
Comprehensive Care after Myocardial Infarction (CCMI): Long-Term Investment in the Health of Polish Citizens


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Genesis of the Programme
3. Qualification Criteria
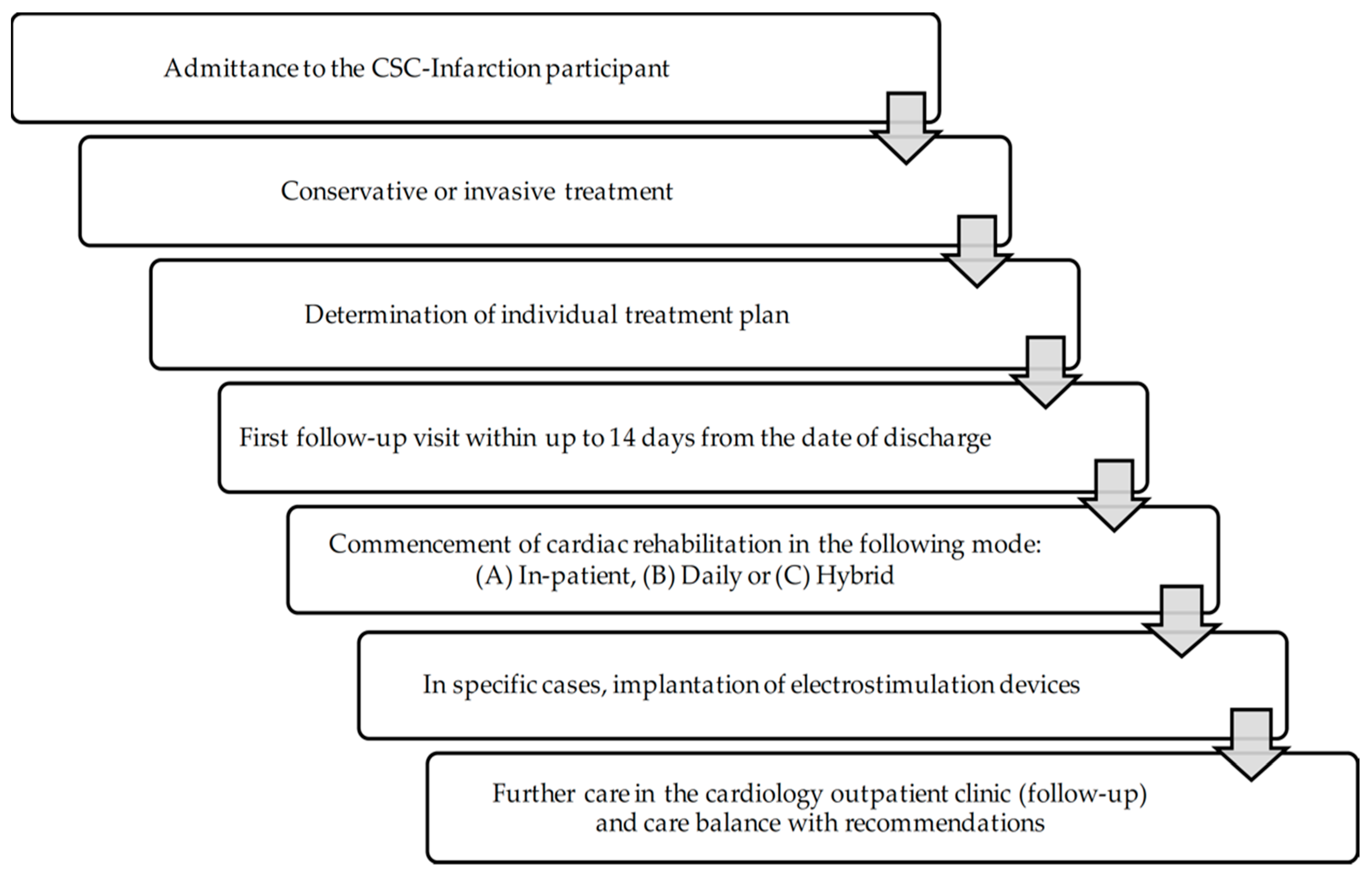
4. Scope of Service
- (1)
- Conservative or invasive treatment or invasive diagnosis of MI;
- (2)
- Implantation of a relevant implantable cardioverter-defibrillator (ICD) or cardiac resynchronisation therapy defibrillator (CRT-D);
- (3)
- Coordination (follow-up) visits within up to 14 days from discharge, during which the following tests and examinations are performed: electrocardiographic examination, laboratory tests (complete blood count, blood potassium level, blood creatinine level, and C-reactive protein level—CRP).
5. Programme Launching
- Module I covered hospitalisation with conservative/invasive treatment and invasive diagnosis. The first component also included preparing the patient care plan and scheduling the coordinating appointment that completed this module,
- Module II covered cardiac rehabilitation, which could be performed in a day, in-patient or hybrid mode. The rehabilitation component should take place for 14 days from hospital discharge after complete coronary revascularisation,
- Module III covered electrotherapy, which can be performed out of turn. In addition, it enables the implantation of CRT-D or ICD,
- Module IV included specialist cardiac care lasting 12 months from MI event.
6. Improving Programme Implementation
- The need to introduce clear and transparent provisions on early withdrawal from CCMI or transfer of the patient to other centres with a signed contract for the provision of these services;
- Absence of a correction factor for cardiology in institutes, such as in the case of implementing the contract for hospital services;
- The need for remuneration for the entities with an in-house rehabilitation ward (analogically to the coronary artery bypass grafting at the cardiology ward in the in-house organisational structure);
- Enabling settlement of correction factor at the time of issuing the certificate of cardiac contraindications to work;
- The problems with settling the services from the catalogue of services to be summed up and maintained at the Anaesthesiology and Intensive Care Unit;
- Enabling all Diagnosis Related Groups (DRGs) in the scope of electrotherapy to be implemented within CCMI.
- (1)
- TREATMENT covers hospitalisation of the patient with MI involving:
- (a)
- Invasive diagnosis of MI (coronary angiography) or conservative treatment;
- (b)
- Invasive treatment covering, among others, complete coronary revascularisation or cardiac surgery (adequately to the clinical condition of the patient);
- (c)
- Single-stage revascularisation during hospitalisation for MI;
- (d)
- Double-stage revascularisation that can be received at the first hospitalisation for MI or divided into two hospitalisations (first for MI and the second planned hospitalisation);
- (e)
- Electrotherapy, including:
- Implantation/replacement of single-chamber pacemaker;
- Implantation/replacement of double-chamber pacemaker;
- Implantation/replacement of cardiac resynchronisation therapy (CRT) device;
- Implantation/replacement of ICD;
- Implantation/replacement of CRT-D;
- Implantation/replacement of S-ICD after assessment of ejection fraction (EF) in the patient within the individual treatment plan prepared during hospitalisation by the cardiologist (cardiac rehabilitation and cardiology outpatient clinic).
- (f)
- Patient treatment plan should be enclosed in the patient’s medical record;
- (2)
- REHABILITATION covers:
- Cardiac rehabilitation or hybrid cardiac telerehabilitation in in-patient conditions;
- Cardiac rehabilitation or hybrid cardiac telerehabilitation in the centre or daily ward under the eligibility criteria and conditions required to provide such rehabilitation laid down in Appendix 5 to the Rehabilitation Ordinance.
- (3)
- FOLLOW-UP covers:
- Coordinating (follow-up) visits;
- Specialist cardiac care within 12 months from MI according to the individual treatment plan (including consultations covering eligibility for implantation of completely automatic implantable cardioverter-defibrillator (ICD), CRT-D or S-ICD and follow-up of implantable devices); the number of consultations and their frequency should depend on the clinical condition on the patient;
- Specialist consultation to complete care within the CCMI.
6.1. Withdrawal
- (a)
- No subsequent care component was provided within the time frame specified in the Hospital Ordinance, Outpatient Ordinance or Rehabilitation Ordinance;
- (b)
- There is a need for third or subsequent revascularisation;
- (c)
- Another MI event took place;
- (d)
- The patient continued treatment with another healthcare provider with a signed contract for CCMI;
- (e)
- The patient died.
6.2. Financing
- (1)
- In the area of treatment:
- (a)
- Invasive diagnosis, conservative treatment, covering following the clinical condition of the patient, coronary revascularisation or coronary artery bypass grafting provided within hospitalisation: settled within the DRG from the catalogue of comprehensive services;
- (b)
- Additional services settled as unitary products listed in the catalogue of services (Appendix 1c and 1ts to the Hospitalisation Ordinance): to be summed up with relevant DRG from the catalogue of comprehensive services,
- (c)
- Preparation of the individual comprehensive treatment plan after MI: settled as the product from the catalogue of comprehensive services to be summed up with the relevant DRG from this catalogue,
- (d)
- Electrotherapy: settled within the relevant DRG from the catalogue of comprehensive services;
- (2)
- In the area of rehabilitation:
- (a)
- In-patient cardiac rehabilitation: settled within the CRMI group (cardiac rehabilitation as part of comprehensive care after myocardial infarction in an in-patient setting) from the catalogue of comprehensive services;
- (b)
- Cardiac rehabilitation in the centre at the daily ward and hybrid cardiac telerehabilitation provided at the place of stay of the patient: settled as a person/day within the products from the catalogue of comprehensive services.
- (3)
- In the area of follow-up:
- (a)
- Coordinating (follow-up) visit: settled as the product from the catalogue of comprehensive services;
- (b)
- Specialist cardiac care within 12 months from MI covering:
- (c)
- At least three consultations within the period of CCMI coverage: settled on a lump-sum basis after provision within the product from the catalogue of comprehensive services;
- (d)
- Specialist consultation along with care balance in the patient completing the care under CCMI (examinations and assessment of clinical condition): settled within the settlement product: “Specialist cardiac care–care balance” from the catalogue of comprehensive services [10].
6.3. Benefits
- (a)
- In the case of provision of CCMI services at the cardiology ward in the organisational structure, operating in the 24/7 mode with a separated emergency unit, when settling the services of coronary artery bypass grafting within the groups: E04, E05, E06 and E07, the value of these settlement products is corrected with the use of the correction factor of 1.2;
- (b)
- In the case the patient starts cardiac rehabilitation within 14 days from discharge, settlement of provided rehabilitation is corrected with the use of the correction factor of 1.1;
- (c)
- In the case of the provision of CCMI services at the daily cardiac rehabilitation ward in the organisational structure, when settling the daily rehabilitation services, the value of these settlement products is corrected with the use of the correction factor of 1.1;
- (d)
- If a professionally active patient after MI will receive a medical certificate issued by the attending physician of no cardiovascular contraindications to take up/perform a job up to the fourth month from discharge, the value of settlement products (laid down for treatment and follow-up), is corrected with the use of correction factor of 1.1 after issuing of this certificate;
- (e)
- If the patient received all services specified in the individual treatment plan within 12 months under the CCMI assumptions: the value of settlement products (laid down for treatment and follow-up), is corrected with the use of a correction factor of 1.15 when settling the care balance;
- (f)
- For the healthcare providers being:
- The institutes referred to in Article 3 of the Act of 30 April 2010 on research institutes (Journal of Laws of 2019, item 1350);
- Medical entities established and operated by a medical university in the meaning of Article 2 (1) (13) of the Act of 15 April 2011 on medical activity;
- Medical entities established and operated by the State Treasury represented by the minister, involved in post-gradual education of physicians;
- Medical entities providing a medical university with access to organisational units necessary to perform pre- and post-graduate education in medical professions based on the agreement referred to in Article 89(4) of the Act of 15 April 2011 on medical activity (the entity is obliged to present the agreement to the competent branch of the Fund);
- Providing the services to the healthcare providers in the scope of CCMI, DRG value: E10, E11, E12, E12G, E15, E16, E17G, E23G, E24G, E26 and E29 is corrected with the use of the correction factor of 1.1.
- (g)
- In the case of provision of services within the SCS-Infarction within the groups:
- E23G, E24G, E26, E29, E04, E05, E06, E32, E33, E34 and E36, the value of settlement products is corrected with the use of the correction factor of 1.085;
- (h)
- For healthcare providers providing the services within the CCMI, in which the share of hospitalised patients with diagnosed acute MI treated within the CCMI is at least 60% of all hospitalised patients with this diagnosis, the value of products for settlement of hospitalisation in this healthcare provider (settled with the groups E10, E11, E12G and E15) is corrected with the use of the correction factor of 1.02;
- (i)
- For healthcare providers, in which the share of the patients who received all services specified in the individual treatment plan due to the CCMI assumptions is at least 70% (excluding deaths) of all patients covered with CCMI, the value of products for settlement of hospitalisation (settled with groups E10, E11, E12G and E15) within the CCMI is corrected with the use of the correction factor of 1.03 [10].
7. Quality Parameters of the Programme Evaluation
- (1)
- Percentage share of the patients after MI covered with CCMI;
- (2)
- Percentage share of the patients who received the enter individual treatment plan;
- (3)
- Percentage share of re-hospitalisations for cardiovascular reasons;
- (4)
- share of the patients who have undergone the coronary angioplasty procedure within the second stage of revascularisation;
- (5)
- Share of the patients with ICD;
- (6)
- Share of the patients with implanted cardioverter/defibrillator of CRT-D type;
- (7)
- Share of the patients with implanted S-ICD;
- (8)
- Percentage share of deaths after cardiovascular episodes within:
- 6 months from MI;
- 12 months from MI.
- (1)
- Share of the patients who received complete cardiac rehabilitation and reasons for withdrawal from cardiac rehabilitation [%];
- (2)
- Share of the patients who received complete revascularisation and the reasons for failure to provide complete revascularisation;
- (3)
- Share of the patients with left ventricle EF <35%, with implanted relevant
- (4)
- ICD or CRT-D system and the reasons for failure to perform implantation;
- (5)
- Share of the patients who quit smoking [%]–confirmed by a test;
- (6)
- Share of the patients with LDL <1.8 mmol/L [<70 mg%] [%];
- (7)
- Share of the patients with blood pressure <140/90 mmHg [%];
- (8)
- Share of the patients with glycated haemoglobin <7% or fasting blood glucose <7.0 mmol/L [<126 mg%] [%];
- (9)
- Share of the patients with BMI <30 kg/m2 [%].
8. Primary Prevention
- (1)
- Hypertension (RR > 140/90 mmHg);
- (2)
- Lipid disorders (increased total blood cholesterol, LDL-cholesterol, triglycerides and low LDL-cholesterol level);
- (3)
- Tobacco smoking;
- (4)
- Low physical activity;
- (5)
- Overweight and obesity;
- (6)
- Impaired glucose tolerance;
- (7)
- Increased fibrinogen level;
- (8)
- Increased uric acid level;
- (9)
- Excessive stress;
- (10)
- Poor diet;
- (11)
- Age;
- (12)
- Male sex;
- (13)
- Henetic loads listed by the general practitioner at the healthcare provider’s and in a given calendar year, covered with the healthcare service contract, aged 35, 40, 45, 50 and 55, with no diagnosed CVDs and receiving no services provided within the CVDs prevention within the last five years (including in the other healthcare providers).
9. The Required Medical Procedures for Cardiovascular Diseases
- (1)
- Medical history and completing the preventive check-up report;
- (2)
- Blood biochemical tests (total blood cholesterol, LDL-cholesterol, HDL-cholesterol, triglycerides and blood glucose levels), blood pressure measurement, body mass index (BMI) determination;
- (3)
- Scheduling the visit at the general practitioner holding the list with the name of this patient;
- (4)
- Entering the test results into the prevention check-up report;
- (5)
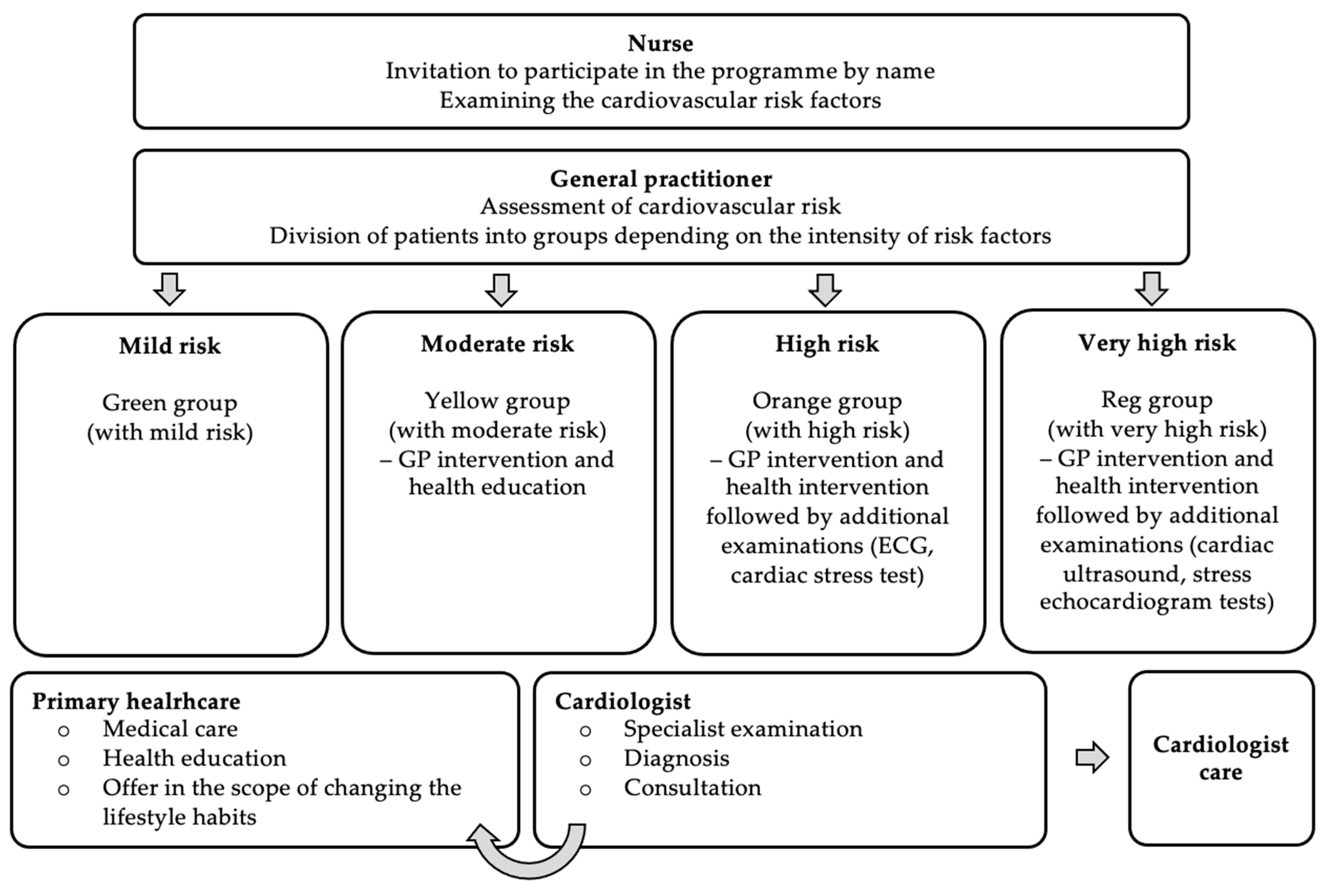
- During the visit at the general practitioner:
- (a)
- Examination of healthcare service recipient and assessment of cardiovascular risk factors;
- (b)
- Classification of the patient into the respective risk group and assessment of the global risk of the cardiovascular incident in future according to SCORE and entering the obtained score in the preventive check-up report;
- (c)
- Health education of the patient and decision on further management.
- (6)
- Providing information on examination results by the general physician to the patient with diagnosed CVD and giving recommendations on the need to change lifestyle habits or referring the patient to further diagnosing or treatment.
10. Conclusions and Recommendations on Health Policy
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wojtyniak, B.; Goryński, P. Health Status of Polish Population and Its Determinants, 2020; National Institute of Public Health—National Institute of Hygiene: Warsaw, Poland, 2020; ISBN 978-83-65870-36-0. [Google Scholar]
- National Health Found. NHF on Health—Ischemic Heart Disease; National Health Found: Warsaw, Poland, 2020.
- Polish Society of Cardiology Laboratory. Database of the Association of Cardiovascular Interventions of the Polish Society of Cardiology. Available online: https://aisn.pl/pracownie/mapa_pracowni (accessed on 20 December 2020).
- Supreme Chamber of Control. Provision of Health Care Services in the Field of Cardiology by Public and Non-Public Health Care Entities; Supreme Chamber of Control: Warsaw, Poland, 2016.
- Agency for Health Technology Assessment and Tariff System. Comprehensive Care after Myocardial Infarction; Agency for Health Technology Assessment and Tariff System (AOTMiT): Warsaw, Poland, 2016.
- Jankowski, P.; Niewada, M.; Bochenek, A.; Bochenek-Klimczyk, K.; Bogucki, M.; Drygas, W.; Dudek, D.; Eysymontt, Z.; Grajek, S.; Kozierkiewicz, A.; et al. Optimal Model of Comprehensive Rehabilitation and Secondary Prevention. Kardiol. Pol. 2013, 71, 995–1003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strzelecki, Z.; Szymborski, J. (Eds.) Morbidity and Mortality of Cardiovascular Diseases and the Demographic Situation of Poland; Rządowa Rada Ludnościowa: Warsaw, Poland, 2015.
- Kubielas, G.; Diakowska, D.; Uchmanowicz, I. Survival Analysis of Patients with Acute Coronary Syndrome Receiving Comprehensive Coordinated Care after Myocardial Infarction (KOS-Zawał). Kardiol. Pol. 2022, 80, 315–321. [Google Scholar] [CrossRef] [PubMed]
- Gziut, A.I.; Sobieszek, A.; Milewski, K. Cardiac rehabilitation in patients with acute myocardial infarction. Kardiol. Inwazyjna 2018, 13, 17–21. [Google Scholar]
- Ministry of Health Announcement of the Minister of Health of 31 December 2020 on the Declaration of the Consolidated Text of the Regulation of the Minister of Health on Guaranteed Benefits in the Field of Hospital Treatment (Journal of Laws 2021, Item 290). Available online: https://isap.sejm.gov.pl/isap.nsf/DocDetails.xsp?id=WDU20210000290 (accessed on 24 November 2021).
- National Health Found Ordinance No. 38/2017/DSOZ of the President of the National Health Fund of 29 May 2017 on Defining the Conditions for Conclusion and Performance of Contracts in the Type of Hospital Treatment—Complex Services. Available online: https://www.nfz.gov.pl/zarzadzenia-prezesa/zarzadzenia-prezesa-nfz/zarzadzenie-nr-382017dsoz,6578.html (accessed on 23 November 2021).
- Sobieszek, A.; Milewski, K. Specialized managed care—Heart attack. Kardiol. Inwazyjna 2017, 12, 4–6. [Google Scholar]
- National Health Found Reporting Instructions for Comprehensive Care Services after Myocardial Infarction. Available online: https://www.nfz.gov.pl/aktualnosci/aktualnosci-centrali (accessed on 23 November 2021).
- Rutkowski, D. KOS Myocardial Infarction-Treatment; Payer Perspective: Krakow, Poland, 2018. [Google Scholar]
- Banach, M.; Kaźmierczak, J.; Mitkowski, P.; Wita, K.; Broncel, M.; Gąsior, M.; Gierlotka, M.; Gil, R.; Jankowski, P.; Niewada, M.; et al. Which patients at risk of cardiovascular disease might benefit the most from inclisiran? Polish experts opinion. The compromise between EBM and possibilities in healthcare. Arch. Med. Sci. 2022, 18, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Wita, K.; Kułach, A.; Wita, M.; Wybraniec, M.T.; Wilkosz, K.; Polak, M.; Matla, M.; Maciejewski, Ł.; Fluder, J.; Kalańska-Łukasik, B.; et al. Managed Care after Acute Myocardial Infarction (KOS-zawał) reduces major adverse cardiovascular events by 45% in 3-month follow-up—single-center results of Poland’s National Health Fund program of comprehensive post-myocardial infarction care. Arch. Med. Sci. 2019, 16, 551–558. [Google Scholar] [CrossRef] [PubMed]
- National Health Found Ordinance No. 10/2019/DSOZ of the President of the National Health Fund of 31 January 2019 on the Conditions for Conclusion and Performance of Agreements in the Type of Hospital Treatment—Complex Services. Available online: https://www.nfz.gov.pl/zarzadzenia-prezesa/zarzadzenia-prezesa-nfz/zarzadzenie-nr-102019dsoz,6874.html (accessed on 23 November 2021).
- Ministry of Health Regulation of the Minister of Health of 27 February 2018 on Health Priorities (Journal of Laws, Item 469). Available online: http://isap.sejm.gov.pl/isap.nsf/DocDetails.xsp?id=WDU20180000469 (accessed on 23 November 2021).
- Council of Ministers Regulation of the Council of Ministers of 4 August 2016 on the National Health Programme 2016–2020 (Journal of Laws, Item 1492). Available online: https://isap.sejm.gov.pl/isap.nsf/DocDetails.xsp?id=WDU20160001492 (accessed on 23 November 2021).
- Pura, A.M.; Wilk, M.; Kuczyńska, G.; Bielecka, K.; Bielecka, L.; Wąchała, K.; Olszowska, M. Acute Myocardial Infarction Risk Factors among Population with Premature Cardiovascular Disease. Arter. Hypertens. 2018, 22, 81–86. [Google Scholar] [CrossRef]
- KORDIAN National Program for Prevention of Arteriosclerosis and Heart Disease through Education of People with Increased Cardiovascular Risk Factors 2021. Available online: https://programkordian.pl (accessed on 20 December 2020).
- Ministry of Health Regulation of the Minister of Health of 24 September 2013 on Guaranteed Services in the Field of Primary Health Care (Journal of Laws of 2021, Item 540). Available online: http://isap.sejm.gov.pl/isap.nsf/DocDetails.xsp?id=WDU20130001248 (accessed on 23 November 2021).
- National Health Found Ordinance No. 160/2021/DSOZ of the President of the National Health Fund of 30 September 2021 on the Conditions for the Conclusion and Implementation of Agreements on the Provision of Health Care Services in the Field of Primary Health Care. Available online: https://www.nfz.gov.pl/zarzadzenia-prezesa/zarzadzenia-prezesa-nfz (accessed on 23 November 2021).





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kubielas, G.; Hydzik, P.; Rypicz, Ł. Comprehensive Care after Myocardial Infarction (CCMI): Long-Term Investment in the Health of Polish Citizens. Int. J. Environ. Res. Public Health 2022, 19, 7518. https://doi.org/10.3390/ijerph19127518
Kubielas G, Hydzik P, Rypicz Ł. Comprehensive Care after Myocardial Infarction (CCMI): Long-Term Investment in the Health of Polish Citizens. International Journal of Environmental Research and Public Health. 2022; 19(12):7518. https://doi.org/10.3390/ijerph19127518
Chicago/Turabian StyleKubielas, Grzegorz, Paulina Hydzik, and Łukasz Rypicz. 2022. "Comprehensive Care after Myocardial Infarction (CCMI): Long-Term Investment in the Health of Polish Citizens" International Journal of Environmental Research and Public Health 19, no. 12: 7518. https://doi.org/10.3390/ijerph19127518