
Exploring Environmental Health Inequalities: A Scientometric Analysis of Global Research Trends (1970–2020)


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Retrieval
2.2. Analysis and Visualization
3. Results
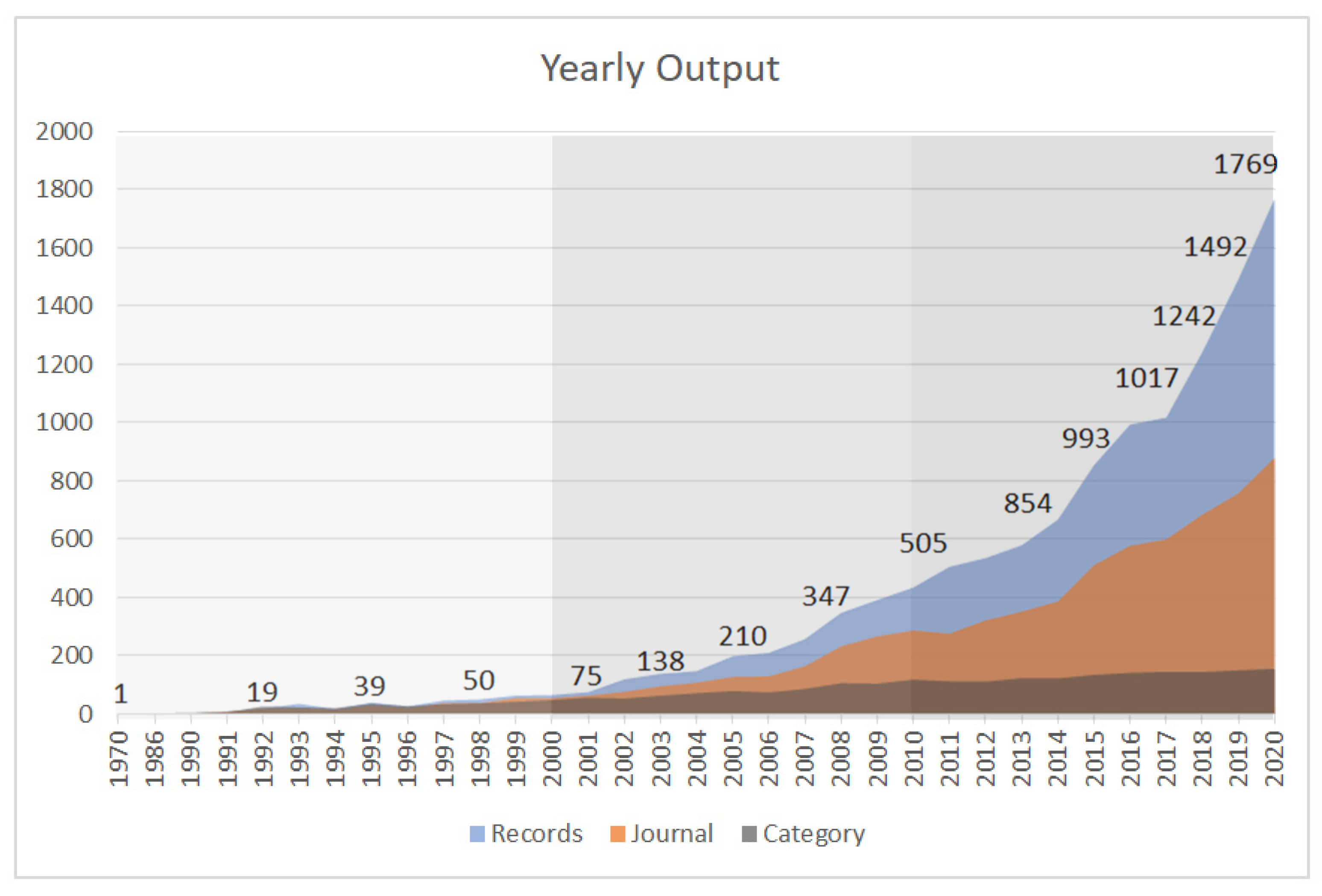
3.1. Evolution of Publication Activity
3.2. Publication Distribution: Countries and Institutions
3.3. Research Trends: Co-Citation Analysis
3.4. Knowledge Domain: Keyword Analysis
3.4.1. Cluster 1 (Green): Environmental Hazards and Benefits
3.4.2. Cluster 2 (Blue): Social Vulnerability
3.4.3. Cluster 3 (Red): Health Disparities
3.5. The Pathway and Framework of Environmental Health Inequality
3.5.1. Driver and Pressure
3.5.2. State: Environmental Hazards and Benefits, Contextual Social Vulnerability
3.5.3. Exposure: Exposure and Access
3.5.4. Effect: Health Outcome Disparities
4. Discussion
4.1. An Overview of EHI Research Status
4.2. The Global Research Trends and Knowledge Domains of EHI
4.3. Perspectives on Potential Mechanisms of EHI
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Evans, G.W.; Kantrowitz, E. Socioeconomic status and health: The potential role of environmental risk exposure. Annu. Rev. Public Health 2002, 23, 303–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bolte, G.; Pauli, A.; Hornberg, C. Environmental justice: Social disparities in environmental exposures and health: Overview. In Encyclopedia of Environmental Health; Elsevier: Amsterdam, The Netherlands, 2011; pp. 459–470. [Google Scholar]
- Schulz, A.; Northridge, M.E. Social Determinants of Health: Implications for Environmental Health Promotion. Health Educ. Behav. 2004, 31, 455–471. [Google Scholar] [CrossRef] [PubMed]
- WHO Regional Office for Europe. Environmental Health Inequalities in Europe. Assessment Report; WHO: Geneva, Switzerland, 2012.
- WHO Regional Office for Europe. Environmental Health Inequalities Resource Package A Tool for Understanding and Reducing Inequalities in Environmental Risk; WHO Regional Office for Europe: Copenhagen, Denmark, 2019. [Google Scholar]
- Bouchard, L.; Albertini, M.; Batista, R.; de Montigny, J. Research on health inequalities: A bibliometric analysis (1966–2014). Soc. Sci. Med. 2015, 141, 100–108. [Google Scholar] [CrossRef]
- European Environment Agency. Unequal Exposure and Unequal Impacts—European Environment Agency; European Environment Agency: Copenhagen, Denmark, 2018.
- Markevych, I.; Schoierer, J.; Hartig, T.; Chudnovsky, A.; Hystad, P.; Dzhambov, A.M.; de Vries, S.; Triguero-Mas, M.; Brauer, M.; Nieuwenhujisen, M.J.; et al. Exploring pathways linking greenspace to health: Theoretical and methodological guidance. Environ. Res. 2017, 158, 301–317. [Google Scholar] [CrossRef] [PubMed]
- Hunter, R.F.; Cleland, C.; Cleary, A.; Droomers, M.; Wheeler, B.W.; Sinnett, D.; Nieuwenhujisen, M.J.; Braubach, M. Environmental, health, wellbeing, social and equity effects of urban green space interventions: A meta-narrative evidence synthesis. Environ. Int. 2019, 130, 104923. [Google Scholar] [CrossRef] [PubMed]
- WHO Regional Office for Europe. The Health Benefits of the Great Outdoors: A Systematic Review and Meta-Analysis of GreenSpace Exposure and Health Outcomes; Academic Press Inc.: Cambridge, MA, USA, 2016. [Google Scholar]
- Rojas-Rueda, D.; Nieuwenhuijsen, M.J.; Gascon, M.; Perez-Leon, D.; Mudu, P. Green spaces and mortality: A systematic review and meta-analysis of cohort studies. Lancet Planet. Health 2019, 3, e469–e477. [Google Scholar] [CrossRef] [Green Version]
- Schüle, S.A.; Hilz, L.K.; Dreger, S.; Bolte, G. Social Inequalities in Environmental Resources of Green and Blue Spaces: A Review of Evidence in the WHO European Region. Int. J. Environ. Res. Public Health 2019, 16, 1216. [Google Scholar] [CrossRef] [Green Version]
- Fairburn, J.; Schüle, S.A.; Dreger, S.; Hilz, L.K.; Bolte, G. Social Inequalities in Exposure to Ambient Air Pollution: A Systematic Review in the WHO European Region. Int. J. Environ. Res. Public Health 2019, 16, 3127. [Google Scholar] [CrossRef] [Green Version]
- Guarnieri, M.; Balmes, J.R. Outdoor air pollution and asthma. Lancet 2014, 383, 1581–1592. [Google Scholar] [CrossRef] [Green Version]
- Pope, C.A.; Burnett, R.T.; Thurston, G.D.; Thun, M.J.; Calle, E.E.; Krewski, D.; Godleski, J.J. Cardiovascular Mortality and Long-Term Exposure to Particulate Air Pollution: Epidemiological Evidence of General Pathophysiological Pathways of Disease. Circulation 2004, 109, 71–77. [Google Scholar] [CrossRef] [Green Version]
- Krämer, U.; Herder, C.; Sugiri, D.; Strassburger, K.; Schikowski, T.; Ranft, U.; Rathmann, W. Traffic-related air pollution and incident type 2 diabetes: Results from the SALIA cohort study. Environ. Health Perspect. 2010, 118, 1273–1279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ha, S.; Sundaram, R.; Louis, G.M.B.; Nobles, C.; Seeni, I.; Sherman, S.; Mendola, P. Ambient air pollution and the risk of pregnancy loss: A prospective cohort study. Fertil. Steril. 2018, 109, 148–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansell, A. Noise and Health in Pregnancy and Birth Outcomes; ISEE: Durham, NC, USA, 2018. [Google Scholar]
- Gidlöf-Gunnarsson, A.; Öhrström, E. Noise and well-being in urban residential environments: The potential role of perceived availability to nearby green areas. Landsc. Urban Plan. 2007, 83, 115–126. [Google Scholar] [CrossRef]
- Dreger, S.; Schüle, S.; Hilz, L.; Bolte, G. Social Inequalities in Environmental Noise Exposure: A Review of Evidence in the WHO European Region. Int. J. Environ. Res. Public Health 2019, 16, 1011. [Google Scholar] [CrossRef] [Green Version]
- Knol, A.B.; Briggs, D.J.; Lebret, E. Assessment of complex environmental health problems: Framing the structures and structuring the frameworks. Sci. Total Environ. 2010, 408, 2785–2794. [Google Scholar] [CrossRef]
- WHO Regional Office for Europe. Environmental Health Inequalities in Europe: Second Assessment Report; WHO: Geneva, Switzerland, 2019.
- Brousmiche, D.; Occelli, F.; Genin, M.; Cuny, D.; Deram, A.; Lanier, C. Spatialized composite indices to evaluate environmental health inequalities: Meeting the challenge of selecting relevant variables. Ecol. Indic. 2020, 111, 106023. [Google Scholar] [CrossRef]
- Lakes, T.; Brückner, M.; Krämer, A. Development of an environmental justice index to determine socio-economic disparities of noise pollution and green space in residential areas in Berlin. J. Environ. Plan. Manag. 2014, 57, 538–556. [Google Scholar] [CrossRef]
- Fortunato, S.; Bergstrom, C.T.; Börner, K.; Evans, J.A.; Helbing, D.; Milojević, S.; Petersen, A.M.; Radicchi, F.; Sinatra, R.; Uzzi, B.; et al. Science of science. Science 2018, 359, 6379. [Google Scholar] [CrossRef] [Green Version]
- Mao, G.; Liu, X.; Du, H.; Zuo, J.; Li, N. An Expanding and Shifting Focus in Recent Environmental Health Literature: A Quantitative Bibliometric Study. J. Environ. Health 2016, 78, 54–61. [Google Scholar]
- Orimoloye, I.R.; Ololade, O.O. Global trends assessment of environmental health degradation studies from 1990 to 2018. Environ. Dev. Sustain. 2021, 23, 3251–3264. [Google Scholar] [CrossRef]
- Wang, M.; Liu, P.; Zhang, R.; Li, Z.; Li, X. A scientometric analysis of global health research. Int. J. Environ. Res. Public Health 2020, 17, 2963. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.; Li, K.; Gu, D.; Wang, X.; Yang, X.; Zhu, K.; Liang, G. Visualizing knowledge evolution and hotspots of rural environment and health: A systematic review and research direction. IEEE Access 2019, 7, 72538–72550. [Google Scholar] [CrossRef]
- Zhang, J.; Yu, Z.; Zhao, B.; Sun, R.; Vejre, H. Links between green space and public health: A bibliometric review of global research trends and future prospects from 1901 to 2019. Environ. Res. Lett. 2020, 15, 063001. [Google Scholar] [CrossRef]
- Dhital, S.; Rupakheti, D. Bibliometric analysis of global research on air pollution and human health: 1998–2017. Environ. Sci. Pollut. Res. 2019, 26, 13103–13114. [Google Scholar] [CrossRef]
- Hamidi, A.; Ramavandi, B. Evaluation and scientometric analysis of researches on air pollution in developing countries from 1952 to 2018. Air Qual. Atmos. Health 2020, 13, 797–806. [Google Scholar] [CrossRef]
- Sweileh, W.M. Bibliometric analysis of peer-reviewed literature on climate change and human health with an emphasis on infectious diseases. Glob. Health 2020, 16, 44. [Google Scholar] [CrossRef] [PubMed]
- Nelson, J.R.; Grubesic, T.H. Environmental Justice: A Panoptic Overview Using Scientometrics. Sustainability 2018, 10, 1022. [Google Scholar] [CrossRef] [Green Version]
- Wang, Q.; Waltman, L. Large-scale analysis of the accuracy of the journal classification systems of Web of Science and Scopus. J. Informetr. 2016, 10, 347–364. [Google Scholar] [CrossRef] [Green Version]
- Aria, M.; Cuccurullo, C. bibliometrix: An R-tool for comprehensive science mapping analysis. J. Informetr. 2017, 11, 959–975. [Google Scholar] [CrossRef]
- Hussein, A.S. Visualizing document similarity using n-grams and latent semantic analysis. In Proceedings of the 2016 SAI Computing Conference, SAI 2016, London, UK, 13–15 July 2016; pp. 269–279. [Google Scholar]
- Chen, C. CiteSpace II: Detecting and visualizing emerging trends and transient patterns in scientific literature. J. Am. Soc. Inf. Sci. Technol. 2006, 57, 359–377. [Google Scholar] [CrossRef] [Green Version]
- Van Eck, N.J.; Waltman, L. Software survey: VOSviewer, a computer program for bibliometric mapping. Scientometrics 2010, 84, 523–538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.; Yu, Q.; Zheng, F.; Long, C.; Lu, Z.; Duan, Z. Comparing keywords plus of WOS and author keywords: A case study of patient adherence research. J. Assoc. Inf. Sci. Technol. 2016, 67, 967–972. [Google Scholar] [CrossRef]
- Bullard, R.D.; Wright, B.H. Environmental justice for all: Community perspectives on health and research needs. Toxicol. Ind. Health 1993, 9, 821–841. [Google Scholar] [CrossRef] [PubMed]
- Brown, P. Race, class, and environmental health: A review and systematization of the literature. Environ. Res. 1995, 69, 15–30. [Google Scholar] [CrossRef]
- Lynch, J.W.; Smith, G.D.; Kaplan, G.A.; House, J.S. Income inequality and mortality: Importance to health of individual income, psychosocial environment, or material conditions. Br. Med. J. 2000, 320, 1200–1204. [Google Scholar] [CrossRef] [Green Version]
- Lynch, J.; Smith, G.D.; Hillemeier, M.; Shaw, M.; Raghunathan, T.; Kaplan, G. Income inequality, the psychosocial environment, and health: Comparisons of wealthy nations. Lancet 2001, 358, 194–200. [Google Scholar] [CrossRef]
- Williams, D.R.; Neighbors, H. Racism, discrimination and hypertension: Evidence and needed research. Ethn. Dis. 2001, 11, 800–816. [Google Scholar]
- Morello-Frosch, R.; Jesdale, B.M. Separate and unequal: Residential segregation and estimated cancer risks associated with ambient air toxins in U.S. metropolitan areas. Environ. Health Perspect. 2006, 114, 386–393. [Google Scholar] [CrossRef] [Green Version]
- Pickett, K.E.; Pearl, M. Multilevel analyses of neighbourhood socioeconomic context and health outcomes: A critical review. J. Epidemiol. Community Health 2001, 55, 111–122. [Google Scholar] [CrossRef] [Green Version]
- Macintyre, S.; Ellaway, A.; Cummins, S. Place effects on health: How can we conceptualise, operationalise and measure them? Soc. Sci. Med. 2002, 55, 125–139. [Google Scholar] [CrossRef]
- Mitchell, R.; Popham, F. Effect of exposure to natural environment on health inequalities: An observational population study. Lancet 2008, 372, 1655–1660. [Google Scholar] [CrossRef] [Green Version]
- Larson, N.I.; Story, M.T.; Nelson, M.C. Neighborhood Environments. Disparities in Access to Healthy Foods in the U.S. Am. J. Prev. Med. 2009, 36, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Gordon-Larsen, P.; Nelson, M.C.; Page, P.; Popkin, B.M. Inequality in the built environment underlies key health disparities in physical activity and obesity. Pediatrics 2006, 117, 417–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brulle, R.J.; Pellow, D.N. ENVIRONMENTAL JUSTICE: Human Health and Environmental Inequalities. Annu. Rev. Public Health 2006, 27, 103–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morello-Frosch, R.; Zuk, M.; Jerrett, M.; Shamasunder, B.; Kyle, A.D. Understanding the cumulative impacts of inequalities in environmental health: Implications for policy. Health Aff. 2011, 30, 879–887. [Google Scholar] [CrossRef]
- Huang, H.; Wang, A.; Morello-Frosch, R.; Lam, J.; Sirota, M.; Padula, A.; Woodruff, T.J. Cumulative Risk and Impact Modeling on Environmental Chemical and Social Stressors. Curr. Environ. Health Rep. 2018, 5, 88–99. [Google Scholar] [CrossRef]
- Wolch, J.R.; Byrne, J.; Newell, J.P. Urban green space, public health, and environmental justice: The challenge of making cities just green enough. Landsc. Urban Plan. 2014, 125, 234–244. [Google Scholar] [CrossRef] [Green Version]
- Rigolon, A. A complex landscape of inequity in access to urban parks: A literature review. Landsc. Urban Plan. 2016, 153, 160–169. [Google Scholar] [CrossRef]
- Hartig, T.; Mitchell, R.; de Vries, S.; Frumkin, H. Nature and health. Annu. Rev. Public Health 2014, 35, 207–228. [Google Scholar] [CrossRef] [Green Version]
- Hajat, A.; Hsia, C.; O’Neill, M.S. Socioeconomic Disparities and Air Pollution Exposure: A Global Review. Curr. Environ. Health Rep. 2015, 2, 440–450. [Google Scholar] [CrossRef] [Green Version]
- Story, M.; Kaphingst, K.M.; Robinson-O’Brien, R.; Glanz, K. Creating healthy food and eating environments: Policy and environmental approaches. Annu. Rev. Public Health 2008, 29, 253–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sallis, J.F.; Cerin, E.; Conway, T.L.; Adams, M.A.; Frank, L.D.; Pratt, M.; Salvo, D.; Schipperijn, J.; Smith, G.; Cain, K.L.; et al. Physical activity in relation to urban environments in 14 cities worldwide: A cross-sectional study. Lancet 2016, 387, 2207–2217. [Google Scholar] [CrossRef] [Green Version]
- Ogden, C.L.; Carroll, M.D.; Kit, B.K.; Flegal, K.M. Prevalence of childhood and adult obesity in the United States, 2011–2012. JAMA 2004, 311, 806–814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gee, G.C.; Payne-Sturges, D.C. Environmental health disparities: A framework integrating psychosocial and environmental concepts. Environ. Health Perspect. 2004, 112, 1645–1653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, Y.; Yang, Y.; Wang, F.; Zhang, P.; Shi, C.; Zou, Y.; Qin, H. Obesity and Risk of Colorectal Cancer: A Systematic Review of Prospective Studies. PLoS ONE 2013, 8, e53916. [Google Scholar] [CrossRef] [Green Version]
- Carneiro, F.F.; Oliveira ML, C.; Netto, G.F.; Galvão, L.A.; Cancio, J.A.; Bonini, E.M.; Corvalan, C.F.; the Participants in the International Symposium on the Development of Indicators for Environmental Health Integrated Management. Meeting Report: Development of Environmental Health Indicators in Brazil and Other Countries in the Americas. Environ. Health Perspect. 2006, 114, 1407–1408. [Google Scholar] [CrossRef] [Green Version]
- Hambling, T.; Weinstein, P.; Slaney, D. A Review of Frameworks for Developing Environmental Health Indicators for Climate Change and Health. Int. J. Environ. Res. Public Health 2011, 8, 2854–2875. [Google Scholar] [CrossRef]
- Briggs, D. Making a Difference: Indicators to Improve Children’s Environmental Health; WHO: Geneva, Switzerland, 2003; pp. 1–52.
- WHO. Environmental Health Indicators: Framework and Methodologies; WHO: Geneva, Switzerland, 1999.
- Gupta, J.; Scholtens, J.; Perch, L.; Dankelman, I.; Seager, J.; Sánder, F.; Stanley-jones, M.; Kempf, I. Re-imagining the driver–pressure–state–impact–response framework from an equity and inclusive development perspective. Sustain. Sci. 2020, 15, 503–520. [Google Scholar] [CrossRef] [Green Version]
- Spangenberg, J.H.; Maxim, L. Bridging the gap between two analytical frameworks. In Proceedings of the 9th Biennial Conference of ISEE Ecological Sustainability and Human Well-Being, New Delhi, India, 15–19 December 2006. [Google Scholar]
- Waheed, B.; Khan, F.; Veitch, B. Linkage-based frameworks for sustainability assessment: Making a case for driving force-pressure-state-exposure-effect-action (DPSEEA) frameworks. Sustainability 2009, 1, 441–463. [Google Scholar] [CrossRef] [Green Version]
- CSDH. Closing the Gap in a Generation: Health Equity through Action on the Social Determinants of Health; CSDH: Geneva, Switzerland, 2008. [Google Scholar]
- deFur, P.L.; Evans, G.W.; Hubal, E.A.C.; Kyle, A.D.; Morello-Frosch, R.A.; Williams, D.R. Vulnerability as a function of individual and group resources in cumulative risk assessment. Environ. Health Perspect. 2007, 115, 817–824. [Google Scholar] [CrossRef]
- Roux, A.V.D.; Mair, C. Neighborhoods and health. Ann. N. Y. Acad. Sci. 2010, 1186, 125–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fry, A.; Littlejohns, T.J.; Sudlow, C.; Doherty, N.; Adamska, L.; Sprosen, T.; Collins, R.; Allen, N.E. Comparison of Sociodemographic and Health-Related Characteristics of UK Biobank Participants with Those of the General Population. Am. J. Epidemiol. 2017, 186, 1026–1034. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borim, F.S.A.; Francisco PM, S.B.; Neri, A.L. Sociodemographic and health factors associated with mortality in community-dwelling elderly. Rev. Saude Publica 2017, 51, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adler, N.E.; Newman, K. Socioeconomic disparities in health: Pathways and policies. Health Aff. 2002, 21, 60–76. [Google Scholar] [CrossRef] [PubMed]
- Schüle, S.A.; Gabriel, K.M.A.; Bolte, G. Relationship between neighbourhood socioeconomic position and neighbourhood public green space availability: An environmental inequality analysis in a large German city applying generalized linear models. Int. J. Hyg. Environ. Health 2017, 220, 711–718. [Google Scholar] [CrossRef]
- Bundy, J.D.; Bazzano, L.A.; Xie, D.; Cohan, J.; Dolata, J.; Fink, J.C.; Hsu, C.-Y.; Jamerson, K.; Lash, J.; Makos, G.; et al. Self-reported tobacco, alcohol, and illicit drug use and progression of chronic kidney disease. Clin. J. Am. Soc. Nephrol. 2018, 13, 993–1001. [Google Scholar] [CrossRef]
- Twinamasiko, B.; Lukenge, E.; Nabawanga, S.; Nansalire, W.; Kobusingye, L.; Ruzaaza, G.; Bajunirwe, F. Sedentary lifestyle and hypertension in a periurban area of mbarara, South Western Uganda: A population based cross sectional survey. Int. J. Hypertens. 2018, 2018, 8253948. [Google Scholar] [CrossRef] [Green Version]
- Nepal, G.; Tuladhar, E.T.; Dahal, S.; Ahamad, S.T.; Adhikari, S.; Kandel, A. Lifestyle Practices and Obesity in Nepalese Youth: A Cross-sectional Study. Cureus 2018, 10, e2209. [Google Scholar] [CrossRef] [Green Version]
- WHO Regional Office for Europe. Urban Green Spaces and Health—A Review of Evidence; WHO: Geneva, Switzerland, 2016.
- Adger, W.N. Social vulnerability to climate change and extremes in coastal Vietnam. World Dev. 1999, 27, 249–269. [Google Scholar] [CrossRef]
- Messer, L.C.; Jagai, J.S.; Rappazzo, K.M.; Lobdell, D.T. Construction of an environmental quality index for public health research. Environ. Health 2014, 13, 39. [Google Scholar] [CrossRef] [Green Version]
- Doiron, D.; Setton, E.M.; Shairsingh, K.; Brauer, M.; Hystad, P.; Ross, N.A.; Brook, J.R. Healthy built environment: Spatial patterns and relationships of multiple exposures and deprivation in Toronto, Montreal and Vancouver. Environ. Int. 2020, 143, 106003. [Google Scholar] [CrossRef] [PubMed]
- Pineo, H.; Zimmermann, N.; Cosgrave, E.; Aldridge, R.W.; Acuto, M.; Rutter, H. Promoting a healthy cities agenda through indicators: Development of a global urban environment and health index. Cities Health 2018, 2, 27–45. [Google Scholar] [CrossRef] [Green Version]
- Pearson, A.L.; Pearce, J.; Kingham, S. Deprived yet healthy: Neighbourhood-level resilience in New Zealand. Soc. Sci. Med. 2013, 91, 238–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Estoque, R.C.; Murayama, Y. Social–ecological status index: A preliminary study of its structural composition and application. Ecol. Indic. 2014, 43, 183–194. [Google Scholar] [CrossRef]
- Liu, C.; Fuertes, E.; Tiesler, C.M.; Birk, M.; Babisch, W.; Bauer, C.P.; Koletzko, S.; von Berg, A.; Hoffman, B.; Heinrich, J.; et al. The associations between traffic-related air pollution and noise with blood pressure in children: Results from the GINIplus and LISAplus studies. Int. J. Hyg. Environ. Health 2014, 217, 499–505. [Google Scholar] [CrossRef]
- Riedel, N.; Köckler, H.; Scheiner, J.; Berger, K. Objective exposure to road traffic noise, noise annoyance and self-rated poor health—Framing the relationship between noise and health as a matter of multiple stressors and resources in urban neighbourhoods. J. Environ. Plan. Manag. 2014, 58, 336–356. [Google Scholar] [CrossRef]
- Gascon, M.; Zijlema, W.; Vert, C.; White, M.P.; Nieuwenhuijsen, M.J. Outdoor blue spaces, human health and well-being: A systematic review of quantitative studies. Int. J. Hyg. Environ. Health 2017, 220, 1207–1221. [Google Scholar] [CrossRef]
- White, M.P.; Elliott, L.R.; Gascon, M.; Roberts, B.; Fleming, L.E. Blue space, health and well-being: A narrative overview and synthesis of potential benefits. Environ. Res. 2020, 191, 110169. [Google Scholar] [CrossRef]
- Levallois, P.; Barn, P.; Valcke, M.; Gauvin, D.; Kosatsky, T. Public Health Consequences of Lead in Drinking Water. Curr. Environ. Health Rep. 2018, 5, 255–262. [Google Scholar] [CrossRef]
- Taylor, D.L.; Kahawita, T.M.; Cairncross, S.; Ensink, J.H.J. The impact of water, sanitation and hygiene interventions to control cholera: A systematic review. PLoS ONE 2015, 10, e0135676. [Google Scholar] [CrossRef] [Green Version]
- Klompmaker, J.O.; Hoek, G.; Bloemsma, L.D.; Gehring, U.; Strak, M.; Wijga, A.H.; van de Brink, C.; Brunekreef, B.; Lebert, E.; Janssen, N.A.H. Green space definition affects associations of green space with overweight and physical activity. Environ. Res. 2018, 160, 531–540. [Google Scholar] [CrossRef] [PubMed]
- Jaakkola, J.J.K. Case-crossover design in air pollution epidemiology. Eur. Respir. J. 2003, 21, 81s–85s. [Google Scholar] [CrossRef] [PubMed]
- Crane, M.; Bohn-Goldbaum, E.; Grunseit, A.; Bauman, A. Using natural experiments to improve public health evidence: A review of context and utility for obesity prevention. Health Res. Policy Syst. 2020, 18, 48. [Google Scholar] [CrossRef] [PubMed]
- Vardoulakis, S.; Dimitroulopoulou, S.; Mitsakou, C.; Heaviside, C.; Katsouyanni, K.; Samoli, E.; Santana, P. Developing environmental public health indicators for European metropolitan areas. In Proceedings of the International Conference on Urban Risks, Lisboa, Portugal, 30 June–2 July 2016. [Google Scholar]
- Lobdell, D.T.; Jagai, J.S.; Rappazzo, K.; Messer, L.C. Data Sources for an Environmental Quality Index: Availability, Quality, and Utility. Am. J. Public Health 2011, 101, S277–S285. [Google Scholar] [CrossRef]
- Weigand, M.; Wurm, M.; Dech, S.; Taubenböck, H. Remote sensing in environmental justice research-a review. ISPRS Int. J. Geo-Inf. 2019, 8, 20. [Google Scholar] [CrossRef] [Green Version]
- Lai, S.; Erbach-Schoenberg, E.Z.; Pezzulo, C.; Ruktanonchai, N.W.; Sorichetta, A.; Steele, J.; Li, T.; Dooley, C.A.; Tatem, A.J. Exploring the use of mobile phone data for national migration statistics. Palgrave Commun. 2019, 5, 34. [Google Scholar] [CrossRef] [Green Version]
- Gruebner, O.; Sykora, M.; Lowe, S.R.; Shankardass, K.; Galea, S.; Subramanian, S.V. Big data opportunities for social behavioral and mental health research. Soc. Sci. Med. 2017, 189, 167–169. [Google Scholar] [CrossRef] [Green Version]
- Stirnberg, R.; Cermak, J.; Fuchs, J.; Andersen, H. Mapping and Understanding Patterns of Air Quality Using Satellite Data and Machine Learning. J. Geophys. Res. Atmos. 2020, 125, e2019JD031380. [Google Scholar] [CrossRef]
- Chen, G.; Li, S.; Knibbs, L.D.; Hamm, N.A.; Cao, W.; Li, T.; Guo, Y. A machine learning method to estimate PM2.5 concentrations across China with remote sensing, meteorological and land use information. Sci. Total Environ. 2018, 636, 52–60. [Google Scholar] [CrossRef]
- Li, T.; Shen, H.; Yuan, Q.; Zhang, X.; Zhang, L. Estimating Ground-Level PM2.5 by Fusing Satellite and Station Observations: A Geo-Intelligent Deep Learning Approach. Geophys. Res. Lett. 2017, 44, 11985–11993. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Zhang, H.; Chao, C.Y.; Chien, C.H.; Wu, C.Y.; Luo, C.H.; Chen, L.-J.; Biswas, P. Integrating low-cost air quality sensor networks with fixed and satellite monitoring systems to study ground-level PM2.5. Atmos. Environ. 2020, 223, 117293. [Google Scholar] [CrossRef]
- Yang, J.; Sun, J.; Ge, Q.; Li, X. Assessing the impacts of urbanization-associated green space on urban land surface temperature: A case study of Dalian, China. Urban For. Urban Green. 2017, 22, 1–10. [Google Scholar] [CrossRef]
- Banzhaf, E.; Grescho, V.; Kindler, A. Monitoring urban to peri-urban development with integrated remote sensing and GIS information: A Leipzig, Germany case study. Int. J. Remote Sens. 2009, 30, 1675–1696. [Google Scholar] [CrossRef]
- Taubenböck, H.; Esch, T.; Felbier, A.; Wiesner, M.; Roth, A.; Dech, S. Monitoring urbanization in mega cities from space. Remote Sens. Environ. 2012, 117, 162–176. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1970–2000 | 2001–2010 | 2011–2020 | |||
|---|---|---|---|---|---|
| Country | Number of Publications | Country | Number of Publications | Country | Number of Publications |
| United States of America | 192 | United States of America | 1327 | United States of America | 5478 |
| United Kingdom | 87 | United Kingdom | 368 | United Kingdom | 2466 |
| Canada | 31 | Canada | 236 | Canada | 828 |
| Australia | 12 | Australia | 138 | Australia | 731 |
| Sweden | 11 | Netherlands | 73 | People’s Republic of China | 527 |
| Netherlands | 10 | Sweden | 63 | Netherlands | 279 |
| South Africa | 9 | Germany | 49 | Germany | 251 |
| France | 6 | France | 41 | France | 248 |
| Brazil | 5 | New Zealand | 38 | Spain | 243 |
| Denmark | 5 | Spain | 38 | Brazil | 235 |
| Main Topic and Subtopic | Number of Publications | % |
|---|---|---|
| Environmental Hazards and Benefits | 3039 | 24.7 |
| air pollution | 894 | 7.3 |
| built environment | 617 | 5.0 |
| green space | 380 | 3.1 |
| climate change | 380 | 3.1 |
| water | 175 | 1.4 |
| transportation | 174 | 1.4 |
| waste | 78 | 0.6 |
| housing | 68 | 0.6 |
| natural environment | 65 | 0.5 |
| noise | 64 | 0.5 |
| biodiversity | 61 | 0.5 |
| heat | 58 | 0.5 |
| land-use | 25 | 0.2 |
| Social Context | 1787 | 14.5 |
| social capital | 837 | 6.8 |
| healthcare | 208 | 1.7 |
| Participation | 198 | 1.6 |
| residential segregation | 193 | 1.6 |
| crime | 185 | 1.5 |
| violence | 122 | 1.0 |
| food environment | 91 | 0.7 |
| psychosocial environment | 51 | 0.4 |
| Individual vulnerability | 7313 | 59.4 |
| socioeconomic status | 1218 | 9.9 |
| income | 828 | 6.7 |
| race | 825 | 6.7 |
| gender | 448 | 3.6 |
| education | 380 | 3.1 |
| ethnicity | 276 | 2.2 |
| age | 193 | 1.6 |
| minority | 155 | 1.3 |
| immigration | 142 | 1.2 |
| employment | 105 | 0.9 |
| deprivation | 88 | 0.7 |
| occupation | 62 | 0.5 |
| behaviors | 423 | 3.4 |
| lifestyle | 399 | 3.2 |
| genetics | 214 | 1.7 |
| stress | 192 | 1.6 |
| nutrition | 161 | 1.3 |
| diet | 158 | 1.3 |
| availability | 221 | 1.8 |
| mobility | 68 | 0.6 |
| Health outcome | 4669 | 37.9 |
| mortality | 1238 | 10.0 |
| obesity | 836 | 6.8 |
| mental health | 648 | 5.3 |
| asthma | 281 | 2.3 |
| self-rated health | 267 | 2.2 |
| cancer | 194 | 1.6 |
| hiv | 190 | 1.5 |
| cardiovascular-disease | 188 | 1.5 |
| pregnancy | 171 | 1.4 |
| blood-pressure | 162 | 1.3 |
| infant-mortality | 113 | 0.9 |
| birth | 113 | 0.9 |
| breast cancer | 88 | 0.7 |
| chronic disease | 61 | 0.5 |
| injury | 61 | 0.5 |
| psychological distress | 58 | 0.5 |
| Actions | 1073 | 8.7 |
| interventions | 437 | 3.5 |
| risk assessment | 144 | 1.2 |
| health policy | 100 | 0.8 |
| urban planning | 67 | 0.5 |
| Index | 58 | 0.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhuang, S.; Bolte, G.; Lakes, T. Exploring Environmental Health Inequalities: A Scientometric Analysis of Global Research Trends (1970–2020). Int. J. Environ. Res. Public Health 2022, 19, 7394. https://doi.org/10.3390/ijerph19127394
Zhuang S, Bolte G, Lakes T. Exploring Environmental Health Inequalities: A Scientometric Analysis of Global Research Trends (1970–2020). International Journal of Environmental Research and Public Health. 2022; 19(12):7394. https://doi.org/10.3390/ijerph19127394
Chicago/Turabian StyleZhuang, Sida, Gabriele Bolte, and Tobia Lakes. 2022. "Exploring Environmental Health Inequalities: A Scientometric Analysis of Global Research Trends (1970–2020)" International Journal of Environmental Research and Public Health 19, no. 12: 7394. https://doi.org/10.3390/ijerph19127394