randomised Controlled Trials. Lancet Respir. Med. 2014, 2, 611–620. [Google Scholar] [CrossRef] [Green Version]
- Skogen, J.C.; Bøe, T.; Thørrisen, M.M.; Riper, H.; Aas, R.W. Sociodemographic Characteristics Associated with Alcohol Consumption and Alcohol-Related Consequences, a Latent Class Analysis of The Norwegian WIRUS Screening Study. BMC Public Health 2019, 19, 1364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Hcup Nationwide Emergency Department Sample (NEDS). 2016. Available online: https://www.hcup-us.ahrq.gov/db/nation/neds/NEDS_Introduction_2016.jsp (accessed on 29 November 2021).
- Weiss, A.J.; McDermott, K.W.; Heslin, K.C. Table 1, ICD-10-CM Diagnosis Codes Defining Different Opioid-Related Conditions. Available online: http://www.ncbi.nlm.nih.gov/books/NBK538344/table/sb247.tab1/ (accessed on 18 January 2021).
- Bonar, E.E.; Coughlin, L.; Roche, J.S.; Philyaw-Kotov, M.L.; Bixler, E.A.; Sinelnikov, S.; Kolosh, A.; Cihak, M.J.; Cunningham, R.M.; Walton, M.A. Prescription Opioid Misuse among Adolescents and Emerging Adults in the United States: A Scoping Review. Prev. Med. 2020, 132, 105972. [Google Scholar] [CrossRef]
- Ridley, K.; Coleman, M. The Epidemiology of Amphetamine Type Stimulant-Related Admissions in Albany, Western Australia: 2008–2013. Australas. Psychiatry 2015, 23, 241–244. [Google Scholar] [CrossRef]
- Altekruse, S.F.; Cosgrove, C.M.; Altekruse, W.C.; Jenkins, R.A.; Blanco, C. Socioeconomic Risk Factors for Fatal Opioid Overdoses in the United States: Findings from the Mortality Disparities in American Communities Study (MDAC). PLoS ONE 2020, 15, e0227966. [Google Scholar] [CrossRef] [Green Version]
- van Draanen, J.; Tsang, C.; Mitra, S.; Karamouzian, M.; Richardson, L. Socioeconomic Marginalization and Opioid-Related Overdose: A Systematic Review. Drug Alcohol Depend. 2020, 214, 108127. [Google Scholar] [CrossRef]
- Nylund, K.L.; Asparouhov, T.; Muthén, B.O. Deciding on the Number of Classes in Latent Class Analysis and Growth Mixture Modeling: A Monte Carlo Simulation Study. Struct. Equ. Modeling A Multidiscip. J. 2007, 14, 535–569. [Google Scholar] [CrossRef]
- Wurpts, I.C.; Geiser, C. Is Adding More Indicators to a Latent Class Analysis Beneficial or Detrimental? Results of a Monte-Carlo Study. Front. Psychol. 2014, 5, 920. [Google Scholar] [CrossRef] [Green Version]
- Stamovlasis, D.; Papageorgiou, G.; Tsitsipis, G.; Tsikalas, T.; Vaiopoulou, J. Illustration of Step-Wise Latent Class Modeling With Covariates and Taxometric Analysis in Research Probing Children’s Mental Models in Learning Sciences. Front. Psychol. 2018, 9, 532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. STROBE Initiative The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Vowles, K.E.; McEntee, M.L.; Julnes, P.S.; Frohe, T.; Ney, J.P.; van der Goes, D.N. Rates of Opioid Misuse, Abuse, and Addiction in Chronic Pain: A Systematic Review and Data Synthesis. Pain 2015, 156, 569–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fendrich, M.; Becker, J.; Hernandez-Meier, J. Psychiatric Symptoms and Recent Overdose among People Who Use Heroin or Other Opioids: Results from a Secondary Analysis of an Intervention Study. Addict. Behav. Rep. 2019, 10, 100212. [Google Scholar] [CrossRef]
- Cucciare, M.A.; Cheung, R.C.; Rongey, C. Treating Substance Use Disorders in Patients with Hepatitis C. Addiction 2015, 110, 1057–1059. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, Y.-H.; Rothman, R.E.; Laeyendecker, O.B.; Kelen, G.D.; Avornu, A.; Patel, E.U.; Kim, J.; Irvin, R.; Thomas, D.L.; Quinn, T.C. Evaluation of the Centers for Disease Control and Prevention Recommendations for Hepatitis C Virus Testing in an Urban Emergency Department. Clin. Infect. Dis. 2016, 62, 1059–1065. [Google Scholar] [CrossRef]
- Ali, M.M.; Sutherland, H.; Rosenoff, E. Comorbid Health Conditions and Treatment Utilization among Individuals with Opioid Use Disorder Experiencing Homelessness. Subst. Use Misuse 2021, 56, 571–574. [Google Scholar] [CrossRef]
- Tori, M.E.; Larochelle, M.R.; Naimi, T.S. Alcohol or Benzodiazepine Co-Involvement With Opioid Overdose Deaths in the United States, 1999–2017. JAMA Netw. Open 2020, 3, e202361. [Google Scholar] [CrossRef] [Green Version]
- Ahrens, K.A.; McBride, C.A.; O’Connor, A.; Meyer, M.C. Medication for Addiction Treatment and Postpartum Health Care Utilization Among Pregnant Persons with Opioid Use Disorder. J. Addict. Med. 2021, 16, 56–64. [Google Scholar] [CrossRef]
- Haight, S.C.; Ko, J.Y.; Tong, V.T.; Bohm, M.K.; Callaghan, W.M. Opioid Use Disorder Documented at Delivery Hospitalization-United States, 1999–2014. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 845–849. [Google Scholar] [CrossRef]
- Jones, H.E.; Arria, A.M.; Baewert, A.; Heil, S.H.; Kaltenbach, K.; Martin, P.R.; Coyle, M.G.; Selby, P.; Stine, S.M.; Fischer, G. Buprenorphine Treatment of Opioid-Dependent Pregnant Women: A Comprehensive Review. Addiction 2012, 107, 5–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Model | AIC | aBIC | χ2 | Entropy | Smallest Class Size (%) |
|---|---|---|---|---|---|
| 1 class | 83,278,912 | 83,279,015 | 16,759,968 (501) | NA | NA |
| 2 class | 75,387,096 | 75,387,312 | 9,191,275 (492) | 0.908 | 46.6% |
| 3 class | 71,463,079 | 71,462,409 | 5,424,310 (481) | 0.934 | 11.7% |
| 4 class | 69,347,569 | 68,348,013 | 3,396,531 (470) | 0.948 | 19.0% |
| 5 class | 68,231,307 | 68,231,865 | 2,326,259 (459) | 0.978 | 10.6% |
| 6 class | 67,675,778 | 67,676,450 | 1,796,618 (450) | 0.963 | 4.5% |
| 7 class | 67,162,510 | 67,163,296 | 1,086,526 (442) | 0.990 | 1.9% |
| 8 class | 66,415,227 | 66,416,127 | 538,386 (432) | 0.952 | 0.6% |
| 9 class | 66,124,289 | 66,125,302 | 307,504 (415) | 0.968 | 1.0% |
| 10 class | 64,841,155 | 65,842,282 | 32,548 (412) | 0.980 | 0.4% |
| Class 1 Chronic Pain | Class 2 Alcohol Use | Class 3 Depression & Pain | Class 4 Psychosis, Liver Disease & Polysubstance Use | Class 5 Pregnancy | |
|---|---|---|---|---|---|
| Class size | 48.9% | 11.0% | 17.1% | 11.1% | 11.9% |
| Class-defining variable | |||||
| Chronic pain | 1.000 | 0.104 | 0.221 | 0.039 | 0.038 |
| Alcohol use | 0.000 | 1.000 | 0.000 | 0.012 | 0.000 |
| Psychoses | 0.006 | 0.031 | 0.034 | 0.322 | 0.001 |
| Depression | 0.000 | 0.158 | 1.000 | 0.022 | 0.009 |
| Liver disease | 0.010 | 0.108 | 0.025 | 0.329 | 0.000 |
| Pregnancy | 0.002 | 0.001 | 0.003 | 0.003 | 1.000 |
| Cocaine use | 0.002 | 0.048 | 0.011 | 0.103 | 0.001 |
| Amphetamine use | 0.001 | 0.015 | 0.007 | 0.085 | 0.001 |
| Class 1 Chronic Pain | Class 2 Alcohol Use | Class 3 Depression & Pain | Class 4 Psychosis, Liver Disease & Polysubstance Use | Class 5 Pregnancy | |
|---|---|---|---|---|---|
| n | 6,477,223 | 1,377,526 | 2,234,701 | 1,288,114 | 1,565,534 |
| Age (median, IQR) | 48 (32–62) | 48 (35–57) | 52 (35–67) | 47 (32–60) | 27 (22–31) |
| Sex | |||||
| Female | 59% | 30% | 67% | 43% | 100% |
| Male | 41% | 70% | 33% | 57% | 0% |
| Payer | |||||
| Medicare | 29% | 19% | 41% | 32% | 1% |
| Medicaid | 25% | 33% | 24% | 32% | 55% |
| Private | 28% | 23% | 24% | 18% | 31% |
| Self-pay | 13% | 21% | 7% | 14% | 9% |
| No charge | 0% | 1% | 0% | 1% | 0% |
| Other | 5% | 4% | 3% | 3% | 3% |
| Median income | |||||
| Top quartile | 39% | 36% | 34% | 40% | 42% |
| 2nd quartile | 27% | 25% | 28% | 26% | 27% |
| 3rd quartile | 20% | 21% | 22% | 20% | 19% |
| 4th quartile | 14% | 19% | 17% | 14% | 12% |
| Urbanicity | |||||
| Central metropolitan | 28% | 34% | 24% | 34% | 39% |
| Fringe metropolitan | 20% | 22% | 22% | 21% | 20% |
| 250–999 K | 22% | 21% | 24% | 21% | 20% |
| 50–250 K | 11% | 10% | 11% | 9% | 9% |
| Micropolitan | 11% | 8% | 12% | 9% | 8% |
| Non-core | 8% | 5% | 7% | 6% | 5% |
| Latent Class | Descriptor | Hospital Admission | In-Hospital Death | ED Charges | |||
|---|---|---|---|---|---|---|---|
| % | OR (95% CI) | Count (per 1000) | OR (95% CI) | Median (USD) | OR a (95% CI) | ||
| Class 1 | Chronic pain | 10.4% | ref. | 1.7 | ref. | $2177 | ref. |
| Class 2 | Alcohol use | 32.9% | 4.38 (4.36–4.40) | 6.5 | 1.98 (1.95–2.00) | $2817 | 1.26 (1.26–1.27) |
| Class 3 | Depression & pain | 37.0% | 5.24 (5.22–5.27) | 6.7 | 2.01 (1.99–2.04) | $2645 | 1.22 (1.22–1.22) |
| Class 4 | Psychosis, liver disease & polysubstance use | 37.1% | 5.33 (5.31–5.36) | 18.9 | 3.4 (3.39–3.48) | $2881 | 1.29 (1.29–1.30) |
| Class 5 | Pregnancy | 12.5% | 1.24 (1.24–1.25) | <0.1 | 0.00 (0.00–0.00) | $2605 | 1.07 (1.07–1.08) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chhabra, N.; Smith, D.L.; Maloney, C.M.; Archer, J.; Sharma, B.; Thompson, H.M.; Afshar, M.; Karnik, N.S. The Identification of Subphenotypes and Associations with Health Outcomes in Patients with Opioid-Related Emergency Department Encounters Using Latent Class Analysis. Int. J. Environ. Res. Public Health 2022, 19, 8882. https://doi.org/10.3390/ijerph19148882
Chhabra N, Smith DL, Maloney CM, Archer J, Sharma B, Thompson HM, Afshar M, Karnik NS. The Identification of Subphenotypes and Associations with Health Outcomes in Patients with Opioid-Related Emergency Department Encounters Using Latent Class Analysis. International Journal of Environmental Research and Public Health. 2022; 19(14):8882. https://doi.org/10.3390/ijerph19148882
Chicago/Turabian StyleChhabra, Neeraj, Dale L. Smith, Caitlin M. Maloney, Joseph Archer, Brihat Sharma, Hale M. Thompson, Majid Afshar, and Niranjan S. Karnik. 2022. "The Identification of Subphenotypes and Associations with Health Outcomes in Patients with Opioid-Related Emergency Department Encounters Using Latent Class Analysis" International Journal of Environmental Research and Public Health 19, no. 14: 8882. https://doi.org/10.3390/ijerph19148882