
Associations between Physical Activity Level and Health Services Use in Spanish Adults

 , , , , , , and
, , , , , , and 
Abstract
:1. Introduction
2. Materials and Methods
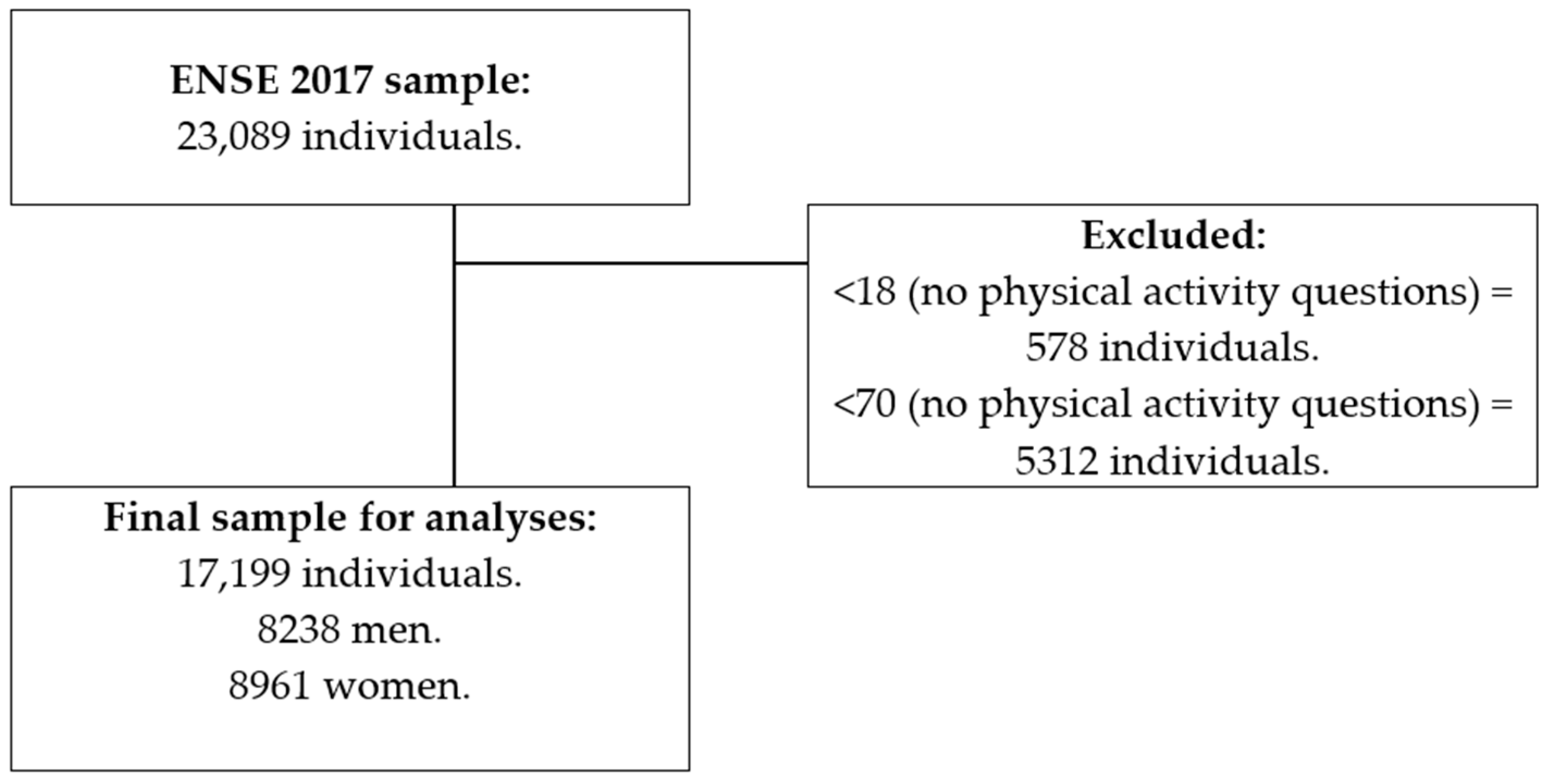
2.1. Desing and Participants
2.2. Measures and Variables
2.3. Ethical Concerns
2.4. Statistical Analysis
3. Results
4. Discussion
4.1. Main Findings and Theoretical Implications
4.2. Practical Implications
4.3. Limitations and Future Lines
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dieleman, J.L.; Sadat, N.; Chang, A.Y.; Fullman, N.; Abbafati, C.; Acharya, P.; Adou, A.K.; Ahmad Kiadaliri, A.; Alam, K.; Alizadeh-Navaei, R.; et al. Trends in future health financing and coverage: Future health spending and universal health coverage in 188 countries, 2016–2040. Lancet 2018, 391, 1783–1798. [Google Scholar] [CrossRef] [Green Version]
- Keehan, S.P.; Cuckler, G.A.; Poisal, J.A.; Sisko, A.M.; Smith, S.D.; Madison, A.J.; Rennie, K.E.; Fiore, J.A.; Hardesty, J.C. National Health Expenditure Projections, 2019–2028: Expected Rebound in Prices Drives Rising Spending Growth: National health expenditure projections for the period 2019–2028. Health Aff. 2020, 39, 704–714. [Google Scholar] [CrossRef] [PubMed]
- Harris, A.; Sharma, A. Estimating the future health and aged care expenditure in Australia with changes in morbidity. PLoS ONE 2018, 13, e0201697. [Google Scholar] [CrossRef] [PubMed]
- Lopreite, M.; Mauro, M. The effects of population ageing on health care expenditure: A Bayesian VAR analysis using data from Italy. Health Policy 2017, 121, 663–674. [Google Scholar] [CrossRef] [PubMed]
- Carlson, S.A.; Fulton, J.E.; Pratt, M.; Yang, Z.; Adams, E.K. Inadequate Physical Activity and Health Care Expenditures in the United States. Prog. Cardiovasc. Dis. 2015, 57, 315–323. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, P.; Le, L.K.-D.; Ananthapavan, J.; Gao, L.; Dunstan, D.W.; Moodie, M. Economics of sedentary behaviour: A systematic review of cost of illness, cost-effectiveness, and return on investment studies. Prev. Med. 2022, 156, 106964. [Google Scholar] [CrossRef]
- Muka, T.; Imo, D.; Jaspers, L.; Colpani, V.; Chaker, L.; van der Lee, S.J.; Mendis, S.; Chowdhury, R.; Bramer, W.M.; Falla, A.; et al. The global impact of non-communicable diseases on healthcare spending and national income: A systematic review. Eur. J. Epidemiol. 2015, 30, 251–277. [Google Scholar] [CrossRef]
- Kazibwe, J.; Tran, P.B.; Annerstedt, K.S. The household financial burden of non-communicable diseases in low- and middle-income countries: A systematic review. Health Res. Policy Syst. 2021, 19, 96. [Google Scholar] [CrossRef]
- Hartman, M.; Martin, A.B.; Washington, B.; Catlin, A.; The National Health Expenditure Accounts Team. National Health Care Spending In 2020: Growth Driven by Federal Spending in Response to the COVID-19 Pandemic: National Health Expenditures study examines US health care spending in 2020. Health Aff. 2022, 41, 13–25. [Google Scholar] [CrossRef]
- Carrera-Hueso, F.J.; Álvarez-Arroyo, L.; Poquet-Jornet, J.E.; Vázquez-Ferreiro, P.; Martínez-Gonzalbez, R.; El-Qutob, D.; Ramón-Barrios, M.A.; Martínez-Martínez, F.; Poveda-Andrés, J.L.; Crespo-Palomo, C. Hospitalization budget impact during the COVID-19 pandemic in Spain. Health Econ. Rev. 2021, 11, 43. [Google Scholar] [CrossRef]
- Shrank, W.H.; DeParle, N.-A.; Gottlieb, S.; Jain, S.H.; Orszag, P.; Powers, B.W.; Wilensky, G.R. Health Costs and Financing: Challenges and Strategies for a New Administration: Commentary recommends health cost, financing, and other priorities for a new US administration. Health Aff. 2021, 40, 235–242. [Google Scholar] [CrossRef] [PubMed]
- OECD and European Observatory on Health Systems and Policies State of Health in the EU. España Perf. Sanit. Nac. 2019, 2019, 507–552.
- Valdrés López, A.; Bruna Barranco, I.; Martínez Giménez, L.; López Zapater, B.; Maestre Aguilar, R. Análisis del sistema sanitario de Estados Unidos de América, salud y negocio. Rev. Sanit. Investig. 2021, 2, 2660–7085. [Google Scholar]
- Ministerio de Sanidad. Consumo y Bienestar Social Principales Datos del Sistema Nacional de Salud; Ministerio de Sanidad: Madrid, Spain, 2021. [Google Scholar]
- Thivel, D.; Tremblay, A.; Genin, P.M.; Panahi, S.; Rivière, D.; Duclos, M. Physical Activity, Inactivity, and Sedentary Behaviors: Definitions and Implications in Occupational Health. Front. Public Health 2018, 6, 288. [Google Scholar] [CrossRef]
- Jakicic, J.M.; Rogers, R.J.; Davis, K.K.; Collins, K.A. Role of physical activity and exercise in treating patients with overweight and obesity. Clin. Chem. 2018, 64, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Jakicic, J.M.; Powell, K.E.; Campbell, W.W.; Dipietro, L.; Pate, R.R.; Pescatello, L.S.; Collins, K.A.; Bloodgood, B.; Piercy, K.L. Physical Activity and the Prevention of Weight Gain in Adults: A Systematic Review. Med. Sci. Sports Exerc. 2019, 51, 1262–1269. [Google Scholar] [CrossRef]
- van Dijk, J.-W.; van Loon, L.J.C. Exercise Strategies to Optimize Glycemic Control in Type 2 Diabetes: A Continuing Glucose Monitoring Perspective. Diabetes Spectr. 2015, 28, 24–31. [Google Scholar] [CrossRef] [Green Version]
- Amanat, S.; Ghahri, S.; Dianatinasab, A.; Fararouei, M.; Dianatinasab, M. Exercise and Type 2 Diabetes. In Physical Exercise for Human Health; Advances in Experimental Medicine and Biology Book Series; Springer: Singapore, 2020; Volume 1228, pp. 91–105. [Google Scholar]
- O’Neill, A.; O’Sullivan, K.; McCreesh, K. Lower levels of physical activity are associated with pain progression in older adults, a longitudinal study. Eur. J. Pain 2021, 25, 1462–1471. [Google Scholar] [CrossRef]
- Lima, L.V.; Abner, T.S.S.; Sluka, K.A. Does exercise increase or decrease pain? Central mechanisms underlying these two phenomena: Exercise pain and analgesia. J. Physiol. 2017, 595, 4141–4150. [Google Scholar] [CrossRef] [Green Version]
- Hu, M.X.; Turner, D.; Generaal, E.; Bos, D.; Ikram, M.K.; Ikram, M.A.; Cuijpers, P.; Penninx, B.W.J.H. Exercise interventions for the prevention of depression: A systematic review of meta-analyses. BMC Public Health 2020, 20, 1255. [Google Scholar] [CrossRef]
- Heissel, A.; Zech, P.; Rapp, M.A.; Schuch, F.B.; Lawrence, J.B.; Kangas, M.; Heinzel, S. Effects of exercise on depression and anxiety in persons living with HIV: A meta-analysis. J. Psychosom. Res. 2019, 126, 109823. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Sun, Y.; Zhan, J.; Wu, Z.; Zhang, P.; Wen, X.; Ge, S.; Han, X.; Lu, L. Effects of Exercise Therapy on Anxiety and Depression in Patients with Coronary Heart Disease: A Meta-Analysis of a Randomized Controlled Study. Front. Cardiovasc. Med. 2021, 8, 730155. [Google Scholar] [CrossRef] [PubMed]
- Mctiernan, A.; Friedenreich, C.M.; Katzmarzyk, P.T.; Powell, K.E.; Macko, R.; Buchner, D.; Pescatello, L.S.; Bloodgood, B.; Tennant, B.; Vaux-Bjerke, A.; et al. Physical Activity in Cancer Prevention and Survival: A Systematic Review. Med. Sci. Sports Exerc. 2019, 51, 1252–1261. [Google Scholar] [CrossRef]
- Koolhaas, C.M.; Dhana, K.; Rooij, F.J.A.; Schoufour, J.D.; Hofman, A.; Franco, O.H. Physical activity types and health-related quality of life among middle-aged and elderly adults: The Rotterdam Study. J. Nutr. Health Aging 2018, 22, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Anokye, N.K.; Trueman, P.; Green, C.; Pavey, T.G.; Taylor, R.S. Physical activity and health related quality of life. BMC Public Health 2012, 12, 624. [Google Scholar] [CrossRef] [Green Version]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Secretaría General de Información Sanitaria. Serie informes monográficos 2: Actividad física, descanso y sueño. In Encuesta Nacional de Salud de España 2017; Gobierno de España: Madrid, Spain, 2019. [Google Scholar]
- Moeini, B.; Rezapur-Shahkolai, F.; Bashirian, S.; Doosti-Irani, A.; Afshari, M.; Geravandi, A. Effect of interventions based on regular physical activity on weight management in adolescents: A systematic review and a meta-analysis. Syst. Rev. 2021, 10, 52. [Google Scholar] [CrossRef]
- Takagi, D.; Nishida, Y.; Fujita, D. Age-associated changes in the level of physical activity in elderly adults. J. Phys. Ther. Sci. 2015, 27, 3685–3687. [Google Scholar] [CrossRef] [Green Version]
- Sari, N. Physical inactivity and its impact on healthcare utilization. Health Econ. 2009, 18, 885–901. [Google Scholar] [CrossRef]
- Arocha Rodulfo, J.I. Sedentarism, a disease from xxi century. Clínica E Investig. En Arterioscler. 2019, 31, 233–240. [Google Scholar] [CrossRef]
- León-Latre, M.; Moreno-Franco, B.; Andrés-Esteban, E.M.; Ledesma, M.; Laclaustra, M.; Alcalde, V.; Peñalvo, J.L.; Ordovás, J.M.; Casasnovas, J.A. Sedentary Lifestyle and Its Relation to Cardiovascular Risk Factors, Insulin Resistance and Inflammatory Profile. Rev. Esp. Cardiol. Engl. Ed. 2014, 67, 449–455. [Google Scholar] [CrossRef] [PubMed]
- Hafner, M.; Yerushalmi, E.; Stepanek, M.; Phillips, W.; Pollard, J.; Deshpande, A.; Whitmore, M.; Millard, F.; Subel, S.; van Stolk, C. Estimating the global economic benefits of physically active populations over 30 years (2020–2050). Br. J. Sports Med. 2020, 54, 1482–1487. [Google Scholar] [CrossRef] [PubMed]
- Langhammer, B.; Bergland, A.; Rydwik, E. The Importance of Physical Activity Exercise among Older People. BioMed Res. Int. 2018, 2018, 7856823. [Google Scholar] [CrossRef] [PubMed]
- Bueno, D.R.; Marucci, M.d.F.N.; Codogno, J.S.; Roediger, M.d.A. Os custos da inatividade física no mundo: Estudo de revisão. Cienc. Saude Coletiva 2016, 21, 1001–1010. [Google Scholar] [CrossRef] [Green Version]
- Kang, S.; Xiang, X. Physical activity and health services utilization and costs among U.S. adults. Prev. Med. 2017, 96, 101–105. [Google Scholar] [CrossRef]
- Wullems, J.A.; Verschueren, S.M.P.; Degens, H.; Morse, C.I.; Onambélé, G.L. A review of the assessment and prevalence of sedentarism in older adults, its physiology/health impact and non-exercise mobility counter-measures. Biogerontology 2016, 17, 547–565. [Google Scholar] [CrossRef] [Green Version]
- Cunningham, C.; O’ Sullivan, R.; Caserotti, P.; Tully, M.A. Consequences of physical inactivity in older adults: A systematic review of reviews and meta-analyses. Scand. J. Med. Sci. Sports 2020, 30, 816–827. [Google Scholar] [CrossRef]
- Dogra, S.; Ashe, M.C.; Biddle, S.J.H.; Brown, W.J.; Buman, M.P.; Chastin, S.; Gardiner, P.A.; Inoue, S.; Jefferis, B.J.; Oka, K.; et al. Sedentary time in older men and women: An international consensus statement and research priorities. Br. J. Sports Med. 2017, 51, 1526–1532. [Google Scholar] [CrossRef]
- Gebel, K.; Ding, D.; Chey, T.; Stamatakis, E.; Brown, W.J.; Bauman, A.E. Effect of moderate to vigorous physical activity on all-cause mortality in middle-aged and older Australians. JAMA Intern. Med. 2015, 175, 970–977. [Google Scholar] [CrossRef]
- Su, C.-L.; Wang, L.; Ho, C.-C.; Nfor, O.N.; Hsu, S.-Y.; Lee, C.-T.; Ko, P.-C.; Lin, Y.-T.; Liaw, Y.-P. Physical activity is associated with lower health care costs among Taiwanese individuals with diabetes mellitus. Medicine 2020, 99, e19613. [Google Scholar] [CrossRef]
- Towne, S.D.; Li, Y.; Lee, S.; Smith, M.L.; Han, G.; Quinn, C.; Du, Y.; Benden, M.; Ory, M.G. Physical activity and associated medical cost savings among at-risk older adults participating a community-based health & wellness program. PLoS ONE 2018, 13, e0198239. [Google Scholar] [CrossRef]
- Aragón-Vela, J.; Delgado-Floody, P.; Guzmán-Guzmán, I.P.; Salas-Sánchez, J.; Martínez-Redondo, M.; Lucena Zurita, M.; Herrador Sánchez, J.; Cardona Linares, A.J.; Consuegra González, P.J.; Santos E Campos, M.A.; et al. Effect of COVID-19 confinement on physical activity patterns in relation to sociodemographic parameters in Spanish population. J. Sports Med. Phys. Fit. 2021, 62, 830–837. [Google Scholar] [CrossRef] [PubMed]
- López-Sánchez, G.F.; López-Bueno, R.; Gil-Salmerón, A.; Zauder, R.; Skalska, M.; Jastrzębska, J.; Jastrzębski, Z.; Schuch, F.B.; Grabovac, I.; Tully, M.A.; et al. Comparison of physical activity levels in Spanish adults with chronic conditions before and during COVID-19 quarantine. Eur. J. Public Health 2021, 31, 161–166. [Google Scholar] [CrossRef]
- Ministerio de Sanidad. Consumo y Bienestar Social Cuestionario de Adultos. In Encuesta Nacional de Salud de España 2017; Gobierno de España: Madrid, Spain, 2019. [Google Scholar]
- Sanidad Consumo, M.; Social, B. Encuesta Nacional de Salud 2017 ENSE 2017 Metodología. Encuesta Nac. Salud 2017, 64, 1381–1395. [Google Scholar]
- Craig, C.L.; Marshall, A.L.; SjöStröM, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Denche-Zamorano, Á.; Franco-García, J.M.; Carlos-Vivas, J.; Mendoza-Muñoz, M.; Pereira-Payo, D.; Pastor-Cisneros, R.; Merellano-Navarro, E.; Adsuar, J.C. Increased Risks of Mental Disorders: Youth with Inactive Physical Activity. Healthcare 2022, 10, 237. [Google Scholar] [CrossRef]
- European Parliament and of the Council Regulation (EU) 2016/679 of the of 27 April 2016 on the Protection of Natural Persons with Regard to the Processing of Personal Data and on the Free Movement of such Data, and Repealing Directive 95/46/EC (General Data Protection Regulation); Official Journal of the European Union: Luxembourg, 2016.
- Ministerio de Sanidad. Consumo y Bienestar Social, Gobierno de España Encuesta Nacional de Salud; Ministerio de Sanidad: Madrid, Spain, 2017. [Google Scholar]
- Luben, R.; Hayat, S.; Wareham, N.; Pharoah, P.; Khaw, K.-T. Usual physical activity and subsequent hospital usage over 20 years in a general population: The EPIC-Norfolk cohort. BMC Geriatr. 2020, 20, 165. [Google Scholar] [CrossRef]
- Bertakis, K.D.; Azari, R.; Helms, L.J.; Callahan, E.J.; Robbins, J.A. Gender differences in the utilization of health care services. J. Fam. Pract. 2000, 49, 147–152. [Google Scholar]
- Hunt, K.; Adamson, J.; Hewitt, C.; Nazareth, I. Do women consult more than men? A review of gender and consultation for back pain and headache. J. Health Serv. Res. Policy 2011, 16, 108–117. [Google Scholar] [CrossRef] [Green Version]
- Redondo-Sendino, Á.; Guallar-Castillón, P.; Banegas, J.R.; Rodríguez-Artalejo, F. Gender differences in the utilization of health-care services among the older adult population of Spain. BMC Public Health 2006, 6, 155. [Google Scholar] [CrossRef] [Green Version]
- Parra-Rizo, M.A. Diferencias de género en la percepción de salud en personas mayores de 60 años físicamente activas = Gender differences in the perception of health in physically active people over 60 years of age. Rev. Española Comun. Salud 2017, 8, 219–227. [Google Scholar] [CrossRef]
- Gomes, R.; Do Nascimento, E.F.; De Araújo, F.C. Por que os homens buscam menos os serviços de saúde do que as mulheres? As explicações de homens com baixa escolaridade e homens com ensino superior. Cad. Saude Publica 2007, 23, 565–574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deeks, A.; Lombard, C.; Michelmore, J.; Teede, H. The effects of gender and age on health related behaviors. BMC Public Health 2009, 9, 213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Templeton, K.J. Sex and Gender Issues in Pain Management. J. Bone Jt. Surg. 2020, 102, 32–35. [Google Scholar] [CrossRef]
- Bacigalupe, A.; Cabezas, A.; Bueno, M.B.; Martín, U. Gender as a determinant of mental health and its medicalization. Gac. Sanit. 2020, 34, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Caner, A.; Cilasun, S.M. Health Care Services and the Elderly: Utilization and Satisfaction in the Aftermath of the Turkish Health Transformation Program. Gerontol. Geriatr. Med. 2019, 5, 233372141882286. [Google Scholar] [CrossRef] [PubMed]
- Nie, J.X.; Wang, L.; Tracy, C.S.; Moineddin, R.; Upshur, R.E. Health care service utilization among the elderly: Findings from the Study to Understand the Chronic Condition Experience of the Elderly and the Disabled (SUCCEED project). J. Eval. Clin. Pract. 2008, 14, 1044–1049. [Google Scholar] [CrossRef]
- Kalseth, J.; Halvorsen, T. Health and care service utilisation and cost over the life-span: A descriptive analysis of population data. BMC Health Serv. Res. 2020, 20, 435. [Google Scholar] [CrossRef]
- Amini, H.; Habibi, S.; Islamoglu, A.H.; Isanejad, E.; Uz, C.; Daniyari, H. COVID-19 pandemic-induced physical inactivity: The necessity of updating the Global Action Plan on Physical Activity 2018-2030. Environ. Health Prev. Med. 2021, 26, 32. [Google Scholar] [CrossRef]


{kind=link}
| Age (Years) | Men = 8238 | Women = 8961 | Total = 17,199 | p |
|---|---|---|---|---|
| Median (IQR) | 47 (20) | 47 (21) | 47 (21) | 0.467 |
| Mean (SD) | 46.7 (13.2) | 46.9 (13.3) | 46.8 (13.2) | - |
| Age Group (years) | Men n (%) | Women n (%) | Total n (%) | p * |
| 18–34 | 1573 (19.1) a | 1743 (19.5) a | 3316 (19.3) | 0.227 |
| 35–49 | 3007 (36.5) a | 3188 (35.6) a | 6195 (36.0) | |
| 50–64 | 2874 (34.9) a | 3103 (34.6) a | 5977 (34.8) | |
| 65–69 | 784 (9.5) a | 927 (10.3) a | 1711 (9.9) | |
| Hospitalization | Men = 8238 n (%) | Women = 8961 n (%) | Total = 17,199 n (%) | p * |
| Yes | 601 (7.3) a | 615 (6.9) a | 1216 (7.1) | 0.269 |
| No | 7637 (92.7) a | 8346 (93.1) a | 15,983 (92.9) | |
| Use of Emergency Services | Men = 8238 n (%) | Women = 8961 n (%) | Total = 17,199 n (%) | p * |
| Yes | 2181 (26.5) a | 2784 (31.1) b | 4965 (28.9) | <0.001 |
| No | 6057 (73.5) a | 6177 (68.9) b | 12,234 (71.1) | |
| Visits to Emergency Services | Men = 8234 | Women = 8953 | Total = 17,187 | p |
| Median (IQR) | 0 (1) | 0 (1) | 0 (1) | <0.001 |
| Mean (SD) | 0.42 (1.02) | 0.60 (1.44) | 0.51 (1.27) | - |
| CI (95%) | 0.40–0.44 | 0.57–0.63 | 0.49–0.53 | - |
| PAL | Men = 8199 n (%) | Women = 8942 n (%) | Total = 17,141 n (%) | p * |
| Inactive (PAI = 0) | 1156 (14.1) | 1326 (14.8) | 2482 (14.5) | <0.001 |
| Walkers (PAI = 0) | 3335 (40.7) | 4566 (51.1) | 7901 (46.1) | |
| Low (PAI = 1–15) | 1077 (13.1) | 1262 (14.1) | 2339 (13.6) | |
| Medium PAI = 16–30) | 1273 (15.5) | 1076 (12.0) | 2349 (13.7) | |
| High (PAI = 31–45) | 877 (10.7) | 476 (5.3) | 1353 (7.9) | |
| Very High (PAI > 45) | 481 (5.9) | 236 (2.6) | 717 (4.2) |
| Men (n = 8238) | Women (n = 8961) | Total (n = 17,199) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Age Group (Years) | Yes | No | p | Yes | No | p | Yes | No | p |
| 18–34 (n = 3316) | 64 (4.1) a | 1509 (95.9) b | <0.001 | 87 (5.0) a | 1656 (95.0) b | <0.001 | 151 (4.6) a | 3165 (95.4) b | <0.001 |
| 35–49 (n = 6195) | 170 (5.7) a | 2837 (94.3) b | 176 (5.5) a | 3012 (94.5) b | 346 (5.6) a | 5849 (94.4) b | |||
| 50–64 (n = 5977) | 261 (9.1) a | 2613 (90.9) b | 249 (8.0) a | 2854 (92.0) b | 510 (8.5) a | 5467 (91.5) b | |||
| 65–69 (n = 1711) | 106 (13.5) a | 678 (86.5) b | 103 (11.1) a | 824 (88.9) b | 209 (12.2) a | 1502 (87.8) b | |||
| Total (n = 17,199) | 601 (7.3) | 7637 (92.7) | 615 (6.9) | 8346 (93.1) | 1216 (7.1) | 15,983 (92.9) | |||
| Men (n = 8199) | Women (n = 8942) | Total (n = 17,141) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| PAL | Yes | No | p | Yes | No | p | Yes | No | p |
| Inactive n = 2482 | 137 (11.9) a | 1019 (88.1) b | 0.001 | 150 (11.3) a | 1176 (88.7) b | <0.001 | 287 (11.6) a | 2195 (88.4) b | <0.001 |
| Walkers n = 7901 | 281 (8.4) a | 3054 (91.6) b | 320 (7.0) a | 4246 (93.0) a | 601 (7.6) a | 7300 (92.4) b | |||
| Low n = 2339 | 58 (5.4) a | 1019 (94.6) b | 67 (5.3) a | 1195 (94.7) b | 125 (5.3) a | 2214 (94.7) b | |||
| Medium n = 2349 | 73 (5.7) a | 1200 (94.3) b | 50 (4.6) a | 1026 (95.4) b | 123 (5.2) a | 2226 (94.8) b | |||
| High n = 1353 | 32 (3.6) a | 845 (96.4) b | 19 (4.0) a | 457 (96.0) b | 51 (3.8) a | 1302 (96.2) b | |||
| Very High n = 717 | 18 (3.7) a | 463 (96.3) b | 9 (3.8) a | 227 (96.2) b | 27 (3.8) a | 690 (96.2) b | |||
| Total n = 17,141 | 599 (7.3) | 7600 (92.7) | 615 (6.9) | 8327 (93.1) | 1214 (7.1) | 15,927 (92.9) | |||
| 18–34 Years (n = 3297) | 35–49 Years (n = 6177) | 50–64 Years (n = 5956) | 65–69 Years (n = 1711) | Total (n = 17,141) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PAL | Yes n (%) | No n (%) | p | Yes n (%) | No n (%) | p | Yes n (%) | No n (%) | p | Yes n (%) | No n (%) | p | Yes n (%) | No n (%) | p |
| Inactive n = 2485 | 33 (7.8) a | 388 (92.2) b | 0.002 | 79 (8.4) a | 856 (91.6) b | <0.001 | 127 (14.5) a | 751 (85.5) b | <0.001 | 48 (19.4) a | 200 (80.6) b | 0.002 | 287 (11.6) a | 2195 (88.4) b | <0.001 |
| Walkers n = 7910 | 61 (5.0) a | 1158 (95.0) a | 158 (6.2) a | 2407 (93.8) a | 263 (8.4) a | 2861 (91.6) a | 119 (12.0) a | 874 (88.0) a | 601 (7.6) a | 7300 (92.4) b | |||||
| Low n = 2342 | 22 (4.6) a | 456 (95.4) a | 38 (3.9) a | 932 (96.1) b | 52 (7.5) a | 644 (92.5) a | 13 (6.7) a | 182 (93.3) b | 125 (5.3) a | 2214 (94.7) b | |||||
| Medium n = 2353 | 18 (3.4) a | 512 (96.6) a | 43 (4.9) a | 838 (95.1) a | 39 (5.2) a | 704 (94.8) b | 23 (11.8) a | 172 (88.2) a | 123 (5.2) a | 2226 (94.8) b | |||||
| High n = 1355 | 14 (3.2) a | 427 (96.8) a | 21 (3.8) a | 533 (96.2) a | 12 (3.9) a | 294 (96.1) b | 4 (7.7) a | 48 (92.3) a | 51 (3.8) a | 1302 (96.2) b | |||||
| Very High n = 734 | 3 (1.4) a | 205 (98.6) b | 7 (2.6) a | 265 (97.4) b | 15 (7.2) a | 194 (92.8) a | 2 (7.1) a | 26 (92.9) a | 27 (3.8) a | 690 (96.2) b | |||||
| Total n = 17,141 | 151 (4.6) | 3146 (95.4) | 346 (5.6) | 5831 (94.4) | 508 (8.5) | 5448 (91.5) | 209 (12.2) | 1502 (87.8) | 1214 (7.1) | 15,927 (92.9) | |||||
| Men (n = 8238) | Women (n = 8961) | Total (n = 17,199) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Age Groups | Yes n (%) | No n (%) | p | Yes n (%) | No n (%) | p | Yes n (%) | No n (%) | p |
| 18–34 years (n = 3316) | 486 (30.9) a | 1087 (69.1) b | <0.001 | 673 (38.6) a | 1070 (61.4) b | <0.001 | 1159 (35.0) a | 2157 (65.0) b | <0.001 |
| 35–49 years (n = 6195) | 813 (27.0) a | 2194 (73.0) a | 977 (30.6) a | 2211 (69.4) a | 1790 (28.9) a | 4405 (71.1) a | |||
| 50–64 years (n = 5977) | 688 (23.9) a | 2186 (76.1) b | 865 (27.9) a | 2238 (72.1) b | 1553 (26.0) a | 4424 (74.0) b | |||
| 65–69 years (n = 1711) | 194 (24.7) a | 590 (75.3) a | 269 (29.0) a | 658 (71.0) a | 463 (27.1) a | 1248 (72.9) a | |||
| Total (n = 17,199) | 2181 (26.5) | 6057 (73.5) | 2784 (31.1) | 6177 (68.9) | 4965 (28.8) | 12,234 (71.2) | |||
| Men (n = 8199) | Women (n = 8942) | Total (n = 17,141) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| PAL | Yes n (%) | No n (%) | p | Yes n (%) | No n (%) | p | Yes n (%) | No n (%) | p |
| Inactive n = 2482 | 407 (35.2) a | 749 (64.8) b | 0.002 | 550 (41.5) a | 776 (58.5) b | <0.001 | 957 (38.6) a | 1525 (61.4) b | <0.001 |
| Walkers n = 7901 | 883 (26.5) a | 2452 (73.5) a | 1409 (30.9) a | 3157 (69.1) a | 2292 (29.0) a | 5609 (71.0) a | |||
| Low n = 2339 | 244 (22.7) a | 833 (77.3) b | 353 (28.0) a | 909 (72.0) b | 597 (25.5) a | 1742 (74.5) b | |||
| Medium n = 2349 | 315 (24.7) a | 958 (75.3) a | 285 (26.5) a | 791 (73.5) b | 600 (25.5) a | 1749 (74.5) b | |||
| High n = 1353 | 227 (25.9) a | 650 (74.1) a | 127 (26.7) a | 349 (73.3) b | 354 (26.2) a | 999 (73.8) b | |||
| Very High n = 717 | 99 (20.6) a | 382 (79.4) b | 60 (25.4) a | 176 (74.6) a | 159 (22.2) a | 558 (77.8) b | |||
| Total n = 17,141 | 2175 (26.5) | 6024 (73.5) | 2784 (31.1) | 6158 (68.9) | 4959 (28.9) | 12,182 (71.1) | |||
| 18–34 Years (n = 3297) | 35–49 Years (n = 6177) | 50–64 Years (n = 5956) | 65–69 Years (n = 1711) | Total (n = 17,141) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PAL | Yes n (%) | No n (%) | p | Yes n (%) | No n (%) | p | Yes n (%) | No n (%) | p | Yes n (%) | No n (%) | p | Yes n (%) | No n (%) | p |
| Inactive n = 2482 | 178 (42.3) a | 243 (57.7) b | 0.001 | 343 (36.7) a | 592 (63.3) b | <0.001 | 334 (38.0) a | 544 (62.0) b | <0.001 | 102 (41.1) a | 146 (58.9) b | 0.001 | 957 (38.6) a | 1525 (61.4) b | <0.001 |
| Walkers n = 7901 | 454 (37.2) a | 765 (62.8) b | 758 (29.6) a | 1807 (70.4) a | 809 (25.9) a | 2315 (74.1) a | 271 (27.3) a | 722 (72.7) a | 2292 (29.0) a | 5609 (71.0) a | |||||
| Low n = 2339 | 149 (31.2) a | 329 (68.8) a | 265 (27.3) a | 705 (72.7) b | 139 (20.0) a | 557 (80.0) b | 44 (22.6) a | 151 (77.4) a | 597 (25.5) a | 1742 (74.5) b | |||||
| Medium n = 2349 | 178 (33.6) a | 352 (66.4) a | 229 (26.0) a | 652 (74.0) b | 161 (21.7) a | 582 (78.3) b | 32 (16.4) a | 163 (83.6) b | 600 (25.5) a | 1749 (74.5) b | |||||
| High n = 1353 | 144 (32.7) a | 297 (67.3) a | 134 (24.2) a | 420 (75.8) b | 68 (22.2) a | 238 (77.8) a | 8 (15.4) a | 44 (84.6) a | 354 (26.2) a | 999 (73.8) b | |||||
| Very High n = 717 | 54 (26.0) a | 154 (74.0) b | 60 (22.1) a | 212 (77.9) b | 39 (18.7) a | 170 (81.3) b | 6 (21.4) a | 22 (78.6) a | 159 (22.2) a | 558 (74.8) b | |||||
| Total n = 17,141 | 1157 (35.1) | 2140 (64.9) | 1789 (29.0) | 4388 (71.0) | 1550 (26.0) | 4406 (74.0) | 463 (27.1) | 1248 (72.9) | 4959 (28.9) | 12,182 (71.1) | |||||
| Men | ||||||||
| PAL | n | Mean | (SD) | CI (95%) | Med | (IQR) | p | p * |
| Inactive | 1156 | 0.66 | (1.39) | 0.58–0.74 | 0 | (1) | <0.001 | a |
| Walkers | 3333 | 0.43 | (1.06) | 0.39–0.46 | 0 | (1) | b | |
| Low | 1076 | 0.34 | (0.91) | 0.29–0.40 | 0 | (0) | c | |
| Medium | 1273 | 0.35 | (0.83) | 0.31–0.40 | 0 | (0) | bc | |
| High | 877 | 0.37 | (0.79) | 0.32–0.42 | 0 | (1) | bc | |
| Very High | 481 | 0.28 | (0.65) | 0.23–0.34 | 0 | (0) | c | |
| Women | ||||||||
| PAL | n | Mean | (SD) | CI (95%) | Med | (IQR) | p | p * |
| Inactive | 1322 | 0.99 | (2.22) | 0.87–1.11 | 0 | (1) | <0.001 | a |
| Walkers | 4562 | 0.58 | (1.34) | 0.54–0.61 | 0 | (1) | b | |
| Low | 1262 | 0.46 | (1.08) | 0.40–0.52 | 0 | (1) | c | |
| Medium | 1076 | 0.44 | (1.09) | 0.37–0.50 | 0 | (1) | c | |
| High | 476 | 0.47 | (1.04) | 0.37–0.56 | 0 | (1) | b | |
| Very High | 236 | 0.51 | (1.30) | 0.35–0.68 | 0 | (1) | b | |
| Total | ||||||||
| PAL | n | Mean | (SD) | CI (95%) | Med | (IQR) | p | p * |
| Inactive | 2478 | 0.84 | (1.89) | 0.76–0.91 | 0 | (1) | <0.001 | a |
| Walkers | 7895 | 0.51 | (1.23) | 0.49–0.54 | 0 | (1) | b | |
| Low | 2338 | 0.41 | (1.00) | 0.37–0.45 | 0 | (1) | c | |
| Medium | 2349 | 0.39 | (0.96) | 0.35–0.43 | 0 | (1) | c | |
| High | 1353 | 0.41 | (0.89) | 0.36–0.45 | 0 | (1) | c | |
| Very High | 717 | 0.36 | (0.92) | 0.29–0.43 | 0 | (0) | c | |
| B | SE | Wald | Df | Sig | Exp(B) | 95% CI for EXP(B) | ||
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| Years | 0.031 | 0.003 | 154.816 | 1 | <0.001 | 1.032 | 1.027 | 1.037 |
| Inactive | 56.134 | 5 | <0.001 | |||||
| Walkers | −0.350 | 0.079 | 19.473 | 1 | <0.001 | 0.705 | 0.603 | 0.823 |
| Low | −0.561 | 0.115 | 23.698 | 1 | <0.001 | 0.571 | 0.455 | 0.715 |
| Medium | −0.593 | 0.116 | 26.191 | 1 | <0.001 | 0.553 | 0.440 | 0.694 |
| High | −0.848 | 0.161 | 27.799 | 1 | <0.001 | 0.428 | 0.313 | 0.587 |
| Very High | −0.826 | 0.211 | 15.294 | 1 | <0.001 | 0.438 | 0.289 | 0.662 |
| Sex | −0.203 | 0.062 | 10.526 | 1 | <0.001 | 0.817 | 0.723 | 0.923 |
| Urgencies | −1.704 | 0.064 | 704.894 | 1 | <0.001 | 0.182 | 0.160 | 0.206 |
| Constant | −2.668 | 0.146 | 333.764 | 1 | <0.001 | 0.069 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Denche-Zamorano, Á.; Mendoza-Muñoz, M.; Carlos-Vivas, J.; Muñoz-Bermejo, L.; Rojo-Ramos, J.; Giakoni-Ramírez, F.; Godoy-Cumillaf, A.; Barrios-Fernandez, S. Associations between Physical Activity Level and Health Services Use in Spanish Adults. Int. J. Environ. Res. Public Health 2022, 19, 8867. https://doi.org/10.3390/ijerph19148867
Denche-Zamorano Á, Mendoza-Muñoz M, Carlos-Vivas J, Muñoz-Bermejo L, Rojo-Ramos J, Giakoni-Ramírez F, Godoy-Cumillaf A, Barrios-Fernandez S. Associations between Physical Activity Level and Health Services Use in Spanish Adults. International Journal of Environmental Research and Public Health. 2022; 19(14):8867. https://doi.org/10.3390/ijerph19148867
Chicago/Turabian StyleDenche-Zamorano, Ángel, María Mendoza-Muñoz, Jorge Carlos-Vivas, Laura Muñoz-Bermejo, Jorge Rojo-Ramos, Frano Giakoni-Ramírez, Andrés Godoy-Cumillaf, and Sabina Barrios-Fernandez. 2022. "Associations between Physical Activity Level and Health Services Use in Spanish Adults" International Journal of Environmental Research and Public Health 19, no. 14: 8867. https://doi.org/10.3390/ijerph19148867