
Association between Thyroid Cancer and Weight Change: A Longitudinal Follow-Up Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
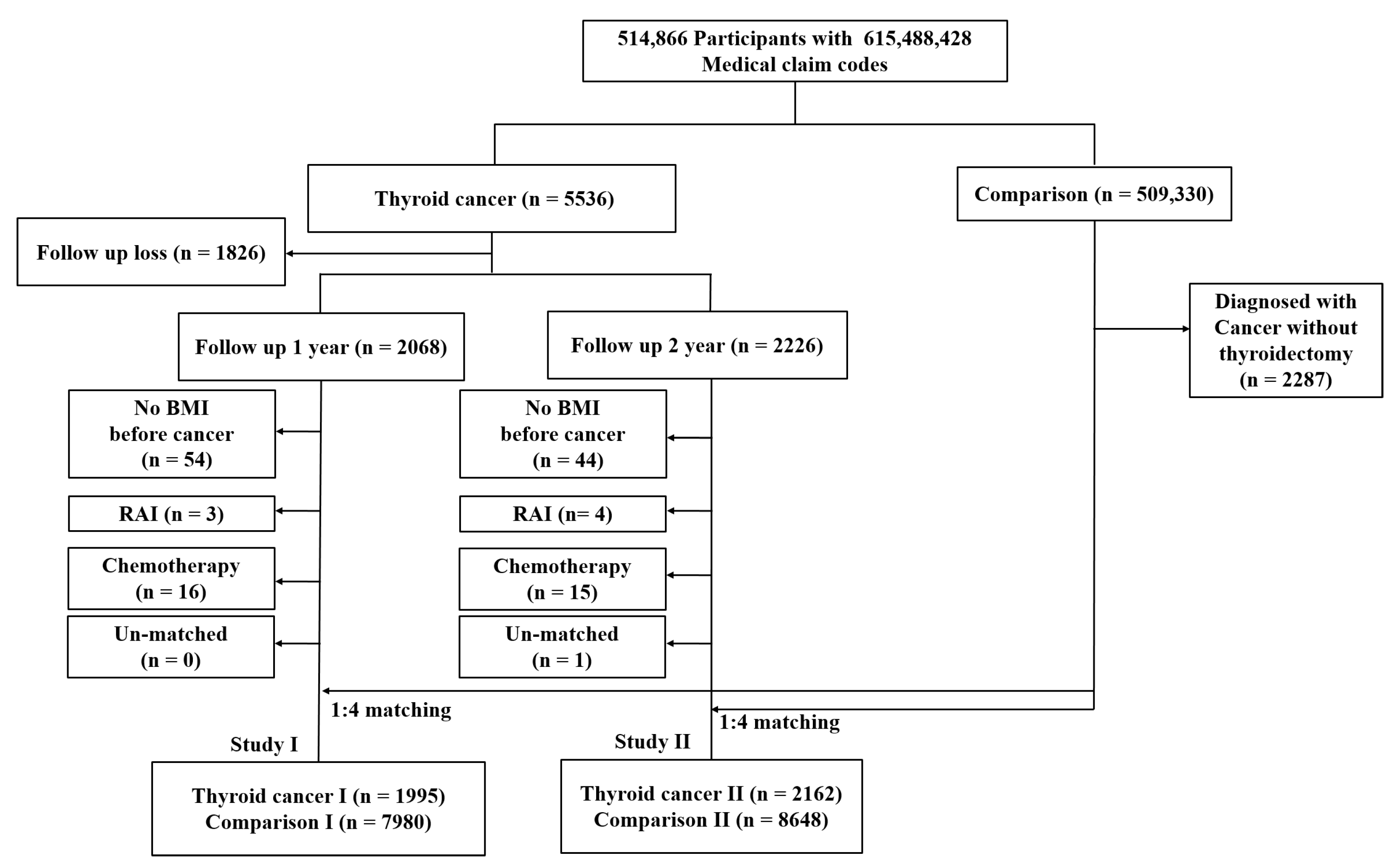
2.1. Study Population
2.2. Definition of Thyroid Cancer (Independent Variable)
2.3. Definition of Weight Change (Dependent Variable)
2.4. Definition of Blood Pressure Change (Dependent Variable)
2.5. Participant Selection
2.6. Covariates
2.7. Statistical Analyses
3. Results
Detailed Descriptions
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Blüher, M. Obesity: Global epidemiology and pathogenesis. Nat. Rev. Endocrinol. 2019, 15, 288–298. [Google Scholar] [CrossRef] [PubMed]
- Mills, K.T.; Stefanescu, A.; He, J. The global epidemiology of hypertension. Nat. Rev. Nephrol. 2020, 16, 223–237. [Google Scholar] [CrossRef] [PubMed]
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef] [Green Version]
- Ma, J.; Huang, M.; Wang, L.; Ye, W.; Tong, Y.; Wang, H. Obesity and risk of thyroid cancer: Evidence from a meta-analysis of 21 observational studies. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2015, 21, 283. [Google Scholar]
- Sharma, A.M.; Padwal, R. Obesity is a sign–over-eating is a symptom: An aetiological framework for the assessment and management of obesity. Obes. Rev. 2010, 11, 362–370. [Google Scholar] [CrossRef]
- Davies, L.; Welch, H.G. Current thyroid cancer trends in the United States. JAMA Otolaryngol. Head Neck Surg. 2014, 140, 317–322. [Google Scholar] [CrossRef] [Green Version]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: The American Thyroid Association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [Green Version]
- Kim, B. Thyroid hormone as a determinant of energy expenditure and the basal metabolic rate. Thyroid 2008, 18, 141–144. [Google Scholar] [CrossRef]
- Pearce, E.N. Thyroid hormone and obesity. Curr. Opin. Endocrinol. Diabetes Obes. 2012, 19, 408–413. [Google Scholar] [CrossRef]
- Huynh, C.N.; Pearce, J.V.; Kang, L.; Celi, F.S. Weight gain after thyroidectomy: A systematic review and meta-analysis. J. Clin. Endocrinol. Metab. 2021, 106, 282–291. [Google Scholar] [CrossRef]
- Jonklaas, J.; Nsouli-Maktabi, H. Weight changes in euthyroid patients undergoing thyroidectomy. Thyroid 2011, 21, 1343–1351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rotondi, M.; Croce, L.; Pallavicini, C.; La Manna, L.; Accornero, S.M.; Fonte, R.; Magri, F.; Chiovato, L. Body weight changes in a large cohort of patients subjected to thyroidectomy for a wide spectrum of thyroid diseases. Endocr. Pract. 2014, 20, 1151–1158. [Google Scholar] [CrossRef] [PubMed]
- Polotsky, H.N.; Brokhin, M.; Omry, G.; Polotsky, A.J.; Tuttle, R.M. Iatrogenic hyperthyroidism does not promote weight loss or prevent ageing-related increases in body mass in thyroid cancer survivors. Clin. Endocrinol. 2012, 76, 582–585. [Google Scholar] [CrossRef] [PubMed]
- Kedia, R.; Lowes, A.; Gillis, S.; Markert, R.; Koroscil, T. Iatrogenic Subclinical Hyperthyroidism Does Not Promote Weight Loss. South. Med. J. 2016, 109, 97–100. [Google Scholar] [CrossRef]
- Weinreb, J.T.; Yang, Y.; Braunstein, G.D. Do patients gain weight after thyroidectomy for thyroid cancer? Thyroid 2011, 21, 1339–1342. [Google Scholar] [CrossRef]
- Berta, E.; Lengyel, I.; Halmi, S.; Zrínyi, M.; Erdei, A.; Harangi, M.; Páll, D.; Nagy, E.V.; Bodor, M. Hypertension in thyroid disorders. Front. Endocrinol. 2019, 10, 482. [Google Scholar] [CrossRef] [Green Version]
- Lin, S.-Y.; Huang, S.-C.; Sheu, W.H.-H. Circulating adiponectin concentrations were related to free thyroxine levels in thyroid cancer patients after thyroid hormone withdrawal. Metabolism 2010, 59, 195–199. [Google Scholar] [CrossRef]
- An, S.-Y.; Kim, S.Y.; Oh, D.J.; Min, C.; Sim, S.; Choi, H.G. Obesity is positively related and tobacco smoking and alcohol consumption are negatively related to an increased risk of thyroid cancer. Sci. Rep. 2020, 10, 19279. [Google Scholar] [CrossRef]
- Choi, H.G.; Park, B.; Ji, Y.B.; Tae, K.; Song, C.M. Depressive disorder in thyroid cancer patients after thyroidectomy: A longitudinal follow-up study using a national cohort. Otolaryngol. Head Neck Surg. 2019, 160, 239–245. [Google Scholar] [CrossRef]
- Quan, H.; Li, B.; Couris, C.M.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.-M.; Sundararajan, V. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef] [Green Version]
- Kyriacou, A.; Kyriacou, A.; Makris, K.C.; Syed, A.A.; Perros, P. Weight gain following treatment of hyperthyroidism—A forgotten tale. Clin. Obes. 2019, 9, e12328. [Google Scholar] [CrossRef] [PubMed]
- Dale, J.; Daykin, J.; Holder, R.; Sheppard, M.; Franklyn, J. Weight gain following treatment of hyperthyroidism. Clin. Endocrinol. 2001, 55, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Tigas, S.; Idiculla, J.; Beckett, G.; Toft, A. Is excessive weight gain after ablative treatment of hyperthyroidism due to inadequate thyroid hormone therapy? Thyroid 2000, 10, 1107–1111. [Google Scholar] [CrossRef] [PubMed]
- Glick, R.; Chang, P.; Michail, P.; Serpell, J.W.; Grodski, S.; Lee, J.C. Body weight change is unpredictable after total thyroidectomy. ANZ J. Surg. 2018, 88, 162–166. [Google Scholar] [CrossRef] [PubMed]
- Klok, M.D.; Jakobsdottir, S.; Drent, M. The role of leptin and ghrelin in the regulation of food intake and body weight in humans: A review. Obes. Rev. 2007, 8, 21–34. [Google Scholar] [CrossRef]
- Gazdag, A.; Nagy, E.; Erdei, A.; Bodor, M.; Berta, E.; Szabó, Z.; Jenei, Z. Aortic stiffness and left ventricular function in patients with differentiated thyroid cancer. J. Endocrinol. Investig. 2015, 38, 133–142. [Google Scholar] [CrossRef] [Green Version]
- Ancker, O.V.; Wehland, M.; Bauer, J.; Infanger, M.; Grimm, D. The adverse effect of hypertension in the treatment of thyroid cancer with multi-kinase inhibitors. Int. J. Mol. Sci. 2017, 18, 625. [Google Scholar] [CrossRef] [Green Version]
- Cho, H.-R.; Song, R.-Y.; Kang, K.H. Weight change in patients with differentiated thyroid carcinoma after total thyroidectomy versus lobectomy. Korean J. Clin. Oncol. 2020, 16, 127–130. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Study I | Study II | |||||
|---|---|---|---|---|---|---|---|
| Thyroid Cancer I | Comparison I | p-Value | Thyroid Cancer II | Comparison II | p-Value | ||
| Age (years old, n, %) | 1.000 | 1.000 | |||||
| 40–44 | 29 (1.5) | 116 (1.5) | 46 (2.1) | 184 (2.1) | |||
| 45–49 | 345 (17.3) | 1380 (17.3) | 328 (15.2) | 1312 (15.2) | |||
| 50–54 | 593 (29.7) | 2372 (29.7) | 748 (34.6) | 2992 (34.6) | |||
| 55–59 | 559 (28.0) | 2236 (28.0) | 482 (22.3) | 1928 (22.3) | |||
| 60–64 | 224 (11.2) | 896 (11.2) | 287 (13.3) | 1148 (13.3) | |||
| 65–69 | 154 (7.7) | 616 (7.7) | 139 (6.4) | 556 (6.4) | |||
| 70–74 | 63 (3.2) | 252 (3.2) | 109 (5.0) | 436 (5.0) | |||
| 75–79 | 26 (1.3) | 104 (1.3) | 18 (0.8) | 72 (0.8) | |||
| 80–84 | 2 (0.1) | 8 (0.1) | 5 (0.2) | 20 (0.2) | |||
| Sex (n, %) | 1.000 | 1.000 | |||||
| Male | 512 (25.7) | 2048 (25.7) | 510 (23.6) | 2040 (23.6) | |||
| Female | 1483 (74.3) | 5932 (74.3) | 1652 (76.4) | 6608 (76.4) | |||
| Income (n, %) | 1.000 | 1.000 | |||||
| 1 (lowest) | 262 (13.1) | 1048 (13.1) | 257 (11.9) | 1028 (11.9) | |||
| 2 | 284 (14.2) | 1136 (14.2) | 248 (11.5) | 992 (11.5) | |||
| 3 | 314 (15.7) | 1256 (15.7) | 344 (15.9) | 1376 (15.9) | |||
| 4 | 338 (16.9) | 1352 (16.9) | 430 (19.9) | 1720 (19.9) | |||
| 5 (highest) | 797 (40.0) | 3188 (40.0) | 883 (40.8) | 3532 (40.8) | |||
| Region of residence (n, %) | 1.000 | 1.000 | |||||
| Urban | 953 (47.8) | 3812 (47.8) | 1058 (48.9) | 4232 (48.9) | |||
| Rural | 1042 (52.2) | 4168 (52.2) | 1104 (51.1) | 4416 (51.1) | |||
| Obesity ‡ | 1.000 | 1.000 | |||||
| Underweight | 20 (1.0) | 80 (1.0) | 31 (1.4) | 124 (1.4) | |||
| Normal | 668 (33.5) | 2672 (33.5) | 725 (33.5) | 2900 (33.5) | |||
| Overweight | 571 (28.6) | 2284 (28.6) | 631 (29.2) | 2524 (29.2) | |||
| Obese I | 662 (33.2) | 2648 (33.2) | 687 (31.8) | 2748 (31.8) | |||
| Obese II | 74 (3.7) | 296 (3.7) | 88 (4.1) | 352 (4.1) | |||
| Smoking status (n, %) | <0.001 * | 0.018 * | |||||
| Nonsmoker | 1712 (85.8) | 6601 (82.7) | 1872 (86.6) | 7327 (84.7) | |||
| Past smoker | 166 (8.3) | 661 (8.3) | 154 (7.1) | 620 (7.2) | |||
| Current smoker | 117 (5.9) | 718 (9.0) | 136 (6.3) | 701 (8.1) | |||
| Alcohol consumption (n, %) | 0.124 | 0.102 | |||||
| <1 time a week | 1556 (78.0) | 6094 (76.4) | 1723 (79.7) | 6752 (78.1) | |||
| ≥1 time a week | 439 (22.0) | 1886 (23.6) | 439 (20.3) | 1896 (21.9) | |||
| Fasting blood glucose (n, %) | 0.447 | 0.078 | |||||
| <100 mg/dL | 1386 (69.5) | 5508 (69.0) | 1533 (70.9) | 5936 (68.6) | |||
| 100–125 mg/dL | 497 (24.9) | 1963 (24.6) | 510 (23.6) | 2151 (24.9) | |||
| ≥126 mg/dL | 112 (5.6) | 509 (6.4) | 119 (5.5) | 561 (6.5) | |||
| Total cholesterol (n, %) | 0.059 | 0.002 * | |||||
| <200 mg/dL | 1073 (53.8) | 4059 (50.9) | 1157 (53.5) | 4263 (49.3) | |||
| 200–239 mg/dL | 657 (32.9) | 2763 (34.6) | 716 (33.1) | 3066 (35.5) | |||
| ≥240 mg/dL | 265 (13.3) | 1158 (14.5) | 289 (13.4) | 1319 (15.3) | |||
| CCI score (n, %) | <0.001 * | <0.001 * | |||||
| 0 | 1270 (63.7) | 6440 (80.7) | 1374 (63.6) | 6988 (80.8) | |||
| 1 | 314 (15.7) | 916 (11.5) | 336 (15.5) | 998 (11.5) | |||
| 2 | 94 (4.7) | 334 (4.2) | 127 (5.9) | 357 (4.1) | |||
| 3 | 36 (1.8) | 144 (1.8) | 35 (1.6) | 151 (1.8) | |||
| ≥4 | 281 (14.1) | 146 (1.8) | 290 (13.4) | 154 (1.8) | |||
| Systolic blood pressure (mean, SD) | 123.95 ± 15.38 | 123.33 ± 15.90 | 0.116 | 123.77 ± 15.16 | 123.47 ± 15.78 | 0.430 | |
| Diastolic blood pressure (mean, SD) | 77.38 ± 10.21 | 76.77 ± 10.51 | 0.019 † | 77.46 ± 10.06 | 76.86 ± 10.35 | 0.017 † | |
| Characteristics | Thyroid Cancer I | Comparison I | Interaction ‡ | Linear Mixed Model ¶ | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Previous (Mean, SD) | Post 1 yr (Mean, SD) | p-Value | Previous (Mean, SD) | Post 1 yr (Mean, SD) | p-Value | p-Value | EV § | p-Value | ||
| Total participants (n = 9975) | ||||||||||
| BMI | 24.26 ± 2.97 | 24.19 ± 3.05 | 0.020 | 24.22 ± 2.94 | 24.21 ± 2.94 | 0.262 | 0.245 | 0.029 | 0.691 | |
| SBP | 123.95 ± 15.38 | 123.45 ± 14.20 | 0.152 | 123.33 ± 15.90 | 123.36 ± 15.02 | 0.880 | 0.423 | −0.299 | 0.214 | |
| DBP | 77.38 ± 10.21 | 76.88 ± 9.63 | 0.043 | 76.77 ± 10.51 | 76.57 ± 9.85 | 0.106 | 0.837 | 0.325 | 0.044 † | |
| Age < 55 years old, men (n = 1365) | ||||||||||
| BMI | 24.57 ± 2.52 | 24.60 ± 2.65 | 0.656 | 24.60 ± 2.74 | 24.57 ± 2.64 | 0.488 | 0.598 | −0.021 | 0.906 | |
| SBP | 124.15 ± 13.92 | 122.77 ± 13.29 | 0.127 | 125.20 ± 14.52 | 124.47 ± 14.65 | 0.104 | 0.172 | −1.493 | 0.012 † | |
| DBP | 79.27 ± 9.92 | 78.86 ± 10.21 | 0.532 | 79.77 ± 10.11 | 79.03 ± 10.00 | 0.027 | 0.209 | 0.152 | 0.710 | |
| Age < 55 years old, women (n = 3470) | ||||||||||
| BMI | 23.59 ± 2.93 | 23.58 ± 2.97 | 0.867 | 23.57 ± 2.79 | 23.62 ± 2.85 | 0.015 * | 0.187 | 0.019 | 0.871 | |
| SBP | 120.19 ± 13.90 | 120.42 ± 14.26 | 0.688 | 119.18 ± 15.23 | 119.56 ± 14.13 | 0.176 | 0.868 | 0.152 | 0.688 | |
| DBP | 75.43 ± 9.85 | 75.52 ± 9.69 | 0.827 | 74.71 ± 10.50 | 74.90 ± 9.69 | 0.345 | 0.931 | 0.191 | 0.458 | |
| Age ≥ 55 years old, men (n = 1195) | ||||||||||
| BMI | 24.95 ± 2.73 | 24.86 ± 2.67 | 0.296 | 24.96 ± 2.69 | 24.83 ± 2.70 | <0.001 * | 0.461 | −0.002 | 0.990 | |
| SBP | 127.86 ± 14.79 | 126.24 ± 13.23 | 0.090 | 127.68 ± 15.50 | 127.66 ± 15.08 | 0.965 | 0.613 | −1.112 | 0.127 | |
| DBP | 80.13 ± 9.37 | 78.50 ± 8.78 | 0.018 | 79.44 ± 10.30 | 78.92 ± 9.66 | 0.159 | 0.694 | 0.684 | 0.187 | |
| Age ≥ 55 years old, women (n = 3945) | ||||||||||
| BMI | 24.52 ± 3.12 | 24.37 ± 3.26 | 0.003 * | 24.45 ± 3.09 | 24.41 ± 3.11 | 0.069 | 0.119 | 0.065 | 0.594 | |
| SBP | 126.00 ± 16.55 | 125.51 ± 14.23 | 0.397 | 125.02 ± 16.27 | 125.01 ± 15.17 | 0.982 | 0.934 | −0.041 | 0.921 | |
| DBP | 77.61 ± 10.53 | 76.89 ± 9.43 | 0.079 | 76.73 ± 10.28 | 76.48 ± 9.67 | 0.200 | 0.712 | 0.426 | 0.115 | |
| Characteristics | Thyroid Cancer II | Comparison II | Interaction ‡ | Linear Mixed Model ¶ | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Previous (Mean, SD) | Post 2 yr (Mean, SD) | p-Value | Previous (Mean, SD) | Post 2 yr (Mean, SD) | p-Value | p-Value | EV § | p-Value | ||
| Total participants (n = 10,810) | ||||||||||
| BMI | 24.22 ± 2.93 | 24.15 ± 3.00 | 0.016 | 24.23 ± 2.99 | 24.21 ± 3.03 | 0.130 | 0.300 | −0.005 | 0.937 | |
| SBP | 123.77 ± 15.16 | 123.44 ± 14.36 | 0.338 | 123.47 ± 15.78 | 123.45 ± 15.26 | 0.934 | 0.978 | −0.370 | 0.123 | |
| DBP | 77.46 ± 10.06 | 76.73 ± 9.34 | 0.002 * | 76.86 ± 10.35 | 76.41 ± 9.91 | <0.001 * | 0.724 | 0.493 | 0.002 † | |
| Age < 55 years old, men (n = 1430) | ||||||||||
| BMI | 24.81 ± 2.65 | 24.88 ± 2.85 | 0.328 | 24.85 ± 2.67 | 24.81 ± 2.70 | 0.219 | 0.151 | −0.012 | 0.943 | |
| SBP | 124.16 ± 14.33 | 123.66 ± 13.13 | 0.557 | 125.36 ± 13.70 | 125.50 ± 14.33 | 0.750 | 0.259 | −0.726 | 0.218 | |
| DBP | 80.03 ± 10.14 | 78.27 ± 9.55 | 0.005 * | 79.69 ± 10.01 | 79.41 ± 9.59 | 0.388 | 0.040 | 1.088 | 0.009 † | |
| Age < 55 years old, women (n = 4180) | ||||||||||
| BMI | 23.67 ± 2.96 | 23.68 ± 2.96 | 0.810 | 23.64 ± 2.99 | 23.66 ± 3.02 | 0.340 | 0.700 | −0.005 | 0.967 | |
| SBP | 121.52 ± 15.17 | 121.34 ± 14.18 | 0.745 | 119.43 ± 14.81 | 119.79 ± 14.50 | 0.162 | 0.244 | 0.391 | 0.262 | |
| DBP | 75.90 ± 9.91 | 75.92 ± 9.28 | 0.958 | 74.81 ± 10.16 | 74.81 ± 9.81 | 0.992 | 0.263 | −0.041 | 0.865 | |
| Age ≥ 55 years old, men (n = 1120) | ||||||||||
| BMI | 24.76 ± 2.58 | 24.63 ± 2.66 | 0.139 | 24.85 ± 2.72 | 24.75 ± 2.74 | 0.024 | 0.758 | −0.074 | 0.708 | |
| SBP | 126.48 ± 13.73 | 125.26 ± 12.00 | 0.236 | 128.92 ± 15.70 | 127.42 ± 14.65 | 0.011 * | 0.909 | −1.473 | 0.063 | |
| DBP | 79.13 ± 9.77 | 77.94 ± 8.40 | 0.011 * | 80.17 ± 10.06 | 78.55 ± 9.51 | <0.001 * | 0.585 | 0.263 | 0.615 | |
| Age ≥ 55 years old, women (n = 4080) | ||||||||||
| BMI | 24.45 ± 3.00 | 24.25 ± 3.10 | <0.001 * | 24.45 ± 3.06 | 24.41 ± 3.13 | 0.121 | 0.015 † | 0.007 | 0.953 | |
| SBP | 125.20 ± 15.53 | 125.02 ± 15.27 | 0.757 | 125.45 ± 16.47 | 125.40 ± 15.74 | 0.868 | 0.561 | −0.715 | 0.092 | |
| DBP | 77.69 ± 10.00 | 76.69 ± 9.50 | 0.011 * | 77.07 ± 10.25 | 76.42 ± 9.88 | <0.001 * | 0.464 | 0.779 | 0.004 † | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jin, Y.J.; Hah, J.H.; Kwon, M.J.; Kim, J.H.; Kim, J.-H.; Kim, S.-K.; Park, B.; Choi, H.G. Association between Thyroid Cancer and Weight Change: A Longitudinal Follow-Up Study. Int. J. Environ. Res. Public Health 2022, 19, 6753. https://doi.org/10.3390/ijerph19116753
Jin YJ, Hah JH, Kwon MJ, Kim JH, Kim J-H, Kim S-K, Park B, Choi HG. Association between Thyroid Cancer and Weight Change: A Longitudinal Follow-Up Study. International Journal of Environmental Research and Public Health. 2022; 19(11):6753. https://doi.org/10.3390/ijerph19116753
Chicago/Turabian StyleJin, Young Ju, Jeong Hun Hah, Mi Jung Kwon, Ji Hee Kim, Joo-Hee Kim, Sung-Kyun Kim, Bumjung Park, and Hyo Geun Choi. 2022. "Association between Thyroid Cancer and Weight Change: A Longitudinal Follow-Up Study" International Journal of Environmental Research and Public Health 19, no. 11: 6753. https://doi.org/10.3390/ijerph19116753