
Effects of Free Play and Partly Structured Playground Activity on Motor Competence in Preschool Children: A Pragmatic Comparison Trial

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
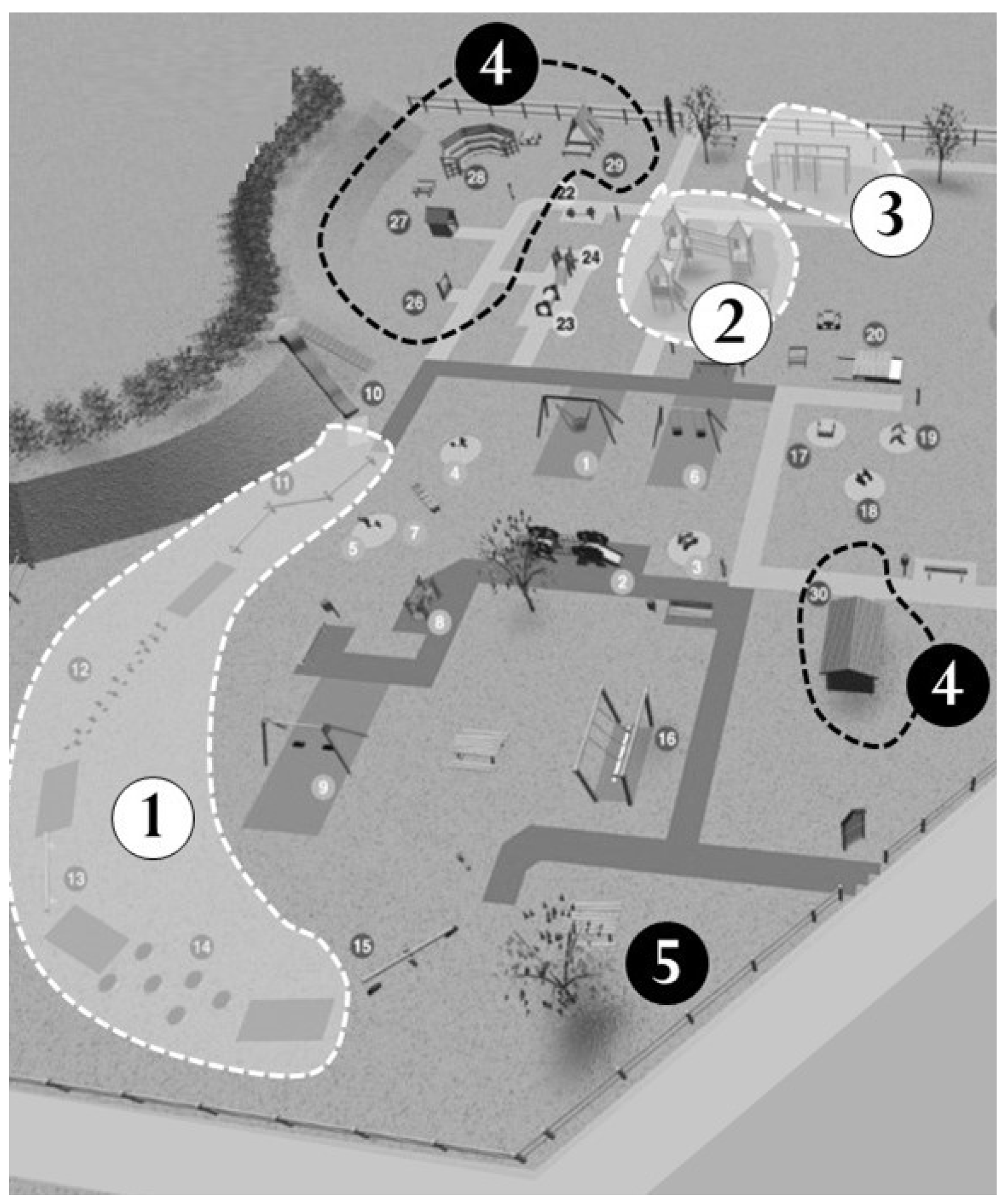
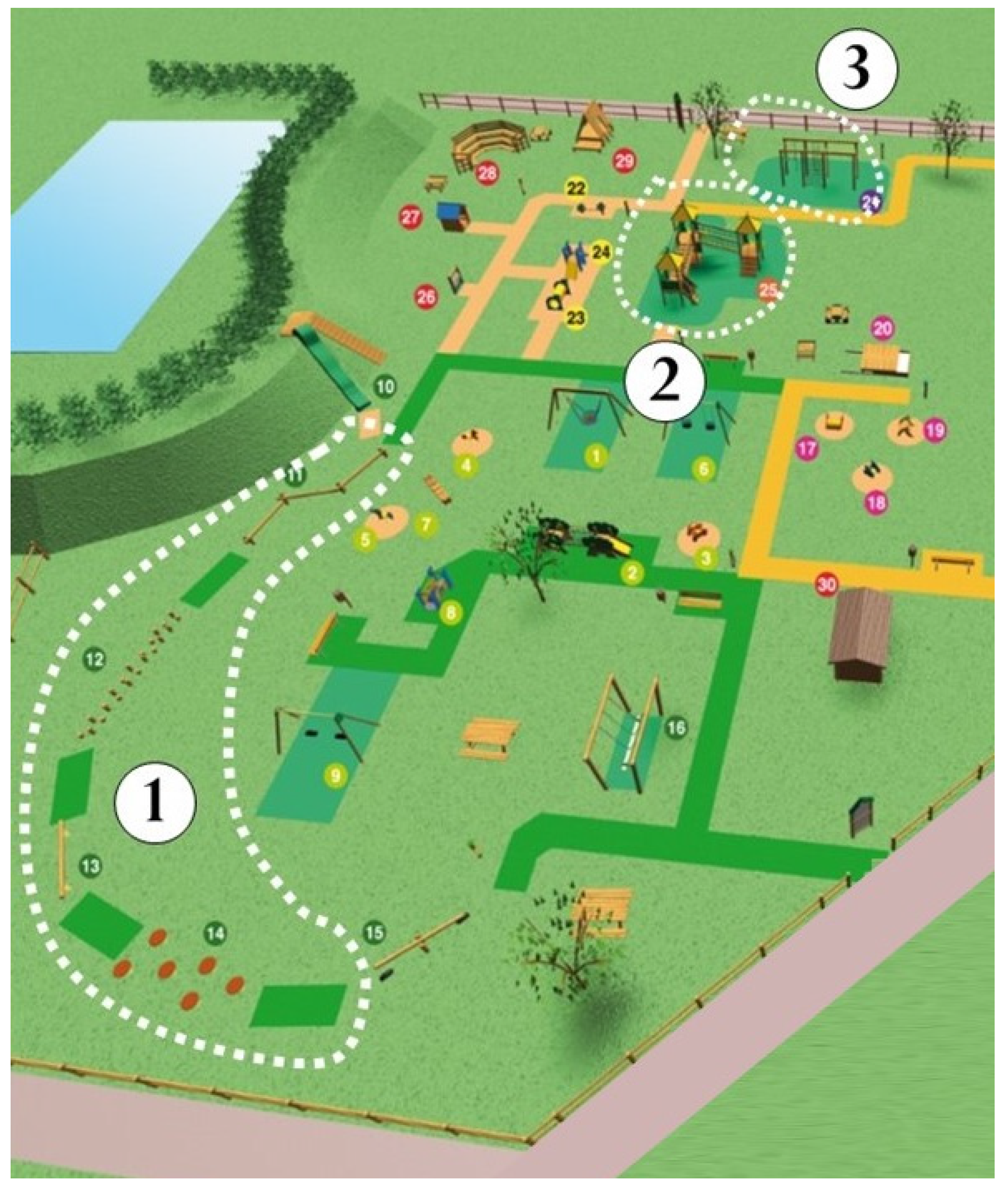
2.3. The Primo Sport 0246 Playground
2.4. Organization of Activities at the Playground
2.4.1. The Group of Partly Structured Activity
2.4.2. The Group of Free Play
2.4.3. The Control Group
2.5. Assessment of Motor Competence
2.5.1. Test of Motor Competence (TMC)
2.5.2. Movement Assessment Battery for Children (MABC-2)
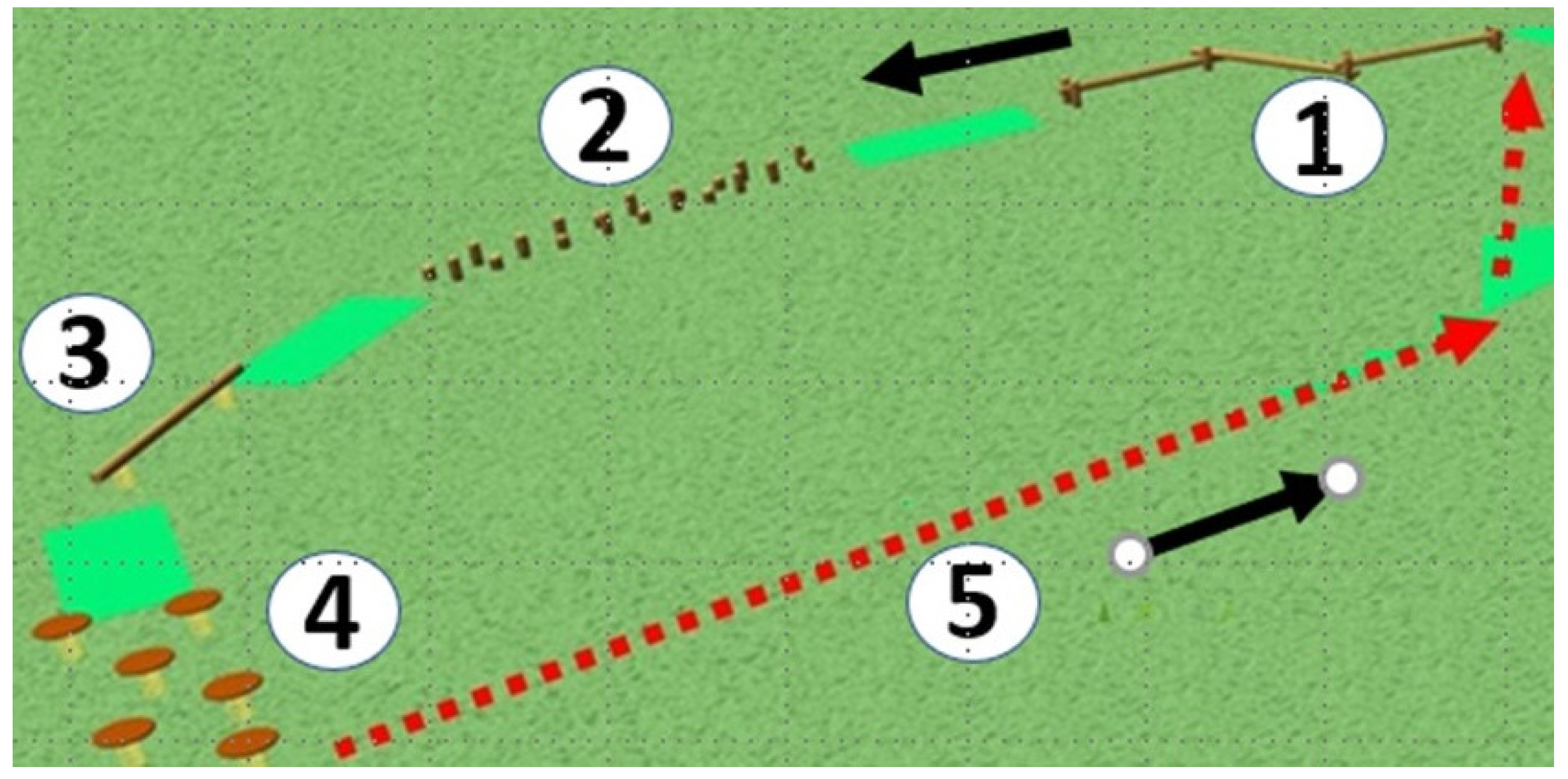
2.5.3. Playground-Specific Tests
2.5.4. Balance on Elastic Platforms Task
2.5.5. Balance on Beam Task
2.6. Statistical Analysis
3. Results
3.1. Test of Motor Competence (TMC)
Movement Assessment Battery for Children (MABC-2)
3.2. Playground-Specific Assessments
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bardid, F.; Rudd, J.; Elenoir, M.; Polman, R.; Barnett, L.M. Cross-cultural comparison of motor competence in children from Australia and Belgium. Front. Psychol. 2015, 6, 964. [Google Scholar] [CrossRef] [PubMed]
- Brian, A.; Bardid, F.; Barnett, L.M.; Deconinck, F.J.; Lenoir, M.; Goodway, J.D. Actual and Perceived Motor Competence Levels of Belgian and United States Preschool Children. J. Mot. Learn. Dev. 2018, 6, S320–S336. [Google Scholar] [CrossRef] [Green Version]
- Brian, A.; Pennell, A.; Taunton, S.; Starrett, A.; Howard-Shaughnessy, C.; Goodway, J.D.; Wadsworth, D.; Rudisill, M.; Stodden, D. Motor Competence Levels and Developmental Delay in Early Childhood: A Multicenter Cross-Sectional Study Conducted in the USA. Sports Med. 2019, 49, 1609–1618. [Google Scholar] [CrossRef] [PubMed]
- Andersen, E.; Borch-Jenssen, J.; Øvreås, S.; Ellingsen, H.; Jørgensen, K.A.; Moser, T. Objectively measured physical activity level and sedentary behavior in Norwegian children during a week in preschool. Prev. Med. Rep. 2017, 7, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Ellis, Y.G.; Cliff, D.P.; Janssen, X.; Jones, R.A.; Reilly, J.J.; Okely, A.D. Sedentary time, physical activity and compliance with IOM recommendations in young children at childcare. Prev. Med. Rep. 2017, 7, 221–226. [Google Scholar] [CrossRef]
- Burton, A.W.; Rodgerson, R.W. New Perspectives on the Assessment of Movement Skills and Motor Abilities. Adapt. Phys. Act. Q. 2001, 18, 347–365. [Google Scholar] [CrossRef]
- Henderson, S.E.; Sugden, D.A.; Barnett, A. Movement Assessment Battery for Children, 2nd ed.; Examiner’s Manual; Harcourt Assessment: London, UK, 2007. [Google Scholar]
- Cattuzzo, M.T.; Henrique, R.D.S.; Ré, A.; de Oliveira, I.S.; Melo, B.M.; Moura, M.D.S.; de Araújo, R.C.; Stodden, D. Motor competence and health related physical fitness in youth: A systematic review. J. Sci. Med. Sport 2016, 19, 123–129. [Google Scholar] [CrossRef]
- Lima, R.A.; Pfeiffer, K.; Larsen, L.R.; Bugge, A.; Møller, N.C.; Anderson, L.B.; Stodden, D. Physical Activity and Motor Competence Present a Positive Reciprocal Longitudinal Relationship Across Childhood and Early Adolescence. J. Phys. Act. Health 2017, 14, 440–447. [Google Scholar] [CrossRef]
- Vedul-Kjelsås, V.; Sigmundsson, H.; Stensdotter, A.K.; Haga, M. The relationship between motor competence, physical fitness and self-perception in children. Child Care Health Dev. 2012, 38, 394–402. [Google Scholar] [CrossRef]
- Timler, A.; McIntyre, F.; Rose, E.; Hands, B. Exploring the influence of self-perceptions on the relationship between motor competence and identity in adolescents. PLoS ONE 2019, 14, e0224653. [Google Scholar] [CrossRef]
- Jefferies, P.; Ungar, M.; Aubertin, P.; Kriellaars, D. Physical Literacy and Resilience in Children and Youth. Front. Public Health 2019, 7, 346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sigmundsson, H.; Haga, M. Motor competence is associated with physical fitness in four to six-year-old pre-school children. Eur. Early Child. Educ. Res. J. 2016, 24, 477–488. [Google Scholar] [CrossRef]
- Stodden, D.F.; Goodway, J.D.; Langendorfer, S.J.; Roberton, M.A.; Rudisill, M.E.; Garcia, C.; Garcia, L.E. A developmental perspective on the role of motor skill competence in physical activity: An emergent relationship. Quest 2008, 60, 290–306. [Google Scholar] [CrossRef]
- Hulteen, R.M.; Morgan, P.J.; Barnett, L.M.; Stodden, D.F.; Lubans, D.R. Development of Foundational Movement Skills: A Conceptual Model for Physical Activity Across the Lifespan. Sports Med. 2018, 48, 1533–1540. [Google Scholar] [CrossRef]
- Truelove, S.; Vanderloo, L.M.; Tucker, P. Defining and Measuring Active Play Among Young Children: A Systematic Review. J. Phys. Act. Health 2017, 14, 155–166. [Google Scholar] [CrossRef]
- Lubans, D.R.; Morgan, P.J.; Cliff, D.P.; Barnett, L.M.; Okely, A.D. Fundamental movement skills in children and adolescents: Review of associated health benefits. Sports Med. 2010, 40, 1019–1035. [Google Scholar] [CrossRef] [Green Version]
- MacNamara, A.; Collins, D.; Giblin, S. Just let them play? Deliberate preparation as the most appropriate foundation for lifelong physical activity. Front. Psychol. 2015, 6, 1548. [Google Scholar] [CrossRef]
- Giblin, S.; Collins, D.; MacNamara, A.; Kiely, J. “Deliberate Preparation” as an Evidence-Based Focus for Primary Physical Education. Quest 2014, 66, 385–395. [Google Scholar] [CrossRef]
- WHO. Guidelines on Physical Activity, Sedentary Behaviour and Sleep for Children under 5 Years of Age; Licence: CC BY-NC-SA 3.0 IGO; World Health Organization: Geneva, Switzerland, 2019; Available online: https://www.who.int/publications/i/item/9789241550536 (accessed on 3 June 2022).
- Newell, K.M. Constraints on the Development of Coordination. In Motor Development in Children: Aspects of Coordination and Control; Wade, M.G., Whiting, H.T.A., Eds.; Martinus Nijhoff: Dordrecht, The Netherlands, 1986; pp. 341–360. [Google Scholar]
- Adolph, K.E.; Hoch, J.E. Motor Development: Embodied, Embedded, Enculturated, and Enabling. Annu. Rev. Psychol. 2019, 70, 141–164. [Google Scholar] [CrossRef]
- Yu, J.J.; Burnett, A.F.; Sit, C.H. Motor Skill Interventions in Children with Developmental Coordination Disorder: A Systematic Review and Meta-Analysis. Arch. Phys. Med. Rehabil. 2018, 99, 2076–2099. [Google Scholar] [CrossRef]
- Kleim, J.A.; Jones, T.A. Principles of experience-dependent neural plasticity: Implications for rehabilitation after brain damage. J. Speech Lang. Hear. Res. 2008, 51, 225–239. [Google Scholar] [CrossRef]
- Smits-Engelsman, B.; Vincon, S.; Blank, R.; Quadrado, V.H.; Polatajko, H.; Wilson, P.H. Evaluating the evidence for motor-based interventions in developmental coordination disorder: A systematic review and meta-analysis. Res. Dev. Disabil. 2018, 74, 72–102. [Google Scholar] [CrossRef] [PubMed]
- Okely, A.D.; Booth, M.; Patterson, J.W. Relationship of Physical Activity to Fundamental Movement Skills among Adolescents. Med. Sci. Sports Exerc. 2001, 33, 1899–1904. [Google Scholar] [CrossRef] [PubMed]
- Wrotniak, B.H.; Epstein, L.H.; Dorn, J.M.; Jones, K.E.; Kondilis, V.A. The relationship between motor proficiency and physical activity in children. Pediatrics 2006, 118, e1758–e1765. [Google Scholar] [CrossRef]
- Palma, M.S.; Pereira, B.O.; Valentini, N.C. Guided play and free play in an enriched environment: Impact on motor development. Motriz 2014, 20, 177–185. [Google Scholar] [CrossRef] [Green Version]
- Robinson, L.E.; Palmer, K.K.; Bub, K.L. Effect of the children’s health activity Motor Program on Motor skills and self-regulation in head start Preschoolers: An efficacy Trial. Front. Public Health 2016, 4, 173. [Google Scholar] [CrossRef] [Green Version]
- Robinson, L.E.; Veldman, S.L.; Palmer, K.K.; Okely, A.D. A Ball Skills Intervention in Preschoolers: The CHAMP Randomized Controlled Trial. Med. Sci. Sports Exerc. 2017, 49, 2234–2239. [Google Scholar] [CrossRef]
- Tortella, P.; Haga, M.; Lorås, H.; Sigmundsson, H.; Fumagalli, G. Motor skill development in Italian pre-school children induced by structured activities in a specific playground. PLoS ONE 2016, 11, e0160244. [Google Scholar] [CrossRef]
- Veldman, S.L.; Jones, R.A.; Okely, A.D. Efficacy of gross motor skill interventions in young children: An updated systematic review. BMJ Open Sport Exerc. Med. 2016, 2, e000067. [Google Scholar] [CrossRef]
- Johnstone, A.; Hughes, A.R.; Martin, A.; Reilly, J.J. Utilising active play interventions to promote physical activity and improve fundamental movement skills in children: A systematic review and meta-analysis. BMC Public Health 2018, 18, 789. [Google Scholar] [CrossRef]
- Palmer, K.K.; Matsuyama, A.L.; Robinson, L.E. Impact of structured movement time on preschoolers’ physical activity engagement. Early Child. Educ. J. 2017, 45, 201–206. [Google Scholar] [CrossRef]
- Pate, R.R.; Brown, W.F.; Pfeiffer, K.A.; Howie, E.K.; Saunders, R.P.; Addy, C.L.; Dowda, M. An intervention to increase physical activity in children: A randomized controlled trial with 4-year-old in preschools. Am. J. Prev. Med. 2016, 51, 12–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tortella, P.; Haga, M.; Ingebrigtsen, J.E.; Sigmundsson, H.; Fumagalli, G.F. Comparing free play and partly structured play in 4-5-years-old children in an outdoor playground. Front. Public Health 2019, 7, 197. [Google Scholar] [CrossRef] [Green Version]
- True, L.; Pfeiffer, K.A.; Dowda, M.; Williams, H.G.; Brown, W.H.; O’Neill, J.R.; Pate, R.R. Motor competence and characteristics within the preschool environment. J. Sci. Med. Sport 2017, 20, 751–755. [Google Scholar] [CrossRef]
- Niemistö, D.; Finni, T.; Haapala, E.A.; Cantell, M.; Korhonen, E.; Sääkslahti, A. Environmental Correlates of Motor Competence in Children—The Skilled Kids Study. Int. J. Environ. Res. Public Health 2019, 16, 1989. [Google Scholar] [CrossRef] [Green Version]
- Sugiyama, T.; Okely, A.D.; Masters, J.M.; Moore, G. Attributes of childcare centers and outdoor play areas associated with preschoolers’ physical activity and sedentary behavior. Environ. Behav. 2012, 44, 334–349. [Google Scholar] [CrossRef]
- Adams, J.; Veitch, J.; Barnett, L. Physical Activity and Fundamental Motor Skill Performance of 5–10-Year-Old Children in Three Different Playgrounds. Int. J. Environ. Res. Public Health 2018, 15, 1896. [Google Scholar] [CrossRef] [Green Version]
- Buzzavo, G.; Dalt, L.D.; Durigon, V.; Fumagalli, G.; Maffeis, C.; Moghetti, P.; Romano, M.; Tortella, P. Surroundings and Activities just Right for Growing Up Well Milano: Edizioni Libreria dello Sport. 2011. Available online: https://www.0246.it/wp-content/uploads/2018/06/book-eng-low.pdf (accessed on 15 January 2020).
- Sigmundsson, H.; Lorås, H.; Haga, M. Assessment of motor competence across the life span: Aspects of reliability and validity of a new test battery. SAGE Open 2016, 6, 2158244016633273. [Google Scholar] [CrossRef] [Green Version]
- Yoon, D.Y.; Scott, K.; Hill, M.N.; Levitt, N.S.; Lambert, E.V. Review of three tests of motor proficiency in children. Percept. Mot. Ski. 2006, 102, 543–551. [Google Scholar] [CrossRef]
- Rinne, M.B.; Pasanen, M.E.; Miilunpalo, S.I.; Oja, P. Test-retest reproducibility and inter-rater reliability of a motor skill test battery for adults. Int. J. Sports Med. 2001, 22, 192–200. [Google Scholar] [CrossRef]
- Rooks, D.S.; Kiel, D.P.; Parsons, C.; Hayes, W.C. Self-paced resistance training and walking exercise in community-dwelling older adults: Effects on neuromotor performance. J. Gerontol. Ser. A Psychol. Sci. Soc. Sci. 1997, 52, M161–M168. [Google Scholar] [CrossRef] [PubMed]
- Johansson, G.; Jarnlo, G.-B. Balance training in 70-year-old women. Physiother. Theory Pract. 1991, 7, 121–125. [Google Scholar] [CrossRef]
- Henderson, S.E.; Sugden, D.A. The Movement Assessment Battery for Children; The Psychological Corp: Kent, UK, 1992. [Google Scholar]
- Tan, S.K.; Parker, H.E.; Larkin, D. Concurrent validity of motor tests used to identify children with motor impairment. Adapt. Phys. Act. Quart. 2001, 18, 168–182. [Google Scholar] [CrossRef]
- Bruininks, R.H. Bruininks-Oseretsky Test of Motor Proficiency: Examiners Manual Circle Pines; American Guidance Service: Circle Pines, MN, USA, 1978. [Google Scholar]
- Crawford, S.G.; Wilson, B.N.; Dewey, D. Identifying developmental coordination disorder: Consistency between tests. Phys. Occup. Ther. Pediatr. 2001, 20, 29–50. [Google Scholar] [CrossRef] [PubMed]
- Slater, L.M.; Hillier, S.L.; Civetta, L.R. The clinimetric properties of performance-based gross motor tests used for children with developmental coordination disorder: A systematic review. Pediatr. Phys. Ther. 2010, 22, 170–179. [Google Scholar] [CrossRef]
- Van Waevelde, H.; Peersman, W.; Lenoir, M.; Smits Engelsman, B.C.M. Convergent validity between two motor tests: Movement ABC and PDMS-2. Adapt. Phys. Act. Quart. 2007, 24, 59–69. [Google Scholar] [CrossRef]
- Kiphard, E.J.; Schilling, F. Körperkoordinationstest für Kinder 2, überarbeitete und ergänzte Aufgabe. Beltz test, Weinham. Med. Sci. Sports 2007, 21, 378–388. [Google Scholar] [CrossRef]
- Blank, R.; Barnett, A.L.; Cairney, J.; Green, D.; Kirby, A.; Polatajko, H.; Rosenblum, S.; Smits-Engelsman, B.; Sugden, D.; Wilson, P.; et al. International clinical practice recommendations on the definition, diagnosis, assessment, intervention, and psychosocial aspects of developmental coordination disorder. Dev. Med. Child Neurol. 2019, 61, 242–285. [Google Scholar] [CrossRef]
- Vygotsky, L.S. Thought and Language; MIT Press: Cambridge, MA, USA, 1962. [Google Scholar]
- Tortella, P.; Fumagalli, G. Activities in the zone of proximal development between the development of motor skills and school readiness: Studies in kindergartens. Eur. J. Res. Educ. Teach. 2015, 13, 355–368. [Google Scholar]
- Gallahue, D.L.; Ozmun, J.C.; Goodway, J. Understanding Motor Development. Infants, Children, Adolescents, Adults, 7th ed.; McGraw-Hill: New York, NY, USA, 2012. [Google Scholar]
- Sigmundsson, H.; Newell, K.M.; Polman, R.; Haga, M. Exploration of the Specificity of Motor Skills Hypothesis in 7–8-Year-Old Primary School Children: Exploring the Relationship Between 12 Different Motor Skills from Two Different Motor Competence Test Batteries. Front. Psychol. 2021, 12, 2384. [Google Scholar] [CrossRef]
- Hadders-Algra, M. Variation and Variability: Key Words in Human Motor Development. Phys. Ther. 2010, 90, 1823–1837. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sigmundsson, H.; Trana, L.; Polman, R.; Haga, M. What is trained develops! theoretical perspective on skill learning. Sports 2017, 5, 38. [Google Scholar] [CrossRef] [PubMed]
- Zeng, N.; Ayyub, M.; Sun, H.; Wen, X.; Xiang, P.; Gao, Z. Effects of physical activity on motor skills and cogni-tive development in early childhood: A systematic review. BioMed Res. Int. 2017, 2017, 2760716. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Education and Research. Framework Plan for the Content and Tasks of Kindergartens. 2017. Available online: https://www.udir.no/rammeplan (accessed on 3 June 2022).
- Truelove, S.; Bruijns, B.A.; Vanderloo, L.M.; O’Brien, K.T.; Johnson, A.M.; Tucker, P. Physical activity and sedentary time during childcare outdoor play sessions: A systematic review and meta-analysis. Prev. Med. 2018, 108, 74–85. [Google Scholar] [CrossRef] [PubMed]
- Sando, O.J. The outdoor environment and children’s health: A multilevel approach. Int. J. Play. 2019, 8, 39–52. [Google Scholar] [CrossRef]
- Haga, M. Body and movement in early childhood: Spaces for movement-based play. J. Phys. Educ. Sport 2021, 21, 526–529. [Google Scholar]
- Sääkslahti, A.; Niemistö, D. Outdoor activities and motor development in 2–7-year-old boys and girls. J. Phys. Educ. Sport 2021, 21, 463–468. [Google Scholar] [CrossRef]
- Cairney, J.; Dudley, D.; Kwan, M.; Bulten, R.; Kriellaars, D. Physical literacy, physical activity and health: Toward an evidence-informed conceptual model. Sports Med. 2019, 49, 371–383. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study Group | ||||||
|---|---|---|---|---|---|---|
| Control | Structured Activity | Free Play | ||||
| Variable | Pretest | Posttest | Pretest | Posttest | Pretest | Posttest |
| Placing bricks (s) | 83.54 (12.17) | 92.91 (12.93) | 93.94 (18.86) | 98.93 (21.77) | 88.51 (15.15) | 87.84 (17.65) |
| Building bricks (s) | 23.32 (5.27) | 28.70 (9.54) | 25.42 (7.94) | 29.31 (9.28) | 24.07 (5.77) | 27 (6.72) |
| Heel-to-Toe walking (s) | 34.61 (12.67) | 38.27 (9.55) | 39.45 (15.94) | 38.85 (9.18) | 41.09 (11.77) | 40.93 (11.64) |
| Walking/running in slopes (s) | 8.59 (2.08) | 9.07 (2.51) | 11.41 (3.64) | 9.08 (2.73) | 12.47 (3.71) | 8.33 (1.71) |
| Sumscore (s) | 125.11 (46.51) | 154.33 (36.11) | 149.66 (44.94) | 152.72 (44.68) | 149.88 (40.42) | 153.01 (27.32) |
| Study Group | ||||||
|---|---|---|---|---|---|---|
| Control | Structured Activity | Free Play | ||||
| Variable | Pretest | Posttest | Pretest | Posttest | Pretest | Posttest |
| Posting Coins (s) | 50.30 (7.34) | 46.81 (5.73) | 54.06 (9.47) | 48.35 (10.70) | 51.70 (11.45) | 46.34 (7.16) |
| Threading beads (s) | 70.15 (15.27) | 66.07 (14.51) | 80.98 (28.29) | 72.37 (31.86) | 74.56 (27.00) | 68.58 (26.45) |
| Drawing Trail errors (n) | 1.45 (1.30) | 1.97 (1.59) | 2.02 (2.82) | 2.27 (2.71) | 1.92 (1.92) | 1.82 (2.22) |
| Catching beanbags (n) | 5.54 (2.73) | 8.06 (1.53) | 5.86 (2.77) | 7.66 (2.15) | 5.78 (3.16) | 7.49 (1.98) |
| Throwing beanbags (n) | 4.00 (4.58) | 4.57 (1.84) | 2.68 (2.02) | 4.02 (2.18) | 2.90 (1.77) | 2.81 (1.93) |
| One leg balance (s) | 23.85 (14.94) | 30.27 (15.50) | 27.00 (22.88) | 17.54 (8.77) | 29.13 (19.34) | 18.11 (16.68) |
| Walking heels raised (n) | 10.72 (5.77) | 11.83 (4.21) | 8.54 (6.00) | 6.79 (5.57) | 9.10 (5.92) | 8.71 (5.80) |
| Jumping on mats (n) | 2.59 (1.81) | 2.00 (1.72) | 1.52 (1.57) | 1.93 (1.82) | 1.56 (1.53) | 2.15 (1.95) |
| Sumscore | 45.42 (14.67) | 55.95 (7.35) | 45.24 (15.21) | 46.73 (15.07) | 47.81 (15.49) | 49.73 (14.26) |
| Study Group | ||||||
|---|---|---|---|---|---|---|
| Control | Structured Activity | Free Play | ||||
| Variable | Pretest | Posttest | Pretest | Posttest | Pretest | Posttest |
| Elastic (s) | 27.26 (12.70) | 20.28 (11.72) | 21.79 (11.11) | 12.41 (5.93) | 28.64 (17.92) | 14.42 (11.00) |
| Elastic (n errors) | 1.16 (1.65) | 1.55 (2.06) | 0.98 (1.75) | 0.11 (0.49) | 1.79 (2.14) | 0.55 (1.39) |
| Beams (s) | 22.79 (14.14) | 14.18 (7.84) | 24.97 (18.86) | 13.03 (11.20) | 23.30 (15.79) | 10.44 (5.28) |
| Beams (n errors) | 3.91 (3.58) | 2.17 (2.14) | 3.25 (3.06) | 1.84 (2.92) | 4.45 (3.87) | 1.47 (1.75) |
| Sumscore | 46.48 (14.23) | 48.21 (10.05) | 47.40 (13.05) | 53.90 (1.93) | 44.39 (13.68) | 47.39 (12.02) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tortella, P.; Haga, M.; Lorås, H.; Fumagalli, G.F.; Sigmundsson, H. Effects of Free Play and Partly Structured Playground Activity on Motor Competence in Preschool Children: A Pragmatic Comparison Trial. Int. J. Environ. Res. Public Health 2022, 19, 7652. https://doi.org/10.3390/ijerph19137652
Tortella P, Haga M, Lorås H, Fumagalli GF, Sigmundsson H. Effects of Free Play and Partly Structured Playground Activity on Motor Competence in Preschool Children: A Pragmatic Comparison Trial. International Journal of Environmental Research and Public Health. 2022; 19(13):7652. https://doi.org/10.3390/ijerph19137652
Chicago/Turabian StyleTortella, Patrizia, Monika Haga, Håvard Lorås, Guido Francesco Fumagalli, and Hermundur Sigmundsson. 2022. "Effects of Free Play and Partly Structured Playground Activity on Motor Competence in Preschool Children: A Pragmatic Comparison Trial" International Journal of Environmental Research and Public Health 19, no. 13: 7652. https://doi.org/10.3390/ijerph19137652