
Analgesic Effects of Continuous Wound Infusion Combined with Intravenous Patient-Controlled Analgesia for Thoracic Surgery: A Retrospective Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Statement
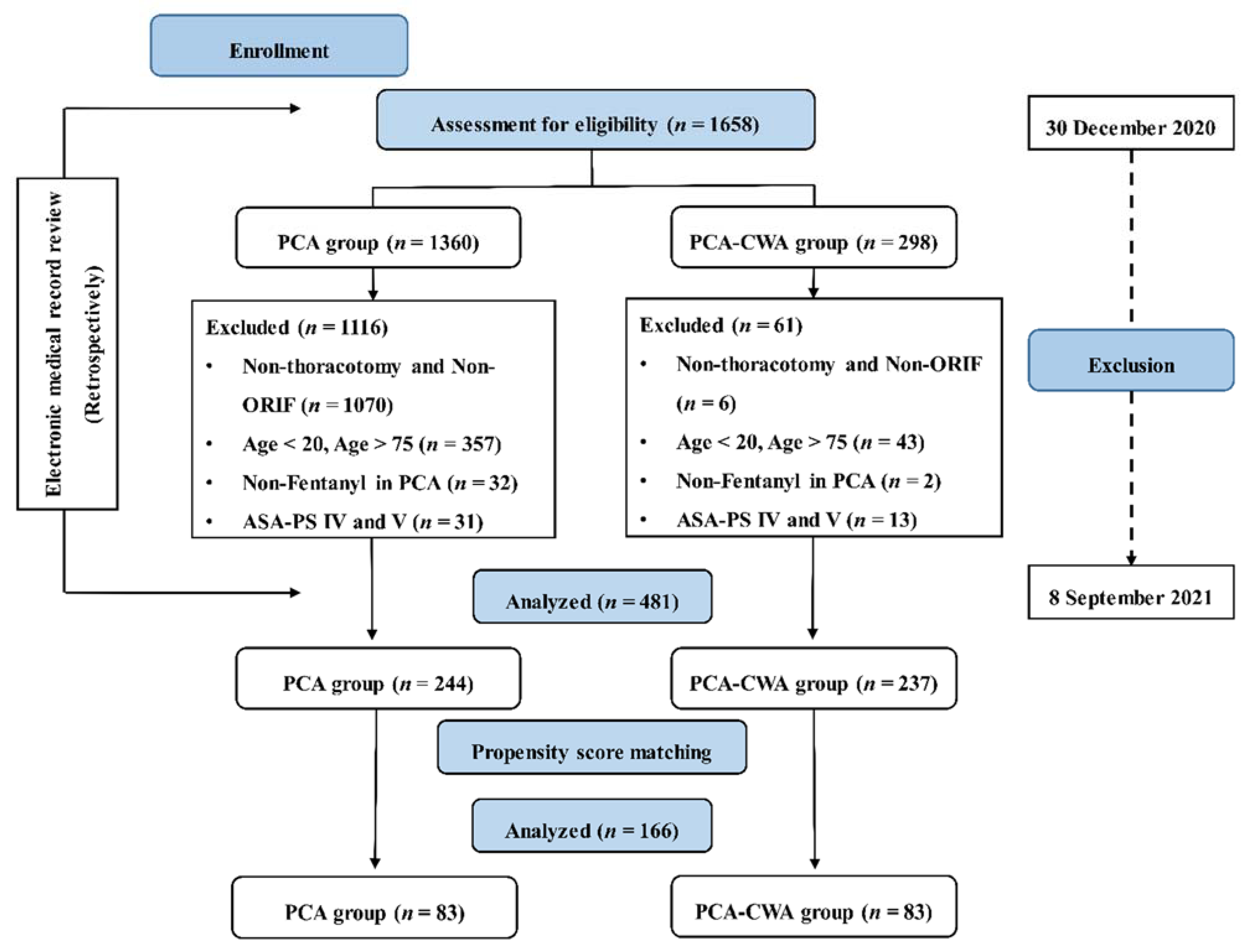
2.2. Selection of the Study Population
2.3. Interventions
2.3.1. PCA
2.3.2. CWA
2.4. Outcomes
2.5. Analysis
3. Results
3.1. Demographic and Clinical Data
3.2. Postoperative Analgesia Modalities
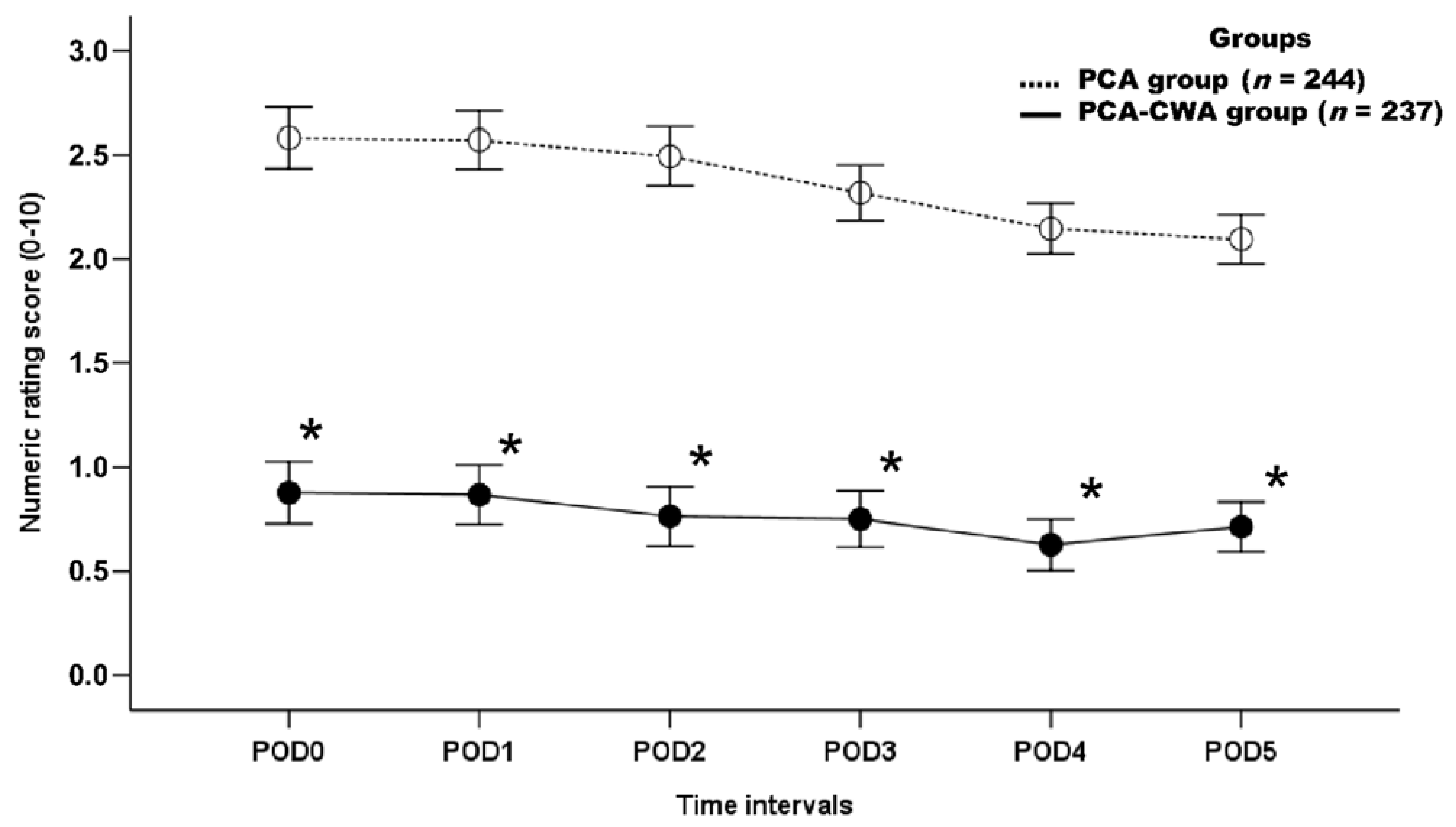
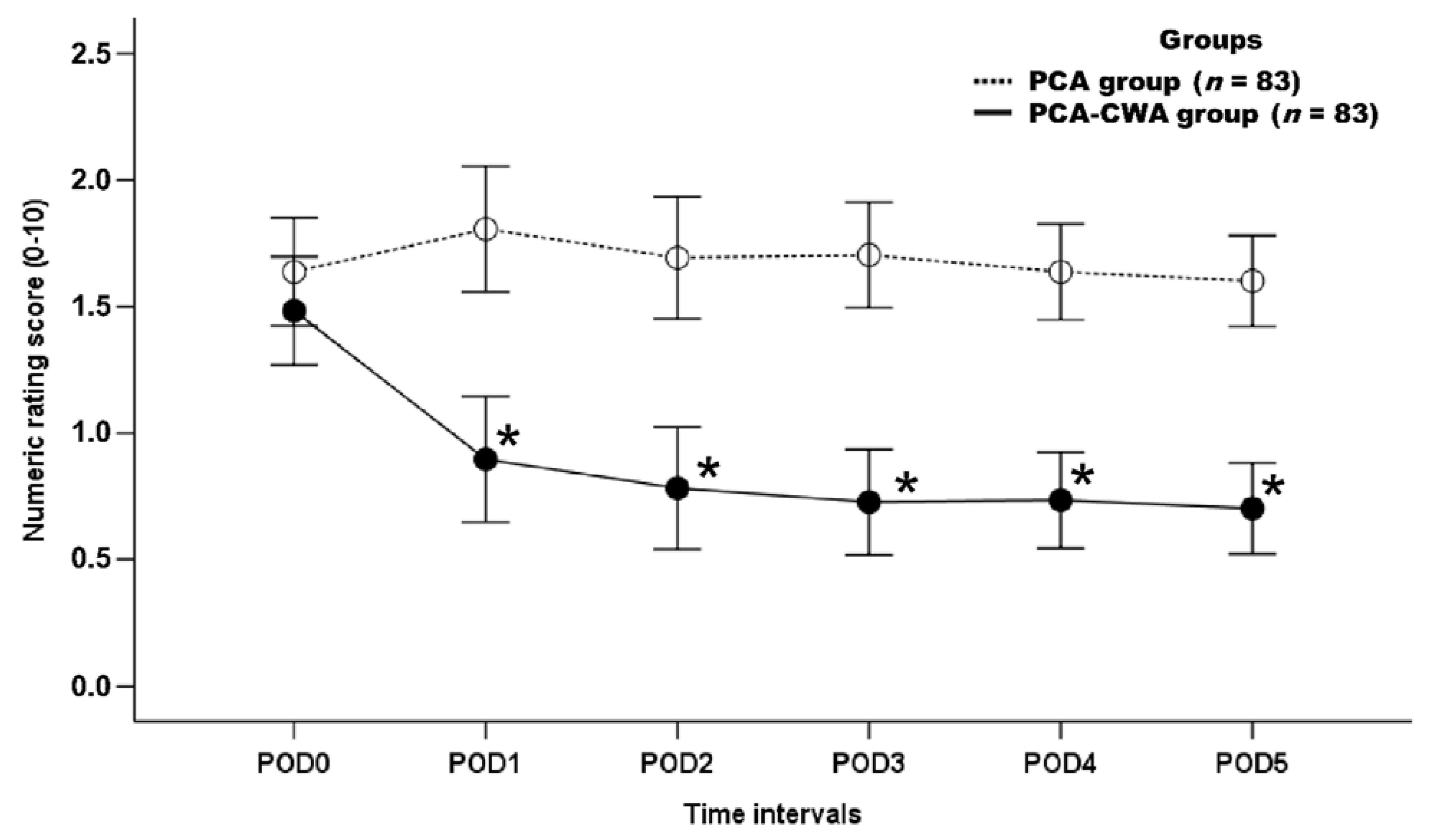
3.3. Postoperative Analgesic Effect
3.4. Postoperative Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lederman, D.; Easwar, J.; Feldman, J.; Shapiro, V. Anesthetic considerations for lung resection: Preoperative assessment, intraoperative challenges and postoperative analgesia. Ann. Transl. Med. 2019, 7, 356. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.F.; Liu, X.M.; Liu, X.Y.; Tang, J.; Jin, L.; Li, W.Y.; Zhang, L.D. Postoperative continuous wound infusion of ropivacaine has comparable analgesic effects and fewer complications as compared to traditional patient-controlled analgesia with sufentanil in patients undergoing non-cardiac thoracotomy. Int. J. Clin. Exp. Med. 2015, 8, 5438–5445. [Google Scholar]
- Alzahrani, T. Pain relief following thoracic surgical procedures: A literature review of the uncommon techniques. Saudi J. Anaesth. 2017, 11, 327–331. [Google Scholar] [CrossRef] [PubMed]
- D’Ercole, F.; Arora, H.; Kumar, P.A. Paravertebral Block for Thoracic Surgery. J. Cardiothorac. Vasc. Anesth. 2018, 32, 915–927. [Google Scholar] [CrossRef] [PubMed]
- Raines, S.; Hedlund, C.; Franzon, M.; Lillieborg, S.; Kelleher, G.; Ahlén, K. Ropivacaine for continuous wound infusion for postoperative pain management: A systematic review and meta-analysis of randomized controlled trials. Eur. Surg. Res. 2014, 53, 43–60. [Google Scholar] [CrossRef] [PubMed]
- Ventham, N.T.; Hughes, M.; O’Neill, S.; Johns, N.; Brady, R.R.; Wigmore, S.J. Systematic review and meta-analysis of continuous local anaesthetic wound infiltration versus epidural analgesia for postoperative pain following abdominal surgery. Br. J. Surg. 2013, 100, 1280–1289. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.E.; Park, Y.J.; Lee, J.W. Ropivacaine continuous wound infusion after mastectomy with immediate autologous breast reconstruction: A retrospective observational study. Medicine 2021, 100, e26337. [Google Scholar] [CrossRef] [PubMed]
- Kone, L.B.; Kunda, N.M.; Tran, T.B.; Maker, A.V. Surgeon-Placed Continuous Wound Infusion Pain Catheters Markedly Decrease Narcotic Use and Improve Outcomes After Pancreatic Tumor Resection. Ann. Surg. Oncol. 2021, 28, 2287–2295. [Google Scholar] [CrossRef] [PubMed]
- Thangavel, A.R.; Sethi, S.; Gupta, V. Comparison of Continuous Wound Infusion versus Continuous Epidural Infusion in Upper Abdominal Surgery: Noninferiority Randomized Controlled Trial. Anesth. Essays Res. 2019, 13, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Liang, S.S.; Ying, A.J.; Affan, E.T.; Kakala, B.F.; Strippoli, G.F.; Bullingham, A.; Currow, H.; Dunn, D.W.; Yeh, Z.Y. Continuous local anaesthetic wound infusion for postoperative pain after midline laparotomy for colorectal resection in adults. Cochrane Database Syst. Rev. 2019, 10, CD012310. [Google Scholar] [CrossRef] [PubMed]
- Fusco, P.; Cofini, V.; Petrucci, E.; Scimia, P.; Fiorenzi, M.; Paladini, G.; Behr, A.U.; Borghi, B.; Flamini, S.; Pizzoferrato, R.; et al. Continuous wound infusion and local infiltration analgesia for postoperative pain and rehabilitation after total hip arthroplasty. Minerva Anestesiol. 2018, 84, 556–564. [Google Scholar] [CrossRef] [PubMed]
- Lenz, N.; Hirschburger, M.; Roehrig, R.; Menges, T.; Mueller, M.; Padberg, W.; Mann, V. Application of Continuous Wound-Infusion Catheters in Lung Transplantation: A Retrospective Data Analysis. Thorac. Cardiovasc. Surg. 2017, 65, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Fiorelli, A.; Izzo, A.C.; Frongillo, E.M.; Del Prete, A.; Liguori, G.; Di Costanzo, E.; Vicidomini, G.; Santini, M. Efficacy of wound analgesia for controlling post-thoracotomy pain: A randomized double-blind study. Eur. J. Cardiothorac. Surg. 2016, 49, 339–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gebhardt, R.; Mehran, R.J.; Soliz, J.; Cata, J.P.; Smallwood, A.K.; Feeley, T.W. Epidural versus ON-Q local anesthetic-infiltrating catheter for post-thoracotomy pain control. J. Cardiothorac. Vasc. Anesth. 2013, 27, 423–426. [Google Scholar] [CrossRef] [PubMed]
- Fortier, S.; Hanna, H.A.; Bernard, A.; Girard, C. Comparison between systemic analgesia, continuous wound catheter analgesia and continuous thoracic paravertebral block: A randomised, controlled trial of postthoracotomy pain management. Eur. J. Anaesthesiol. 2012, 29, 524–530. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.H.; Lee, C.K.; Kim, S.H.; Kim, Y.; Kim, J.E.; Shin, Y.K.; Seok, J.; Cho, H.M. Prevalence of chronic post-thoracotomy pain in patients with traumatic multiple rib fractures in South Korea: A cross-sectional study. Sci. Rep. 2021, 11, 2615. [Google Scholar] [CrossRef] [PubMed]
- Jung, K.T.; So, K.Y.; Kim, S.C.; Kim, S.H. Effect of Nefopam-Based Patient-Controlled Analgesia with and without Fentanyl on Postoperative Pain Intensity in Patients Following Laparoscopic Cholecystectomy: A Prospective, Randomized, Controlled, Double-Blind Non-Inferiority Trial. Medicina 2021, 57, 316. [Google Scholar] [CrossRef] [PubMed]
- Amour, J.; Cholley, B.; Ouattara, A.; Longrois, D.; Leprince, P.; Fellahi, J.L.; Riou, B.; Hariri, S.; Latremouille, C.; Remy, A.; et al. The effect of local anesthetic continuous wound infusion for the prevention of postoperative pneumonia after on-pump cardiac surgery with sternotomy: The STERNOCAT randomized clinical trial. Intensive Care Med. 2019, 45, 33–43. [Google Scholar] [CrossRef] [PubMed]
- El-Boghdadly, K.; Pawa, A.; Chin, K.J. Local anesthetic systemic toxicity: Current perspectives. Local Reg. Anesth. 2018, 11, 35–44. [Google Scholar] [CrossRef] [Green Version]
- Mattila, I.; Patila, T.; Rautiainen, P.; Korpela, R.; Nikander, S.; Puntila, J.; Salminen, J.; Suominen, P.K.; Tynkkynen, P.; Hiller, A. The effect of continuous wound infusion of ropivacaine on postoperative pain after median sternotomy and mediastinal drain in children. Paediatr. Anaesth. 2016, 26, 727–733. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| PCA Group (n = 244) | PCA-CWA Group (n = 237) | p-Value | |
|---|---|---|---|
| Age (year) | 57.2 (55.7–58.8) | 60.1 (58.7–61.5) | 0.008 * |
| Sex (male/female) | 188/56 (77/23) | 180/57 (75.9/24.1) | 0.776 |
| Weight (kg) | 64.1 (62.6–65.5) | 63.9 (62.4–65.4) | 0.866 |
| Height (cm) | 165.4 (164.3–166.6) | 165.4 (164.3–166.5) | 0.971 |
| BMI (kg/m2) | 23.3 (22.9–23.8) | 23.3 (22.8–23.7) | 0.868 |
| ASA-PS (I/II/III) | 49/142/53 (20.1/58.2/21.7) | 25/133/79 (10.5/56.1/33.3) | 0.001 * |
| Hypertension (yes) | 67 (27.5) | 84 (35.4) | 0.059 |
| Diabetic mellitus (yes) | 45 (18.4) | 54 (22.8) | 0.239 |
| Smoking (yes) | 78 (32) | 69 (29.1) | 0.497 |
| Duration of anesthesia (min) | 174.6 (165.2–184.1) | 183 (174.2–191.8) | 0.202 |
| Duration of operation (min) | 149.5 (140.3–158.6) | 157.7 (149–166.5) | 0.198 |
| Hospital stay (d) | 19.5 (17.9–21.1) | 21.7 (18.9–24.5) | 0.172 |
| Surgical procedures (ORIF/thoracotomy) | 119/125 (48.8/51.2) | 64/173 (27/73) | <0.001 * |
| PCA Group (n = 83) | PCA-CWA Group (n = 83) | p-Value | |
|---|---|---|---|
| Age (year) | 56.9 (54.1–59.7) | 58.1 (55.7–60.6) | 0.514 |
| Sex (male/female) | 59/24 (71.1/28.9) | 59/24 (71.1/28.9) | 1.000 |
| Weight (kg) | 63 (60.2–65.8) | 64.6 (62–67.3) | 0.406 |
| Height (cm) | 164.3 (161.8–166.7) | 166.1 (164.2–167.9) | 0.258 |
| BMI (kg/m2) | 23.2 (22.4–24.1) | 23.3 (22.6–24.1) | 0.804 |
| ASA-PS (I/II/III) | 8/53/22 (9.6/63.9/26.5) | 14/43/26 (16.9/51.8/31.3) | 0.222 |
| Hypertension (yes) | 26 (31.3) | 27 (32.5) | 0.868 |
| Diabetic mellitus (yes) | 16 (19.3) | 16 (19.3) | 1.000 |
| Smoking (yes) | 26 (31.3) | 22 (26.5) | 0.493 |
| Duration of anesthesia (min) | 181.5 (163.8–199.3) | 183.2 (170.1–196.3) | 0.879 |
| Duration of operation (min) | 160.3 (142.8–177.9) | 156.6 (143.5–169.6) | 0.734 |
| Hospital stay (d) | 21.8 (18.1–25.5) | 20.3 (17–23.6) | 0.547 |
| Surgical Procedures (ORIF/thoracotomy) | 44/39 (53/47) | 37/46 (44.6/55.4) | 0.277 |
| PCA Group (n = 244) | PCA-CWA Group (n = 237) | p-Value | |
|---|---|---|---|
| Fentanyl used for PCA | 244 (100) | 237 (100) | 1.000 |
| Doses (μg) | 1107 (1075.2–1138.8) | 944.7 (922–967.5) | <0.001 * |
| Adjuvant analgesics (nefopam/ketorolac/none) | 107/93/44 (43.9/38.1/18) | 228/4/5 (96.2/1.7/2.1) | <0.001 * |
| Dose (μg) | 526.6 (490.5–562.8) | 705.1 (685.3–724.8) | <0.001 * |
| Adjuvant antiemetics (ramosetron) | 244 (100) | 237 (100) | 1.000 |
| Dose (mg) | 0.9 (0.9–0.9) | 1.2 (1.2–1.2) | <0.001 * |
| PCA Group (n = 83) | PCA-CWA Group (n = 83) | p-Value | |
|---|---|---|---|
| Fentanyl used for PCA | 83 (100) | 83 (100) | 1.000 |
| Dose (μg) | 986.7 (935.2–1038.3) | 974.7 (936.7–1012.6) | 0.709 |
| Adjuvant analgesics (nefopam/ketorolac/none) | 71/2/10 (85.5/2.4/12) | 74/4/5 (89.2/4.8/6) | 0.302 |
| Dose (μg) † | 643.4 (584.4–702.4) | 691.6 (22.3–647.2) | 0.196 |
| Adjuvant antiemetics (ramosetron) | 83 (100) | 83 (100) | 1.000 |
| Dose (mg) | 1 (1–1.1) | 1.2 (1.2–1.2) | <0.001 * |
| PCA Group (n = 244) | PCA-CWA Group (n = 237) | p-Value | |
|---|---|---|---|
| PONV (yes) | 15 (6.1) | 10 (4.2) | 0.341 |
| Rescue analgesics (yes) | 114 (46.7) | 132 (55.7) | 0.049 * |
| Rescue antiemetics (yes) | 10 (4.1) | 12 (5.1) | 0.613 |
| Hypotension (yes) | 12 (4.9) | 4 (1.7) | 0.072 |
| Dizziness (yes) | 9 (3.7) | 4 (1.7) | 0.261 |
| Headache (yes) | 2 (0.8) | 0 (0) | 0.499 |
| Pruritus (yes) | 3 (1.2) | 2 (0.8) | 1.000 |
| Sedation (yes) | 28 (11.5) | 2 (0.8) | <0.001 * |
| Urinary retention (yes) | 47 (19.3) | 68 (28.7) | 0.015 * |
| Motor weakness (yes) | 0 (0) | 1 (0.4) | 0.493 |
| Respiratory difficulty (yes) | 7 (2.9) | 5 (2.1) | 0.772 |
| PCA stop (yes) | 29 (3.7) | 9 (3.8) | 0.950 |
| Persistent pain after 3 months postoperatively (yes) | 0 (0) | 2 (0.8) | 0.242 |
| Persistent pain after 6 months postoperatively (yes) | 0 (0) | 2 (0.8) | 0.242 |
| PCA Group (n = 83) | PCA-CWA Group (n = 83) | p-Value | |
|---|---|---|---|
| PONV (yes) | 4 (4.8) | 2 (1.2) | 0.682 |
| Rescue analgesics (yes) | 36 (43.4) | 38 (45.8) | 0.755 |
| Rescue antiemetics (yes) | 2 (2.4) | 4 (4.8) | 0.682 |
| Hypotension (yes) | 2 (2.4) | 1 (1.2) | 1.000 |
| Dizziness (yes) | 1 (1.2) | 0 (0) | 1.000 |
| Headache (yes) | 0 (0) | 0 (0) | 1.000 |
| Pruritus (yes) | 1 (1.2) | 0 (0) | 1.000 |
| Sedation (yes) | 8 (9.6) | 1 (1.2) | 0.034 * |
| Urinary retention (yes) | 18 (21.7) | 25 (30.1) | 0.215 |
| Motor weakness (yes) | 0 (0) | 0 (0) | 1.000 |
| Respiratory difficulty (yes) | 6 (7.2) | 1 (1.2) | 0.117 |
| PCA stop (yes) | 3 (3.6) | 5 (6) | 0.720 |
| Persistent pain after 3 months postoperatively (yes) | 0 (0) | 1 (1.2) | 1.000 |
| Persistent pain after 6 months postoperatively (yes) | 0 (0) | 1 (1.2) | 1.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jang, B.H.; So, K.Y.; Kim, S.H. Analgesic Effects of Continuous Wound Infusion Combined with Intravenous Patient-Controlled Analgesia for Thoracic Surgery: A Retrospective Study. Int. J. Environ. Res. Public Health 2022, 19, 6920. https://doi.org/10.3390/ijerph19116920
Jang BH, So KY, Kim SH. Analgesic Effects of Continuous Wound Infusion Combined with Intravenous Patient-Controlled Analgesia for Thoracic Surgery: A Retrospective Study. International Journal of Environmental Research and Public Health. 2022; 19(11):6920. https://doi.org/10.3390/ijerph19116920
Chicago/Turabian StyleJang, Bo Hyun, Keum Young So, and Sang Hun Kim. 2022. "Analgesic Effects of Continuous Wound Infusion Combined with Intravenous Patient-Controlled Analgesia for Thoracic Surgery: A Retrospective Study" International Journal of Environmental Research and Public Health 19, no. 11: 6920. https://doi.org/10.3390/ijerph19116920