
A Systematic Review of Internet-Based Interventions for the Prevention and Self-Management of Cardiovascular Diseases among People of African Descent


Abstract
:1. Introduction
2. Materials and Methods
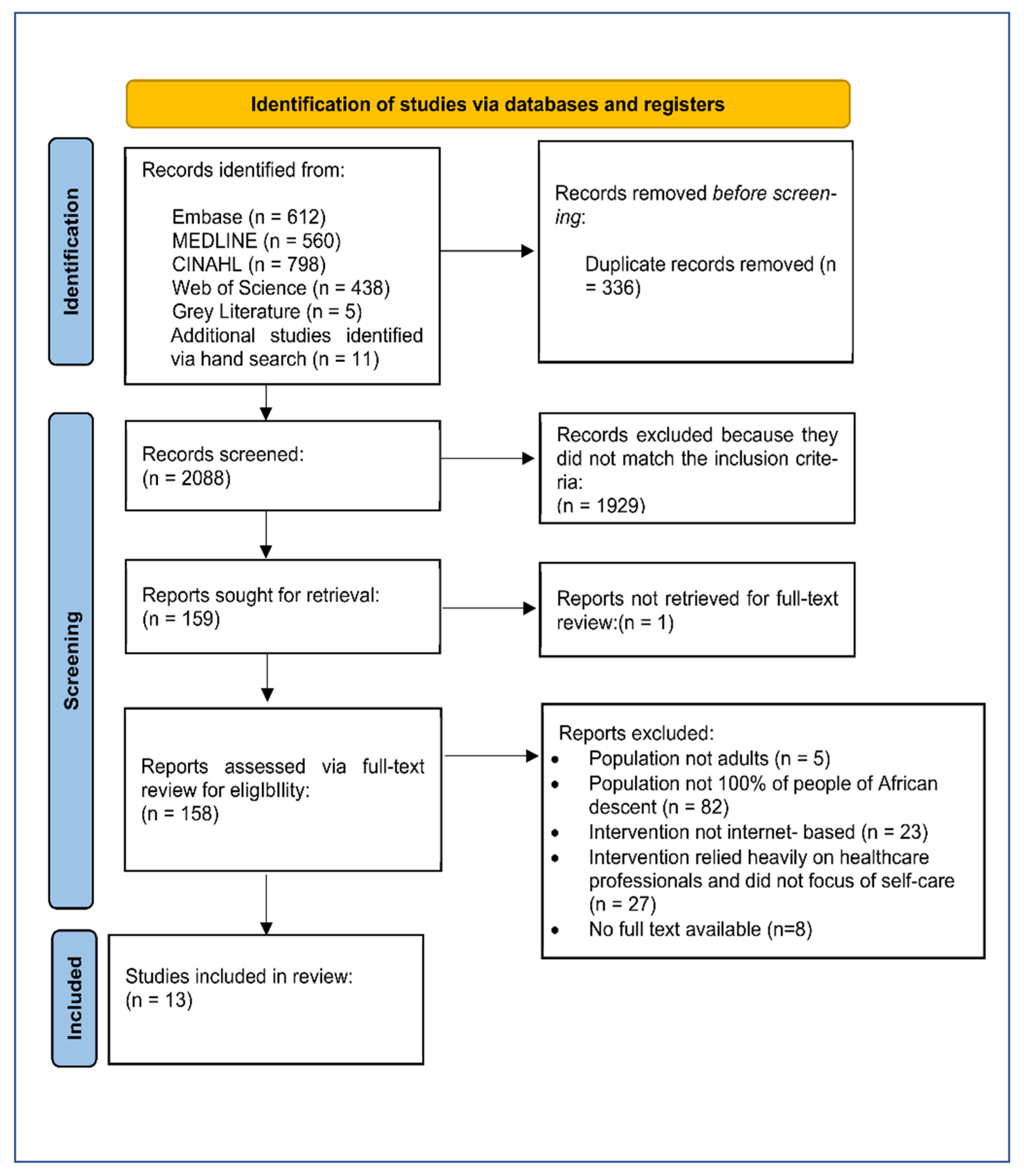
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction and Analyses
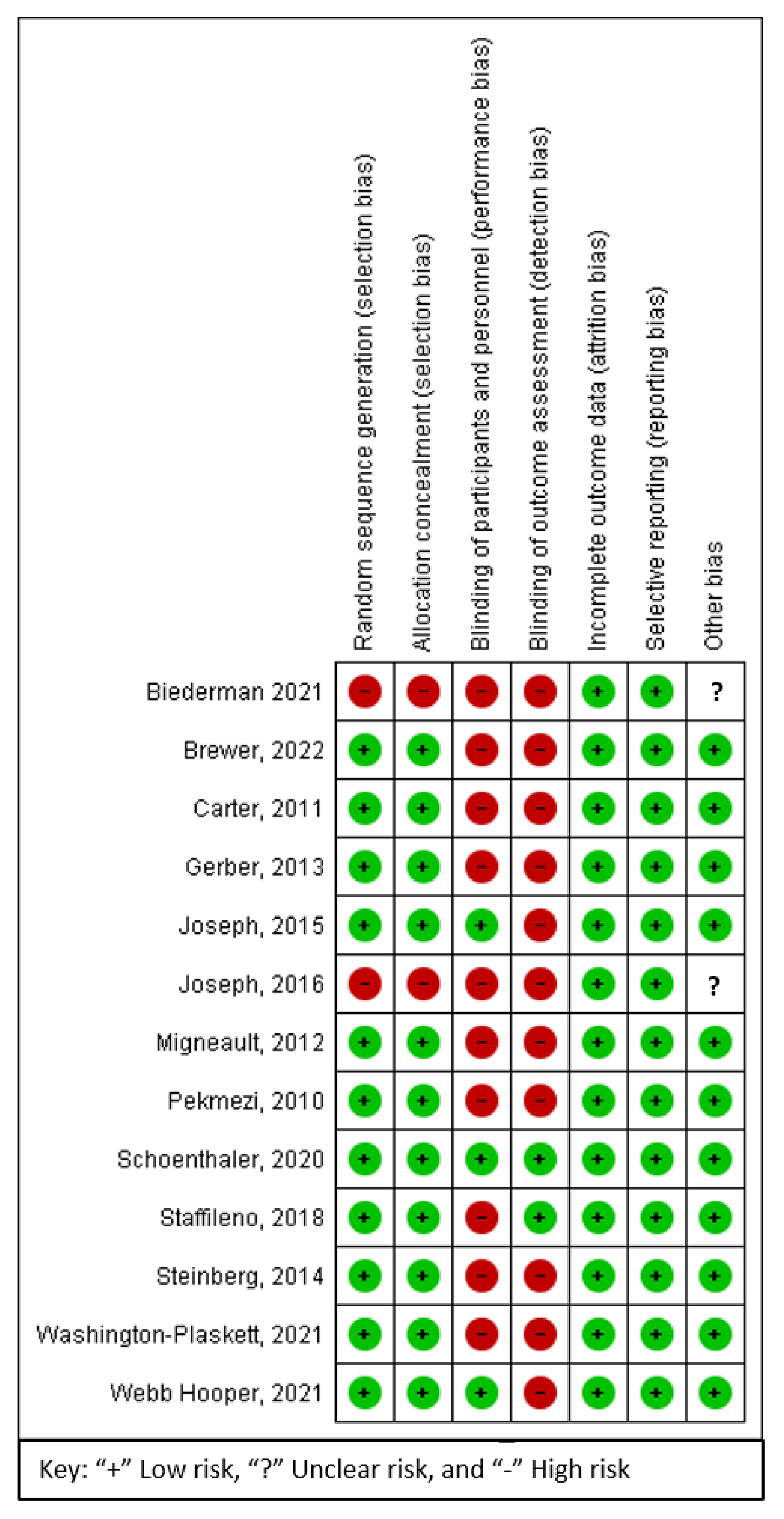
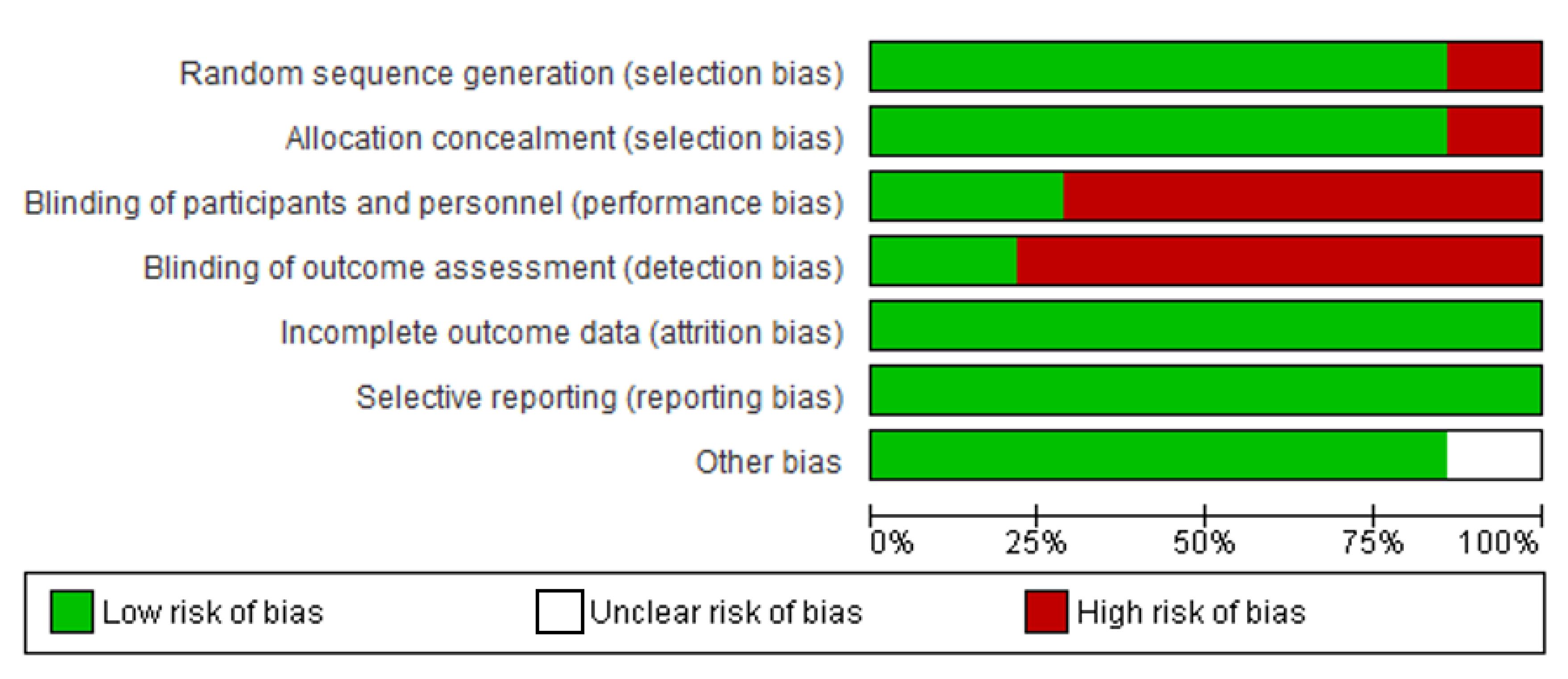
2.4. Risk of Bias Assessment
3. Results
3.1. Study Characteristics
3.2. Intervention Modalities and Features
3.3. Comparison
3.4. Risk of Bias and Quality Assessment


3.5. Clinical Outcomes
3.6. Behavioural/Lifestyle Outcomes
3.7. Acceptability and Adherence
4. Discussion
4.1. Strengths and Limitations of the Studies Reviewed
4.2. Limitations of the Review
4.3. Important Findings and Recommendations
- Even though the results of this review were mixed, there is potential for IbIs to improve clinical and behavioural outcomes of CVDs.
- Despite the compelling evidence supporting the critical role sodium plays in the regulation of blood pressure, which is central in the development of CVDs, none of the studies reviewed in this study focused on dietary salt reduction. This knowledge gap thus provides an opportunity for future research.
- Most of the studies were conducted in the past five years; this suggests a recent emphasis on IbIs in the prevention and promotion of self-management of chronic diseases. Although IbIs were gaining popularity before the COVID-19 pandemic, the demand for these innovative technologies has surged since the outbreak.
- There is a need for robust research designs and long-term follow-ups to determine whether IbIs can permanently cause lifestyle changes in PAD at risk of CVDs.
- All the studies were carried out in the United States. Similar studies are required in other countries with a substantial PAD population.
- Although cost-effectiveness is frequently cited as an advantage of mHealth, none of the studies we reviewed examined the cost-effectiveness of IbIs.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Thomas, H.; Diamond, J.; Vieco, A.; Chaudhuri, S.; Shinnar, E.; Cromer, S.; Perel, P.; Mensah, G.A.; Narula, J.; Johnson, C.O.; et al. Global Atlas of Cardiovascular Disease 2000–2016: The Path to Prevention and Control. Glob. Heart 2018, 13, 143–163. [Google Scholar] [CrossRef] [PubMed]
- Jackson, C.L.; Redline, S.; Emmons, K.M. Sleep as a Potential Fundamental Contributor to Disparities in Cardiovascular Health. Annu. Rev. Public Health 2015, 36, 417–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lip, G.Y.H.; Barnett, A.H.; Bradbury, A.; Cappuccio, F.P.; Gill, P.S.; Hughes, E.; Imray, C.; Jolly, K.; Patel, K. Ethnicity and Cardiovascular Disease Prevention in the United Kingdom: A Practical Approach to Management. J. Hum. Hypertens. 2007, 21, 183–211. [Google Scholar] [CrossRef]
- Wang, R.; Dong, Y.; Weng, J.; Kontos, E.Z.; Chervin, R.D.; Rosen, C.L.; Marcus, C.L.; Redline, S. Associations among Neighbourhood, Race, and Sleep Apnea Severity in Children. A Six-City Analysis. Ann. Am. Thorac. Soc. 2017, 14, 76–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- British Heart Foundation. 2022. Available online: https://www.bhf.org.uk/-/media/files/research/heart-statistics/bhf-cvd-statistics---uk-factsheet.pdf (accessed on 10 May 2022).
- Public Health England. Health Matters: Preventing Cardiovascular Disease. 2019. Available online: https://www.gov.uk/government/publications/health-matters-preventing-cardiovascular-disease/health-matters-preventing-cardiovascular-disease (accessed on 16 April 2022).
- NHS Long Term Plan. Available online: https://www.longtermplan.nhs.uk/ (accessed on 7 May 2022).
- Kanjilal, S.; Gregg, E.W.; Cheng, Y.J.; Zhang, P.; Nelson, D.E.; Mensah, G.; Beckles, G.L.A. Socioeconomic Status and Trends in Disparities in 4 Major Risk Factors for Cardiovascular Disease Among US Adults, 1971–2002. Arch. Intern. Med. 2006, 166, 2348–2355. [Google Scholar] [CrossRef] [Green Version]
- Mensah, G.A.; Mokdad, A.H.; Ford, E.S.; Greenlund, K.J.; Croft, J.B. State of Disparities in Cardiovascular Health in the United States. Circulation 2005, 111, 1233–1241. [Google Scholar] [CrossRef]
- Dimsdale, J.E. Stalked by the Past: The Influence of Ethnicity on Health. Psychosom. Med. 2000, 6, 161–170. [Google Scholar] [CrossRef]
- Onwuanyi, A.; Hodges, D.; Avancha, A.; Weiss, L.; Rabinowitz, D.; Shea, S.; Francis, C.K. Hypertensive Vascular Disease as a Cause of Death in Blacks Versus Whites. Hypertension 1998, 31, 1070–1076. [Google Scholar] [CrossRef] [Green Version]
- Lane, D.; Beevers, D.G.; Lip, G.Y.H. Ethnic Differences in Blood Pressure and the Prevalence of Hypertension in England. J. Hum. Hypertens. 2002, 16, 267–273. [Google Scholar] [CrossRef] [Green Version]
- Chaturvedi, N.; McKeigue, P.M.; Marmot, M.G. Resting and Ambulatory Blood Pressure Differences in Afro-Caribbeans and Europeans. Hypertension 1993, 22, 90–96. [Google Scholar] [CrossRef] [Green Version]
- Moore, A.P.; Rivas, C.R.; Stanton-Fay, S.; Harding, S.; Goff, L.M. Designing the Healthy Eating and Active Lifestyles for Diabetes (HEAL-D) Self-Management and Support Programme for UK African and Caribbean Communities: A Culturally Tailored, Complex Intervention under-Pinned by Behaviour Change Theory. BMC Public Health 2019, 19, 1146. [Google Scholar] [CrossRef] [PubMed]
- Nesbitt, S.D. Hypertension in Black Patients: Special Issues and Considerations. Curr. Hypertens. Rep. 2005, 7, 244–248. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.C.; Clark, L.T.; Cooper, R.S.; Daniels, S.R.; Kumanyika, S.K.; Ofili, E.; Quinones, M.A.; Sanchez, E.J.; Saunders, E.; Tiukinhoy, S.D. Discovering the Full Spectrum of Cardiovascular Disease. Circulation 2005, 111, e134–e139. [Google Scholar] [CrossRef]
- Vita, J. Nitric Oxide and Vascular Reactivity in African American Patients with Hypertension*1. J. Card. Fail. 2003, 9, S199–S204. [Google Scholar] [CrossRef]
- Reyes, M.V. The Disproportional Impact of COVID-19 on African Americans. Health Hum. Rights 2020, 22, 299–307. [Google Scholar]
- Tai, D.B.G.; Shah, A.; Doubeni, C.A.; Sia, I.G.; Wieland, M.L. The Disproportionate Impact of COVID-19 on Racial and Ethnic Minorities in the United States. Clin. Infect. Dis. 2021, 72, 703–706. [Google Scholar] [CrossRef] [PubMed]
- Bodenheimer, T.; Lorig, K.; Holman, H.; Grumbach, K. Patient Self-Management of Chronic Disease in Primary Care. JAMA 2002, 288, 2469–2475. [Google Scholar] [CrossRef] [PubMed]
- Bosworth, H.; Olsen, M.; Neary, A.; Orr, M.; Grubber, J.; Svetkey, L.; Adams, M.; Oddone, E. Take Control of Your Blood Pressure (TCYB) Study: A Multifactorial Tailored Behavioral and Educational Intervention for Achieving Blood Pressure Control. Patient Educ. Couns. 2008, 70, 338–347. [Google Scholar] [CrossRef] [Green Version]
- Kelley, G.A.; Kelley, K.S. Progressive Resistance Exercise and Resting Blood Pressure. Hypertension 2000, 35, 838–843. [Google Scholar] [CrossRef]
- Xin, X.; He, J.; Frontini, M.; Ogden, L.; Motsamai, O.; Whelton, P. Effects of Alcohol Reduction on Blood Pressure. Hypertension 2001, 38, 1112–1117. [Google Scholar] [CrossRef]
- Liu, S.; Dunford, S.; Leung, Y.; Brooks, D.; Thomas, S.; Eysenbach, G.; Nolan, R. Reducing Blood Pressure with Internet-Based Interventions: A Meta-Analysis. Can. J. Cardiol. 2013, 29, 613–621. [Google Scholar] [CrossRef] [PubMed]
- McManus, R.J.; Little, P.; Stuart, B.; Morton, K.; Raftery, J.; Kelly, J.; Bradbury, K.; Zhang, J.; Zhu, S.; Murray, E.; et al. Home and Online Management and Evaluation of Blood Pressure (HOME BP) Using a Digital Intervention in Poorly Controlled Hypertension: Randomised Controlled Trial. BMJ 2021, 372, m4858. [Google Scholar] [CrossRef] [PubMed]
- Richard, E.; Jongstra, S.; Soininen, H.; Brayne, C.; Moll van Charante, E.; Meiller, Y.; Van Der Groep, B.; Beishuizen, C.R.L.; Mangialasche, F.; Barbera, M.; et al. Healthy Ageing Through Internet Counselling in the Elderly: The HATICE Randomised Controlled Trial for the Prevention of Cardiovascular Disease and Cognitive Impairment. BMJ Open 2016, 6, e010806. [Google Scholar] [CrossRef] [PubMed]
- Saner, H.; van der Velde, E. EHealth in Cardiovascular Medicine: A Clinical Update. Eur. J. Prev. Cardiol. 2016, 23, 5–12. [Google Scholar] [CrossRef] [Green Version]
- Office for National Statistics. Internet Users, UK: 2019; Office for National Statistics: London, UK, 2019.
- Drijver, A.; Reijneveld, J.; Wesselman, L.; Klein, M. A Web-Based Lifestyle Intervention Aimed at Improving Cognition in Patients with Cancer Returning to Work in an Outpatient Setting: Protocol for a Randomized Controlled Trial. JMIR Res. Protoc. 2021, 10, 22670. [Google Scholar] [CrossRef]
- Lehtisalo, J.; Ngandu, T.; Lindstrom, J.; Levälahti, E.; Peltonen, M.; Hänninen, T.; Antikainen, R.; Laatikainen, T.; Strandberg, T.; Tuomilehto, J.; et al. Dietary Intervention Adherence and Cognitive Changes Among Individuals with Elevated Risk of Dementia: The Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability (FINGER). Alzheimer’s Dement. 2017, 13, 616. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Microsoft Corporation. Microsoft Excel Spreadsheet Software | Microsoft 365. 2018. Available online: https://www.microsoft.com/en-us/microsoft-365/excel (accessed on 2 June 2022).
- Cumpston, M.; Li, T.; Page, M.J.; Chandler, J.; Welch, V.A.; Higgins, J.P.; Thomas, J. Updated Guidance for Trusted Systematic Reviews: A New Edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst. Rev. 2019, 10, 14651858. [Google Scholar] [CrossRef] [Green Version]
- Campbell, M.; Katikireddi, S.V.; Sowden, A.; McKenzie, J.E.; Thomson, H. Improving Conduct and Reporting of Narrative Synthesis of Quantitative Data (ICONS-Quant): Protocol for a Mixed Methods Study to Develop a Reporting Guideline. BMJ Open 2018, 8, e020064. [Google Scholar] [CrossRef]
- Lucas, P.J.; Baird, J.; Arai, L.; Law, C.; Roberts, H.; Lucas, P.J.; Baird, J.; Arai, L.; Roberts, H.M. Worked Examples of Alternative Methods for the Synthesis of Qualitative and Quantitative Research in Systematic Reviews. BMC Med. Res. Methodol. 2007, 7, 4. [Google Scholar] [CrossRef]
- Harden, A.; Garcia, J.; Oliver, S.; Rees, R.; Shepherd, J.; Brunton, G.; Oakley, A. Applying Systematic Review Methods to Studies of People’s Views: An Example from Public Health Research. J. Epidemiol. Community Health 2004, 58, 794. [Google Scholar] [CrossRef] [PubMed]
- Eysenck, H.J. An Exercise in Mega-Silliness. Am. Psychol. 1978, 33, 517. [Google Scholar] [CrossRef]
- Ioannidis, J.; Patsopoulos, N.; Rothstein, H. Reasons or excuses for avoiding meta-analysis in forest plots. BMJ 2008, 336, 1413–1415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, K.; Kwan, H.; Yu, Z.; Tong, T. Model selection between the fixed-effects model and the random-effects model in meta-analysis. Stat. Interface 2020, 13, 501–510. [Google Scholar] [CrossRef]
- Spineli, L.; Pandis, N. Fixed-effect versus random-effects model in meta-regression analysis. Am. J. Orthod. Dentofac. Orthop. 2020, 158, 770–772. [Google Scholar] [CrossRef] [PubMed]
- Jadad, A.; Moore, R.; Carroll, D.; Jenkinson, C.; Reynolds, D.; Gavaghan, D.; McQuay, H. Assessing the Quality of Reports of Randomised Clinical Trials: Is Blinding Necessary? Control. Clin. Trials 1997, 17, 1–12. [Google Scholar] [CrossRef]
- Higgins, J.; Green, S. Cochrane Handbook of Systematic Reviews of Interventions; Wiley: Chichester, UK, 2008. [Google Scholar]
- Brewer, L.; Jenkins, S.; Hayes, S.; Kumbamu, A.; Jones, C.; Burke, L.; Cooper, L.A.; Patten, C.A. Community- Based, Cluster-Randomized Pilot Trial of a Cardiovascular MHealth Intervention: Rationale, Design, and Baseline Findings of the FAITH! Trial. Am. Heart J. 2022, 247, 1–14. [Google Scholar] [CrossRef]
- Washington-Plaskett, T.; Idris, M.; Mubasher, M.; Ko, Y.; Islam, S.; Dunbar, S.; Taylor, H.; Quyyumi, A.A.; Pemu, P. Impact of Technology-Based Intervention for Improving Self-Management Behaviors in Black Adults with Poor Cardiovascular Health: A Randomised. Int. J. Environ. Res. Public Health 2021, 18, 3660. [Google Scholar] [CrossRef]
- Biederman, D.; Sabol, V.; Thompson, J.; Duncan, Q.; Pereira, K.C. Increasing Physical Activity with African American Women Using FacebookTM and Pedometers. Public Health Nurs. 2021, 38, 671–674. [Google Scholar] [CrossRef]
- Carter, E.L.; Nunlee-Bland, G.; Callender, C. A Patient-Centric, Provider-Assisted Diabetes Telehealth Self-Management Intervention for Urban Minorities. Perspect. Health Inf. Manag. 2011, 8, 1. [Google Scholar]
- Gerber, B.S.; Schiffer, L.; Brown, A.A.; Berbaum, M.L.; Rimmer, J.H.; Braunschweig, C.L.; Fitzgibbon, M.L. Video Telehealth for Weight Maintenance of African American Women. J. Telemed. Telecare 2013, 19, 266–272. [Google Scholar] [CrossRef] [Green Version]
- Joseph, R.; Keller, C.; Adams, M.; Ainsworth, B. Print versus a Culturally Relevant Facebook and Text Message Delivered Intervention to Promote Physical Activity in African American Women: A Randomised Pilot Trial. BMC Women’s Health 2015, 15, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joseph, R.P.; Pekmezi, D.; Dutton, G.R.; Cherrington, A.L.; Kim, Y.I.; Allison, J.J.; Durant, N.H. Results of a Culturally Adapted Internet-Enhanced Physical Activity Pilot Intervention for Overweight and Obese Young Adult African American Women. J. Transcult. Nurs. 2016, 27, 136–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Migneault, J.; Dedier, J.; Wright, J.; Heeren, T.; Campbell, M.; Morisky, D.; Rudd, P.; Friedman, R.H. A Culturally Adapted Telecommunication System to Improve Physical Activity, Diet Quality, and Medication Adherence Among Hypertensive African Americans: A Randomized Controlled Trial. Ann. Behav. Med. 2012, 43, 62–73. [Google Scholar] [CrossRef] [PubMed]
- Pekmezi, D.; Williams, D.; Dunsiger, S.; Jennings, E.; Lewis, B.; Jakicic, J.; Marcus, B. Feasibility of Using Computer-Tailored and Internet-Based Interventions to Promote Physical Activity in Underserved Populations. Telemed. e-Health 2010, 16, 498–503. [Google Scholar] [CrossRef] [Green Version]
- Schoenthaler, A.; Leon, M.; Butler, M.; Steinhaeuser, K.; Wardzinski, W. Development and Evaluation of a Tailored Mobile Health Intervention to Improve Medication Adherence in Black Patients with Uncontrolled Hypertension and Type 2 Diabetes: Pilot Randomized Feasibility Trial. JMIR mHealth uHealth 2020, 8, e17135. [Google Scholar] [CrossRef]
- Staffileno, B.; Tangney, C.; Fogg, L. Favorable Outcomes Using an EHealth Approach to Promote Physical Activity and Nutrition Among Young African American Women. J. Cardiovasc. Nurs. 2018, 33, 62–71. [Google Scholar] [CrossRef]
- Steinberg, D.; Levine, E.; Lane, I.; Askew, S.; Foley, P.; Puleo, E.; Bennett, G.; Turner-McGrievy, B.; Tevelde, S. Adherence to Self-Monitoring via Interactive Voice Response Technology in an EHealth Intervention Targeting Weight Gain Prevention Among Black Women: Randomized Controlled Trial. J. Med. Internet Res. 2014, 16, e114. [Google Scholar] [CrossRef] [Green Version]
- Webb Hooper, M.; Miller, D.; Saldivar, E.; Mitchell, C.; Johnson, L.; Burns, M.; Huang, M. Randomized Controlled Trial Testing a Video-Text Tobacco Cessation Intervention among Economically Disadvantaged African American Adults. Psychol. Addict. Behav. 2021, 35, 769–777. [Google Scholar] [CrossRef]
- Hamine, S.; Gerth-Guyette, E.; Faulx, D.; Green, B.; Ginsburg, A. Impact of MHealth Chronic Disease Management on Treatment Adherence and Patient Outcomes: A Systematic Review. J. Med. Internet Res. 2015, 17, 52. [Google Scholar] [CrossRef] [Green Version]
- Anglada-Martinez, H.; Riu-Viladoms, G.; Martin-Conde, M.; Rovira-Illamola, M.; Sotoca-Momblona, J.; Codina-Jane, C. Does MHealth Increase Adherence to Medication? Results of a Systematic Review. Int. J. Clin. Pract. 2014, 69, 9–32. [Google Scholar] [CrossRef] [PubMed]
- Hall, A.; Cole-Lewis, H.; Bernhardt, J. Mobile Text Messaging for Health: A Systematic Review of Reviews. Annu. Rev. Public Health 2015, 36, 393–415. [Google Scholar] [PubMed] [Green Version]
- Pfaeffli Dale, L.; Dobson, R.; Whittaker, R.; Maddison, R. The Effectiveness of Mobile-Health Behaviour Change Interventions for Cardiovascular Disease Self-Management: A Systematic Review. Eur. J. Prev. Cardiol. 2015, 23, 801–817. [Google Scholar] [CrossRef]
- Chow, C.; Jolly, S.; Rao-Melacini, P.; Fox, K.; Anand, S.; Yusuf, S. Association of Diet, Exercise, and Smoking Modification with Risk of Early Cardiovascular Events After Acute Coronary Syndromes. Circulation 2010, 121, 750–758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Free, C.; Phillips, G.; Galli, L.; Watson, L.; Felix, L.; Edwards, P.; Patel, V.; Haines, A. The Effectiveness of Mobile-Health Technology-Based Health Behaviour Change or Disease Management Interventions for Health Care Consumers: A Systematic Review. PLoS Med. 2013, 10, e1001362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wittes, J. Sample Size Calculations for Randomized Controlled Trials. Epidemiol. Rev. 2002, 24, 39–53. [Google Scholar] [CrossRef] [Green Version]
- Desu, M.M.; Raghavarao, D. Sample Size Methodology; Academic Press: Boston, MA, USA, 1990. [Google Scholar]
- Sackett, D.L. Bias in Analytic Research. J. Chronic Dis. 1979, 32, 51–63. [Google Scholar] [CrossRef]
- Moher, D.; Hopewell, S.; Schulz, K.; Montori, V.; Gøtzsche, P.; Devereaux, P. CONSORT 2010 Explanation and Elaboration: Updated Guidelines for Reporting Parallel Group Randomised Trials. J. Clin. Epidemiol. 2010, 63, 1–37. [Google Scholar] [CrossRef] [Green Version]
- Gaziano, T.; Bitton, A.; Anand, S.; Abrahams-Gessel, S.; Murphy, A. Growing Epidemic of Coronary Heart Disease in Low- and Middle-Income Countries. Curr. Probl. Cardiol. 2010, 35, 72–115. [Google Scholar] [CrossRef] [Green Version]
- Campbell, N.; Legowski, B.; Legetic, B.; Wilks, R.; Vasconcellos, A.P.D.A.; Prt Group on Cardio Prevention through Dietary Salt Reduction. PAHO/WHO Regional Expert Group Policy Statement—Preventing cardiovascular disease in the Americas by reducing dietary salt intake population wide. Glob. Heart 2009, 4, 189. [Google Scholar] [CrossRef]
- World Health Organization. 2022. Available online: http://apps.who.int/iris/bitstream/10665/94384/1/9789241506236_eng.pdf?ua=1 (accessed on 10 May 2022).
- Burch, J.; Tort, S. What are the effects of dietary advice on reducing salt intake for preventing cardiovascular disease? Cochrane Clin. Answ. 2020. [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| PICO Terms | Search Term(s) | Search Strategy |
|---|---|---|
| Population | Adults of African Descent with CVDs or risk factors | “People of African descent” OR “Black British” OR “Black*” OR “Black African*” OR “Black Caribbean*” OR “Afro-Caribbean*” OR “African American*” OR “Black Ethnic Group” |
| Intervention | Interventions delivered via the Internet | “Mobile Technolog*” OR “Lifestyle intervention*” OR “Lifestyle” OR “Health Technolog*” OR “Internet” OR “Online” OR “Web-Based” OR “Digital Health” OR “Internet-Based Intervention” OR “Telemedicine” |
| Comparison | Interventions not delivered via the Internet | |
| Outcome | Changes in behaviour and Individual CVD risk factors. Adherence and acceptability | “Cardiovascular risk factors” OR “Weight Management” OR “Cardiovascular Disease*” OR “Cardiometabolic” OR “Body Mass index” OR “Waist Circumference” OR “Blood Pressure” OR “Haemoglobin A1c” OR “Fasting Plasma Glucose” OR Triglyceride OR “Total Cholesterol” OR LDL-C OR HDL-C OR “Physical Activit*” OR “Medication Adherence” OR “Smoking Cessation” |
| Study design | Experimental or quasi-experimental |
Population:
|
Intervention:
|
Comparator:
|
Outcomes:
|
Study Design:
|
| Study | Setting | Design/Duration/Intervention Type | Demographics Information and Study Characteristics | |||||
|---|---|---|---|---|---|---|---|---|
| N | Dropout | Gender [%] | Ethnicity [%] | Mean Age [Years] | Target Disease | |||
| Biederman et al., 2021 [45] | African American women in Gastonia, NC, USA. | Pre-test and Post-test quasi-experiment. 5-week intervention via Facebook and Pedometers. The intervention was evidence-based, but no specific model/theory was used. | 20. No defined control group. | 7 | Female 100% | African Americans 100% | 40 | Hypertension |
| Brewer et al., 2022 [43] | African American churches in the USA. | 6-month pilot cluster Randomised Control Trial (RCT). The intervention was via a web-based mobile App called FAITH. The intervention was designed according to the Precaution Adoption Process Model (PAPM). | 76. Test group (n = 34). Control group (n = 42). | 9 | Female 71%. Male 29%. | African Americans 100% | 54.5 | Cardiovascular diseases |
| Carter et al., 2011 [46] | Washington, DC, USA. | 9-month RCT focusing on weight, blood pressure, and glucose measurement using a laptop with peripherals such as a blood pressure cuff, glucometer, and wireless scale. The intervention was not based on any specific model/theory. | 47. Test group (n = 26). Control group (n = 21). | 27 | Female 63.8%. Male 36.2% | African Americans 100% | 56 | Diabetes |
| Gerber et al., 2013 [47] | Two community churches in Chicago, IL, USA. | 3-month RCT for weight loss and 9-month RCT for weight maintenance. The intervention was via video telehealth. The intervention was not based on any specific theory/model. | 89. Test group (n = 45). Control group (n = 43). | 5 | Female 100% | African Americans 100% | 50 | Obesity and Overweight |
| Joseph et al., 2015 [48] | Metropolitan area of Phoenix, AZ, USA. | 8-week, 2-arm RCT. The intervention was delivered via Facebook and text messages. The intervention was based on Social Cognitive Theory. | 29. Test group (n = 14). Control group (n = 15). | 0 | Female 100%. | African Americans 100% | 35.5 | Physical inactivity |
| Joseph et al., 2016 [49] | College students in Phoenix, AZ, USA. | 3-month, single group, pre-test and Post-test, quasi-experiment. A culturally relevant physical activity (PA) promotion website and four moderate-intensity PA sessions per week were used to deliver the intervention. The intervention was based on Social Cognitive Theory. | 31. No defined control group. | 6 | Female 100% | African Americans 100% | 21.9 | Obesity and Overweight |
| Migneault et al., 2012 [50] | Urban-dwelling AA adults in the USA. | 8-month RCT. The intervention was delivered through a Telephone Linked-Care system, an automated, computer-based, interactive telephone counselling system. The intervention was based on Social Cognitive Theory, Motivational Interviewing, and the Transtheoretical behavioral change model. | 337. Test group (n = 169). Control group (n = 168). | 72 | Female 70% Male 30% | African American 100% | 56.5 | Hypertension |
| Pekmezi et al., 2010 [51] | Community dwellers in Rhodes Island and Pittsburgh, PA, USA. | 1-year, 3-arm RCT. Intervention delivered via Tailored Internet, Tailored Print, or Standard Internet. The intervention was based on Transtheoretical Model and Social Cognitive Theory constructs. | 38 Test group (n = 38). Control group (n = 211). | 8 | Female 92.6%. Male 7.4% | African American 100% | 42.6 | Obesity and Overweight |
| Schoenthaler et al., 2020 [52] | Primary care clinic in New York City, NY, USA. | 3-month RCT. The intervention was via a mHealth device built using Microsoft’s Models, Views, and Controllers Entity Framework as the development environment. The intervention was based on the Information-Motivation-Behavioural skills model of adherence. | Phase 1 (n = 10). Phase 2 (n = 42). Test group (n = 21). Control group (n = 21). | 0 | Phase 1: Female 70%, Male 30%. Phase 2: Female 45.2%, Male 54.8% | African Americans 100% | Phase 1: 65.8 Phase 2: 57.6 | Hypertension and Diabetes |
| Staffileno et al., 2018 [53] | Young African American Women in the USA. | 2-arm, 3-month RCT. The intervention was web-based and accessible via the Internet and mobile devices. Intervention is designed according to Social Cognitive Theory. | 35. Both control and test groups received IbI. | 9 | Female 100% | African Americans 100% | 35.2 | Pre-hypertension |
| Steinberg et al., 2014 [54] | Five community health centres in NC, USA. | 2-arm, 12-month RCT. The intervention utilised the interactive obesity treatment approach (iOTA). Several behaviours change theories were used in the design of the intervention. | 194. Test group (n = 97). Control group (n = 97). | 9 | Female 100% | African American 100% | 35.4 | Obesity |
| Washington-Plaskett et al., 2021 [44] | Atlanta Metro area, USA. | 6-month RCT. The intervention was via Health360x, a web-based or mobile application that supports behaviour. The intervention took a theory-based approach to engage vulnerable populations in a technology-enabled behavioural intervention. | 146. Both control and test groups received IbI. | 26 | Female 66.7%. Male 33.3% | African Americans 100% | 55.6 | CVDs |
| Webb Hooper et al., 2021 [55] | A Midwestern city in the USA. | 6-week, 2-arm pilot RCT. The intervention was a video text-messaging program known as Path2Quit. The intervention was not based on any specific model/theory. | 119. Intervention group (n = 61). Control group (n = 58). | 9 | Female 52%. Male 48%. | African Americans 100% | 53.5 | Smoking |
| Study | Purpose | Findings | Jadad Quality Rating |
|---|---|---|---|
| Biederman et al., 2021 [45] | Evaluate the efficacy of combining FacebookTM and pedometers to provide a physical activity intervention to African American women. | Weekly steps increased by 190% in participants after the intervention (p = 0.005). Compared to baseline, about 80% of participants reported being active at least twice a week (35.7%). | Low (Jadad Score 2/5) |
| Brewer et al., 2022 [43] | Evaluate the feasibility and preliminary effectiveness of a web-based application promoting LS7 among African American churchgoers. | The primary outcomes are significant changes in LS7 score from baseline after six months of intervention and app engagement/usability. | High (Jadad Score 3/5) |
| Carter et al., 2011 [46] | Report the design, implementation, and outcomes of IbIs targeting African Americans with type 2 diabetes living in urban areas. | The results indicate that participants have favourable outcomes in decreased haemoglobin A1c and body mass index measures compared to the control group. | High (Jadad Score 3/5) |
| Gerber et al., 2013 [47] | Based on group interaction, assess the impact of home telehealth on weight maintenance following a weight loss programme. | Both control and test groups saw no significant changes in weight during maintenance. The groups did not have significant differences regarding nutrition, exercise, social support, or feelings of self-efficacy throughout the maintenance phase. | High (Jadad Score 3/5) |
| Joseph et al., 2015 [48] | Examine the effectiveness of a multi-component intervention based on the Social Cognitive Theory and utilising Facebook and text messages to encourage physical activity in African American women. | Facebook and text message-based physical activity reduced sedentary behaviour, increased light, and moderate-lifestyle intensity physical activity, improved psychosocial outcomes and increased participant satisfaction. | High (Jadad Score 4/5) |
| Joseph et al., 2016 [49] | Evaluate the efficacy of an Internet-enhanced physical activity (PA) pilot programme created for overweight/obese AA female college students. | This exploratory study provides early evidence in favour of IbIs being used to promote PA in overweight or obese AA women. | Low (Jadad Score 2/5) |
| Migneault et al., 2012 [50] | Analyse the efficacy of a culturally tailored automated phone system for hypertensive urban African-American adults and evidence-based recommendations for better eating habits and physical activity. | The intervention improved the food quality and the amount of energy expended in general. Systolic BP decreased, but the drop was not statistically significant. | High (Jadad Score 3/5) |
| Pekmezi et al., 2010 [51] | A subsample of AA adults was studied to see if Internet-powered, multiple contact physical activity interventions were feasible and effective. | The findings indicate that computer-tailored and Internet-based therapies can result in significant long-term gains in physical activity and associated process variables in AA adults. | High (Jadad Score 3/5) |
| Schoenthaler et al., 2020 [52] | Evaluate the acceptability (phase 1) and preliminary efficacy (phase 2) of a customised mobile health intervention to improve medication adherence, diastolic blood pressure (DBP), haemoglobin A1c (HbA1c), and systolic blood pressure (SBP) in black patients. | During Phase 1 semi-structured interviews, interferences in daily routines, concerns about side effects, forgetfulness, the difficulty of medication administration, and a desire for natural treatments were all identified as significant hurdles to adherence. Both groups exhIbIted considerable improvements in medication adherence and SBP in Phase 2, although there was no meaningful change. | High (Jadad Score 4/5) |
| Staffileno et al., 2018 [53] | Examine the effectiveness of an Internet-based, culturally relevant lifestyle change intervention for AA women to promote PA and a balanced diet. | The eHealth platform offers an alternative strategy to target young AA women and was beneficial in reducing PA and dietary behaviours. | High (Jadad Score 4/5) |
| Steinberg et al., 2014 [54] | Explore the patterns and predictors of low-income black women’s self-monitoring adherence to Interactive Voice Recognition (IVR) and the connection between adherence and weight change. | Adherence of socioeconomically disadvantaged black women to the IbI was high. Using IVR to encourage self-monitoring has the potential for widespread use and long-term sustainability. | High (Jadad Score 3/5) |
| Washington-Plaskett et al., 2021 [44] | Examine the impact of a technology-based intervention on behaviour change among AA with high cardiovascular risk in Atlanta, Georgia. | This study reveals that improvements in LS7 are associated with a 7% reduction in incident CVDs throughout a lifetime, and self-management aided by technology may be a viable way for Blacks to manage certain CVD risk factors. Females statistically significantly improved their BMI and diastolic blood pressure and decreased their self-reported physical activity. Health coaches can assist persons living in high-risk neighbourhoods in improving their overall LS7. | High (Jadad Score 3/5) |
| Webb Hooper et al., 2021 [55] | Determine the acceptability and short-term effects of a culturally tailored mobile health (mHealth) intervention (Path2Quit) among a sample of poor African American (AA) individuals. | It was found that a culturally-specific mHealth intervention improved Nicotine Replacement Therapy (NRT) and short-term abstinence. | High (Jadad Score 4/5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Usman, J.E.; Childs, C.; Rogerson, D.; Klonizakis, M. A Systematic Review of Internet-Based Interventions for the Prevention and Self-Management of Cardiovascular Diseases among People of African Descent. Int. J. Environ. Res. Public Health 2022, 19, 8872. https://doi.org/10.3390/ijerph19148872
Usman JE, Childs C, Rogerson D, Klonizakis M. A Systematic Review of Internet-Based Interventions for the Prevention and Self-Management of Cardiovascular Diseases among People of African Descent. International Journal of Environmental Research and Public Health. 2022; 19(14):8872. https://doi.org/10.3390/ijerph19148872
Chicago/Turabian StyleUsman, Jesse Enebi, Charmaine Childs, David Rogerson, and Markos Klonizakis. 2022. "A Systematic Review of Internet-Based Interventions for the Prevention and Self-Management of Cardiovascular Diseases among People of African Descent" International Journal of Environmental Research and Public Health 19, no. 14: 8872. https://doi.org/10.3390/ijerph19148872