
Initial Surgical Strategy for the Treatment of Type A Acute Aortic Dissection: Does Proximal or Distal Extension of the Aortic Resection Influence the Outcomes?

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients’ Population
2.2. Patient Selection and Study Design
2.3. Surgical Techniques
2.4. Follow-Up
2.5. Analyzed Variables
2.6. Statistics
3. Results
3.1. Intraoperative Data
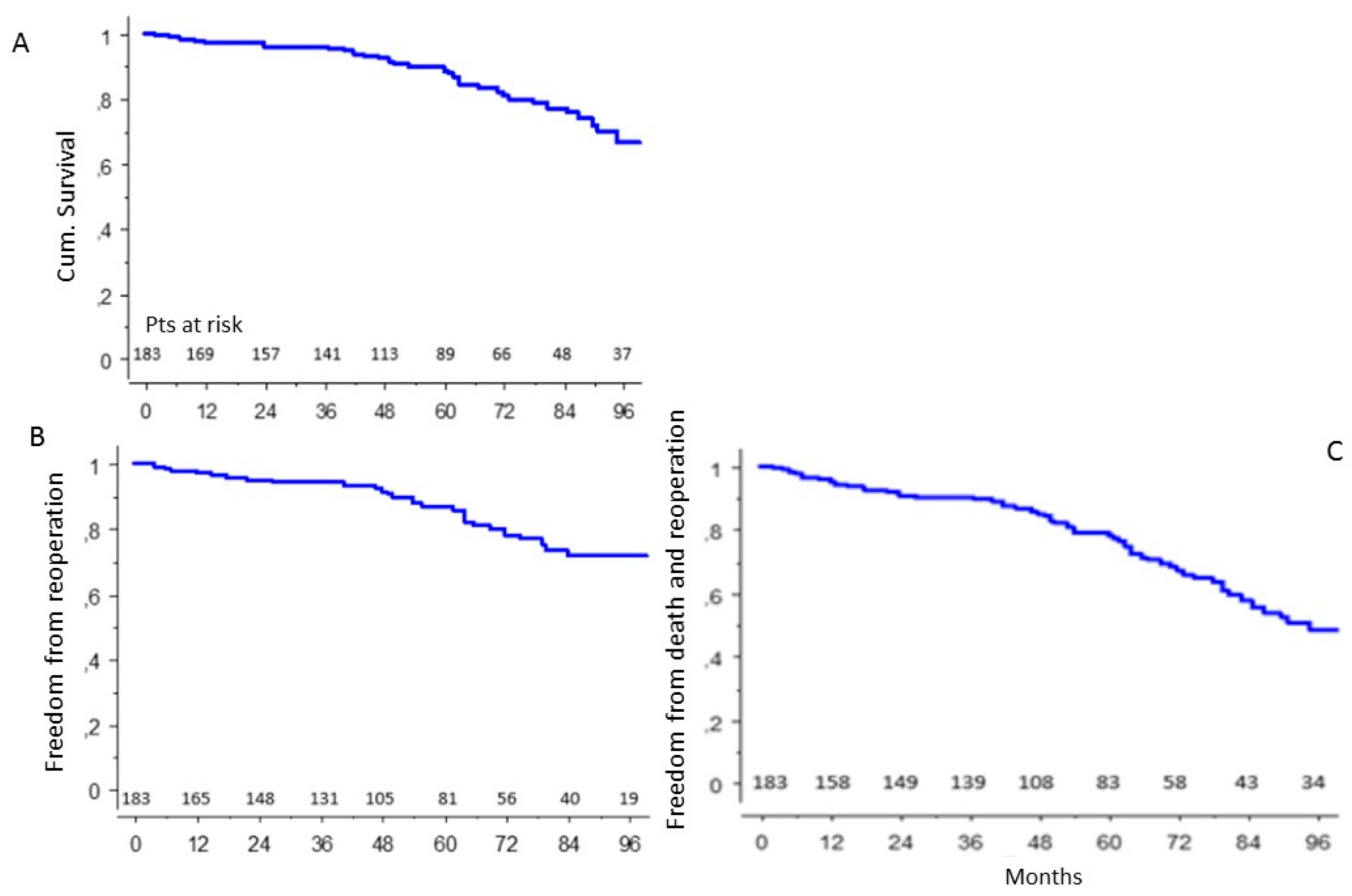
3.2. Long-Term Results
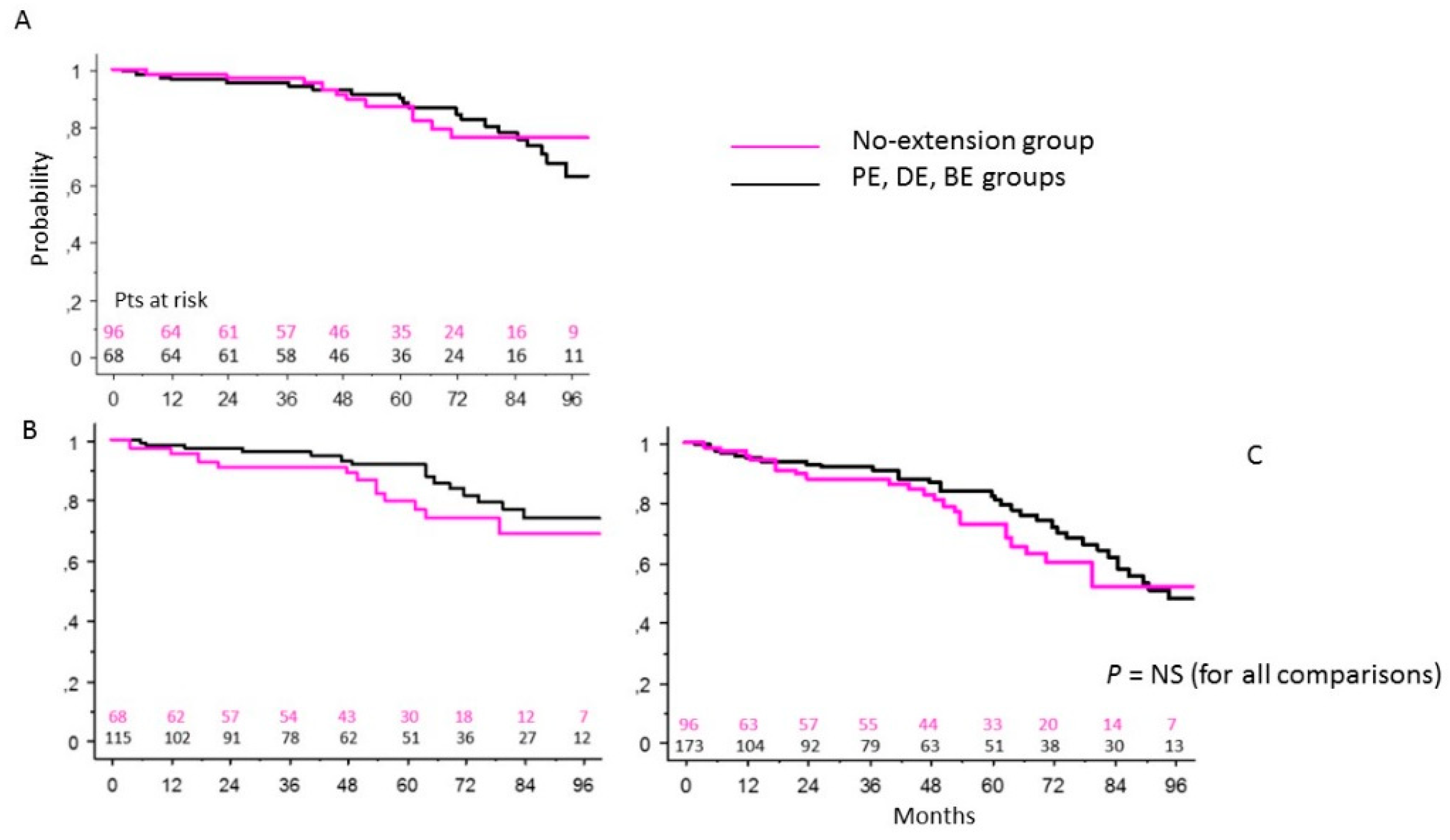
3.3. NE Patients Group vs. Extended Intervention (Proximal, Distal or Both) Groups of Patients
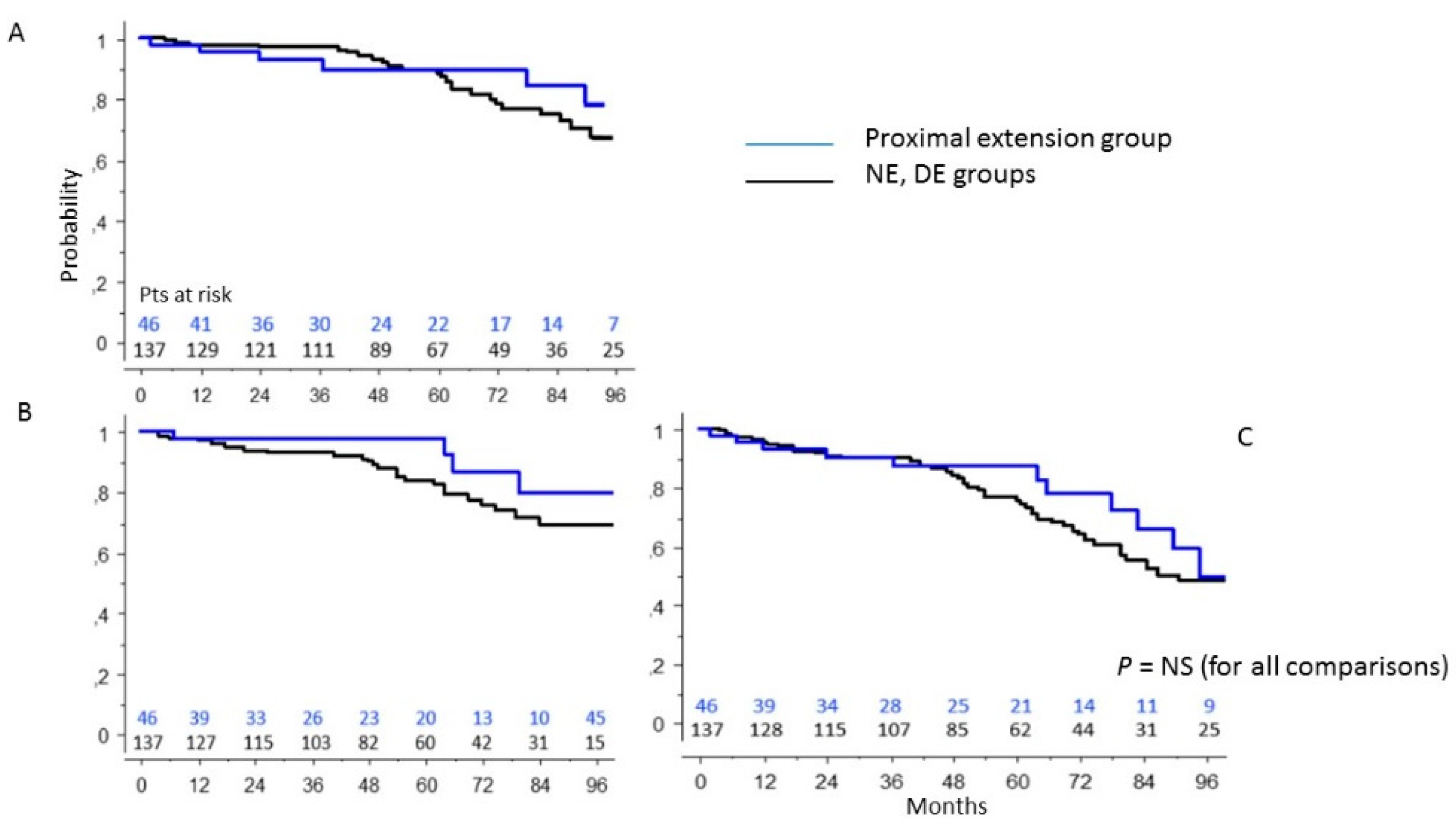
3.4. PE Group vs. Patients’ Population without Aortic Root Surgery
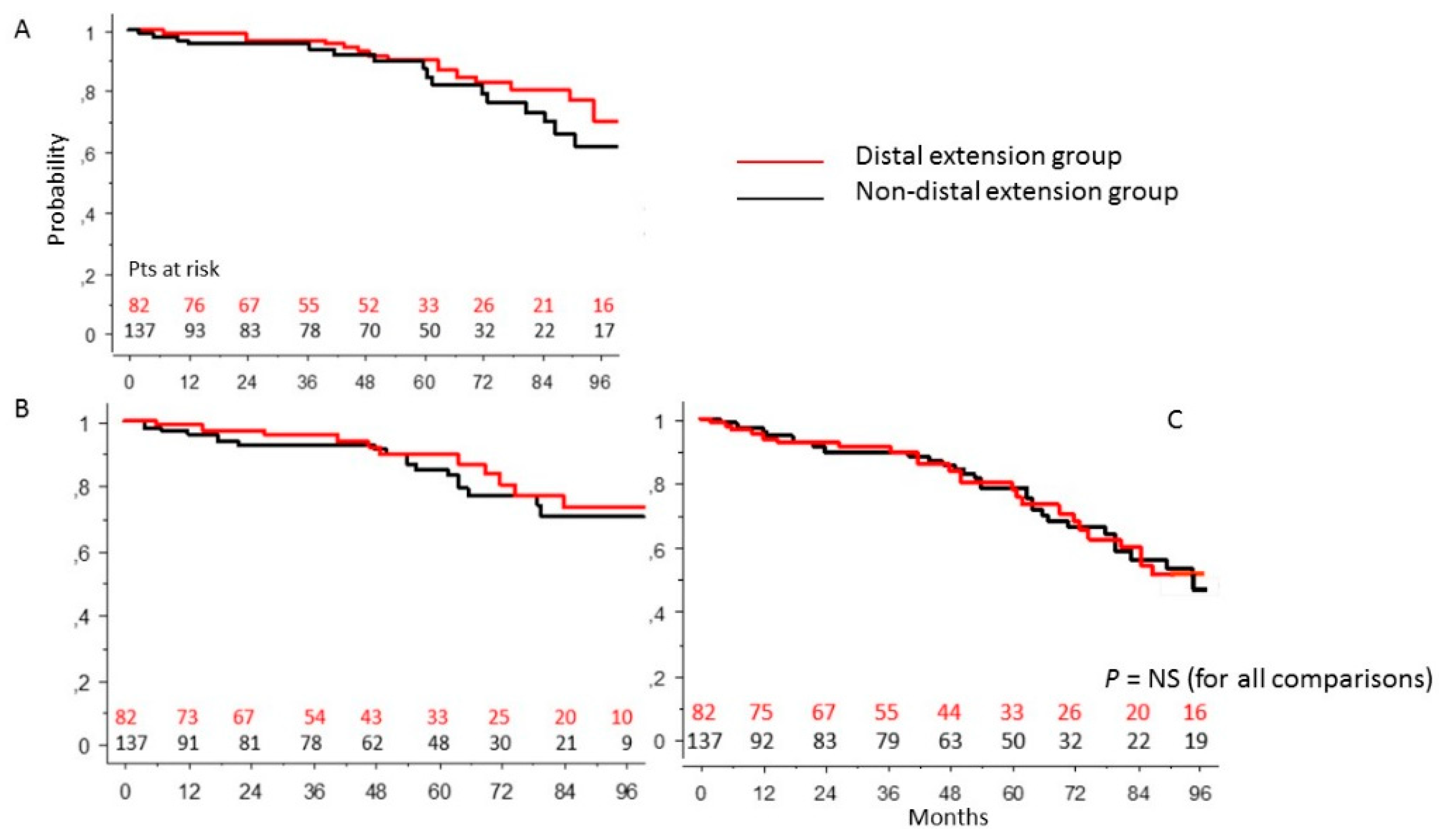
3.5. DE Group vs. Non-Arch Surgery Patients’ Population
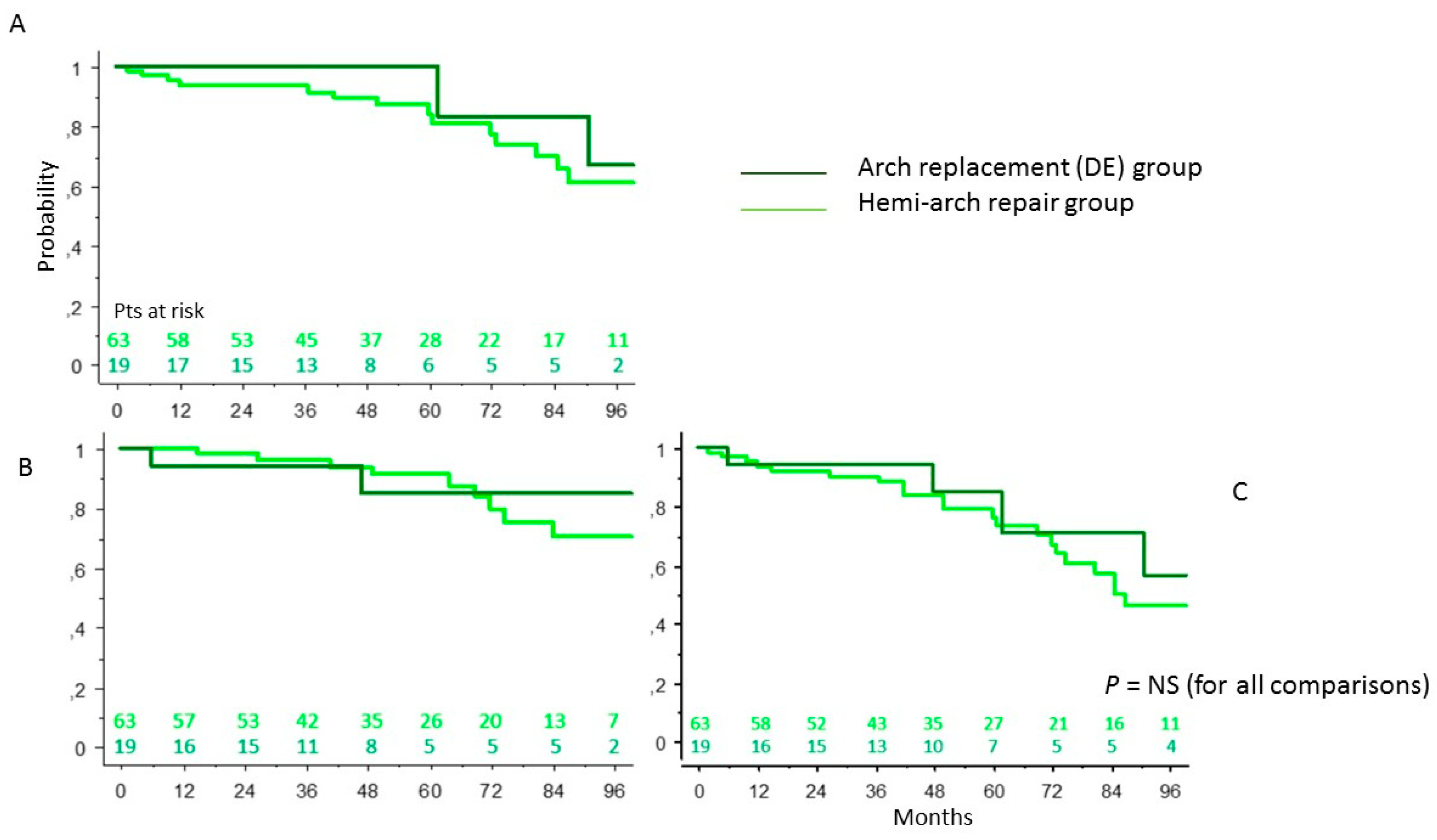
3.6. DE Group: Conservative Surgery vs. Radical Surgery of the Aortic Arch
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Trimarchi, S.; Eagle, K.A.; Nienaber, C.A.; Rampoldi, V.; Jonker, F.H.; De Vincentiis, C.; Frigiola, A.; Menicanti, L.; Tsai, T.; Froehlich, J.; et al. Role of age in acute type A aortic dissection outcome: Report from the International Registry of Acute Aortic Dissection (IRAD). J. Thorac. Cardiovasc. Surg. 2010, 140, 784–789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, T.T.; Fattori, R.; Trimarchi, S.; Isselbacher, E.; Myrmel, T.; Evangelista, A.; Hutchison, S.; Sechtem, U.; Cooper, J.V.; Smith, D.E.; et al. International Registry of Acute Aortic Dissection. Long-term survival in patients presenting with type A acute aortic 48 dissection: Insights from the international registry of acute aortic dissection. Circulation 2006, 114, I350–I1356. [Google Scholar] [PubMed] [Green Version]
- Chiu, P.; Miller, D.C. Evolution of surgical therapy for Stanford acute type A aortic dissection. Ann. Cardiothorac. Surg. 2016, 5, 275–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirsch, M.; Legras, A.; Bruzzi, M.; Louis, N. Fate of the distal aorta after surgical repair of acute DeBakey type I aortic dissection: A review. Arch. Cardiovasc. Dis. 2011, 104, 125–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmerman, K.P.; Oderich, G.; Pochettino, A.; Hanson, K.T.; Habermann, E.B.; Bower, T.C.; Gloviczki, P.; De Martino, R.R. Improving mortality trends for hospitalization of aortic dissection in the National Inpatient Sample. J. Vasc. Surg. 2016, 64, 606–615.e1. [Google Scholar] [CrossRef] [Green Version]
- Nardi, P.; Scafuri, A.; Pellegrino, A.; Bassano, C.; Zeitani, J.; Bertoldo, F.; De Peppo, A.P.; Chiariello, L. Surgery for type A aortic dissection: Long-term results and risk factor analysis. G. Ital. Cardiol. 2007, 8, 580–585. [Google Scholar]
- Geirsson, A.; Bavaria, J.E.; Swarr, D.; Keane, M.; Woo, Y.J.; Szeto, W.Y.; Pochettino, A. Fate of the Residual Distal and Proximal Aorta After Acute Type A Dissection Repair Using a Contemporary Surgical Reconstruction Algorithm. Ann. Thorac. Surg. 2007, 84, 1955–1964. [Google Scholar] [CrossRef]
- Gorlitzer, M.; Weiss, G.; Meinhart, J.; Waldenberg, F.; Thalmann, M.; Folkmann, S.; Moidl, R.; Grabenwoeger, M. Fate of false lume after combined surgical and endovascular repair treating Stanford Type A aortic dissection. Ann. Thorac. Surg. 2010, 89, 794–799. [Google Scholar] [CrossRef]
- Nardi, P.; Vacirca, S.R.; Russo, M.; Colella, D.F.; Bassano, C.; Scafuri, A.; Pellegrino, A.; Melino, G.; Ruvolo, G. Cold crystalloid versus warm blood cardioplegia in patients undergoing aortic valve replacement. J. Thorac. Dis. 2018, 10, 1490–1499. [Google Scholar] [CrossRef] [Green Version]
- Zierer, A.; Risteski, P.; El-Sayed Ahmad, A.; Moritz, A.; Diegeler, A.; Urbanski, P.P. The impact of unilateral versus bilateral antero-grade cerebral perfusion on surgical outcomes after aortic arch replacement: A propensity-matched analysis. J. Thorac. Cardiovasc. Surg. 2014, 147, 1212–1217. [Google Scholar] [CrossRef] [Green Version]
- Conzelmann, L.O.; Weigang, E.; Mehlhorn, U.; Abugameh, A.; Hoffmann, I.; Blettner, M.; Etz, C.D.; Czerny, M.; Vahl, C.F. Mortality in patients with acute aortic dissection type A: Analysis of pre- and intraoperative risk factors from the German Registry for Acute Aortic Dissection Type A (GERAADA). Eur. J. Cardio-Thorac. Surg. 2015, 49, e44–e52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bassano, C.; Buioni, D.; Scafuri, A.; Nardi, P.; Pisano, C.; Bertoldo, F.; Ruvolo, G. Surgical “elephant trunk” arch replacement with a branched arch prosthesis: Two alternative operative techniques. Pol. J. Thorac. Cardiovasc. Surg. 2021, 18, 67–70. [Google Scholar] [CrossRef] [PubMed]
- Bovio, E.; Mvondo, C.M.; Chiariello, G.A.; Bassano, C. Single cannulation, bilateral brain perfusion. Ann. Thorac. Surg. 2013, 95, 1138–1139. [Google Scholar] [CrossRef] [PubMed]
- Mvondo, C.M.; Bovio, E.; Chiariello, L.; Bassano, C. Bilateral Cerebral Perfusion via Right Axillary Artery Cannulation Alone in Aortic Arch Surgery. Thorac. Cardiovasc. Surg. 2013, 61, 584–586. [Google Scholar] [CrossRef]
- Bassano, C.; De Matteis, G.M.; Nardi, P.; Buratta, M.M.; Zeitani, J.; De Paulis, R.; Chiariello, L. Mid-term follow-up of aortic root re-modelling compared to Bentall operation. Eur. J. Cardiothorac. Surg. 2001, 19, 601–605. [Google Scholar] [CrossRef] [Green Version]
- Nardi, P.; Bassano, C.; Pisano, C.; Altieri, C.; Ferrante, M.; Greci, M.; Buioni, D.; Bertoldo, F.; Farinaccio, A.; Ruvolo, G. The effects of DeBakey type acute aortic dissection and preoperative peripheral and cardiac malperfusion on the outcomes after surgical repair. Pol. J. Thorac. Cardiovasc. Surg. 2021, 18, 1–7. [Google Scholar] [CrossRef]
- Shi, E.; Gu, T.; Yu, Y.; Yu, L.; Wang, C.; Fang, Q.; Zhang, Y. Early and midterm outcomes of hemiarch repair combined with stented elephant trunk in the management of acute DeBakey type I aortic dissection: Comparison with total arch repair. J. Thorac. Cardiovasc. Surg. 2014, 148, 2125–2131. [Google Scholar] [CrossRef] [Green Version]
- Westaby, S.; Saito, S.; Katsumata, T. Acute type A dissection: Conservative methods provide consistently low mortality. Ann. Thorac. Surg. 2002, 73, 707–713. [Google Scholar] [CrossRef]
- Urbanski, P.; Siebel, A.; Zacher, M.; Robert, W. Hacker. Is Extended Aortic Replacement in Acute Type A Dissection Justifiable? Ann. Thorac. Surg. 2003, 75, 525–529. [Google Scholar] [CrossRef]
- Di Eusanio, M.; Berretta, P.; Cefarelli, M.; Jacopo, A.; Murana, G.; Castrovinci, S.; Di Bartolomeo, R. Total Arch Replacement Versus More Conservative Management in Type A Acute Aortic Dissection. Ann. Thorac. Surg. 2015, 100, 88–94. [Google Scholar] [CrossRef]
- Kazui, T.; Washiyama, N.; Muhammad, B.A.H.; Terada, H.; Yamashita, K.; Takinami, M.; Tamiya, Y. Extended total arch replacement for acute type a aortic dissection: Experience with seventy patients. J. Thorac. Cardiovasc. Surg. 2000, 119, 558–565. [Google Scholar] [CrossRef] [Green Version]
- Di Eusanio, M.; Castrovinci, S.; Tian, D.H.; Folesani, G.; Cefarelli, M.; Pantaleo, A.; Murana, G.; Berretta, P.; Yan, T.D.; Bartolomeo, R.D. Antegrade stenting of the descending thoracic aorta during DeBakey type 1 acute aortic dissection repair. Eur. J. Cardio-Thorac. Surg. 2014, 45, 967–975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uchida, N.; Shibamura, H.; Katayama, A.; Shimada, N.; Sutoh, M. Total arch replacement with an open stent graft for acute type A aortic dissection: Fate of the false lumen. Eur. J. Cardio-Thorac. Surg. 2009, 35, 83–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fattori, R.; Bacchi-Reggiani, L.; Bertaccini, P.; Napoli, G.; Fusco, F.; Longo, M.; Pierangeli, A.; Gavelli, G. Evolution of aortic dissection after surgical repair. Am. J. Cardiol. 2000, 86, 868–872. [Google Scholar] [CrossRef]
- Zierer, A.; Voeller, R.K.; Hill, K.E.; Kouchoukos, N.T.; Damiano, R.J.; Moon, M.R. Aortic Enlargement and Late Reoperation After Repair of Acute Type a Aortic Dissection. Ann. Thorac. Surg. 2007, 84, 479–487. [Google Scholar] [CrossRef]
- Khaladj, N.; Shrestha, M.; Meck, S.; Peterss, S.; Kamiya, H.; Kallenbach, K.; Winterhalter, M.; Hoy, L.; Haverich, A.; Hagl, C. Hypothermic circulatory arrest with selective antegrade cerebral perfusion in ascending aortic and aortic arch surgery: A risk factor analysis for adverse outcome in 501 patients. J. Thorac. Cardiovasc. Surg. 2008, 135, 908–914. [Google Scholar] [CrossRef] [Green Version]
- Westaby, S.; Katsumata, T.; Vaccari, G. Arch and descending aortic aneurysms: Influence of perfusion technique on neurological outcome1. Eur. J. Cardio-Thorac. Surg. 1999, 15, 180–185. [Google Scholar] [CrossRef] [Green Version]
- Berretta, P.; Patel, H.J.; Gleason, T.J.; Sundt, T.M.; Myrmel, T.; Desai, N.; Korach, A.; Panza, A.; Bavaria, J.; Khoynezhad, A.; et al. IRAD expe-rience on surgical type A acute dissection patients: Results and predictors of mortality. Ann. Cardiothorac. Surg. 2016, 5, 346–351. [Google Scholar] [CrossRef] [Green Version]
- Rylski, B.; Suedkamp, M.; Beyersdorf, F.; Nitsch, B.; Hoffmann, I.; Blettner, M.; Weigang, E. Outcome after surgery for acute aortic dissection type A in patients over 70 years: Data analysis from the German Registry for Acute Aortic Dissection Type A (GERAADA). Eur. J. Cardio-Thorac. Surg. 2011, 40, 435–440. [Google Scholar] [CrossRef] [Green Version]
- Komatsu, K.; Takano, T.; Terasaki, T.; Wada, Y.; Seto, T.; Fukui, D.; Amano, J. Surgical Outcomes of Acute Type A Aortic Dissection in Elderly Patients. Ann. Thorac. Surg. 2014, 97, 1576–1581. [Google Scholar] [CrossRef] [Green Version]
- Vendramin, I.; Lechiancole, A.; Piani, D.; Sponga, S.; Di Nora, C.; Muser, D.; Bortolotti, U.; Livi, U. An Integrated Approach for Treatment of Acute Type a Aortic Dissection. Medicina 2021, 57, 1155. [Google Scholar] [CrossRef] [PubMed]
- Erbel, R.; Aboyans, V.; Boileau, C.; Bossone, E.; Bartolomeo, R.D.; Eggebrecht, H.; Evangelista, A.; Falk, V.; Frank, H.; Gaemperli, O.; et al. ESC Committee for Practice Guidelines. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur. Heart J. 2014, 35, 2873–2926. [Google Scholar] [PubMed] [Green Version]
- Pape, L.A.; Tsai, T.T.; Isselbacher, E.M.; Oh, J.K.; O’Gara, P.T.; Evangelista, A.; Fattori, R.; Meinhardt, G.; Trimarchi, S.; Bossone, E.; et al. Aortic diameter > or = 5.5 cm is not a good predictor of type A aortic dis-section: Observations from the International Registry of Acute Aortic Dissection (IRAD). Circulation 2007, 116, 1120–1127. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | |
|---|---|
| Age (years), mean ± SD | 63.1 ± 12.8 |
| Age > 75 years, n (%) | 48 (17) |
| Female, n (%) | 78 (29) |
| BMI (kg/m2), mean ± SD | 27.5 ± 5.1 |
| BSA (m2), mean ± SD | 1.96 ± 0.23 |
| Hypertension, n (%) | 238 (88.5) |
| Family history, n (%) | 29 (10.8) |
| Diabetes, n (%) | 17 (6.3) |
| Tobacco use, n (%) | 76 (28.3) |
| Obesity, n (%) | 63 (23.4) |
| Coronary artery disease, n (%) | 25 (9.3) |
| Previous cardiac surgery, n (%) | 17 (6.3) |
| Preoperative IOT, n (%) | 40 (14.9) |
| Preoperative neurological damage, n (%) | 35 (13) |
| Diameter of the ascending aorta (mm), mean ± SD | 54.2 ± 10.4 |
| Variable | No Extension (NE) (n = 96) | Proximal Extension (PE) (n = 41) | Distal Extension (DE) (n = 112) | Bilateral Extension (BE) (n = 20) | p-Value |
|---|---|---|---|---|---|
| Age (years), mean ± SD | 65.2 ± 11.9 | 55.3 ± 14.9 | 65.1 ± 10.9 | 57.4 ± 14.6 | 0.0001 |
| Age > 75 years, n (%) | 22 (23) | 2 (5) | 24 (21) | 0 (0) | 0.0001 |
| Female, n (%) | 38 (39.6) | 8 (19.5) | 29 (25.9) | 3 (15) | 0.024 |
| BMI (kg/m2), mean ± SD | 26.7 ± 4.5 | 27.2 ± 4.5 | 28.3 ± 5.7 | 28.3 ± 4.2 | 0.114 |
| BSA (m2), mean ± SD | 1.89 ± 0.20 | 2.0 ± 0.25 | 1.99 ± 0.24 | 2.02 ± 0.18 | 0.002 |
| Hypertension, n (%) | 86 (89.6) | 35 (84.4) | 99 (88.4) | 18 (90) | 0.908 |
| Family history, n (%) | 14 (14.6) | 5 (12.2) | 9 (8) | 1 (5) | 0.376 |
| Diabetes, n (%) | 7 (7.3) | 2 (4.9) | 6 (5.3) | 2 (10) | 0.818 |
| Tobacco use, n (%) | 30 (31.2) | 13 (31.7) | 28 (25) | 5 (25) | 0.716 |
| Obesity, n (%) | 16 (16.7) | 11 (26.8) | 30 (26.8) | 6 (30) | 0.244 |
| Coronary artery disease, n (%) | 8 (8.3) | 4 (9.7) | 9 (8) | 4 (20) | 0.385 |
| Previous cardiac surgery, n (%) | 5 (5.2) | 5 (12.2) | 7 (6.2) | 0 (0) | 0.268 |
| Preoperative IOT, n (%) | 11 (11.5) | 8 (19.5) | 18 (16.1) | 3 (15) | 0.634 |
| Preoperative neurological damage, n (%) | 10 (10.4) | 4 (9.8) | 16 (14.3) | 5 (25) | 0.314 |
| Variable | Hemi-Arch (n = 92) | Aortic Arch (n = 40) | p-Value |
|---|---|---|---|
| Age (years), mean ± SD | 65.5 ± 10.9 | 60.2 ± 13.1 | 0.016 |
| Age > 75 years, n (%) | 19 (20) | 5 (12) | 0.246 |
| Female, n (%) | 24 (26.1) | 8 (20) | 0.453 |
| BMI (kg/m2), mean ± SD | 28.2 ± 5.8 | 28.5 ± 4.8 | 0.768 |
| BSA (m2), mean ± SD | 1.99 ± 0.2 | 2.00 ± 0.2 | 0.806 |
| Hypertension, n (%) | 78 (84.8) | 38 (95) | 0.129 |
| Family history, n (%) | 7 (7.6) | 3 (7.5) | 0.983 |
| Diabetes, n (%) | 5 (5.4) | 3 (7.5) | 0.648 |
| Tobacco use, n (%) | 22 (23.9) | 11 (27.5) | 0.662 |
| Obesity, n (%) | 23 (25) | 13 (32.5) | 0.414 |
| Coronary artery disease, n (%) | 10 (10.9) | 3 (7.5) | 0.550 |
| Previous cardiac surgery, n (%) | 6 (6.5) | 1 (2.5) | 0.343 |
| Preoperative OTI, n (%) | 12 (13) | 9(22.5) | 0.169 |
| Preoperative neurological damage, n (%) | 14 (15.2) | 7 (17.5) | 0.716 |
| Variable | |
|---|---|
| Axillary cannulation, n (%) | 134 (49.8) |
| Femoral cannulation, n (%) | 112 (41.6) |
| Central cannulation, n (%) | 23 (8.6) |
| Monolateral perfusion, n (%) | 82 (30.5) |
| Bilateral perfusion, n (%) | 80 (29.7) |
| CPB time (min), n (%) | 169 ± 84.8 |
| X-Clamp time (min), mean ± SD | 97 ± 49.4 |
| Circulatory arrest time (min), mean ± SD | 39 ± 31.6 |
| Circulatory arrest temperature (°C), mean ± SD | 27 ± 2.4 |
| Concomitant procedures: | |
| Aortic valve replacement, n (%) | 17 (6.3) |
| CABG, n (%) | 22 (8.2) |
| Variable | No Extension (n = 96) | Proximal Extension (n = 41) | Distal Extension (n = 112) | Bilateral Extension (n = 20) | p-Value |
|---|---|---|---|---|---|
| Axillary cannulation, n (%) | 25 (26.0) | 17 (41.5) | 78 (69.6) | 14 (70.0) | 0.0001 |
| Femoral cannulation, n (%) | 56 (58.3) | 20 (48.8) | 30 (26.8) | 6 (30.0) | 0.0001 |
| Central cannulation, n (%) | 15 (15.6) | 4 (9.7) | 4 (3.6) | 0 (0) | 0.009 |
| Monolateral perfusion, n (%) | 14 (14.6) | 8 (19.5) | 50 (44.6) | 10 (50.0) | 0.0001 |
| Bilateral perfusion, n (%) | 5 (5.2) | 3 (7.3) | 62 (55.3) | 10 (50.0) | 0.0001 |
| CPB time (min), n (%) | 107 ± 53 | 195 ± 91.2 | 196 ± 74.4 | 250 ± 76.1 | 0.0001 |
| X-Clamp time (min), mean ± SD | 65 ± 30.1 | 127 ± 43.0 | 102 ± 49.3 | 151 ± 43.1 | 0.0001 |
| Circulatory arrest time (min), mean ± SD | 17 ± 17.6 | 22 ± 16.3 | 46 ± 33.6 | 37 ± 24.4 | 0.0001 |
| Circulatory arrest temperature (°C), mean ± SD | 28 ± 3.0 | 27 ± 3.1 | 27 ± 2.1 | 26 ± 1.9 | 0.038 |
| Concomitant procedures: | |||||
| Aortic valve replacement, n (%) | 11 (10.4) | 0 (0) | 6 (53.6) | 0 (0) | 0.036 |
| CABG, n (%) | 4 (4.2) | 8 (19.5) | 7 (6.2) | 3 (15.0) | 0.012 |
| Variable | Hemi-Arch (n = 92) | Aortic Arch (n = 40) | p-Value |
|---|---|---|---|
| Axillary Cannulation, n (%) | 63 (68.5) | 29 (72.5) | 0.644 |
| Femoral Cannulation, n (%) | 25 (27.2) | 11 (27.5) | 0.969 |
| Central Cannulation, n (%) | 4 (4.3) | 0 (0) | 0.180 |
| Monolateral Perfusion, n (%) | 39 (42.4) | 21 (52.5) | 0.284 |
| Bilateral Perfusion, n (%) | 53 (57.6) | 19 (47.5) | 0.284 |
| CPB time (min), n (%) | 183 ± 64.2 | 254 ± 80.9 | 0.0001 |
| X-Clamp time (min), mean ± SD | 94 ± 40.7 | 146 ± 55.5 | 0.0001 |
| Circulatory Arrest Time (min), mean ± SD | 32 ± 19.6 | 76 ± 36.3 | 0.0001 |
| Concomitant procedures: | |||
| Aortic valve replacement, n (%) | 5 (5.4) | 1 (2.5) | 0.457 |
| CABG, n (%) | 8 (8.7) | 2 (5.0) | 0.461 |
| Variable | |
|---|---|
| Mortality, n (%): | 86 (32.0) |
| Intraoperative, n (%) | 23 (26.7) |
| Postoperative, n (%) | 63 (73.3) |
| Postoperative causes of mortality: | |
| MOF, n (%) | 29 (10.8) |
| LCOS, n (%) | 12 (4.5) |
| Septic shock, n (%) | 11 (4.1) |
| Coma, n (%) | 2 (0.7) |
| Other, n (%) | 9 (3.3) |
| Permanent neurological damage, n (%) | 28 (10.4) |
| Transitory neurological damage, n (%) | 17 (6.3) |
| Organ ischemia, n (%) | 7 (2.6) |
| Respiratory failure, n (%) | 75 (27.9) |
| Acute kidney Injury, n (%) | 49 (18.2) |
| Variable | No Extension (n = 96) | Proximal Extension (n = 41) | Distal Extension (n = 112) | Bilateral Extension (n = 20) | p-Value |
|---|---|---|---|---|---|
| Mortality, n (%) | 28 (29.1) | 8 (19.5) | 43 (38.4) | 7 (35.0) | 0.140 |
| Intraoperative, n (%) | 5 (17.9) | 2 (25) | 12 (27.9) | 4 (20.0) | 0.089 |
| Postoperative, n (%) | 23 (82.1) | 6 (75) | 31 (72.1) | 3 (80) | 0.254 |
| Postoperative causes of mortality: | |||||
| MOF, n (%) | 11 (11.5) | 2 (4.9) | 14 (12.5) | 2 (10.0) | 0.542 |
| LCO, n (%) | 6 (6.2) | 2 (4.9) | 4 (3.6) | 0 (0) | 0.666 |
| Septic Shock, n (%) | 3 (3.1) | 2 (4.9) | 6 (5.4) | 0 (0) | 0.653 |
| Coma, n (%) | 1 (1.0) | 0 (0) | 1 (0.9) | 0 (0) | 0.899 |
| Other, n (%) | 2 (2.1) | 0 (0) | 6 (5.4) | 1 (5.0) | 0.273 |
| Permanent neurological injury, n (%) | 13 (13.5) | 3 (7.3) | 10 (8.9) | 2 (10.0) | 0.660 |
| Transitory neurological injury, n (%) | 5 (5.2) | 2 (4.9) | 10 (8.9) | 0 (0) | 0.388 |
| Organ ischemia, n (%) | 2 (2.1) | 2 (4.9) | 3 (2.7) | 0 (0) | 0.729 |
| Respiratory failure, n (%) | 30 (31.2) | 9 (21.9) | 32 (28.6) | 4 (20.0) | 0.607 |
| Acute kidney Injury, n (%) | 17 (17.7) | 4 (9.8) | 24 (21.4) | 4 (20.0) | 0.274 |
| Variable | Emiarch (n = 92) | Aortic Arch (n = 40) | p-Value |
|---|---|---|---|
| Mortality, n (%) | 29 (31.5) | 21 (52.5) | 0.022 |
| Intraoperative, n (%) | 7 (24.1) | 9 (42.9) | 0.013 |
| Postoperative, n (%) | 22 (75.9) | 12 (57.1) | 0.179 |
| Postoperative causes of mortality: | |||
| MOF, n (%) | 13 (14.1) | 3 (7.5) | 0.438 |
| LCO, n (%) | 3 (3.3) | 1 (2.5) | 0.937 |
| Septic Shock, n (%) | 4 (4.3) | 2 (5) | 0.707 |
| Coma, n (%) | 1 (1.1) | 0 (0) | 0.544 |
| Other, n (%) | 1 (1.1) | 6 (15) | 0.000 |
| Permanent neurological injury, n (%) | 11 (12) | 1 (2.5) | 0.139 |
| Transitory neurological injury, n (%) | 7 (7.6) | 3 (7.5) | 0.768 |
| Organ ischemia, n (%) | 2 (2.2) | 1 (2.5) | 0.772 |
| Respiratory failure, n (%) | 28 (30.4) | 8 (20) | 0.500 |
| Acute kidney Injury, n (%) | 23 (25) | 5 (12.5) | 0.242 |
| Variable | Odds Ratio | CI 95% | p-Value |
|---|---|---|---|
| Age a | 1.04 | 1.01—1.08 | 0.009 |
| CPB a | 1.01 | 1.003—1.02 | 0.006 |
| Preoperative OTI | 3.40 | 1.19—9.64 | 0.022 |
| Groups | |
|---|---|
| General population | 16.9% |
| NE | 20.3% |
| PE | 8.7% |
| DE | 12.6% |
| BE | 0% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bassano, C.; Pugliese, M.; Mve Mvondo, C.; Pisano, C.; Nardi, P.; Buioni, D.; Bertoldo, F.; Scognamiglio, M.; Salvati, A.C.; Altieri, C.; et al. Initial Surgical Strategy for the Treatment of Type A Acute Aortic Dissection: Does Proximal or Distal Extension of the Aortic Resection Influence the Outcomes? Int. J. Environ. Res. Public Health 2022, 19, 8878. https://doi.org/10.3390/ijerph19148878
Bassano C, Pugliese M, Mve Mvondo C, Pisano C, Nardi P, Buioni D, Bertoldo F, Scognamiglio M, Salvati AC, Altieri C, et al. Initial Surgical Strategy for the Treatment of Type A Acute Aortic Dissection: Does Proximal or Distal Extension of the Aortic Resection Influence the Outcomes? International Journal of Environmental Research and Public Health. 2022; 19(14):8878. https://doi.org/10.3390/ijerph19148878
Chicago/Turabian StyleBassano, Carlo, Marta Pugliese, Charles Mve Mvondo, Calogera Pisano, Paolo Nardi, Dario Buioni, Fabio Bertoldo, Mattia Scognamiglio, Alessandro C. Salvati, Claudia Altieri, and et al. 2022. "Initial Surgical Strategy for the Treatment of Type A Acute Aortic Dissection: Does Proximal or Distal Extension of the Aortic Resection Influence the Outcomes?" International Journal of Environmental Research and Public Health 19, no. 14: 8878. https://doi.org/10.3390/ijerph19148878