1. Introduction
During the last two years of the COVID-19 pandemic, domestic violence crimes against women and children have increased. This increase is linked to both isolation stress and children in the home due to school closures [
1,
2,
3,
4,
5,
6]. Moreover, Mamun and colleagues highlighted how economic distress and fear of being infected are considered risk factors for the infanticide–suicide phenomenon [
7].
According to the National Centre for Injury Prevention and Control, infanticide is the fifth leading cause of death for children under the age of five. Nine times out of ten, it is the mother who kills her child(ren) [
8].
The United Nations Office on Drugs and Crime (UNODC) [
9] estimated that during the ten-year period 2008–2017, a total of 205,153 children aged 0 to 14 years lost their lives worldwide (41 countries included) as a result of homicide. In Italy, 447 children were murdered by their parents during the period 2000–2017 [
10].
The literature review showed that most studies report that filicides occur predominantly by the fourth month of a child’s life, and the characteristics of homicidal mothers include young age, low education level, having more than one child, low socioeconomic status, and not having adequate prenatal care knowledge. Relationships with partners and biological fathers are often unstable, dysfunctional, and violent. Most of these women do not experience adequate support systems. The co-occurrence of these factors among young mothers can lead to unpreparedness for the increasing emotional, material, and financial care required by a newborn child [
11].
Regarding risk factors, some studies agree that filicide is primarily linked to psychosocial stress [
12,
13,
14,
15]. For example, trauma, substance abuse [
16], precarious financial conditions, relationships marked by discord and violence, a history of childhood abuse, and parental separation are recurrent factors in women who kill their children. Other studies have highlighted the relationship between filicide and society’s unrealistic expectations of motherhood [
17]. In one study [
18], it was found that 72% of the women who had committed filicide had no specific diagnosis of a mental disorder before the crime. Only four out of 96 women presented with a diagnosis of post-partum depression [
11]. Aggressive thoughts and—in some cases—even homicidal ideation towards their children are also found among women in the general population [
19]. This especially occurs in cases of intestinal colic and inconsolable crying, where the aim is silencing their baby, even in violent ways [
20]. The period between birth and the first year of a child’s life represents a unique moment of biological change that can cause a psychological disturbance. Fifty to eighty percent of women develop the ‘baby blues’ within 4–5 days post-delivery [
21]. Symptoms of such conditions include anxiety, unmotivated crying, impatience, irritability, lack of self-confidence, and restlessness [
22].
Filicide is highly correlated with postpartum psychosis (PP), which has an incidence of approximately 1–4 cases per 1000 births. However, PP may not be detected by professionals because the symptoms are intermittent, and some women tend to hide them to not disappoint their families [
23]. These symptoms are often associated with suicidal ideation, which can take the form of suicide/filicide situations. Personality disorders are also highly correlated with violent crimes: many filicidal mothers have had negative and traumatic experiences in childhood and adolescence, which has impacted their personality development. Anxiety and dependency traits and low self-esteem were particularly observed. These results indicate a complex picture involving social, relational, emotional, and personality aspects.
Recidivism risk assessment is fundamental in cases of maternal filicide, especially when the mother has other children. Structured interviews can be an important source of data both to formulate a diagnosis of mental pathology and to contextualise the event as much as possible [
11]. In Anglo-Saxon countries, the use of scientific tools is customary in many areas—for example, during the eligibility assessment for parole and probation, in psychiatric and forensic hospitals, prisons, courts, and to manage treatment programmes.
For years, forensic psychology research has been concerned with demonstrating the reliability and predictive validity of violence risk assessment tools [
24,
25,
26,
27,
28,
29,
30]. Currently, there are more than 200 violence risk assessment tools with a wide range of applications and varying levels of accuracy [
31,
32].
In 34 USA states, even the use of validated assessment tools is mandatory for the risk assessment of youth probationers [
33,
34]. They help professionals assess, manage, and reduce recidivism risk. Risk assessment tools assume even more relevance in adolescents and young adults because of the impact that evaluations and programmes can have on their development.
In Italy, evaluations are carried out by professionals appointed by judges. Although several authors have proposed standardised evaluation models—considering individual, social, and environmental characteristics linked to two macro-categories of indicators (internal and external) [
24,
35]—the choice of tools to be used is still discretionary. A purely clinical approach leads to subjective and non-generalisable evaluations, conditioned by professional experience. Therefore, the likelihood of predicting the risk of violence or criminal behaviours decreases significantly. In this way, the predictive accuracy of the assessments demonstrated by previous research is no better than chance (see, for example, [
24,
25]).
The use of standardised tools is also functional to the risk management process, which allows one to identify and monitor the most useful treatment for the offender and to effectively contribute to the prevention and reduction of violence and other forms of reoffending. In addition, the use of such tools promotes greater adherence by professionals to the risk-need-responsivity model (RNR) [
36,
37,
38]. This model comes from the general personality and cognitive social learning theory of criminal conduct [
38], and it is currently considered the leading assessment and treatment model for offenders. Based on the RNR model, the Level of Service (LS) instruments allow one to assess the offenders’ recidivism risk considering static risk factors, criminogenic needs, responsiveness factors, as well as their strengths.
There is an ongoing debate about the sensitivity of violence risk assessment tools for female populations. Their effectiveness is relevant because of the impact of violent behaviours on their children [
39]. According to Bonta and Andrews [
38], risk assessment tools that allow both assessment and case management are the most suitable. De Vogel and colleagues [
40] found that the Level of Supervision Inventory (LSI) [
41] is the most effective tool for assessing general and violent recidivism in both men and women. Other studies demonstrated the predictive validity of both Historical Clinical Risk-20 (HCR-20) [
42] and Level of Service/Case Management Inventory (LS/CMI) [
43] among adult offenders and Youth Level of Service/Case Management Inventory (YLS/CMI) [
44] and Structured Assessment of Violence Risk in Youth (SAVRY) [
45] among juvenile offenders [
46,
47,
48].
Despite these results, in the forensic field, the most widely used standardised assessment instruments are the Minnesota Multiphasic Personality Inventory (MMPI) [
49] and the Rorschach [
50]. They are used in 96% and 36% of cases, respectively, against 11% associated with the use of the Psychopathy Checklist-Revised (PCL-R) [
51] and 1% of the Violence Risk Appraisal Guide (VRAG) [
52,
53,
54]. MMPI and Rorschach provide useful elements for evaluation, but they do not allow for an objective prediction of violent behaviours.
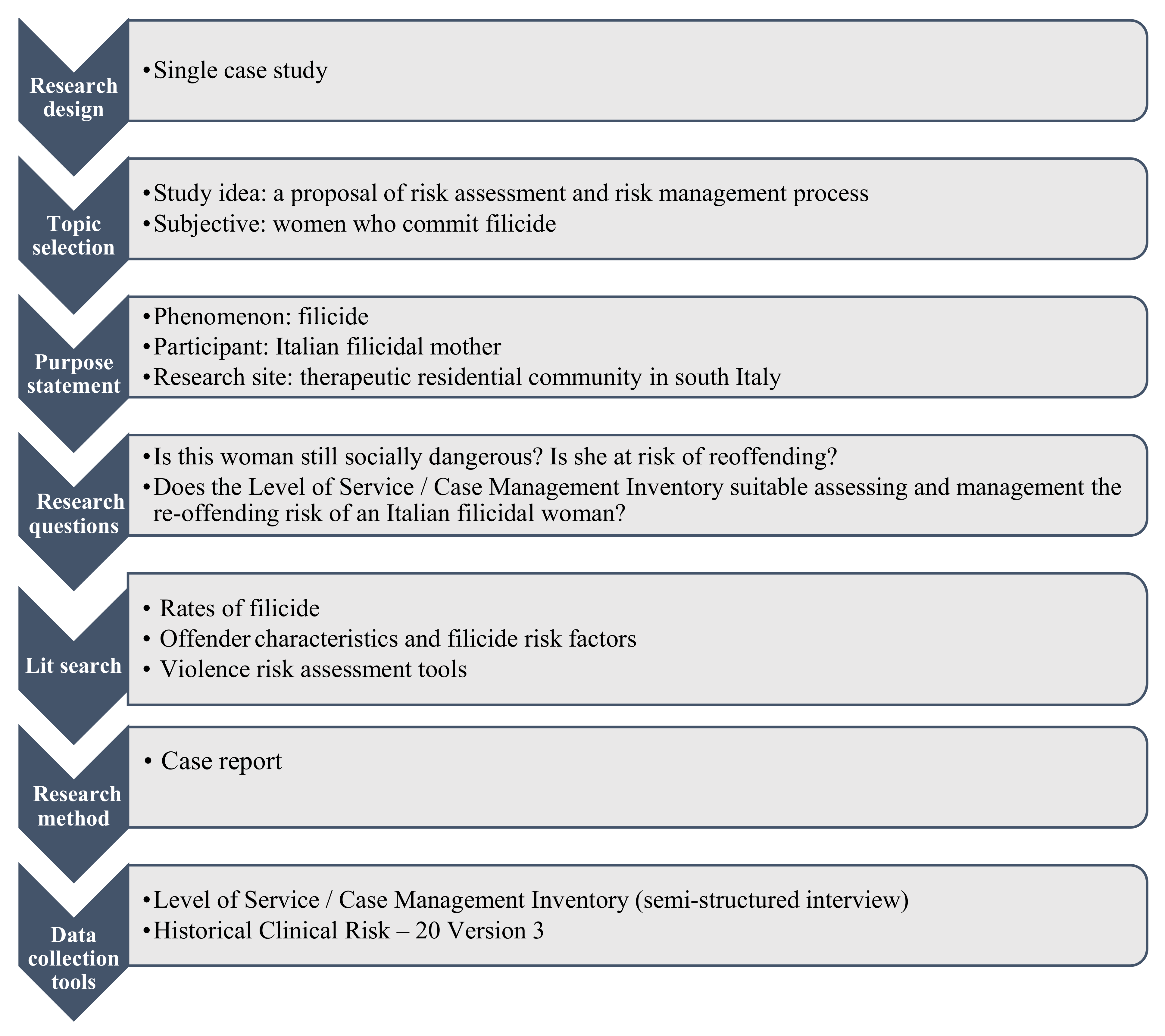
This research is part of a larger study on the Italian adaptation of the LS/CMI tool. The aim of the present study (see
Figure A1) is to assess the re-offending risk of an Italian woman perpetrator of filicide, to give an example of a violence risk assessment procedure based on the use of a risk assessment tool already used worldwide evaluating its suitability in the Italian context.
The objective risk assessment and current social dangerousness of this single case, using the LS/CMI and the HCR-20 V3 instruments, will be useful for the identification and management of social reintegration programmes that respect women’s needs. Moreover, this study represents a first step towards adapting the national evaluation processes to the international panorama in the field of forensic psychology.
4. Discussion
The aim of the present study was to assess the current recidivism risk and social dangerousness of an Italian filicidal woman to provide an example of a violence risk assessment procedure based on the use of LS/CMI tool while evaluating its suitability in the Italian context.
As demonstrated by previous research, when filicide occurs, assessment of recidivism risk becomes even more important, especially when the offender has other children. Structured interviews with offenders can be an important source of information. Considering the primary role of social stressors influencing the filicide phenomenon [
11], structured interviews help guide professionals through the contextualisation of the event.
Although other researchers analysed the cases of filicidal mothers [
59,
60,
61], few studies have focused on other aspects besides psychiatric issues. For example, Ben Ammar and colleagues [
62] used the same research design as our study to analyse the association between Delusional misidentification syndromes (DMS) and the murder of a child by his mother. In an Italian study, Giacchetti and colleagues focused on personality traits in a sample of filicidal mothers, while other researchers focused on prevention measures [
63].
In this study, data collected through LS/CMI and HCR-20 V3 revealed a range of information about different life areas that had not been underlined in the documentary survey. Knowing such information is useful both to define the persistence of offenders’ social dangers and to plan the offenders’ psychosocial rehabilitation programme. Although from the second year of Anna’s probation, the information about her condition increases, ambiguities, and inconsistencies between them increase as well. This is probably due to the different professionals who have dealt with this single case over the past 11 years. Ambiguities and inconsistencies are particularly evident in the determination of Anna’s psychopathological diagnosis.
We reported (see
Box A1) that the diagnoses formulated during the Security Measure by different professionals both through the DSM-IV TR [
64] and the DSM-5 [
65] varied from schizoaffective disorder depressive type in a subject with borderline personality disorder to depressive disorder with psychotic symptoms to, finally, depressive disorder with post-partum onset specifier. However, it is well known that the diagnostic process operated through the DSM does not allow the above-mentioned diagnoses to be made simultaneously. This inconsistency hinders the objective process of Anna’s social dangerousness assessment so far based on the incurability of the disorder from which she suffers. In the context of this single case—since there is not even an unequivocal opinion as to the real disorder that Anna suffers from and the relative and potential prognosis—how can she be defined as incurable and then base the assessment of recidivism risk mainly on these prognoses?
As several authors argue [
11,
66], the hypothesis that Anna was affected peripartum by major depressive disorder with psychotic symptoms is well-suited to the situational picture presented. Taking this into account, the psychosocial rehabilitation programme of the offender deserves to be reviewed. The symptom compensation should be attributed not only to the psychopharmacological treatment but also to her containment in the therapeutic residential community. Rather, it could be traced back to stressful psychosocial factors, which gradually resolved and, consequently, contributed to the remission of her disorder [
66,
67,
68].
Although the recidivism risk level cannot only be defined on the psychopathological condition of the offender, here, it is strongly relied upon to assert the persistence of social dangerousness. It seems like a diagnostic label was being used to fill the need for control.
This situation leads to a sort of endless security measure because, if the psychopathology is incurable—and containable through psychopharmacological treatment and therapeutic community containment—periodically checking the rehabilitation progress results is unnecessary. Continuing to restrict her autonomy hinders the achievement of a better balance between criminogenic needs and strengths and, therefore, her effective social reintegration.
It is more appropriate to consider possible relapses that may be prevented and managed when in the presence of strength elements, identified using scientifically validated assessment tools [
66,
67,
68,
69]. As shown by the results of this study, the use of LS/CMI seems to be appropriate for achieving this aim. It allows the assessment of standardised life areas, orienting the risk assessment process in a more reliable direction. Moreover, standardised tools facilitate communication between different professionals involved in the process, thus decreasing ambiguities due to autonomous practices. The discretionary nature of the assessment and the lack of specific tools could lead to a delay in the gradual acquisition of the autonomy level desired by the subject. In addition, the use of scientifically validated tools allows the rehabilitation programme to be planned in a way that is most useful for the user’s condition and to monitor improvements over time.
As specified by the risk principle of the Risk-Need-Responsivity model (RNR) [
70], recovery, and social reintegration programmes should be calibrated according to the risk level of the individual. Intensive programmes should only target those who are at a moderate–high level, excluding those at a lower risk level, as it reduces contact with higher-risk offenders in criminal justice settings. The responsivity principle of the model also states that programmes should aim to maximise the competencies of the subjects and adapt to their learning style, degree of motivation and abilities.
In this single case, the LS/CMI showed that some sub-components could still represent a criminogenic need for her. To prevent anti-social behaviour, it would be necessary to take these data into account for more accurate planning of the subsequent phases of the psychosocial rehabilitation programme. Concerning family relations, it would be useful to promote a link between Anna’s services and that of her husband to preserve the supporting role that he provides over time and prevent it from becoming a risk factor for her.
Traumatic experiences lived within the family should be considered and consciously placed in Anna’s life story as part of a therapeutic process. The processing of traumatic experiences could take place in a peer support group in which Anna’s connection network can be expanded. In order to fill the lack of satisfaction and to gratify her work commitment, it would be appropriate to encourage Anna’s participation in other recreational activities—outside the community—more inclined to her interests. In this way, it would be possible to increase her motivation level and make these activities an external link and support for her.
Parallel to the criminogenic needs, LS/CMI highlighted Anna’s strengths: the absence of a pro-criminal attitude and an antisocial pattern, as well as her work commitment. We suggest leveraging this last aspect to keep her engaged and prevent possible clinical relapses. It could also be possible to increase the number of working hours or to propose a second job (the first one is a part-time job) more in line with her abilities and from which she can get greater satisfaction.
Actuarial tools do not allow for the identification of the strengths and weaknesses of the individual, which are useful for the development of treatment programmes suitable for reducing the risk of recidivism [
43,
70]. As demonstrated by this single case study, a violence risk assessment and risk management process guided by scientifically validated tools provides psycho-social data, which are fundamental to consider for prognosis, but which can be missed if professionals continue to use a purely clinical approach. Moreover, through the current study, we contributed to the adaptation of the Italian context to an international audience.
Future studies in this field should confirm the usefulness of this methodology and tools to systematise risk assessment and the risk management process and make it homogenous across countries.
The present study is not without some limitations. First, of the two instruments used in the evaluation activity, only the Italian validation study of HCR-20 V3 is currently available. Regarding LS/CMI, even though numerous studies have already demonstrated its effectiveness and reliability, the Italian validation is still in progress. This study is therefore the first exploratory contribution. Here, the HCR-20 V3 represented a support tool for the evaluation carried out using the Italian version of LS/CMI. The latter proved to have the application potential to solve the criticalities associated with complex clinical pictures, such as the one presented.
Second, it is well known that the most widely recognised limitation of single case studies concerns external validity. However, many researchers have stressed that this type of research best enhances the richness of clinical work with patients, without neglecting methodological aspects. If it is true that single cases are unique by their nature, it is also true that they always contain aspects that can be replicated [
71]. The replicability of the study can be seen in the structure of the interview (e.g., LS/CMI- interview guide), which allows the same information to be collected for each administration. In this way, it is possible to obtain a standard assessment process for all the subjects examined. In fact, for the LS/CMI’s authors, the objective of well delineating the subject’s condition to support the prognostic judgement is fundamental.
5. Conclusions
In this work, we underlined how the LS/CMI assessment tool is useful in assessing the risk of reoffending and social dangerousness, and in identifying and managing social rehabilitation programmes.
As highlighted in the results, LS/CMI guides the interviewer through the exploration of eight areas of life considered risk factors and criminogenic needs for the offender. In this way, in addition to an overall recidivism risk score, we have been able to identify which areas need to be strengthened and which ones can be leveraged to make the social reintegration programme more effective. Despite the differences between the Canadian and Italian judicial systems, the tool has proved to be suitable in our context and useful for the evaluation of the participant.
From this single case emerged that although the evaluation carried out by HCR-20 V3 (which is a specific violence risk assessment tool already validated in Italy) provides useful information related to the risk of future violence, it is less detailed than LS/CMI collecting information about different life domains that can positively and negatively influence the social reintegration programme. Moreover—unlike HCR-20 V3—LS/CMI is provided as an interview guide. The possibility of using an interview guide adds more confidence to the interviewer and can make the evaluation faster.
Therefore, assessments guided by tools such as LS/CMI are even more valuable in emergencies—e.g., the last two years of the COVID-19 pandemic—where evaluations need to be carried out rapidly because rapid action needs to be taken in response to these assessments.





{kind=link}