
Effect of Physical Activity on Depression in Patients with Parkinson’s Disease: A Systematic Review and Meta-Analysis



Abstract
:1. Introduction
2. Methods
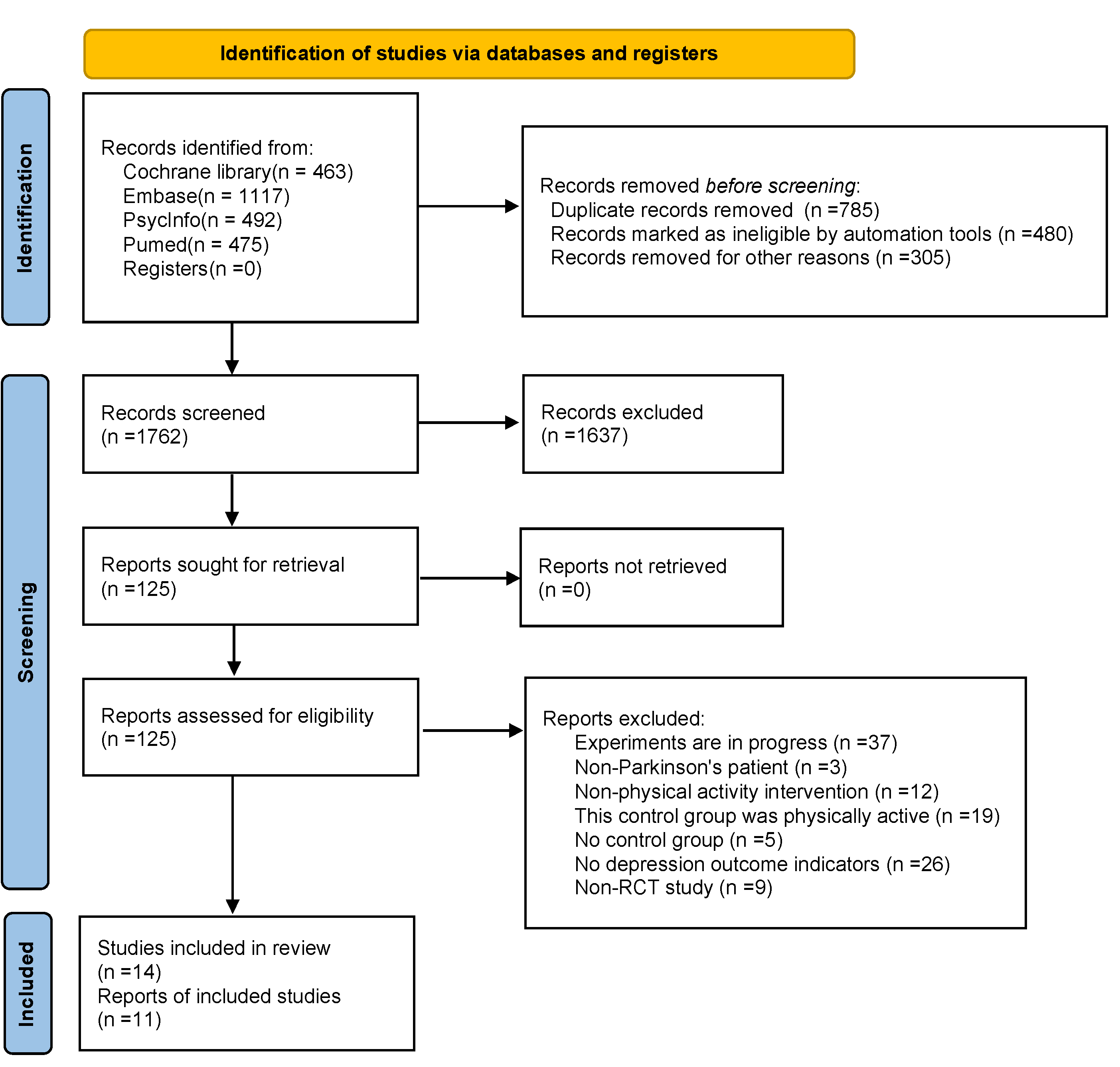
2.1. Literature Search
2.2. Study Selection
2.3. Data Extraction
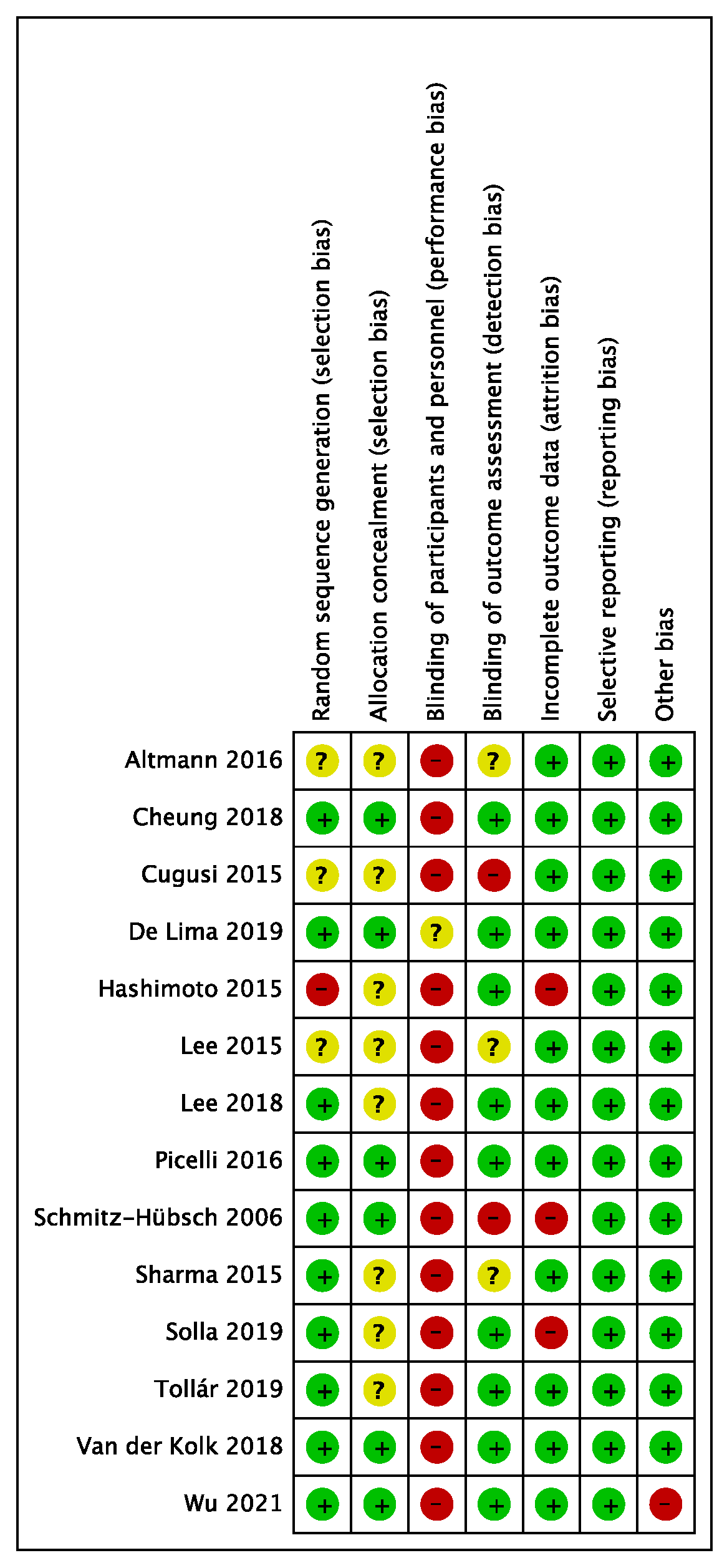
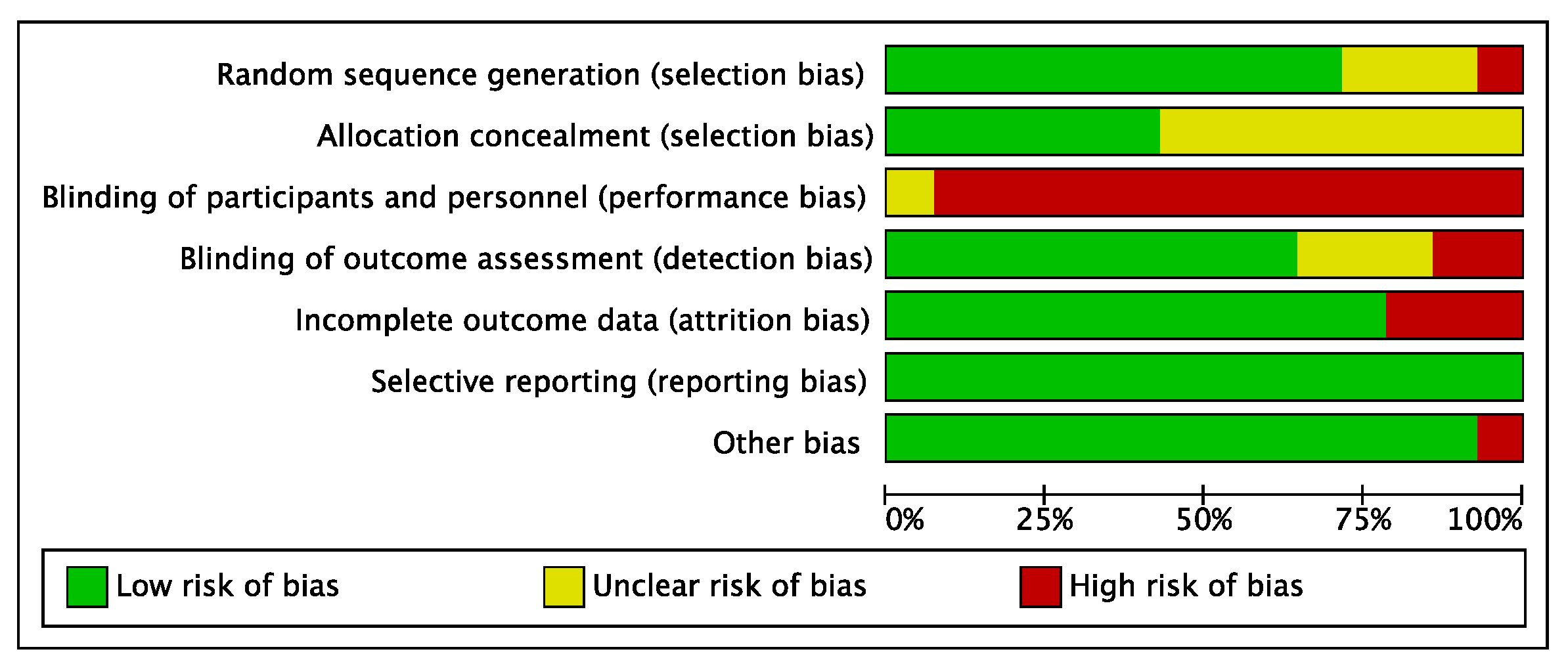
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Included Studies
3.2. Quality Assessment
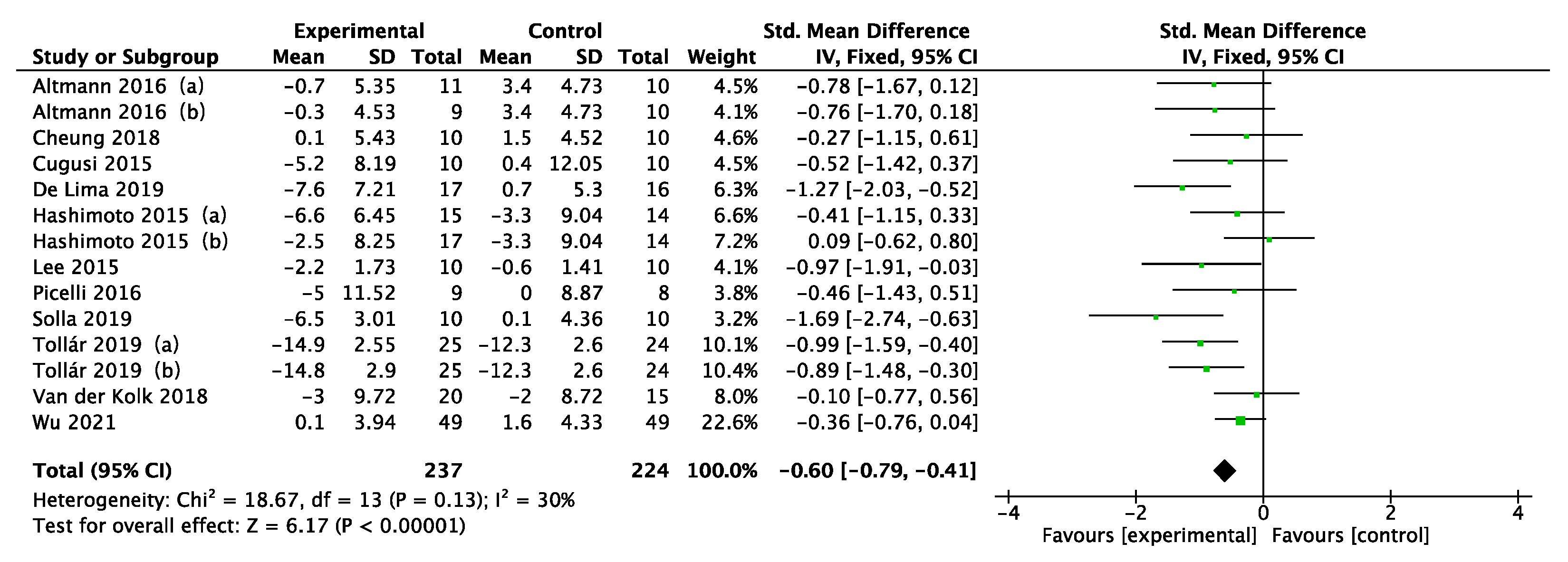
3.3. Effect of the Intervention
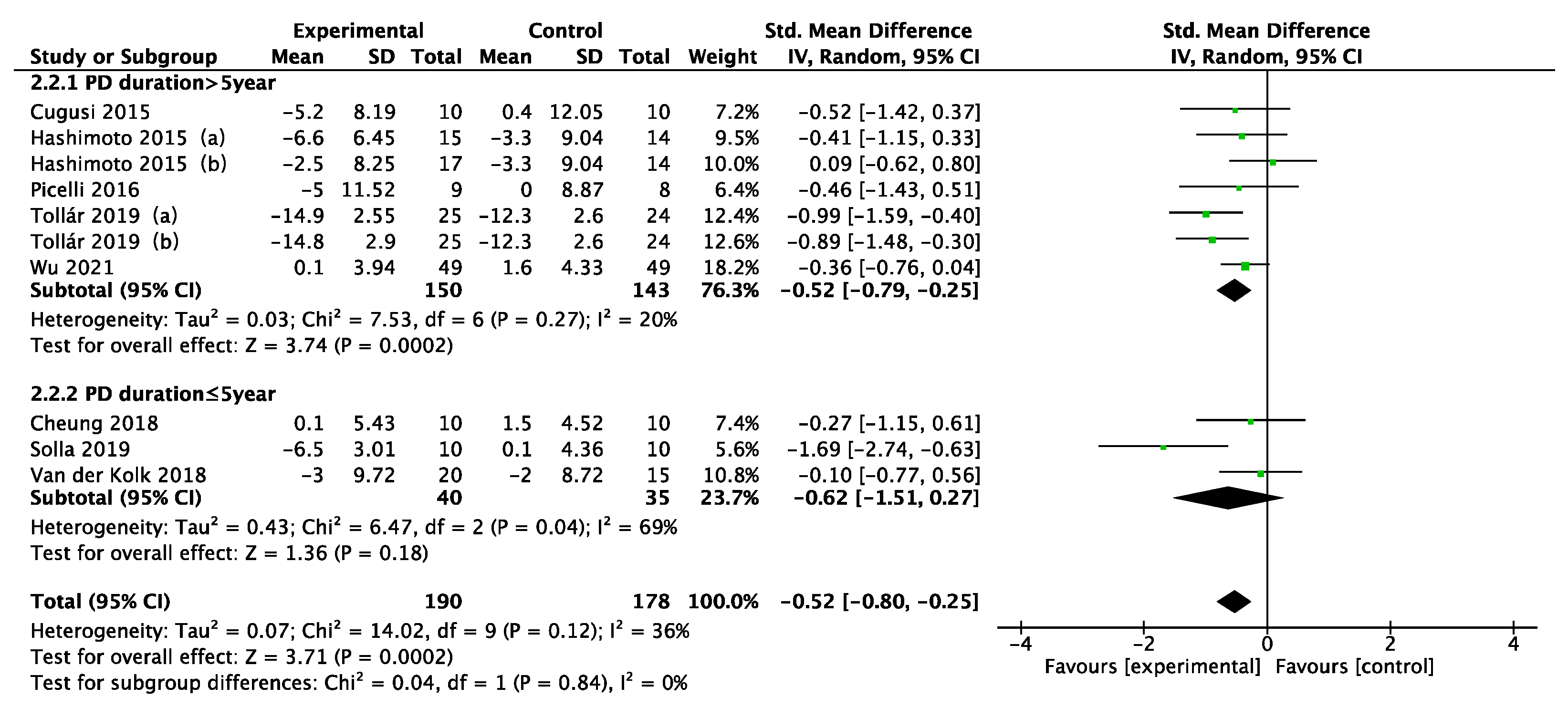
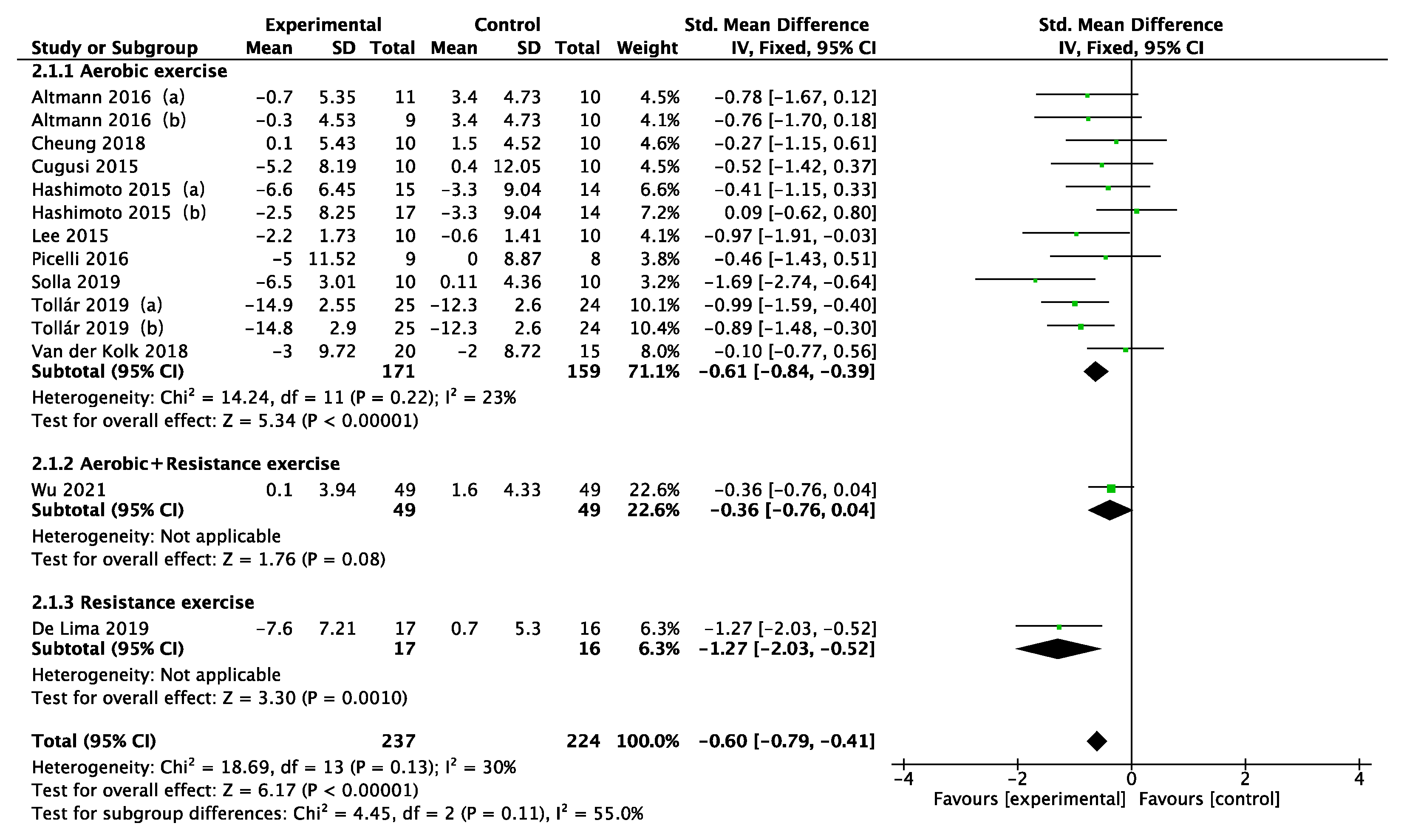
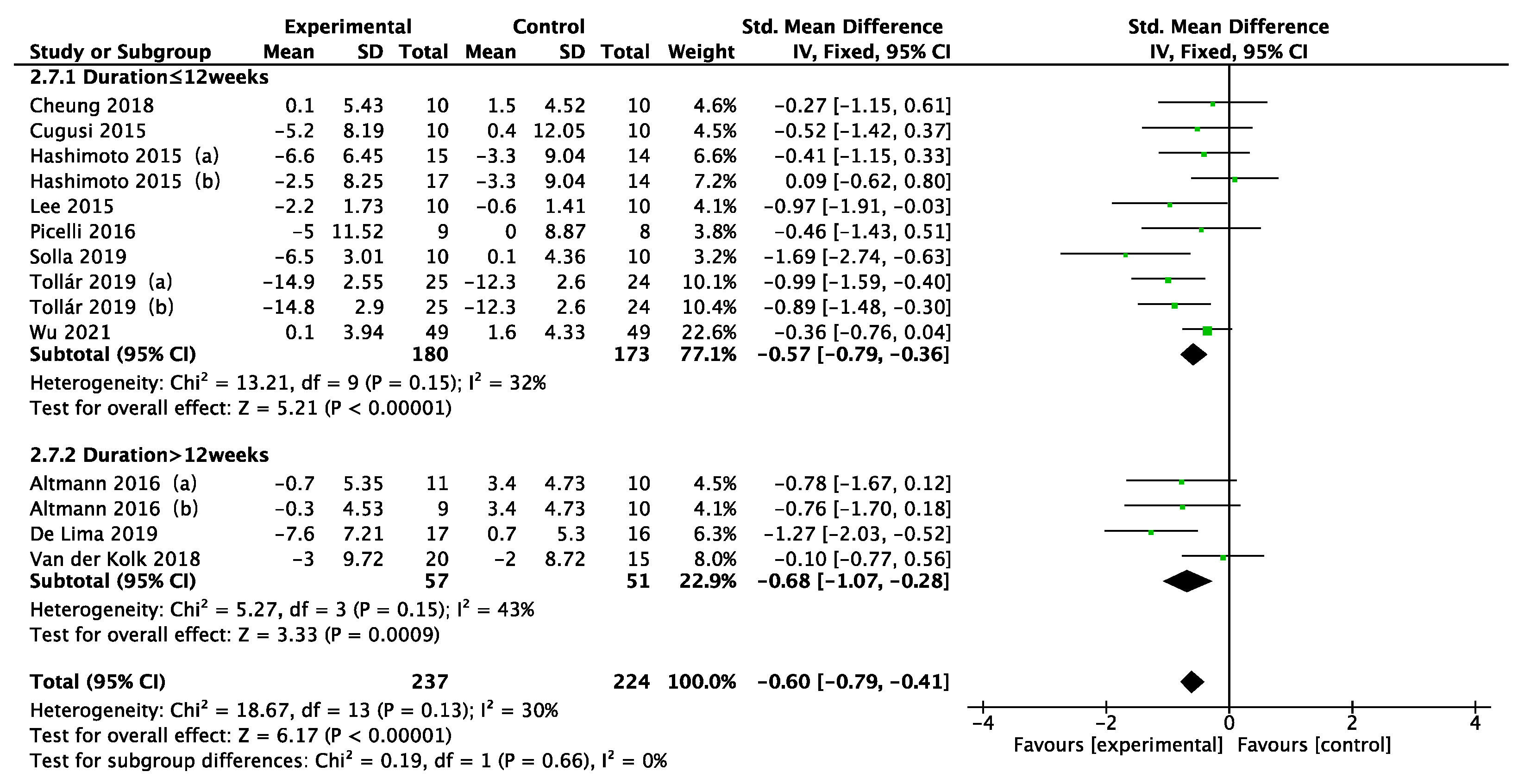
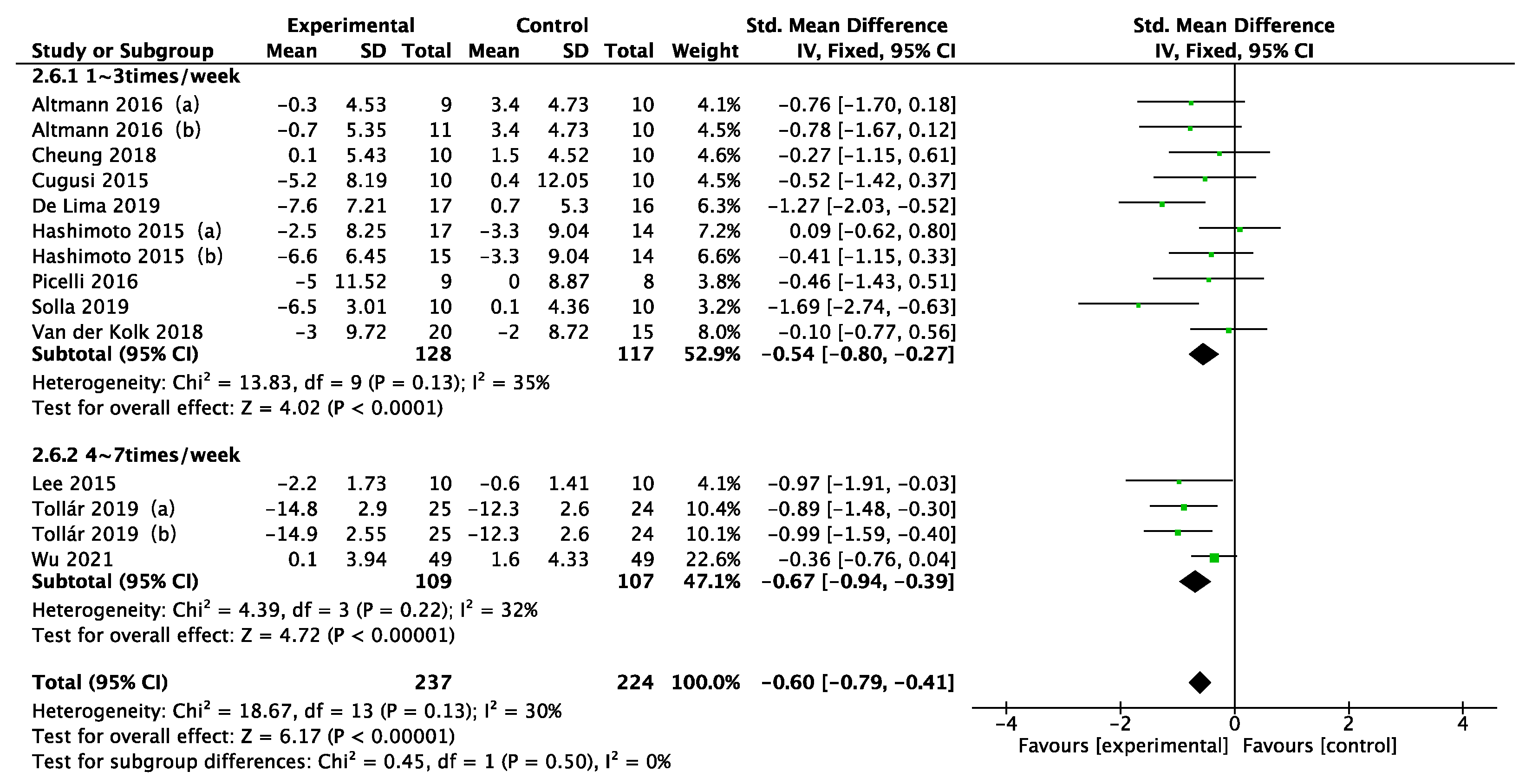
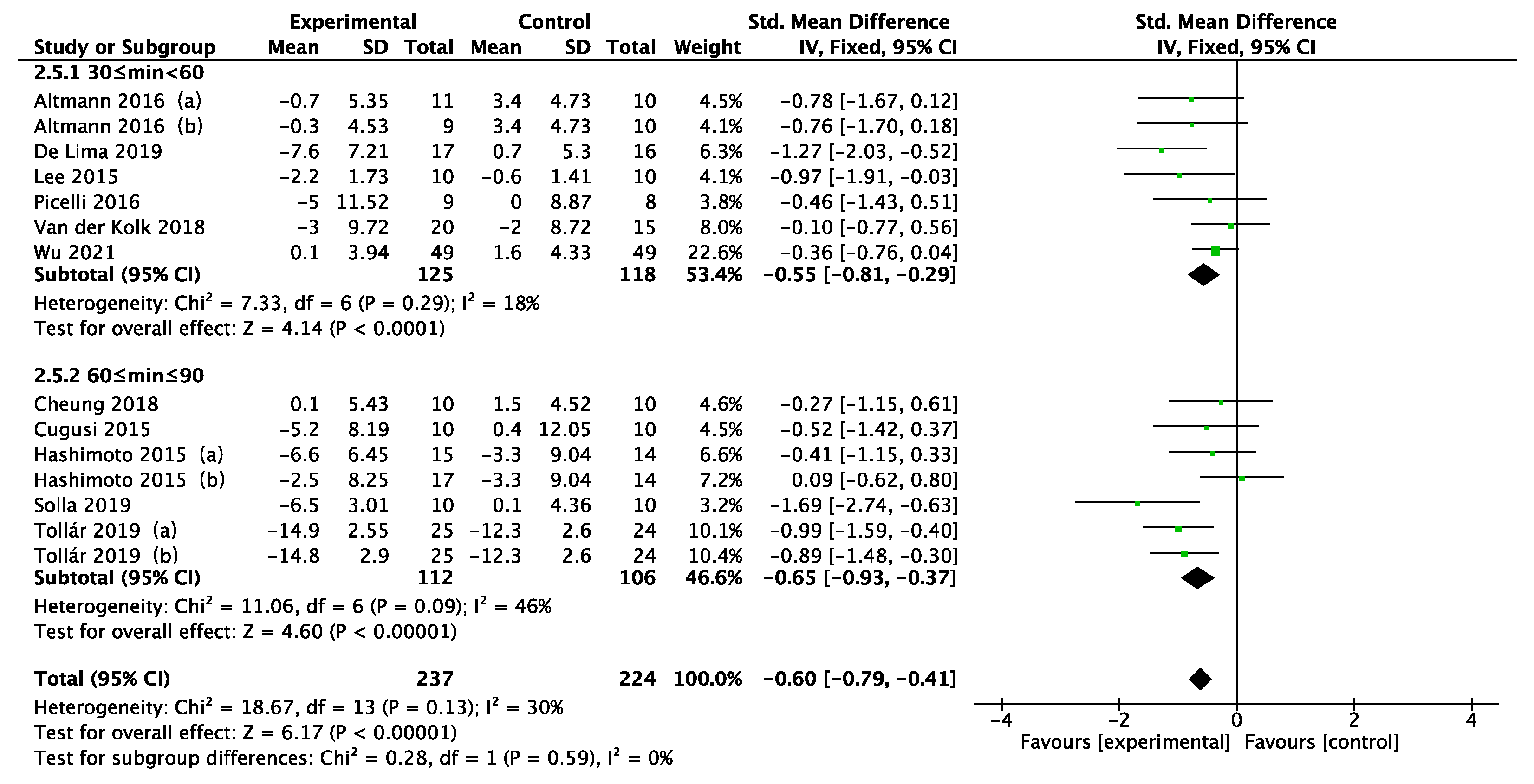
3.4. Subgroup Analysis
3.5. Regression Analysis
3.6. Sensitivity Analysis
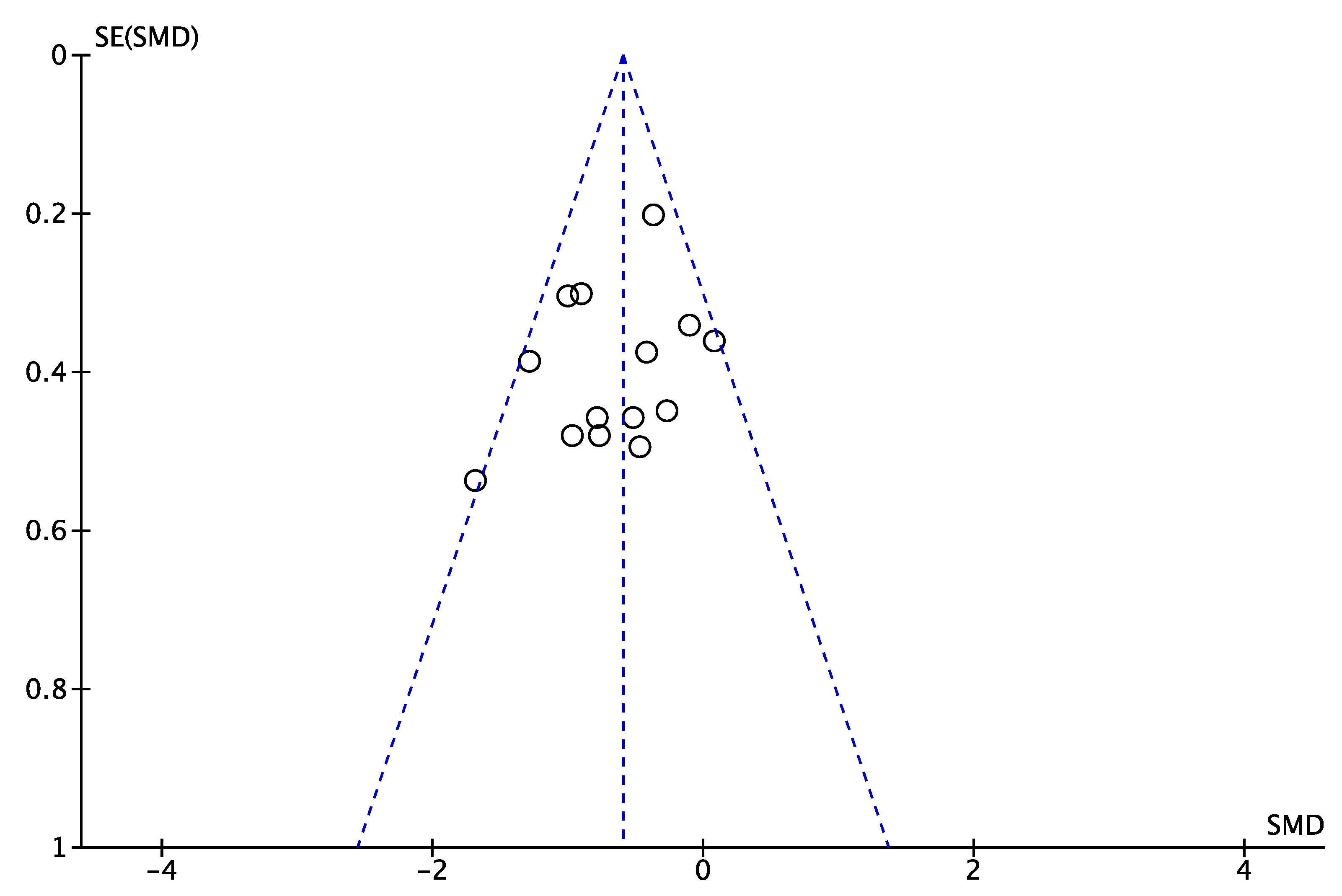
3.7. Publication Bias
3.8. Adverse Events
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schapira, A.H.V. Neurobiology and treatment of Parkinson’s disease. Trends Pharmacol. Sci. 2009, 30, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Poewe, W.; Seppi, K.; Tanner, C.M.; Halliday, G.M.; Brundin, P.; Volkmann, J.; Schrag, A.-E.; Lang, A.E. Parkinson disease. Nat. Rev. Dis. Primers 2017, 3, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Ascherio, A.; Schwarzschild, M.A. The epidemiology of Parkinson's disease: Risk factors and prevention. Lancet Neurol. 2016, 15, 1257–1272. [Google Scholar] [CrossRef]
- Tandberg, E.; Larsen, J.P.; Nessler, E.G.; Riise, T.; Aarli, J.A. The epidemiology of Parkinson's disease in the county of Rogaland, Norway. Mov. Disord. 1995, 10, 541–549. [Google Scholar] [CrossRef]
- Winker, M.A. Aging in the 21st century: A call for papers. JAMA 2002, 287, 1326. [Google Scholar] [CrossRef]
- Wirdefeldt, K.; Adami, H.O.; Cole, P.; Trichopoulos, D.; Mandel, J. Epidemiology and etiology of Parkinson’s disease: A review of the evidence. Eur. J. Epidemiol. 2011, 26, S1–S58. [Google Scholar] [CrossRef]
- Cummings, L.J. Depression and Parkinson’s disease. A review. Am. J. Psychiatry 1992, 149, 443–454. [Google Scholar] [CrossRef]
- Reijnders, J.S.; Ehrt, U.; Weber, W.E.; Aarsland, D.; Leentjens, A.F. A systematic review of prevalence studies of depression in Parkinson's disease. Mov. Disord. 2008, 23, 183–189; quiz 313. [Google Scholar] [CrossRef] [Green Version]
- Pachana, N.A.; Egan, S.J.; Laidlaw, K.; Dissanayaka, N.; Byrne, G.J.; Brockman, S.; Marsh, R.; Starkstein, S. Clinical issues in the treatment of anxiety and depression in older adults with Parkinson’s disease. Mov. Disord. 2013, 28, 1930–1934. [Google Scholar] [CrossRef]
- Beekman, A.T.; Copeland, J.; Prince, M.J. Review of community prevalence of depression in later life. Br. J. Psychiatry 1999, 174, 307–311. [Google Scholar] [CrossRef]
- Ravina, B.; Camicioli, R.; Como, P.G.; Marsh, L.; Jankovic, J.; Weintraub, D.; Elm, J. The impact of depressive symptoms in early Parkinson disease. Neurology 2007, 69, 342–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skapinakis, P.; Bakola, E.; Salanti, G.; Lewis, G.; Kyritsis, A.P.; Mavreas, V. Efficacy and acceptability of selective serotonin reuptake inhibitors for the treatment of depression in Parkinson’s disease: A systematic review and meta-analysis of randomized controlled trials. BMC Neurol. 2010, 10, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edwards, J.G.; Anderson, I. Systematic review and guide to selection of selective serotonin reuptake inhibitors. Drugs 1999, 57, 507–533. [Google Scholar] [CrossRef] [PubMed]
- Seppi, K.; Weintraub, D.; Coelho, M.; Perez-Lloret, S.; Fox, S.H.; Katzenschlager, R.; Hametner, E.M.; Poewe, W.; Rascol, O.; Goetz, C.G.; et al. The Movement Disorder Society Evidence-Based Medicine Review Update: Treatments for the non-motor symptoms of Parkinson's disease. Mov. Disord. 2011, 26, S42–S80. [Google Scholar] [CrossRef]
- Ryan, M.; Eatmon, C.V.; Slevin, J.T. Drug treatment strategies for depression in Parkinson disease. Expert Opin. Pharmacother. 2019, 20, 1351–1363. [Google Scholar] [CrossRef]
- Seppi, K.; Ray Chaudhuri, K.; Coelho, M.; Fox, S.H.; Katzenschlager, R.; Perez Lloret, S.; Weintraub, D.; Sampaio, C.; collaborators of the Parkinson's Disease Update on Non-Motor Symptoms Study Group on behalf of the Movement Disorders Society Evidence-Based Medicine Committee; Chahine, L. Update on treatments for nonmotor symptoms of Parkinson’s disease—an evidence-based medicine review. Mov. Disord. 2019, 34, 180–198. [Google Scholar] [CrossRef] [Green Version]
- Miyasaki, J.M.; Shannon, K.; Voon, V.; Ravina, B.; Kleiner-Fisman, G.; Anderson, K.; Shulman, L.M.; Gronseth, G.; Weiner, W.J. Practice Parameter: Evaluation and treatment of depression, psychosis, and dementia in Parkinson disease (an evidence-based review): Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2006, 66, 996–1002. [Google Scholar] [CrossRef]
- Ban, M.; Yue, X.; Dou, P.; Zhang, P. The Effects of Yoga on Patients with Parkinson’s Disease: A Meta-Analysis of Randomized Controlled Trials. Behav. Neurol. 2021, 2021, 5582488. [Google Scholar] [CrossRef]
- Song, R.; Grabowska, W.; Park, M.; Osypiuk, K.; Vergara-Diaz, G.P.; Bonato, P.; Hausdorff, J.M.; Fox, M.; Sudarsky, L.R.; Macklin, E.; et al. The impact of Tai Chi and Qigong mind-body exercises on motor and non-motor function and quality of life in Parkinson’s disease: A systematic review and meta-analysis. Parkinsonism Relat. Disord. 2017, 41, 3–13. [Google Scholar] [CrossRef]
- Wang, L.L.; Sun, C.J.; Wang, Y.; Zhan, T.T.; Yuan, J.; Niu, C.Y.; Yang, J.; Huang, S.; Cheng, L. Effects of dance therapy on non-motor symptoms in patients with Parkinson’s disease: A systematic review and meta-analysis. Aging Clin. Exp. Res. 2022, 34, 1201–1208. [Google Scholar] [CrossRef]
- Wu, P.L.; Lee, M.; Huang, T.T. Effectiveness of physical activity on patients with depression and Parkinson’s disease: A systematic review. PLoS ONE 2017, 12, e0181515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marotta, N.; Demeco, A.; Indino, A.; de Scorpio, G.; Moggio, L.; Ammendolia, A. Nintendo WiiTM versus Xbox KinectTM for functional locomotion in people with Parkinson’s disease: A systematic review and network meta-analysis. Disabil. Rehabil. 2022, 44, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Dockx, K.; Bekkers, E.M.; Van den Bergh, V.; Ginis, P.; Rochester, L.; Hausdorff, J.M.; Mirelman, A.; Nieuwboer, A. Virtual reality for rehabilitation in Parkinson’s disease. Cochrane Database Syst. Rev. 2016, 12, CD010760. [Google Scholar] [CrossRef] [PubMed]
- de Lima, T.A.; Ferreira-Moraes, R.; Alves, W.M.G.D.C.; Alves, T.G.G.; Pimentel, C.P.; Sousa, E.C.; Abrahin, O.; Cortinhas-Alves, E.A. Resistance training reduces depressive symptoms in elderly people with Parkinson disease: A controlled randomized study. Scand. J. Med. Sci. Sports 2019, 29, 1957–1967. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.L.; Lee, M.; Wu, S.L.; Ho, H.H.; Chang, M.H.; Lin, H.S.; Huang, T.T. Effects of home-based exercise on motor, non-motor symptoms and health-related quality of life in Parkinson’s disease patients: A randomized controlled trial. Jpn. J. Nurs. Sci. 2021, 18, e12418. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: Oxfordshire, UK, 2013. [Google Scholar]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Sharma, N.K.; Robbins, K.; Wagner, K.; Colgrove, Y.M. A randomized controlled pilot study of the therapeutic effects of yoga in people with Parkinson’s disease. Int. J. Yoga 2015, 8, 74. [Google Scholar]
- Schmitz-Hübsch, T.; Pyfer, D.; Kielwein, K.; Fimmers, R.; Klockgether, T.; Wüllner, U. Qigong exercise for the symptoms of Parkinson’s disease: A randomized, controlled pilot study. Mov Disord. 2006, 21, 543–548. [Google Scholar] [CrossRef]
- Lee, H.-J.; Kim, S.-Y.; Chae, Y.; Kim, M.-Y.; Yin, C.; Jung, W.-S.; Cho, K.-H.; Kim, S.-N.; Park, H.-J.; Lee, H. Turo (Qi Dance) program for Parkinson’s disease patients: Randomized, assessor blind, waiting-list control, partial crossover study. Explore 2018, 14, 216–223. [Google Scholar] [CrossRef]
- Altmann, L.J.; Stegemöller, E.; Hazamy, A.A.; Wilson, J.P.; Bowers, D.; Okun, M.S.; Hass, C.J. Aerobic Exercise Improves Mood, Cognition, and Language Function in Parkinson’s Disease: Results of a Controlled Study. J. Int Neuropsychol Soc. 2016, 22, 878–889. [Google Scholar] [CrossRef] [PubMed]
- Cheung, C.; Bhimani, R.; Wyman, J.F.; Konczak, J.; Zhang, L.; Mishra, U.; Terluk, M.; Kartha, R.V.; Tuite, P. Effects of yoga on oxidative stress, motor function, and non-motor symptoms in Parkinson’s disease: A pilot randomized controlled trial. Pilot Feasibility Stud. 2018, 4, 162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cugusi, L.; Solla, P.; Serpe, R.; Carzedda, T.; Piras, L.; Oggianu, M.; Gabba, S.; Di Blasio, A.; Bergamin, M.; Cannas, A.; et al. Effects of a Nordic Walking program on motor and non-motor symptoms, functional performance and body composition in patients with Parkinson’s disease. NeuroRehabilitation 2015, 37, 245–254. [Google Scholar] [CrossRef]
- Hashimoto, H.; Takabatake, S.; Miyaguchi, H.; Nakanishi, H.; Naitou, Y. Effects of dance on motor functions, cognitive functions, and mental symptoms of Parkinson’s disease: A quasi-randomized pilot trial. Complement. Med. 2015, 23, 210–219. [Google Scholar] [CrossRef] [PubMed]
- Lee, N.Y.; Lee, D.K.; Song, H.S. Effect of virtual reality dance exercise on the balance, activities of daily living, and depressive disorder status of Parkinson’s disease patients. J. Phys. Sci. 2015, 27, 145–147. [Google Scholar] [CrossRef] [Green Version]
- Picelli, A.; Varalta, V.; Melotti, C.; Zatezalo, V.; Fonte, C.; Amato, S.; Saltuari, L.; Santamato, A.; Fiore, P.; Smania, N. Effects of treadmill training on cognitive and motor features of patients with mild to moderate Parkinson’s disease: A pilot, single-blind, randomized controlled trial. Funct Neurol. 2016, 31, 25–31. [Google Scholar] [CrossRef]
- Solla, P.; Cugusi, L.; Bertoli, M.; Cereatti, A.; Della Croce, U.; Pani, D.; Fadda, L.; Cannas, A.; Marrosu, F.; Defazio, G.; et al. Sardinian Folk Dance for Individuals with Parkinson’s Disease: A Randomized Controlled Pilot Trial. J. Altern. Complementary Med. 2019, 25, 305–316. [Google Scholar] [CrossRef]
- Tollár, J.; Nagy, F.; Hortobágyi, T. Vastly Different Exercise Programs Similarly Improve Parkinsonian Symptoms: A Randomized Clinical Trial. Gerontology 2019, 65, 120–127. [Google Scholar] [CrossRef]
- van der Kolk, N.M.; de Vries, N.M.; Penko, A.L.; van der Vlugt, M.; Mulder, A.A.; Post, B.; Alberts, J.L.; Bloem, B.R. A remotely supervised home-based aerobic exercise programme is feasible for patients with Parkinson’s disease: Results of a small randomised feasibility trial. J. Neurol. Neurosurg. Psychiatry 2018, 89, 1003–1005. [Google Scholar] [CrossRef]
- Jin, X.; Wang, L.; Liu, S.; Zhu, L.; Loprinzi, P.D.; Fan, X. The Impact of Mind-body Exercises on Motor Function, Depressive Symptoms, and Quality of Life in Parkinson’s Disease: A Systematic Review and Meta-analysis. Int. J. Environ. Res. Public Health 2019, 17, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agudelo, L.Z.; Femenía, T.; Orhan, F.; Porsmyr-Palmertz, M.; Goiny, M.; Martinez-Redondo, V.; Correia, J.C.; Izadi, M.; Bhat, M.; Schuppe-Koistinen, I.; et al. Skeletal muscle PGC-1α1 modulates kynurenine metabolism and mediates resilience to stress-induced depression. Cell 2014, 159, 33–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aarsland, D.; Påhlhagen, S.; Ballard, C.G.; Ehrt, U.; Svenningsson, P. Depression in Parkinson disease—Epidemiology, mechanisms and management. Nat. Rev. Neurol. 2012, 8, 35–47. [Google Scholar] [CrossRef] [PubMed]
- Schaeffer, E.; Roeben, B.; Granert, O.; Hanert, A.; Liepelt-Scarfone, I.; Leks, E.; Otterbein, S.; Saraykin, P.; Busch, J.H.; Synofzik, M.; et al. Effects of exergaming on hippocampal volume and brain-derived neurotrophic factor levels in Parkinson’s disease. Eur. J. Neurol. 2022, 29, 441–449. [Google Scholar] [CrossRef]
- Wegner, M.; Helmich, I.; Machado, S.; Nardi, A.E.; Arias-Carrion, O.; Budde, H. Effects of exercise on anxiety and depression disorders: Review of meta- analyses and neurobiological mechanisms. CNS Neurol. Disord. Drug Targets 2014, 13, 1002–1014. [Google Scholar] [CrossRef] [Green Version]
- Berchtold, N.C.; Kesslak, J.P.; Cotman, C.W. Hippocampal brain-derived neurotrophic factor gene regulation by exercise and the medial septum. J. Neurosci. Res. 2002, 68, 511–521. [Google Scholar] [CrossRef]
- D’Ascola, A.; Bruschetta, G.; Zanghì, G.; Campo, S.; Medica, P.; Campana, S.; Ferlazzo, G.; Gibbs, B.F.; Ferlazzo, A.M. Changes in plasma 5-HT levels and equine leukocyte SERT expression in response to treadmill exercise. Res. Vet. Sci. 2018, 118, 184–190. [Google Scholar] [CrossRef]
- Basso, J.C.; Suzuki, W.A. The Effects of Acute Exercise on Mood, Cognition, Neurophysiology, and Neurochemical Pathways: A Review. Brain Plast. 2017, 2, 127–152. [Google Scholar] [CrossRef] [Green Version]
- Speelman, A.D.; van de Warrenburg, B.P.; van Nimwegen, M.; Petzinger, G.M.; Munneke, M.; Bloem, B.R. How might physical activity benefit patients with Parkinson disease? Nat. Rev. Neurol. 2011, 7, 528–534. [Google Scholar] [CrossRef]
- Zoladz, J.A.; Majerczak, J.; Zeligowska, E.; Mencel, J.; Jaskolski, A.; Jaskolska, A.; Marusiak, J. Moderate-intensity interval training increases serum brain-derived neurotrophic factor level and decreases inflammation in Parkinson’s disease patients. J. Physiol Pharm. 2014, 65, 441–448. [Google Scholar]
- Ravina, B.; Elm, J.; Camicioli, R.; Como, P.G.; Marsh, L.; Jankovic, J.; Weintraub, D. The course of depressive symptoms in early Parkinson’s disease. Mov. Disord. 2009, 24, 1306–1311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Potter, R.; Ellard, D.; Rees, K.; Thorogood, M. A systematic review of the effects of physical activity on physical functioning, quality of life and depression in older people with dementia. Int. J. Geriatr. Psychiatry 2011, 26, 1000–1011. [Google Scholar] [CrossRef] [PubMed]
- ACSM. Available online: https://www.acsm.org/education-resources/trending-topics-resources/resource-library/detail?id=6dec0a8d-215d-4d70-a1e3-2e34c1e8b7df (accessed on 1 March 2022).
- Borrione, P.; Tranchita, E.; Sansone, P.; Parisi, A. Effects of physical activity in Parkinson’s disease: A new tool for rehabilitation. World J. Methodol 2014, 4, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Warburton, D.E.; Nicol, C.W.; Bredin, S.S. Health benefits of physical activity: The evidence. CMAJ 2006, 174, 801–809. [Google Scholar] [CrossRef] [Green Version]
- Dibble, L.E.; Hale, T.F.; Marcus, R.L.; Droge, J.; Gerber, J.P.; LaStayo, P.C. High-intensity resistance training amplifies muscle hypertrophy and functional gains in persons with Parkinson’s disease. Mov. Disord. 2006, 21, 1444–1452. [Google Scholar] [CrossRef]
- Sironi, V.A.; Riva, M.A. Neurological implications and neuropsychological considerations on folk music and dance. Prog. Brain Res. 2015, 217, 187–205. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Main Author | Year | Country/ Region | Age | H and Y | PD Duration | Sample Size (M/F) | Experimental Group Intervention (Duration/Frequency/Time) | Control Group | Depression Outcome Measures | Follow-Up Time (Week) |
|---|---|---|---|---|---|---|---|---|---|---|
| de Lima [24] | 2019 | Brazil | 66.7 ± 5.3 | 1–3 | No reported | 33 (no reported) | Type: resistance training (20 weeks × 2/week × 30–40 min/session) | No exercise | HAMD | 20 weeks |
| Altmann [33] | 2016 | USA | 64.6 ± 8.7 | 1–3 | No reported | 30 (no reported) | Type: G1: aerobic exercise; G2: stretch-balance training (16 weeks × 3/week × from 20 min/session to 45 min by increasing exercise time by 5 min each week) | Continued normal activities | BDI | 16 weeks |
| Cheung [34] | 2018 | USA | 63 ± 8.0 | 1–3 | 4.8 ± 2.9 | 20 (no reported) | Type: yoga (12 weeks × 2/week × 60 min/session) | Wait list | BDI | 26 weeks |
| Cugusi [35] | 2015 | Italy | 67.3 ± 7.8 | 1–3 | 7.0 ± 3.0 | 20 (16/4) | Type: Nordic walking (12 weeks × 2/week × 60 min/session) | Conventional care | BDI | 12 weeks |
| Hashimoto [36] | 2015 | Japan | 66.5 ± 10.4 | 2–4 | 7.0 ± 5.0 | 46 (12/34) | Type: G1: dance; G2: PD exercise (12 weeks × 1/week × 60 min/session) | No intervention | SDS | 12 weeks |
| Lee [37] | 2015 | Korea | 69.3 ± 3.1 | No reported | No reported | 20 (10/10) | Type: virtual reality dance (6 weeks × 5/week × 30 min/session) | No exercise | BDI | 6 weeks |
| Picelli [38] | 2016 | Italy | 71.4 ± 8.1 | 1–3 | 11.0 ± 4.8 | 17 (12/5) | Type: treadmill training (4 weeks × 3/week × 45 min/session) | Regular social interactions | BDI | 4 weeks |
| Solla [39] | 2019 | Italy | 67.4 ± 6.1 | 1–3 | 4.7 ± 3.7 | 20 (13/7) | Type: Sardinian folk dance (12 weeks × 2/week × 90 min/session) | Usual care | BDI | 12 weeks |
| Tollár [40] | 2019 | Hungary | 69.4 ± 4.5 | 2–3 | 7.4 ± 2.0 | 74 (no reported) | Type: G1: agility exergaming; G2: stationary cycling (5 weeks × 5/week × 60 min/session) | Wait list | BDI | 5 weeks |
| van der Kolk [41] | 2018 | USA | 58.9 ±8.8 | 1–2 | 0.92 ± 0.9 | 37 (24/13) | Type: aerobic exercise(stationary bike) (26 weeks × 3/week × 30 min/session) | No intervention | HADS | 26 weeks |
| Wu [25] | 2021 | Taiwan | 65.1 ±7.5 | 1–2 | 5.3 ± 3.9 | 98 (56/42) | Type: home-based exercise (aerobic exercise, resistance training) (8 weeks × >3/OR7/week × 30–50 OR 10–15 min/session) | No exercise | GDS | 8 weeks |
| Lee [32] | 2018 | Korea | 65 ± 6.8 | 1–3 | No reported | 32 (17/15) | Type: Turo (qi dance) (8 weeks × 2/week × 60 min/session) | Wait list | BDI | 8 weeks |
| Sharma [30] | 2015 | USA | 66.9 ± 12.0 | 1–2 | 3.0 ± 0.4 | 13 (8/5) | Type: yoga (12 weeks × 2/week × 60 min/session) | No intervention | GDS | 12 weeks |
| Schmitz-Hübsch [31] | 2006 | Germany | 63.8 ± 7.5 | No reported | 5.8 ± 4.2 | 56 (43/13) | Type: qigong (8 weeks × 1/week × 60 min/session) | No intervention | MADRS | 52 weeks |
| _ES | Coef. | Std. Err. | t | p > |t| | 95% Conf. Interval | |
|---|---|---|---|---|---|---|
| Type | −0.4978215 | 1.30632 | −0.38 | 0.729 | −4.655116 | 3.659473 |
| Time | −0.0546558 | 0.1224466 | −0.45 | 0.686 | −0.4443355 | 0.3350238 |
| Period | −0.1528421 | 0.4147001 | −0.37 | 0.737 | −1.472603 | 1.166919 |
| Frequency | −0.4658228 | 1.165822 | −0.40 | 0.716 | −4.175988 | 3.244342 |
| Age | 0.0591567 | 0.8335549 | 0.07 | 0.948 | −2.593587 | 2.7119 |
| Disease duration | −0.336243 | 1.738527 | −0.19 | 0.859 | −5.869013 | 5.196527 |
| _Cons | 4.253626 | 29.36428 | 0.14 | 0.894 | −89.19663 | 97.70389 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tian, J.; Kang, Y.; Liu, P.; Yu, H. Effect of Physical Activity on Depression in Patients with Parkinson’s Disease: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 6849. https://doi.org/10.3390/ijerph19116849
Tian J, Kang Y, Liu P, Yu H. Effect of Physical Activity on Depression in Patients with Parkinson’s Disease: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2022; 19(11):6849. https://doi.org/10.3390/ijerph19116849
Chicago/Turabian StyleTian, Jianing, Yujie Kang, Peifeng Liu, and Hongyan Yu. 2022. "Effect of Physical Activity on Depression in Patients with Parkinson’s Disease: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 19, no. 11: 6849. https://doi.org/10.3390/ijerph19116849