
Supporting Adolescents with Mental Health Problems in Secondary Education: Feasibility of a Supported Education Intervention

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
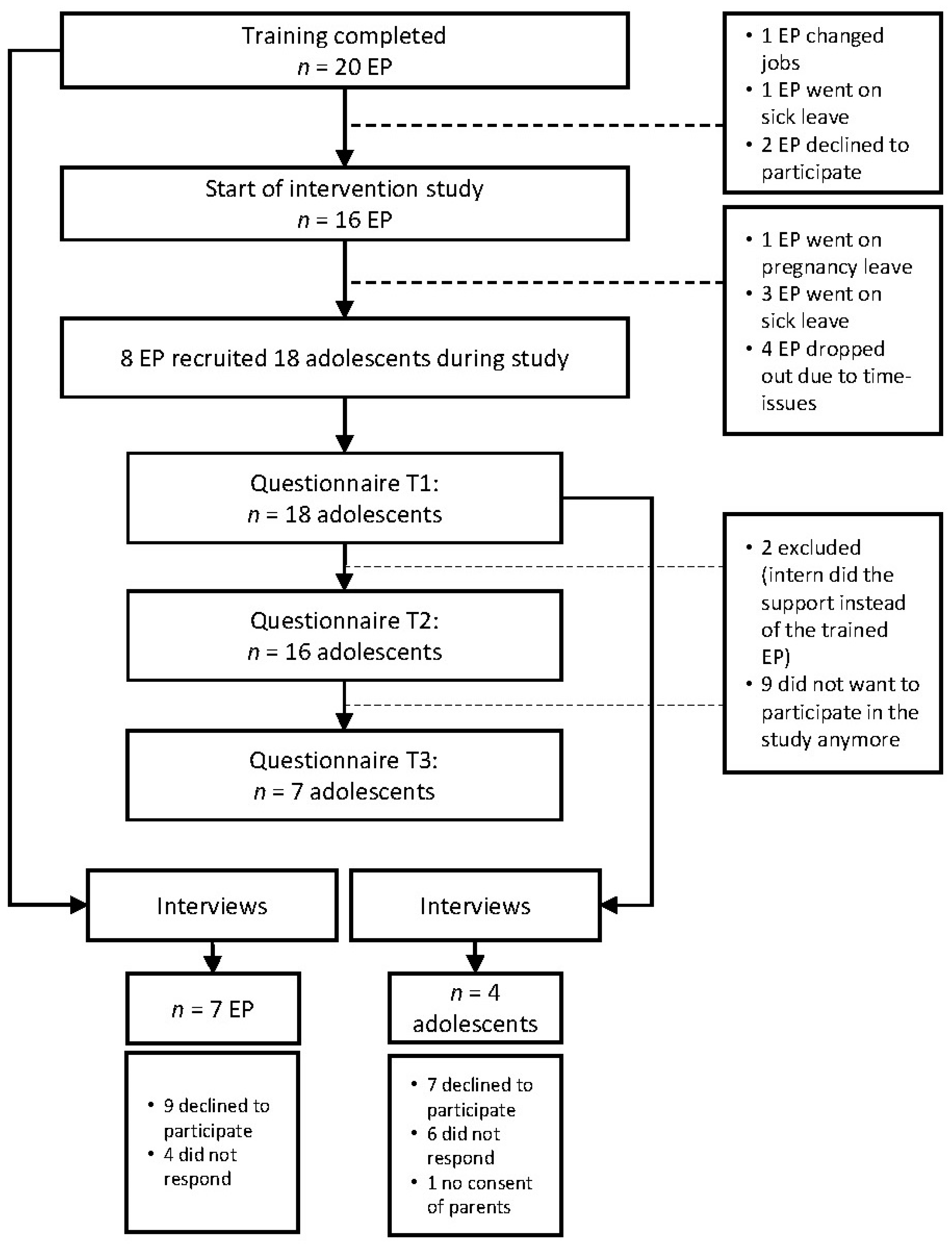
2.1. Participants
2.2. Procedure
2.2.1. Training in the Supported Education Intervention
2.2.2. Data Collection: Questionnaire
2.2.3. Data Collection: Interviews
2.3. Measures
2.3.1. Questionnaire
2.3.2. Interviews
2.4. Data Analysis
2.4.1. Questionnaire
2.4.2. Interviews
3. Results
3.1. Participant Characteristics
3.2. Preliminary Effectiveness
3.3. Acceptability of the Intervention
3.3.1. Educational Professionals (EP)
3.3.2. Adolescents
3.4. Determinants for Successful Implementation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Learning Goals: | |
|---|---|
| Meeting 1 | Understanding the mission and underlying framework of the intervention. |
Understand and practice step 1 of the intervention:
| |
Understand and practice step 2:
| |
| Meeting 2 | Understand and practice step 3:
|
| Meeting 3 | Understand and practice step 4: Developing an Individual Development Plan. |
| Understand and practice step 5: Execute, monitor, and evaluate the Individual Development Plan (is it executed, how do you monitor, and does the plan need to be adjusted). | |
| Meetings 4, 5, 6 | Discuss case studies, questions, and problems of the participants. |
| Practice (parts of) the intervention with other participants. | |
| Reflect on and evaluate the intervention and the training. | |
| For more information on the theoretical background of the intervention and the training, see Hofstra and Korevaar, 2016 [19]) | |
References
- Merikangas, K.R.; He, J.P.; Burstein, M.; Swanson, S.A.; Avenevoli, S.; Cui, L.; Benjet, C.; Georgiades, K.; Swendsen, J. Lifetime prevalence of mental disorders in U.S. adolescents: Results from the national comorbidity survey replication-adolescent supplement (NCS-A). J. Am. Acad. Child Adolesc. Psychiatry 2010, 49, 980–989. [Google Scholar] [CrossRef] [Green Version]
- Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Merikangas, K.R.; Walters, E.E. Lifetime Prevalence and Age-of-Onset Distributions of DSM-IV Disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 593–602. Available online: http://archpsyc.jamanetwork.com/article.aspx?doi=10.1001/archpsyc.62.6.593 (accessed on 10 June 2021). [CrossRef] [Green Version]
- Copeland, W.E.; Shanahan, L.; Costello, E.J.; Angold, A. Childhood and adolescent psychiatric disorders as predictors of young adult disorders? Arch. Gen. Psychiatry 2009, 66, 764–772. [Google Scholar] [CrossRef] [Green Version]
- Bor, W.; Dean, A.J.; Najman, J.; Hayatbakhsh, R. Are child and adolescent mental health problems increasing in the 21st century? A systematic review. Aust. N. Z. J. Psychiatry 2014, 48, 606–616. [Google Scholar] [CrossRef]
- Ormel, J.; Raven, D.; van Oort, F.; Hartman, C.A.; Reijneveld, S.A.; Veenstra, R.; Vollebergh, W.A.; Buitelaar, J.; Verhulst, F.C.; Oldehinkel, A.J. Mental Health in Dutch Adolescents: A TRAILS Report on Prevalence, Severity, Age of Onset, Continuity and Co-Morbidity of DSM Disorders. Psychol. Med. 2015, 45, 345–360. Available online: http://www.ncbi.nlm.nih.gov/pubmed/25066533 (accessed on 1 May 2017). [CrossRef] [Green Version]
- Eekelen, J.; Lanser, H.; Schoenmakers, P.; Schouten, M.; van Rijbroek, C.; Kwant, D. Bevindingen Dossieronderzoek Thuiszitters 2010: Thuiszitters, Sneller Terug Naar School. [Results of School-Absence Investigation 2010: Getting them Back to School]. Arnhem. 2010. Available online: www.ingrado.nl (accessed on 1 June 2020).
- Veldman, K.; Bültmann, U.; Stewart, R.E.; Ormel, J.; Verhulst, F.C.; Reijneveld, S.A. Mental health problems and educational attainment in adolescence: 9-year follow-up of the TRAILS study. PLoS ONE 2014, 9, e101751. [Google Scholar] [CrossRef] [Green Version]
- Kieling, C.; Baker-Henningham, H.; Belfer, M.; Conti, G.; Ertem, I.; Omigbodun, O.; Rohde, L.A.; Srinath, S.; Ulkuer, N.; Rahman, A. Child and adolescent mental health worldwide: Evidence for action. Lancet 2011, 378, 1515–1525. [Google Scholar] [CrossRef]
- Veldman, K.; Bültmann, U.; Almansa, J.; Reijneveld, S.A. Childhood Adversities and Educational Attainment in Young Adulthood: The Role of Mental Health Problems in Adolescence. J. Adolesc. Health 2015, 57, 462–467. [Google Scholar] [CrossRef]
- Salerno, J.P. Effectiveness of Universal School-Based Mental Health Awareness Programs Among Youth in the United States: A Systematic Review. J. Sch. Health 2016, 86, 922–931. Available online: http://europepmc.org/backend/ptpmcrender.fcgi?accid=PMC5123790&blobtype=pdf (accessed on 11 June 2020). [CrossRef]
- Wei, Y.; Hayden, J.A.; Kutcher, S.; Zygmunt, A.; McGrath, P. The effectiveness of school mental health literacy programs to address knowledge, attitudes and help seeking among youth. Early Interv. Psychiatry 2013, 7, 109–121. [Google Scholar] [CrossRef]
- Burns, J.R.; Rapee, R.M. Screening for Mental Health Risk in High Schools: The Development of the Youth RADAR. Psychol. Assess. 2016, 28, 1220–1231. [Google Scholar] [CrossRef]
- Snyder, M. Changing the Tide. NASN Sch. Nurse 2015, 30, 130–132. Available online: http://journals.sagepub.com/doi/10.1177/1942602×14553307 (accessed on 11 June 2020). [CrossRef] [PubMed]
- Caldwell, D.M.; Davies, S.R.; Hetrick, S.E.; Palmer, J.C.; Caro, P.; López-López, J.A.; Gunnell, D.; Kidger, J.; Thomas, J.; French, C.; et al. School-Based Interventions to Prevent Anxiety and Depression in Children and Young People: A Systematic Review and Network Meta-Analysis. Lancet Psychiatry 2019, 6, 1011–1020. Available online: www.thelancet.com/psychiatry (accessed on 24 November 2020). [CrossRef] [Green Version]
- Gijzen, M.W.M.; Creemers, D.H.M.; Rasing, S.P.A.; Smit, F.; Engels, R.C.M.E. Evaluation of a Multimodal School-Based Depression and Suicide Prevention Program among Dutch Adolescents: Design of a Cluster-Randomized Controlled Trial. BMC Psychiatry 2018, 18, 1–12. Available online: https://bmcpsychiatry.biomedcentral.com/articles/10.1186/s12888-018-1710-2 (accessed on 24 November 2020). [CrossRef] [PubMed] [Green Version]
- Gronholm, P.C.; Nye, E.; Michelson, D. Stigma Related to Targeted School-Based Mental Health Interventions: A Systematic Review of Qualitative Evidence. J. Affect. Disord. 2018, 240, 17–26. [Google Scholar] [CrossRef] [Green Version]
- Cilar, L.; Štiglic, G.; Kmetec, S.; Barr, O.; Pajnkihar, M. Effectiveness of school-based mental well-being interventions among adolescents: A systematic review. J. Adv. Nurs. 2020, 76, 2023–2045. [Google Scholar] [CrossRef]
- Health Council of the Netherlands. Participation by Young People with Mental Health Problems; Health Council of the Netherlands: The Hague, The Netherlands, 2014. [Google Scholar]
- Hofstra, J.; Korevaar, E.L. Supported Education Toolkit; Hofstra, J., Korevaar, L., Eds.; De Volharding, Groningen Collaboration: Groningen, The Netherlands, 2016. [Google Scholar]
- Substance Abuse and Mental Health Services Administration. Supported Education: Getting Started with Evidence-Based and Promising Practices; U.S. Department of Health and Human Services: Rockville, MD, USA, 2011.
- Sullivan, A.P.; Nicolellis, D.L.; Danley, K.S.; MacDonald-Wilson, K. Choose-get- keep: A psychiatric rehabilitation approach to Supported Education. Psychosoc. Rehabil. J. 1993, 17, 55–68. [Google Scholar] [CrossRef]
- Anthony, W.; Cohen, M.; Farkas, M.; Gagne, C. Psychiatric Rehabilitation, 2nd ed.; Boston University, Center of Psychiatric Rehabilitation: Boston, MA, USA, 2002. [Google Scholar]
- Rogers, E.S.; Kash-MacDonald, M.; Bruker, D.; Maru, M. Systematic Review of Supported Education Literature, 1989–2009; Boston University, Sargent College, Center for Psychiatric Rehabilitation: Boston, MA, USA, 2010; Available online: http://www.bu.edu/drrk/research-syntheses/psychiatric-disabilities/supported-education/ (accessed on 24 November 2020).
- Mcgorry, P.D.; Mei, C.; Chanen, A.; Hodges, C.; Alvarez-Jimenez, M.; Killackey, E. Designing and scaling up integrated youth mental health care. World Psychiatry 2022, 21, 61–76. [Google Scholar] [CrossRef]
- Bowen, D.J.; Kreuter, M.; Spring, B.; Cofta-Woerpel, L.; Linnan, L.; Weiner, D.; Bakken, S.; Kaplan, C.P.; Squiers, L.; Fabrizio, C.; et al. How We Design Feasibility Studies. Am. J. Prev. Med. 2009, 36, 452–457. Available online: https://europepmc.org/article/pmc/2859314 (accessed on 26 September 2020). [CrossRef] [Green Version]
- Bastiaansen, D.; Koot, H.M.; Bongers, I.L.; Varni, J.W.; Verhulst, F.C. Measuring Quality of Life in Children Referred for Psychiatric Problems: Psychometric Properties of the PedsQLTM 4.0 Generic Core Scales. Qual. Life Res. 2004, 13, 489–495. Available online: https://link.springer.com/content/pdf/10.1023%2FB%3AQURE.0000018483.01526.ab.pdf (accessed on 4 March 2019). [CrossRef]
- Engelen, V.; Haentjens, M.M.; Detmar, S.B.; Koopman, H.M.; Grootenhuis, M.A. Health Related Quality of Life of Dutch Children: Psychometric Properties of the PedsQL in the Netherlands. BMC Pediatr. 2009, 9, 68. Available online: https://bmcpediatr.biomedcentral.com/articles/10.1186/1471-2431-9-68 (accessed on 24 May 2022). [CrossRef] [PubMed] [Green Version]
- Van Widenfelt, B.M.; Goedhart, A.W.; Treffers, P.D.A.; Goodman, R. Dutch Version of the Strengths and Difficulties Questionnaire (SDQ). Eur. Child Adolesc. Psychiatry 2003, 12, 281–289. Available online: http://link.springer.com/10.1007/s00787-003-0341-3 (accessed on 3 May 2020). [CrossRef] [PubMed]
- Muris, P.; Meesters, C.; van den Berg, F. The Strengths and Difficulties Questionnaire (SDQ). Eur. Child Adolesc. Psychiatry 2003, 12, 1–8. Available online: http://link.springer.com/10.1007/s00787-003-0298-2 (accessed on 3 May 2020). [CrossRef] [PubMed]
- Goodman, R. Psychometric Properties of the Strengths and Difficulties Questionnaire. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 1337–1345. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0890856709605438 (accessed on 3 May 2020). [CrossRef]
- Vogels, A.G.; Crone, M.R.; Hoekstra, F.; Reijneveld, S.A. Comparing Three Short Questionnaires to Detect Psychosocial Dysfunction among Primary School Children: A Randomized Method. BMC Public Health 2009, 9, 489. Available online: https://bmcpublichealth.biomedcentral.com/articles/10.1186/1471-2458-9-489 (accessed on 3 May 2020). [CrossRef] [Green Version]
- Teeuw, B.; Schwarzer, R.; Jerusalem, M. Dutch Adaptation of the General Self-Efficacy Scale. Berlin, Germany, 1994. Available online: http://userpage.fu-berlin.de/~health/dutch.htm (accessed on 3 May 2020).
- Luszczynska, A.; Scholz, U.; Schwarzer, R. The General Self-Efficacy Scale: Multicultural Validation Studies. J. Psychol. 2005, 139, 439–457. Available online: https://pubmed.ncbi.nlm.nih.gov/16285214/ (accessed on 13 April 2021). [CrossRef] [Green Version]
- Scholz, U.; Doña, B.G.; Sud, S.; Schwarzer, R. Is general self-efficacy a universal construct? Psychometric findings from 25 countries. Eur. J. Psychol. Assess. 2002, 18, 242–251. [Google Scholar] [CrossRef]
- Kiresuk, T.J.; Sherman, R.E. Goal Attainment Scaling: A General Method for Evaluating Comprehensive Community Mental Health Programs. Community Ment. Health J. 1968, 4, 443–453. Available online: https://pubmed.ncbi.nlm.nih.gov/24185570/ (accessed on 16 February 2021). [CrossRef]
- Stevens, A.; Beurskens, A.; Köke, A.; van der Weijden, T. The Use of Patient-Specific Measurement Instruments in the Process of Goal-Setting: A Systematic Review of Available Instruments and Their Feasibility. Clin. Rehabil. 2013, 27, 1005–1019. Available online: https://pubmed.ncbi.nlm.nih.gov/23881336/ (accessed on 16 February 2021). [CrossRef]
- Fleuren, M.A.H.; Paulussen, T.G.W.M.; Dommelen, P.; van Buuren, S. Towards a measurement instrument for determinants of innovations. Int. J. Qual. Health Care 2014, 26, 501–510. [Google Scholar] [CrossRef] [Green Version]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Guest, G.; MacQueen, K.M.; Namey, E.E. Applied Thematic Analysis; SAGE Publications: Thousand Oaks, CA, USA, 2011. [Google Scholar]
- Knorth, E.J.; Knot-Dickscheit, J.; Thoburn, J. Supporting children when providing services to families experiencing multiple problems. Int. J. Child Fam. Welf. 2015, 16, 2–10. [Google Scholar]
- Demetriou, E.A.; Lampit, A.; Quintana, D.S.; Naismith, S.L.; Song, Y.J.C.; Pye, J.E.; Hickie, I.; Guastella, A.J. Autism Spectrum Disorders: A Meta-Analysis of Executive Function. Mol. Psychiatry 2018, 23, 1198–1204. Available online: https://pubmed.ncbi.nlm.nih.gov/28439105/ (accessed on 14 September 2021). [CrossRef] [PubMed] [Green Version]
- Knight, M.J.; Baune, B.T. Cognitive Dysfunction in Major Depressive Disorder. Curr. Opin. Psychiatry 2018, 31, 26–31. Available online: https://pubmed.ncbi.nlm.nih.gov/29076892/ (accessed on 14 September 2021). [CrossRef] [PubMed]
- Cashmore, J. Promoting the Participation of Children and Young People in Care. Child Abus. Negl. 2002, 26, 837–847. Available online: https://pubmed.ncbi.nlm.nih.gov/12363334/ (accessed on 20 September 2021). [CrossRef]
- Feenstra, B.; Boland, L.; Lawson, M.L.; Harrison, D.; Kryworuchko, J.; Leblanc, M.; Stacey, D. Interventions to Support Children’s Engagement in Health-Related Decisions: A Systematic Review. BMC Pediatr. 2014, 14, 109. Available online: https://europepmc.org/article/pmc/pmc3999734 (accessed on 8 April 2021). [CrossRef] [Green Version]
- Jeremic, V.; Sénécal, K.; Borry, P.; Chokoshvili, D.; Vears, D.F. Participation of Children in Medical Decision-Making: Challenges and Potential Solutions. J. Bioethical Inq. 2016, 13, 525–534. [Google Scholar] [CrossRef]
- Jager, M. Unraveling the Role of Client-Professional Communication in Adolescent Psychosocial Care; Rijksuniversiteit Groningen: Groningen, The Netherlands, 2016. [Google Scholar]
- Forman, S.G.; Olin, S.S.; Hoagwood, K.E.; Crowe, M.; Saka, N. Evidence-Based Interventions in Schools: Developers’ Views of Implementation Barriers and Facilitators. Sch. Ment. Health 2009, 1, 26–36. Available online: www.casel.org/programs/selecting.php (accessed on 20 September 2021). [CrossRef]
- Forman, S.G.; Barakat, N.M. Cognitive-Behavioral Therapy in the Schools: Bringing Research to Practice through Effective Implementation. Psychol. Sch. 2011, 48, 283–296. Available online: https://onlinelibrary.wiley.com/doi/10.1002/pits.20547 (accessed on 20 April 2021). [CrossRef]
- Forman, S.G.; Fagley, N.S.; Chu, B.C.; Walkup, J.T. Factors Influencing School Psychologists’ “Willingness to Implement” Evidence-Based Interventions. Sch. Ment. Health 2012, 4, 207–218. Available online: https://link.springer.com/content/pdf/10.1007%2Fs12310-012-9083-z.pdf (accessed on 25 October 2018). [CrossRef]
- Bast, L.S.; Andersen, H.B.; Andersen, A.; Lauemøller, S.G.; Bonnesen, C.T.; Krølner, R.F. School Coordinators’ Perceptions of Organizational Readiness Is Associated with Implementation Fidelity in a Smoking Prevention Program: Findings from the X:IT II Study. Prev. Sci. 2021, 22, 312–323. [Google Scholar] [CrossRef] [PubMed]

| The supported education (SEd) intervention is an individualized instruction and support intervention, which aims to help people choose an education, obtain an education, and/or keep enrollment in an educational or vocational training program of their choice (Hofstra and Korevaar, 2016 [19]). In the current study, we only focus on the keep intervention. This intervention was developed to help (young) adults with mental health problems to remain in school by increasing their school success and satisfaction through the development of skills and the use of resources that are important in an educational setting. It is designed to help educational professionals (EP) who support (young) adults with mental health problems (e.g., emotional, behavioral, and/or social problems). The approach of SEd consists of: | |
| 1. Goal setting: | The starting point is determined by investigating the problems from the perspective of the student as well as the school. The educational goal of the student is determined. |
| 2. Examination of the problem and brainstorm the potential solutions: | Possible solutions to resolve the problems are examined together with the student as well as how they can reach their own educational goal. |
| 3. Description and prioritizing the necessary critical skills and resources: | a. Functional assessment: The EP investigates, together with the student, which critical skills are needed to be successful and satisfied in a chosen educational setting. What skills does the student need to deal with the limitations of the educational setting? b. Resource assessment: The EP investigates, together with the student, which critical resources are needed to be successful and satisfied in the chosen educational setting. |
| 4. Action plan: | The EP and student create an action plan together in order for the student to learn the necessary new skills and to organize the necessary critical resources. They define how these critical skills and resources are learned and organized (who, what, when, where). |
| 5. Monitor and evaluate: | Monitor and evaluate whether the plan is executed and how the execution is going. Evaluate whether the plan needs adjustment. |
| Educational Professionals (n = 8 a) | |
|---|---|
| Gender female n (%) | 7 (88%) |
| Age M(SD) | 44 (12.2) |
| Adolescents (n = 18 a) | |
| Gender female n (%) | 10 (56%) |
| Age M(SD) | 14 (1.7) |
| Grade n (%) | |
| Grade 1 | 2 (10%) |
| Grade 2 | 3 (17%) |
| Grade 3 | 6 (33%) |
| Grade 4 | 5 (28%) |
| Grade 5 | 1 (6%) |
| Grade 6 | 1 (6%) |
| Educational level n (%) | |
| Lower secondary | 9 (50%) |
| Intermediate and Higher secondary | 9 (50%) |
| T1 | T2 | T3 | |
|---|---|---|---|
| School functioning M(SD) | 69 (8.6) | 63 (11.0) | 67 (13.2) |
| SDQ M(SD) | 15 (4.0) | - | 11 (3.5) |
| General self-efficacy M(SD) | 30 (3.0) | - | 30 (1.6) |
| Improved confidence (0–10) M (SD) | - | 4.6 | 5.2 |
| Improved understanding (0–10) M (SD) | - | 6.9 | 6.5 |
| Goal Attainment Scale (GAS) | |||
| Obtained 1 or more goals n (%) | - | 4 (57%) | 5 (71%) |
| Partly obtained 1 or more goals n (%) | - | 3 (43%) | 2 (29%) |
| Themes | Informant | Supporting Quotes |
|---|---|---|
| Acceptability | ||
| Structure | EP | “The supportive tools of the intervention were very useful. I can fill it in together with the adolescent, so she/he can see what we discuss. Sometimes if you just talk to an adolescent, it doesn’t really become tangible. But if you write it down together, it sticks.” (EP4) “There are a lot of papers in the manual, and a lot of the papers contain a lot of content. It would work better if everything is written down more concise. But it does also help, to have it as a reference. It would just be nicer if we also had everything in a more concise form, to work with.” (EP3) |
| Autonomy | EP | “They’ve become more independent. More goal-oriented. Because they talk more about what they want now. And how they can take charge, and understanding that they have to do it themselves.” (EP1) “He is able to pick up things on his own now, which I think is a very important benefit of the intervention, that he sees for himself: what can I do?” (EP4) |
| Applicability | EP | “It depends on the motivation of the adolescent, and the level of thinking, and what kind of home situation they are in, if they could do these steps and benefit from it. The adolescents that could benefit are the ones that are able to talk about and name their problems.” (EP6) “I don’t think there is a difference between different school levels. You have different conversations of course. But I explain everything on their level and I do think they all have an idea of what they want. When they enjoy school or what is important to them. They can all tell me that. And they all know that good grades are important.” (EP3) “I did not use this intervention with adolescents in lower secondary education because they often need short-term solutions. To correctly use this intervention, you need at least 6 to 8 sessions.” (EP1) |
| Non-judgmental listening | Adolescent | “Some teachers just get angry and the counselor just stays calm and listens. She is friendly and honest and respectful. I feel I can trust her.” (A1) |
| Shared decision making | Adolescent | “We talked about solutions for my concentration problems, and looked at several options together. Then we tried two solutions, the counselor suggested using a stress ball and mine was listening to my mp3 player when I work on assignments in the classroom.” (A2) |
| Structure | Adolescent | “We sort of kept replaying the story: what actually happened, when was the exact point at which things went wrong, when I got angry. And then we talked about what I could do differently next time. I sort of have a strategy now. I am able to stay calm and think about the situation. Think about it step by step. And how to solve it.” (A4) |
| Visualization | Adolescent | “We wrote down on the whiteboard what I need and what I could do [...] That really makes it clear. Then I can also see what I said.” (A1) |
| Themes | Informant | Supporting Quotes |
|---|---|---|
| Implementation | ||
| Time | EP | “Educational professionals are often caught in the daily issues. Something new happens every day, and next to that, as a counselor you are caught in between various parties, internally and externally. And there is a lot more work involved if you want to do it right. I think that it is too burdensome for the time most professionals have.” (EP1) “The intervention becomes easier the more you work with it. But right now, you have to read up on the method every time, which costs time, reporting costs time, it just costs a lot of time. And we do not have that.” (EP7) |
| Personal attitude | EP | “I think EP are just used to taking care of things for adolescents. The intervention is more leaning back and I think they need to practice that. To sit back and let the adolescent do more themselves. That’s what I see happening with my colleagues.” (EP1) “I am convinced that it is so valuable if you let the adolescent think for themselves more, about their problems and the potential solutions. The adolescent being the central point in counseling is very important and I could not work differently.” (EP3) |
| Mastery | EP | “Perhaps if you are working with this method for a longer time and when it has become more of a routine, when you don’t have to prepare so much, then you can easily use this intervention. But I don’t feel like I’m there yet.” (EP4) “I tried working with the whole method, but I did skip some steps sometimes due to practical reasons. Sometimes I thought I was just repeating myself or in other cases it did not seem useful for that person. In that sense it was too extensive for me, the method. And then I chose to be flexible, to adapt it to the adolescent, and maybe skip a step.” (EP7) |
| Complexity of school environment | EP | “It is policy in our school that counseling is 7 weeks, and this intervention barely fits in those weeks. If it helped, okay, then we stop. Someone else must also get their turn. Or in some cases you continue, but only when you notice a positive effect, but haven’t seen much concrete results yet.” (EP2) “With these kind of support interventions, not just this intervention, but in general, you are very dependent on the organizational structure of the school. It is a choice of our school. We just want the kids to get support as soon and as fast as possible. And that is at the expense of this intervention, which is a more extensive method.” (EP7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beukema, L.; Hofstra, J.; Reijneveld, S.A.; de Winter, A.F.; Korevaar, E.L. Supporting Adolescents with Mental Health Problems in Secondary Education: Feasibility of a Supported Education Intervention. Int. J. Environ. Res. Public Health 2022, 19, 6754. https://doi.org/10.3390/ijerph19116754
Beukema L, Hofstra J, Reijneveld SA, de Winter AF, Korevaar EL. Supporting Adolescents with Mental Health Problems in Secondary Education: Feasibility of a Supported Education Intervention. International Journal of Environmental Research and Public Health. 2022; 19(11):6754. https://doi.org/10.3390/ijerph19116754
Chicago/Turabian StyleBeukema, Lindy, Jacomijn Hofstra, Sijmen A. Reijneveld, Andrea F. de Winter, and E. L. Korevaar. 2022. "Supporting Adolescents with Mental Health Problems in Secondary Education: Feasibility of a Supported Education Intervention" International Journal of Environmental Research and Public Health 19, no. 11: 6754. https://doi.org/10.3390/ijerph19116754