
A Review of the Respiratory Health Burden Attributable to Short-Term Exposure to Pollen

 , and
, and 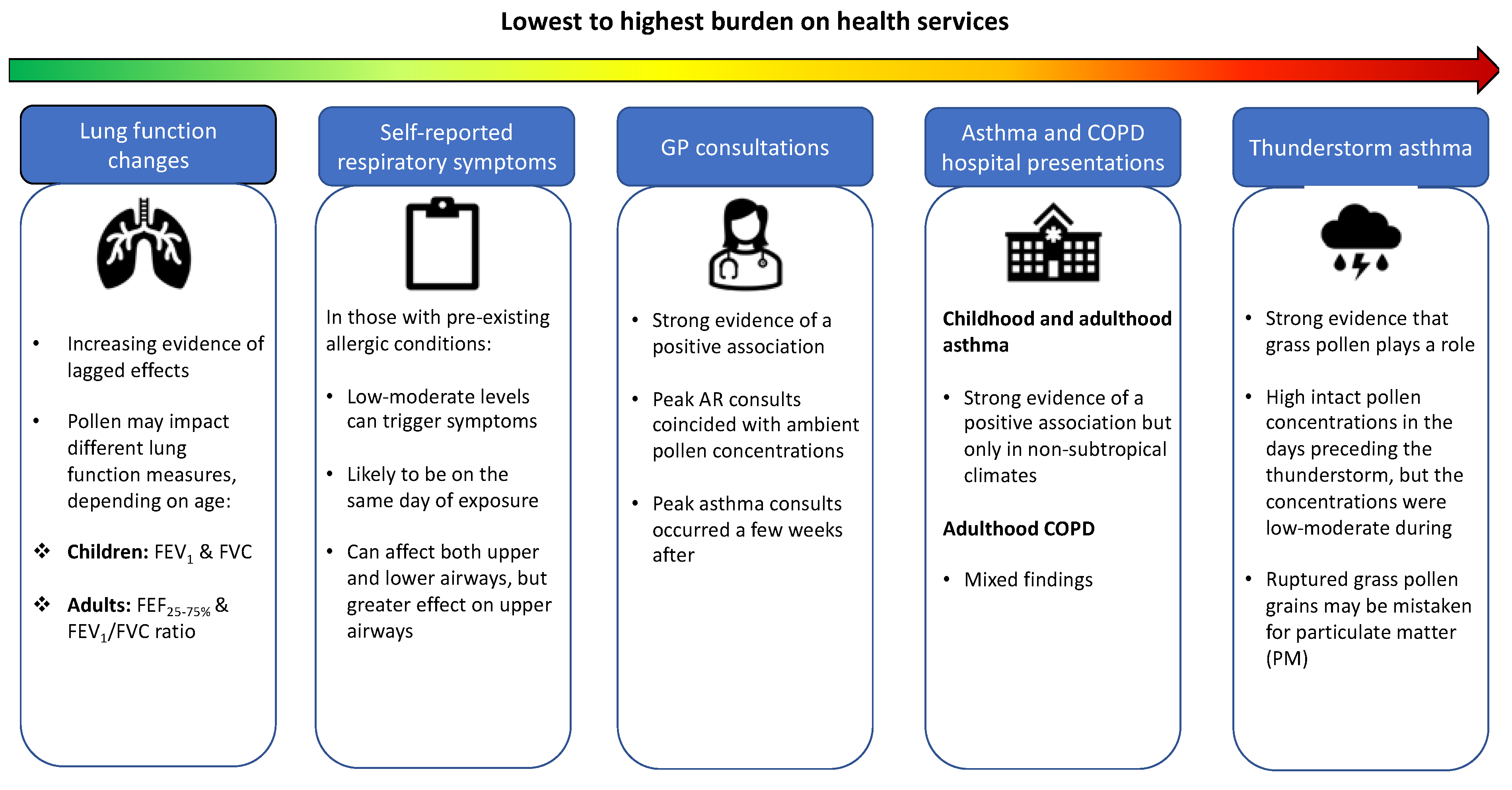{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. Outdoor Pollen Is a Risk Factor for Respiratory Diseases
1.2. What Do We Know about Pollen?
1.3. Proposed Immunological Mechanisms Triggered by Pollen Exposure
2. Aims of This Review and Search Strategy
3. Short-Term Impact of Pollen on Adverse Respiratory Outcomes
3.1. Thunderstorm Asthma (TA)
3.2. Asthma and COPD Hospital Presentations
3.2.1. Childhood Asthma
3.2.2. Adulthood Asthma
3.2.3. Adulthood COPD
3.3. General Practice (GP) Consultations
3.4. Self-Reported Respiratory Symptoms
3.5. Lung Function Changes
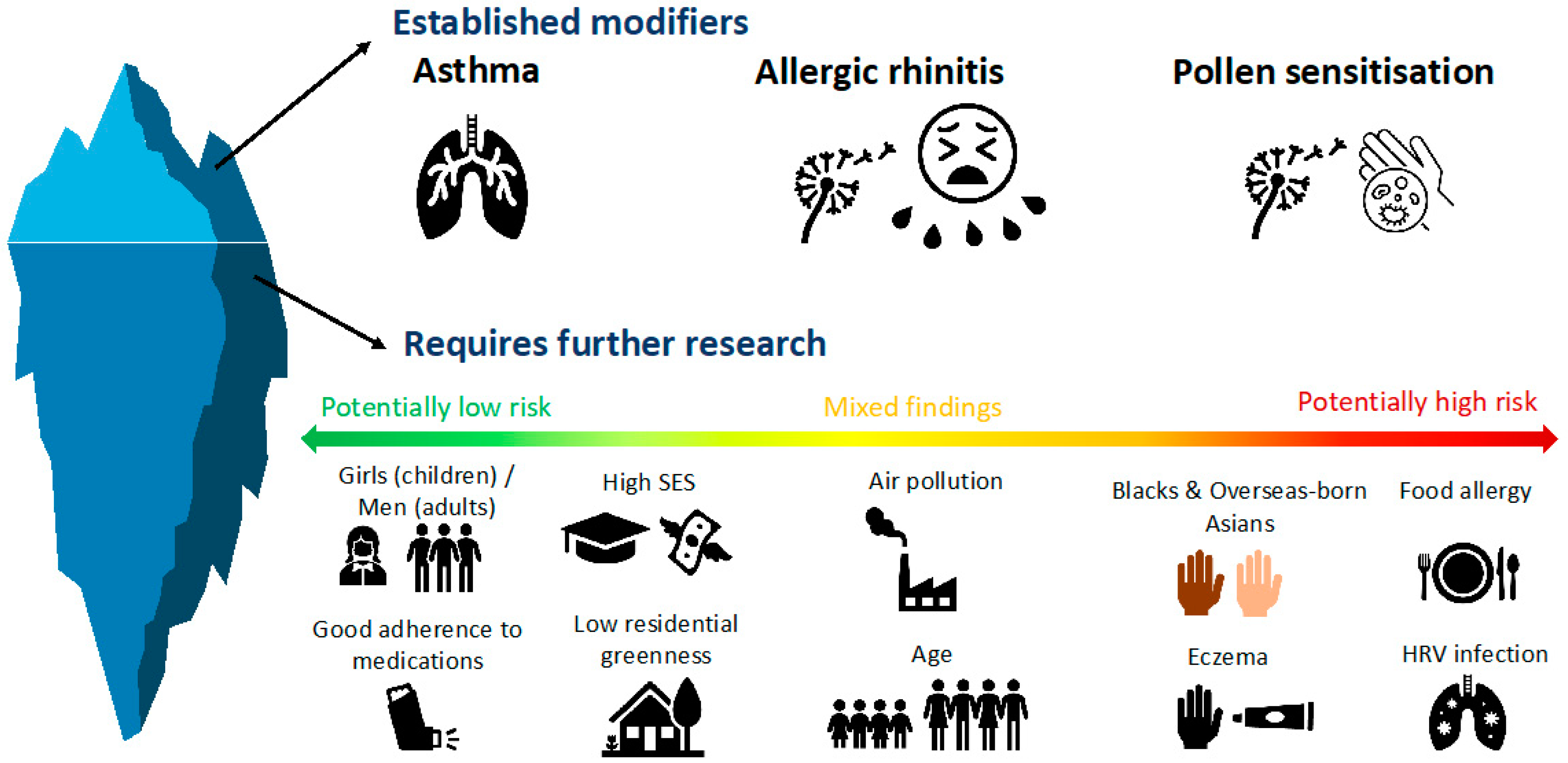
4. Evidence on Potential Effect Modifiers of the above Associations
4.1. Air Pollution
4.2. Residential Greenness
4.3. Asthma, Allergic Rhinitis (AR) and Pollen Sensitisation
4.4. Adherence to Preventer Medications
4.5. Human Rhinovirus Infection (HRV)
4.6. Food Allergy
4.7. Eczema
4.8. Socio-Economic Status (SES)
4.9. Age
4.10. Sex
4.11. Ethnicity
5. Conclusions and Knowledge Gaps
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Taylor, P.E.; Flagan, R.C.; Valenta, R.; Glovsky, M.M. Release of allergens as respirable aerosols: A link between grass pollen and asthma. J. Allergy Clin. Immunol. 2002, 109, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Dales, R.E.; Cakmak, S.; Judek, S.; Coates, F. Tree pollen and hospitalization for asthma in urban Canada. Int. Arch. Allergy Immunol. 2008, 146, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.-Y.; Ma, T.; Zhuang, Y.; Ning, H.-Y.; Shi, H.-Y.; Yu, R.-L.; Yan, D.; Huang, H.-D.; Bai, Y.-F.; Shan, G.-L.; et al. Prevalence of pollen-induced allergic rhinitis with high pollen exposure in grasslands of northern China. Allergy 2018, 73, 1232–1243. [Google Scholar] [CrossRef] [PubMed]
- Cockcroft, D.W.; Ruffin, R.E.; Dolovich, J.; Hargreave, F.E. Allergen-induced increase in non-allergic bronchial reactivity. Clin. Exp. Allergy 1977, 7, 503–513. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.F.; Novey, H.S.; Berke, R.A.; Surprenant, E.L. Deposition of inhaled pollen and pollen extract in human airways. N. Engl. J. Med. 1973, 288, 1056–1058. [Google Scholar] [CrossRef] [PubMed]
- Skjøth, C.A.; Sommer, J.; Stach, A.; Smith, M.; Brandt, J. The long-range transport of birch (Betula) pollen from Poland and Germany causes significant pre-season concentrations in Denmark. Clin. Exp. Allergy 2007, 37, 1204–1212. [Google Scholar] [CrossRef] [Green Version]
- Cecchi, L.; Morabito, M.; Paola Domeneghetti, M.; Crisci, A.; Onorari, M.; Orlandini, S. Long distance transport of ragweed, pollen as a potential cause of allergy in central Italy. Ann. Allergy Asthma Immunol. 2006, 96, 86–91. [Google Scholar]
- Erbas, B.; Jazayeri, M.; Lambert, K.A.; Katelaris, C.H.; Prendergast, L.A.; Tham, R.; Parrodi, M.J.; Davies, J.; Newbigin, E.; Abramson, M.J.; et al. Outdoor pollen is a trigger of child and adolescent asthma emergency department presentations: A systematic review and meta-analysis. Allergy 2018, 73, 1632–1641. [Google Scholar] [CrossRef]
- Lo, F.; Bitz, C.M.; Battisti, D.S.; Hess, J.J. Pollen calendars and maps of allergenic pollen in North America. Aerobiologia 2019, 35, 613–633. [Google Scholar] [CrossRef] [Green Version]
- Spieksma, F.; Corden, J.; Detandt, M.; Millington, W.; Nikkels, H.; Nolard, N.; Schoenmakers, C.; Wachter, R.; De Weger, L.; Willems, R.; et al. Quantitative trends in annual totals of five common airborne pollen types (Betula, Quercus, Poaceae, Urtica, and Artemisia), at five pollen-monitoring stations in western Europe. Aerobiologia 2003, 19, 171–184. [Google Scholar] [CrossRef]
- D’Amato, G.; Lobefalo, G. Allergenic pollens in the southern Mediterranean area. J. Allergy Clin. Immunol. 1989, 83, 116–122. [Google Scholar] [CrossRef]
- Beggs, P.J.; Katelaris, C.H.; Medek, D.; Johnston, F.H.; Burton, P.K.; Campbell, B.; Jaggard, A.K.; Vicendese, D.; Bowman, D.M.; Godwin, I.; et al. Differences in grass pollen allergen exposure across Australia. Aust. N. Z. J. Public Health 2015, 39, 51–55. [Google Scholar] [CrossRef]
- Simunovic, M.; Dwarakanath, D.; Addison-Smith, B.; Susanto, N.H.; Erbas, B.; Baker, P.; Davies, J.M. Grass pollen as a trigger of emergency department presentations and hospital admissions for respiratory conditions in the subtropics: A systematic review. Environ. Res. 2020, 182, 109125. [Google Scholar] [CrossRef] [PubMed]
- Ong, E.K.; Singh, M.B.; Knox, R.B. Grass pollen in the atmosphere of Melbourne: Seasonal distribution over nine years. Grana 1995, 34, 58–63. [Google Scholar] [CrossRef]
- Frei, T.; Gassner, E. Trends in prevalence of allergic rhinitis and correlation with pollen counts in Switzerland. Int. J. Biometeorol. 2008, 52, 841–847. [Google Scholar] [CrossRef]
- Singer, B.D.; Ziska, L.H.; Frenz, D.A.; Gebhard, D.E.; Straka, J.G. Increasing Amb a 1 content in common ragweed (Ambrosia artemisiifolia) pollen as a function of rising atmospheric CO2 concentration. Funct. Plant Biol. 2005, 32, 667–670. [Google Scholar] [CrossRef] [PubMed]
- Ariano, R.; Canonica, G.W.; Passalacqua, G. Possible role of climate changes in variations in pollen seasons and allergic sensitizations during 27 years. Ann. Allergy Asthma Immunol. 2010, 104, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Hamaoui-Laguel, L.; Vautard, R.; Liu, L.; Solmon, F.; Viovy, N.; Khvorostyanov, D.; Chuine, I.; Colette, A.; Semenov, M.A.; Schaffhauser, A.; et al. Effects of climate change and seed dispersal on airborne ragweed pollen loads in Europe. Nat. Clim. Chang. 2015, 5, 766–771. [Google Scholar] [CrossRef]
- Kurganskiy, A.; Creer, S.; de Vere, N.; Griffith Gareth, W.; Osborne Nicholas, J.; Wheeler Benedict, W.; McInnes, R.N.; Clewlow, Y.; Barber, A.; Brennan, G.L.; et al. Predicting the severity of the grass pollen season and the effect of climate change in Northwest Europe. Sci. Adv. 2021, 7, eabd7658. [Google Scholar] [CrossRef]
- Ito, K.; Weinberger, K.R.; Robinson, G.S.; Sheffield, P.E.; Lall, R.; Mathes, R.; Ross, Z.; Kinney, P.L.; Matte, T.D. The associations between daily spring pollen counts, over-the-counter allergy medication sales, and asthma syndrome emergency department visits in New York City, 2002–2012. Environ. Health. 2015, 14, 71. [Google Scholar] [CrossRef] [Green Version]
- Lake, I.R.; Jones, N.R.; Agnew, M.; Goodess, C.M.; Giorgi, F.; Hamaoui-Laguel, L.; Semenov, M.A.; Solomon, F.; Storkey, J.; Vautard, R.; et al. Climate Change and Future Pollen Allergy in Europe. Environ. Health Perspect. 2017, 125, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Serrano, C.D.; Valero, A.; Bartra, J.; Roca-Ferrer, J.; Muñoz-Cano, R.; Sánchez-López, J.; Mullol, J.; Picado, C. Nasal and bronchial inflammation after nasal allergen challenge: Assessment using noninvasive methods. J. Investig. Allergol. Clin. Immunol. 2012, 22, 351–356. [Google Scholar] [PubMed]
- Scadding, G.W.; Calderon, M.A.; Bellido, V.; Koed, G.K.; Nielsen, N.-C.; Lund, K.; Togias, A.; Phippard, D.; Turka, L.A.; Hansel, T.T.; et al. Optimisation of grass pollen nasal allergen challenge for assessment of clinical and immunological outcomes. J. Immunol. Methods 2012, 384, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Idrose, N.S.; Walters, E.H.; Zhang, J.; Vicendese, D.; Newbigin, E.J.; Douglass, J.A.; Erbas, B.; Lowe, A.J.; Perret, J.L.; Lodge, C.J.; et al. Outdoor pollen-related changes in lung function and markers of airway inflammation: A systematic review and meta-analysis. Clin. Exp. Allergy 2021, 51, 636–653. [Google Scholar] [CrossRef]
- Andersson, M.; Svensson, C.; Andersson, P.; Pipkorn, U. Objective monitoring of the allergic inflammatory response of the nasal mucosa in patients with hay fever during natural allergen exposure. Am. Rev. Respir. Dis. 1989, 139, 911–914. [Google Scholar] [CrossRef] [PubMed]
- Connell, J.T. Quantitative intranasal pollen challenge. II. Effect of daily pollen challenge, environmental pollen exposure, and placebo challenge on the nasal membrane. J. Allergy 1968, 41, 123–139. [Google Scholar] [CrossRef]
- Choi, C.H.; Poroyko, V.; Watanabe, S.; Jiang, D.; Lane, J.; Detineo, M.; Baroody, F.M.; Naclerio, R.M.; Pinto, J.M. Seasonal allergic rhinitis affects sinonasal microbiota. Am. J. Rhinol. Allergy 2014, 28, 281–286. [Google Scholar] [CrossRef] [Green Version]
- Lowe, A.J.; Lodge, C.J.; Allen, K.; Abramson, M.J.; Matheson, M.C.; Thomas, P.S.; Barton, C.; Bennett, C.; Erbas, B.; Svanes, C.; et al. Cohort Profile: Melbourne Atopy Cohort study (MACS). Int. J. Epidemiol. 2017, 46, 25–26. [Google Scholar] [CrossRef] [Green Version]
- Idrose, N.S.; Tham, R.C.A.; Lodge, C.J.; Lowe, A.J.; Bui, D.; Perret, J.L.; Vicendese, D.; Newbigin, E.J.; Tang, M.L.K.; Aldakheel, F.M.; et al. Is short-term exposure to grass pollen adversely associated with lung function and airway inflammation in the community? Allergy 2021, 76, 1136–1146. [Google Scholar] [CrossRef]
- Lambert, K.A.; Markevych, I.; Yang, B.Y.; Bauer, C.P.; Berdel, D.; von Berg, A.; Bergmann, K.C.; Lodge, C.; Koletzko, S.; Prendergast, L.A.; et al. Association of early life and acute pollen exposure with lung function and exhaled nitric oxide (FeNO). A prospective study up to adolescence in the GINIplus and LISA cohort. Sci. Total Environ. 2021, 763, 143006. [Google Scholar] [CrossRef]
- Justiz Vaillant, A.A.; Sabir, S.; Jan, A. Physiology, Immune Response; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2022. [Google Scholar]
- Buters, J.; Prank, M.; Sofiev, M.; Pusch, G.; Albertini, R.; Annesi-Maesano, I.; Antunes, C.; Behrendt, H.; Berger, U.; Brandao, R.; et al. Variation of the group 5 grass pollen allergen content of airborne pollen in relation to geographic location and time in season. J. Allergy Clin. Immunol. 2015, 136, 87–95.e6. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, S.K.; Lambert, K.A.; Erbas, B. Ambient pollen concentrations and asthma hospitalization in children and adolescents: A systematic review and meta-analysis. J. Asthma 2021, 58, 1155–1168. [Google Scholar] [CrossRef] [PubMed]
- Idrose, N.S.; Dharmage, S.C.; Lowe, A.J.; Lambert, K.A.; Lodge, C.J.; Abramson, M.J.; Douglass, J.A.; Newbigin, E.J.; Erbas, B. A systematic review of the role of grass pollen and fungi in thunderstorm asthma. Environ. Res. 2020, 181, 108911. [Google Scholar] [CrossRef] [PubMed]
- Elliot, A.J.; Bennett, C.D.; Hughes, H.E.; Morbey, R.A.; Todkill, D.; Thompson, R.; Landeg, O.; OConnell, E.; Seltzer, M.; Lang, W.; et al. Spike in Asthma Healthcare Presentations in Eastern England during June 2021: A Retrospective Observational Study Using Syndromic Surveillance Data. Int. J. Environ. Res. Public Health. 2021, 18, 12353. [Google Scholar] [CrossRef] [PubMed]
- Bannister, T.; Csutoros, D.; Arnold, A.L.; Black, J.; Feren, G.; Russell, R.; Watson, A.; Williams, S.; Silver, J.D.; Hughes, N. Are convergence lines associated with high asthma presentation days? A case-control study in Melbourne, Australia. Sci. Total Environ. 2020, 737, 140263. [Google Scholar] [CrossRef]
- Cockcroft, D.W.; Davis, B.E.; Blais, C.M. Thunderstorm asthma: An allergen-induced early asthmatic response. Ann. Allergy Asthma Immunol. 2018, 120, 120–123. [Google Scholar] [CrossRef] [Green Version]
- Wark, P.A.; Simpson, J.; Hensley, M.J.; Gibson, P.G. Airway inflammation in thunderstorm asthma. Clin. Exp. Allergy 2002, 32, 1750–1756. [Google Scholar] [CrossRef]
- Campbell, S.L.; Fox-Hughes, P.D.; Jones, P.J.; Remenyi, T.A.; Chappell, K.; White, C.J.; Johnston, F.H. Evaluating the Risk of Epidemic Thunderstorm Asthma: Lessons from Australia. Int. J. Environ. Res. Public Health 2019, 16, 837. [Google Scholar] [CrossRef] [Green Version]
- AlQuran, A.; Batra, M.; Harry Susanto, N.; Holland, A.E.; Davies, J.M.; Erbas, B.; Lampugnani, E.R. Community Response to the Impact of Thunderstorm Asthma Using Smart Technology. Allergy Rhinol. 2021, 12, 21526567211010728. [Google Scholar] [CrossRef]
- Clayton-Chubb, D.; Con, D.; Rangamuwa, K.; Taylor, D.; Thien, F.; Wadhwa, V. Thunderstorm asthma: Revealing a hidden at-risk population. Intern. Med. J. 2019, 49, 74–78. [Google Scholar] [CrossRef] [Green Version]
- Silver, J.D.; Sutherland, M.F.; Johnston, F.H.; Lampugnani, E.R.; McCarthy, M.A.; Jacobs, S.J.; Pezza, A.B.; Newbigin, E.J. Seasonal asthma in Melbourne, Australia, and some observations on the occurrence of thunderstorm asthma and its predictability. PLoS ONE 2018, 13, e0194929. [Google Scholar] [CrossRef] [PubMed]
- Chatelier, J.; Chan, S.; Tan, J.A.; Stewart, A.G.; Douglass, J.A. Managing Exacerbations in Thunderstorm Asthma: Current Insights. J. Inflamm. Res. 2021, 14, 4537–4550. [Google Scholar] [CrossRef] [PubMed]
- Suphioglu, C.; Singh, M.B.; Taylor, P.; Knox, R.B.; Bellomo, R.; Holmes, P.; Puy, R. Mechanism of grass-pollen-induced asthma. Lancet 1992, 339, 569–572. [Google Scholar] [CrossRef]
- Emmerson, K.M.; Silver, J.D.; Thatcher, M.; Wain, A.; Jones, P.J.; Dowdy, A.; Newbigin, E.J.; Picking, B.W.; Choi, J.; Ebert, E.; et al. Atmospheric modelling of grass pollen rupturing mechanisms for thunderstorm asthma prediction. PLoS ONE 2021, 16, e0249488. [Google Scholar] [CrossRef]
- Thien, F.; Beggs, P.J.; Csutoros, D.; Darvall, J.; Hew, M.; Davies, J.M.; Bardin, P.G.; Bannister, T.; Barnes, S.; Bellomo, R.; et al. The Melbourne epidemic thunderstorm asthma event 2016: An investigation of environmental triggers, effect on health services, and patient risk factors. Lancet Planet Health 2018, 2, e255–e263. [Google Scholar] [CrossRef]
- Andrew, E.; Nehme, Z.; Bernard, S.; Abramson, M.J.; Newbigin, E.; Piper, B.; Dunlop, J.; Holman, P.; Smith, K. Stormy weather: A retrospective analysis of demand for emergency medical services during epidemic thunderstorm asthma. BMJ 2017, 359, j5636. [Google Scholar] [CrossRef] [Green Version]
- Davidson, A.C.; Emberlin, J.; Cook, A.D.; Venables, K.M. A major outbreak of asthma associated with a thunderstorm: Experience of accident and emergency departments and patients’ characteristics. Thames Regions Accident and Emergency Trainees Association. BMJ 1996, 312, 601–604. [Google Scholar]
- Dales, R.E.; Cakmak, S.; Judek, S.; Dann, T.; Coates, F.; Brook, J.R.; Burnett, R.T. The role of fungal spores in thunderstorm asthma. Chest 2003, 123, 745–750. [Google Scholar] [CrossRef] [Green Version]
- Darvall, J.N.; Durie, M.; Pilcher, D.; Wigmore, G.; French, C.; Karalapillai, D.; McGain, F.; Newbigin, E.; Byrne, T.; Sarode, V.; et al. Intensive care implications of epidemic thunderstorm asthma. Crit. Care Resusc. 2018, 20, 294–303. [Google Scholar]
- Tobías, A.; Galán, I.; Banegas, J.R. Non-linear short-term effects of airborne pollen levels with allergenic capacity on asthma emergency room admissions in Madrid, Spain. Clin. Exp. Allergy 2004, 34, 871–878. [Google Scholar] [CrossRef]
- Jochner, S.; Lüpke, M.; Laube, J.; Weichenmeier, I.; Pusch, G.; Traidl-Hoffmann, C.; Schmidt-Weber, C.B.; Buters, J.; Menzel, A. Seasonal variation of birch and grass pollen loads and allergen release at two sites in the German Alps. Atmos. Environ. 2015, 122, 83–93. [Google Scholar] [CrossRef]
- Erbas, B.; Dharmage, S.C.; Tang, M.L.; Akram, M.; Allen, K.J.; Vicendese, D.; Davies, J.M.; Hyndman, R.J.; Newbigin, E.J.; Taylor, P.E.; et al. Do human rhinovirus infections and food allergy modify grass pollen-induced asthma hospital admissions in children? J. Allergy Clin. Immunol. 2015, 136, 1118–1120.e2. [Google Scholar] [CrossRef] [PubMed]
- Batra, M.; Vicendese, D.; Newbigin, E.; Lambert, K.A.; Tang, M.; Abramson, M.J.; Dharmage, S.C.; Erbas, B. The association between outdoor allergens—pollen, fungal spore season and high asthma admission days in children and adolescents. Int. J. Environ. Health Res. 2021, 32, 1393–1402. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.W.; Yon, D.K.; James, C.C.; Lee, S.; Koh, H.Y.; Sheen, Y.H.; Oh, J.W.; Han, M.Y.; Sugihara, G. Short-term effects of multiple outdoor environmental factors on risk of asthma exacerbations: Age-stratified time-series analysis. J. Allergy Clin. Immunol. 2019, 144, 1542–1550.e1. [Google Scholar] [CrossRef] [Green Version]
- De Roos, A.J.; Kenyon, C.C.; Zhao, Y.; Moore, K.; Melly, S.; Hubbard, R.A.; Henrickson, S.E.; Forrest, C.B.; Diez Roux, A.V.; Maltenfort, M.; et al. Ambient daily pollen levels in association with asthma exacerbation among children in Philadelphia, Pennsylvania. Environ. Int. 2020, 145, 106138. [Google Scholar] [CrossRef]
- Vicendese, D.; Abramson, M.J.; Dharmage, S.C.; Tang, M.L.; Allen, K.J.; Erbas, B. Trends in asthma readmissions among children and adolescents over time by age, gender and season. J. Asthma 2014, 51, 1055–1060. [Google Scholar] [CrossRef]
- Ghosh, D.; Chakraborty, P.; Gupta, J.; Biswas, A.; Roy, I.; Das, S.; Gupta-Bhattacharya, S. Associations between pollen counts, pollutants, and asthma-related hospital admissions in a high-density Indian metropolis. J. Asthma 2012, 49, 792–799. [Google Scholar] [CrossRef]
- Gonzalez-Barcala, F.J.; Aboal-Viñas, J.; Aira, M.J.; Regueira-Méndez, C.; Valdes-Cuadrado, L.; Carreira, J.; Garcia-Sanz, M.T.; Takkouche, B. Influence of pollen level on hospitalizations for asthma. Arch. Environ. Occup. Health 2013, 68, 66–71. [Google Scholar] [CrossRef]
- Guilbert, A.; Cox, B.; Bruffaerts, N.; Hoebeke, L.; Packeu, A.; Hendrickx, M.; De Cremer, K.; Bladt, S.; Brasseur, O.; Van Nieuwenhuyse, A. Relationships between aeroallergen levels and hospital admissions for asthma in the Brussels-Capital Region: A daily time series analysis. Environ. Health 2018, 17, 35. [Google Scholar] [CrossRef] [Green Version]
- Hayden, T.J.; Muscatello, D.J. Increased presentations to emergency departments for asthma associated with rye grass pollen season in inland NSW. NSW Public Health Bull. 2011, 22, 154–158. [Google Scholar] [CrossRef] [Green Version]
- Jariwala, S.; Toh, J.; Shum, M.; de Vos, G.; Zou, K.; Sindher, S.; Patel, P.; Geevarghese, A.; Tavdy, A.; Rosenstreich, D. The association between asthma-related emergency department visits and pollen and mold spore concentrations in the Bronx, 2001–2008. J. Asthma 2014, 51, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Krmpotic, D.; Luzar-Stiffler, V.; Rakusic, N.; Stipic Markovic, A.; Hrga, I.; Pavlovic, M. Effects of traffic air pollution and hornbeam pollen on adult asthma hospitalizations in Zagreb. Int. Arch. Allergy Immunol. 2011, 156, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Makra, L.; Matyasovszky, I.; Bálint, B.; Csépe, Z. Association of allergic rhinitis or asthma with pollen and chemical pollutants in Szeged, Hungary, 1999–2007. Int. J. Biometeorol. 2014, 58, 753–768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- May, L.; Carim, M.; Yadav, K. Adult asthma exacerbations and environmental triggers: A retrospective review of ED visits using an electronic medical record. Am. J. Emerg. Med. 2011, 29, 1074–1082. [Google Scholar] [CrossRef]
- Osborne, N.J.; Alcock, I.; Wheeler, B.W.; Hajat, S.; Sarran, C.; Clewlow, Y.; McInnes, R.N.; Hemming, D.; White, M.; Vardoulakis, S.; et al. Pollen exposure and hospitalization due to asthma exacerbations: Daily time series in a European city. Int. J. Biometeorol. 2017, 61, 1837–1848. [Google Scholar] [CrossRef] [Green Version]
- Rosas, I.; McCartney, H.A.; Payne, R.W.; Calderón, C.; Lacey, J.; Chapela, R.; Ruiz-Velazco, S. Analysis of the relationships between environmental factors (aeroallergens, air pollution, and weather) and asthma emergency admissions to a hospital in Mexico City. Allergy 1998, 53, 394–401. [Google Scholar] [CrossRef]
- Makra, L.; Matyasovszky, I.; Bálint, B. Association of allergic asthma emergency room visits with the main biological and chemical air pollutants. Sci. Total Environ. 2012, 432, 288–296. [Google Scholar] [CrossRef]
- Rossi, O.V.; Kinnula, V.L.; Tienari, J.; Huhti, E. Association of severe asthma attacks with weather, pollen, and air pollutants. Thorax 1993, 48, 244–248. [Google Scholar] [CrossRef] [Green Version]
- Brunekreef, B.; Hoek, G.; Fischer, P.; Spieksma, F.T. Relation between airborne pollen concentrations and daily cardiovascular and respiratory-disease mortality. Lancet 2000, 355, 1517–1518. [Google Scholar] [CrossRef]
- Hanigan, I.C.; Johnston, F.H. Respiratory hospital admissions were associated with ambient airborne pollen in Darwin, Australia, 2004–2005. Clin. Exp. Allergy 2007, 37, 1556–1565. [Google Scholar] [CrossRef]
- Cirera, L.; Garcia-Marcos, L.; Giménez, J.; Moreno-Grau, S.; Tobías, A.; Pérez-Fernández, V.; Elvira-Rendeles, B.; Guillén, J.; Navarro, C. Daily effects of air pollutants and pollen types on asthma and COPD hospital emergency visits in the industrial and Mediterranean Spanish city of Cartagena. Allergol. Immunopathol. 2012, 40, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Sauerzapf, V.; Jones, A.P.; Cross, J. Environmental factors and hospitalisation for chronic obstructive pulmonary disease in a rural county of England. J. Epidemiol. Community Health 2009, 63, 324–328. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Krafft, T.; Zhang, D.; Xu, J.; Wang, W. The association between daily outpatient visits for allergic rhinitis and pollen levels in Beijing. Sci. Total Environ. 2012, 417–418, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Ayres, J.G. Trends in asthma and hay fever in general practice in the United Kingdom 1976–83. Thorax 1986, 41, 111–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedersen, P.A.; Rung Weeke, E. Seasonal variation of asthma and allergic rhinitis. Consultation pattern in general practice related to pollen and spore counts and to five indicators of air pollution. Allergy 1984, 39, 165–170. [Google Scholar] [CrossRef]
- Ross, A.M.; Corden, J.M.; Fleming, D.M. The role of oak pollen in hay fever consultations in general practice and the factors influencing patients’ decisions to consult. Br. J. Gen. Pract. 1996, 46, 451–455. [Google Scholar]
- Huynh, B.T.; Tual, S.; Turbelin, C.; Pelat, C.; Cecchi, L.; D’Amato, G.; Blanchon, T.; Annesi-Maesano, I. Short-term effects of airborne pollens on asthma attacks as seen by general practitioners in the Greater Paris area, 2003–2007. Prim. Care Respir. J. 2010, 19, 254–259. [Google Scholar] [CrossRef] [Green Version]
- Kitinoja, M.A.; Hugg, T.T.; Siddika, N.; Rodriguez Yanez, D.; Jaakkola, M.S.; Jaakkola, J.J.K. Short-term exposure to pollen and the risk of allergic and asthmatic manifestations: A systematic review and meta-analysis. BMJ Open 2020, 10, e029069. [Google Scholar] [CrossRef]
- Jones, P.J.; Koolhof, I.S.; Wheeler, A.J.; Williamson, G.J.; Lucani, C.; Campbell, S.L.; Bowman, D.; Cooling, N.; Gasparrini, A.; Johnston, F.H. Characterising non-linear associations between airborne pollen counts and respiratory symptoms from the AirRater smartphone app in Tasmania, Australia: A case time series approach. Environ. Res. 2021, 200, 111484. [Google Scholar] [CrossRef]
- Gruzieva, O.; Pershagen, G.; Wickman, M.; Melén, E.; Hallberg, J.; Bellander, T.; Lõhmus, M. Exposure to grass pollen—But not birch pollen--affects lung function in Swedish children. Allergy 2015, 70, 1181–1183. [Google Scholar] [CrossRef]
- Lambert, K.A.; Katelaris, C.; Burton, P.; Cowie, C.; Lodge, C.; Garden, F.L.; Prendergast, L.A.; Toelle, B.G.; Erbas, B. Tree pollen exposure is associated with reduced lung function in children. Clin. Exp. Allergy 2020, 50, 1176–1183. [Google Scholar] [CrossRef] [PubMed]
- Amazouz, H.; Bougas, N.; Thibaudon, M.; Lezmi, G.; Beydon, N.; Bourgoin-Heck, M.; Just, J.; Momas, I.; Rancière, F. Association between lung function of school age children and short-term exposure to air pollution and pollen: The PARIS cohort. Thorax 2021, 76, 887–894. [Google Scholar] [CrossRef] [PubMed]
- Lu, S.; Ren, J.; Hao, X.; Liu, D.; Zhang, R.; Wu, M.; Yi, F.; Lin, J.; Shinich, Y.; Wang, Q. Characterization of protein expression of Platanus pollen following exposure to gaseous pollutants and vehicle exhaust particles. Aerobiologia 2014, 30, 281–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wayne, P.; Foster, S.; Connolly, J.; Bazzaz, F.; Epstein, P. Production of allergenic pollen by ragweed (Ambrosia artemisiifolia L.) is increased in CO2-enriched atmospheres. Ann. Allergy Asthma Immunol. 2002, 88, 279–282. [Google Scholar] [CrossRef]
- Beck, I.; Jochner, S.; Gilles, S.; McIntyre, M.; Buters, J.T.M.; Schmidt-Weber, C.; Behrendt, H.; Ring, J.; Menzel, A.; Traidl-Hoffmann, C. High Environmental Ozone Levels Lead to Enhanced Allergenicity of Birch Pollen. PLoS ONE 2013, 8, e80147. [Google Scholar] [CrossRef] [Green Version]
- Anenberg, S.C.; Haines, S.; Wang, E.; Nassikas, N.; Kinney, P.L. Synergistic health effects of air pollution, temperature, and pollen exposure: A systematic review of epidemiological evidence. Environ. Health 2020, 19, 130. [Google Scholar] [CrossRef]
- Lam, H.C.Y.; Jarvis, D.; Fuertes, E. Interactive effects of allergens and air pollution on respiratory health: A systematic review. Sci. Total Environ. 2021, 757, 143924. [Google Scholar] [CrossRef]
- Canova, C.; Heinrich, J.; Anto, J.M.; Leynaert, B.; Smith, M.; Kuenzli, N.; Zock, J.P.; Janson, C.; Cerveri, I.; de Marco, R.; et al. The influence of sensitisation to pollens and moulds on seasonal variations in asthma attacks. Eur. Respir. J. 2013, 42, 935–945. [Google Scholar] [CrossRef]
- Delfino, R.J.; Zeiger, R.S.; Seltzer, J.M.; Street, D.H.; McLaren, C.E. Association of asthma symptoms with peak particulate air pollution and effect modification by anti-inflammatory medication use. Environ. Health Perspect. 2002, 110, A607–A617. [Google Scholar] [CrossRef] [Green Version]
- Murray, C.S.; Poletti, G.; Kebadze, T.; Morris, J.; Woodcock, A.; Johnston, S.L.; Custovic, A. Study of modifiable risk factors for asthma exacerbations: Virus infection and allergen exposure increase the risk of asthma hospital admissions in children. Thorax 2006, 61, 376–382. [Google Scholar] [CrossRef] [Green Version]
- Idrose, N.S.; Vicendese, D.; Peters, R.L.; Koplin, J.J.; Douglass, J.A.; Walters, E.H.; Perret, J.L.; Lowe, A.J.; Tang, M.L.K.; Newbigin, E.J.; et al. Children with food allergy are at risk of lower lung function on high pollen days. J. Allergy Clin. Immunol. Pract. 2022; in press. [Google Scholar] [CrossRef] [PubMed]
- Cakmak, S.; Dales, R.E.; Judek, S.; Coates, F. Does socio-demographic status influence the effect of pollens and molds on hospitalization for asthma? Results from a time-series study in 10 Canadian cities. Ann. Epidemiol. 2005, 15, 214–218. [Google Scholar] [CrossRef] [PubMed]
- Diemer, M.A.; Mistry, R.S.; Wadsworth, M.E.; López, I.; Reimers, F. Best practices in conceptualizing and measuring social class in psychological research. Anal. Soc. Issues Public Policy 2013, 13, 77–113. [Google Scholar] [CrossRef]
- Witonsky, J.; Abraham, R.; Toh, J.; Desai, T.; Shum, M.; Rosenstreich, D.; Jariwala, S.P. The association of environmental, meteorological, and pollen count variables with asthma-related emergency department visits and hospitalizations in the Bronx. J. Asthma 2019, 56, 927–937. [Google Scholar] [CrossRef]
- Wardman, A.E.; Stefani, D.; MacDonald, J.C. Thunderstorm-associated asthma or shortness of breath epidemic: A Canadian case report. Can. Respir. J. 2002, 9, 267–270. [Google Scholar] [CrossRef]
- Girgis, S.T.; Marks, G.B.; Downs, S.H.; Kolbe, A.; Car, G.N.; Paton, R. Thunderstorm-associated asthma in an inland town in south-eastern Australia. Who is at risk? Eur. Respir. J. 2000, 16, 3–8. [Google Scholar] [CrossRef] [Green Version]
- Wüthrich, B.; Schmid-Grendelmeier, P.; Schindler, C.; Imboden, M.; Bircher, A.; Zemp, E.; Probst-Hensch, N. Prevalence of atopy and respiratory allergic diseases in the elderly SAPALDIA population. Int. Arch. Allergy Immunol. 2013, 162, 143–148. [Google Scholar] [CrossRef] [Green Version]
- Keller, T.; Hohmann, C.; Standl, M.; Wijga, A.H.; Gehring, U.; Melén, E.; Almqvist, C.; Lau, S.; Eller, E.; Wahn, U.; et al. The sex-shift in single disease and multimorbid asthma and rhinitis during puberty—A study by MeDALL. Allergy 2018, 73, 602–614. [Google Scholar] [CrossRef] [Green Version]
- Hew, M.; Lee, J.; Susanto, N.H.; Prasad, S.; Bardin, P.G.; Barnes, S.; Ruane, L.; Southcott, A.M.; Gillman, A.; Young, A.; et al. The 2016 Melbourne thunderstorm asthma epidemic: Risk factors for severe attacks requiring hospital admission. Allergy 2019, 74, 122–130. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Idrose, N.S.; Lodge, C.J.; Erbas, B.; Douglass, J.A.; Bui, D.S.; Dharmage, S.C. A Review of the Respiratory Health Burden Attributable to Short-Term Exposure to Pollen. Int. J. Environ. Res. Public Health 2022, 19, 7541. https://doi.org/10.3390/ijerph19127541
Idrose NS, Lodge CJ, Erbas B, Douglass JA, Bui DS, Dharmage SC. A Review of the Respiratory Health Burden Attributable to Short-Term Exposure to Pollen. International Journal of Environmental Research and Public Health. 2022; 19(12):7541. https://doi.org/10.3390/ijerph19127541
Chicago/Turabian StyleIdrose, Nur Sabrina, Caroline J. Lodge, Bircan Erbas, Jo A. Douglass, Dinh S. Bui, and Shyamali C. Dharmage. 2022. "A Review of the Respiratory Health Burden Attributable to Short-Term Exposure to Pollen" International Journal of Environmental Research and Public Health 19, no. 12: 7541. https://doi.org/10.3390/ijerph19127541