
Influence of Sit-Stand Tables in Classrooms on Children’s Sedentary Behavior and Teacher’s Acceptance and Feasibility: A Mixed-Methods Study


Abstract
:1. Introduction
2. Materials and Methods
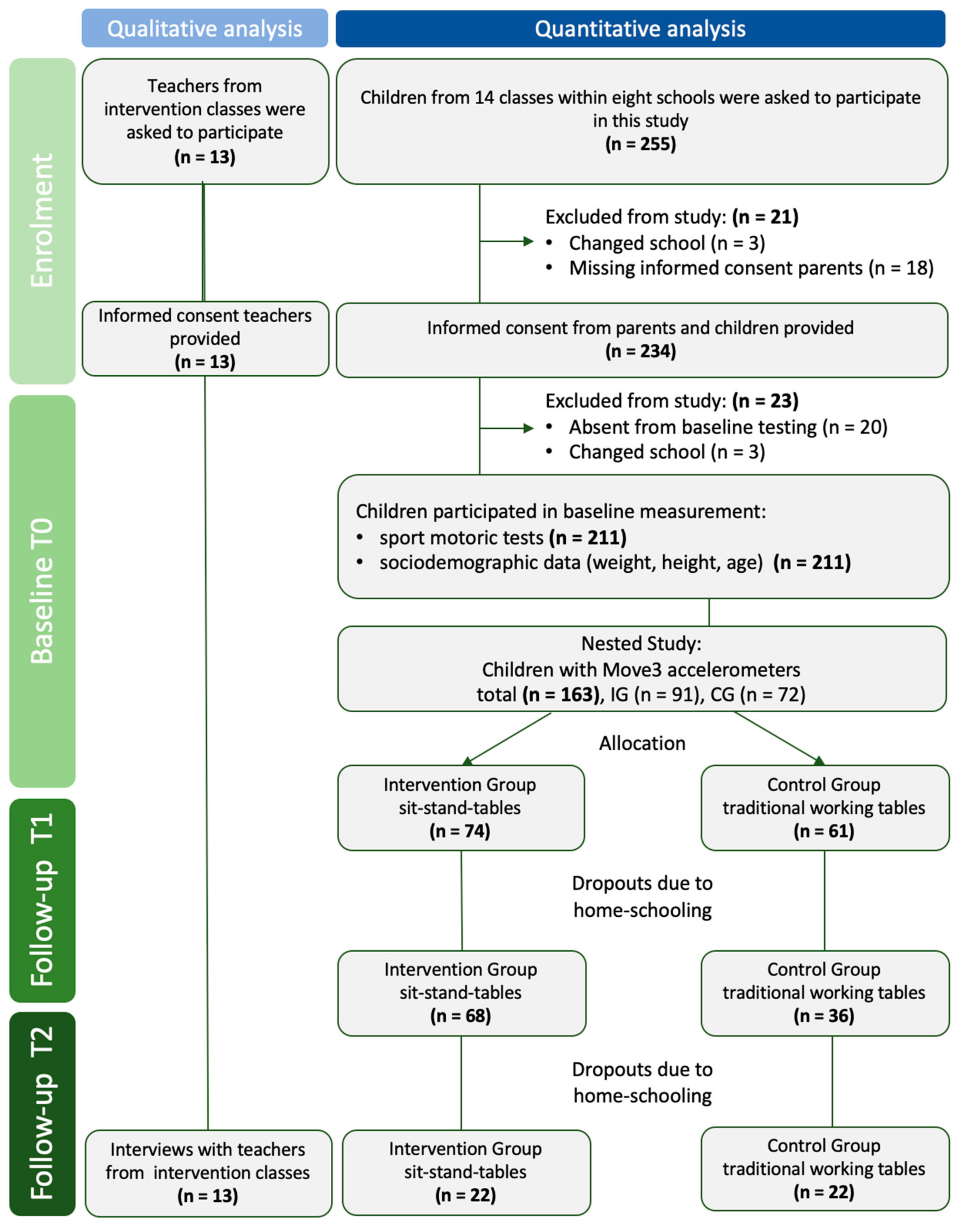
2.1. Study Design
2.2. Intervention
2.3. Study Sample and Participants
3. Measurements and Data Collection
3.1. Quantitative Data
3.2. Qualitative Data
4. Statistical Analyses
4.1. Quantitative Data
4.2. Qualitative Data
5. Results
5.1. Sample Characteristics
5.2. Sitting and Standing Time
5.3. Association of Sedentary Behaviour Regarding Sex, BMI, Sport Activities (Outside the School Setting) and Fitness Level
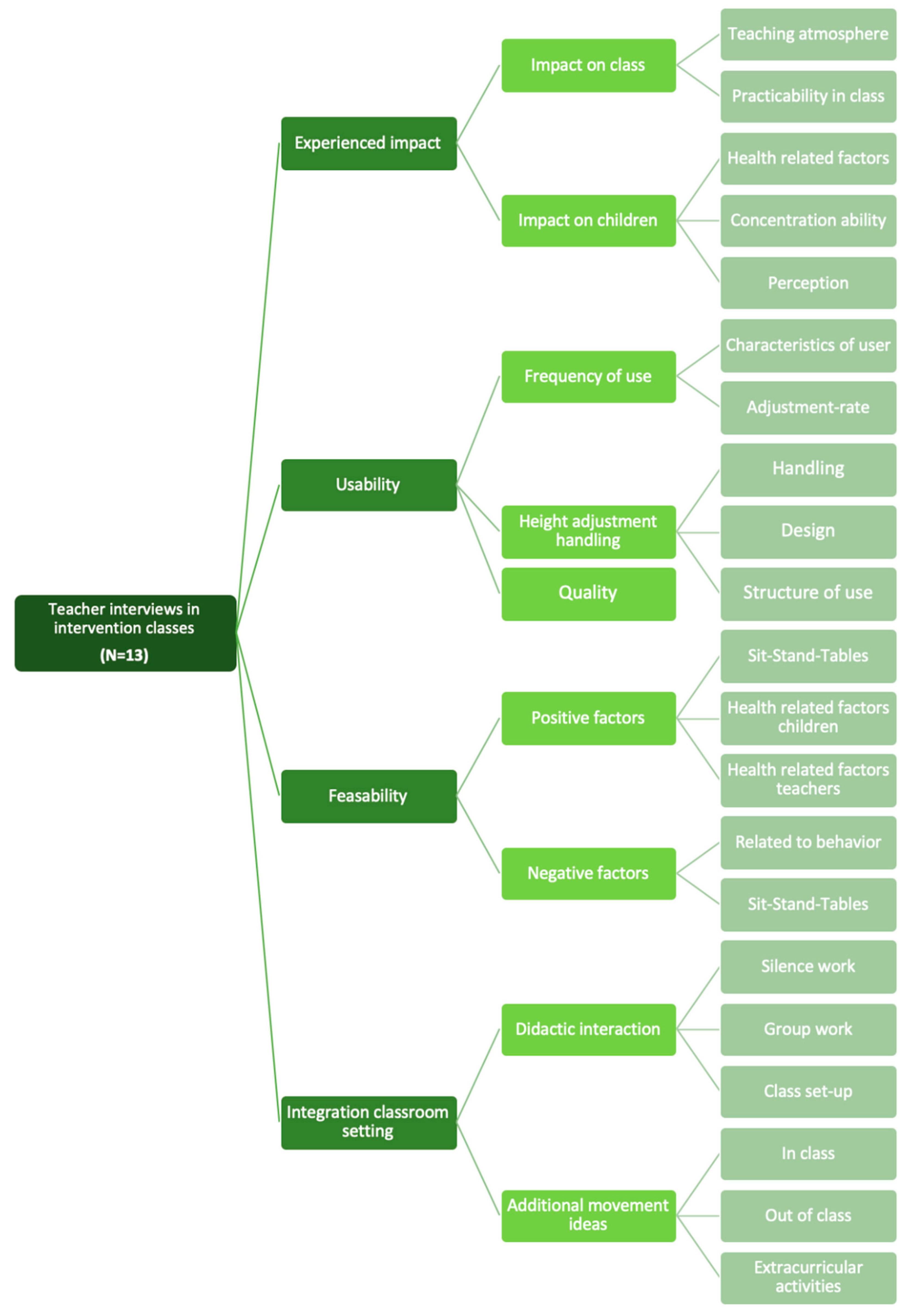
5.4. Results from the Teachers’ Perspective in Intervention Group
5.5. Impact from the Teachers’ Perspective
5.6. Usability from the Teachers’ Perspective
5.7. Feasibility from the Teachers’ Perspective
5.8. Integration in Classroom Setting
6. Discussion
Limitations and Strengths
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Variables | Intervention Group | Control Group | ||
|---|---|---|---|---|
| Primary School | Secondary School | Primary School | Secondary School | |
| Minimum Maximum | Minimum Maximum | Minimum Maximum | Minimum Maximum | |
| Sitting T0 | 14.01 | 22.20 | 35.10 | 44.27 |
| 41.66 | 40.29 | 44.37 | 45.40 | |
| Standing T0 | 3.64 | 4.88 | 0.73 | 0.00 |
| 31.49 | 23.20 | 10.10 | 1.13 | |
| Sitting T1 | 22.72 | 33.40 | 32.41 | 41.48 |
| 43.24 | 40.40 | 44.75 | 45.20 | |
| Standing T1 | 2.19 | 5.05 | 0.58 | 0.30 |
| 22.71 | 11.93 | 12.97 | 3.64 | |
| Sitting T2 | 13.27 | - | 37.37 | - |
| 41.50 | - | 45.50 | - | |
| Standing T2 | 4.00 | - | 0.00 | - |
| 32.39 | - | 8.12 | - | |
| Sitting | 13.27 | 22.20 | 32.41 | 41.48 |
| 43.24 | 40.40 | 45.50 | 45.40 | |
| Standing | 2.19 | 4.88 | 0.00 | 0.00 |
| 32.39 | 23.20 | 12.97 | 3.64 | |
References
- Dobbins, M.; Husson, H.; DeCorby, K.; LaRocca, R. School-based physical activity programs for promoting physical activity and fitness in children and adolescents aged 6 to 18. Cochrane Database Syst. Rev. 2013, 2013, CD007651. [Google Scholar] [CrossRef] [PubMed]
- Janssen, X.; Mann, K.D.; Basterfield, L.; Parkinson, K.N.; Pearce, M.S.; Reilly, J.K.; Adamson, A.J.; Reilly, J.J. Development of sedentary behavior across childhood and adolescence: Longitudinal analysis of the Gateshead Millennium Study. Int. J. Behav.Nutr. Phys. Act. 2016, 13, 88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, H. Obesity prevention programs for children and youth: Why are their results so modest? Health Educ. Res. 2006, 21, 783–795. [Google Scholar] [CrossRef] [PubMed]
- Benden, M.; Zhao, H.; Jeffrey, C.; Wendel, M.; Blake, J. The Evaluation of the Impact of a Stand-Biased Desk on Energy Expenditure and Physical Activity for Elementary School Students. Int. J. Environ. Res. Public Health 2014, 11, 9361–9375. [Google Scholar] [CrossRef] [Green Version]
- Hjorth, M.; Chaput, J.; Damsgaard, C.; Dalskov, S.; Andersen, R.; Astrup, A.; Michaelsen, K.F.; Tetens, I.; Ritz, C.; Sjödin, A. Low physical activity level and short sleep duration are associated with an increased cardio-metabolic risk profile: A longitudinal study in 8–11 year old Danish children. PLoS ONE 2014, 9, e104677. [Google Scholar] [CrossRef]
- Dumuid, D.; Stanford, T.E.; Pedisic, Z.; Maher, C.; Lewis, L.; Martin-Fernandez, J.; Olds, T. Adiposity and the isotemporal substitution of physical activity, sedentary time and sleep among school-aged children: A compositional data analysis approach. BMC Public Health 2018, 18, 311. [Google Scholar] [CrossRef]
- McGill, S. The biomechanics of low back injury: Implications on current practice in industry and the clinic. J. Biomech. 1997, 30, 465–475. [Google Scholar] [CrossRef]
- Hussain, S.; Urquhart, D.; Wang, Y.; Dunstan, D.; Shaw, J.; Magliano, D.; Cicuttini, F. Associations between television viewing and physical activity and low back pain in community-based adults: A cohort study. Medicine 2016, 95, e3963. [Google Scholar] [CrossRef]
- Tremblay, M.; LeBlanc, A.G.; Kho, M.E.; Saunders, T.J.; Larouche, R.; Colley, R.C.; Goldfield, G.; Gorber, S.C. Systematic review of sedentary behaviour and health indicators in school-aged children and youth. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 98. [Google Scholar] [CrossRef] [Green Version]
- Maher, C.; Lewis, L.; Katzmarzyk, P.; Dumuid, D.; Cassidy, L.; Olds, T. The associations between physical activity, sedentary behaviour and academic performance. J. Sci. Med. Sport 2016, 19, 1004–1009. [Google Scholar] [CrossRef]
- McPherson, A.; Mackay, L.; Kunkel, J.; Duncan, S. Physical activity, cognition and academic performance: An analysis of mediating and confounding relationships in primary school children. BMC Public Health 2018, 18, 936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guthold, R.; Stevens, G.; Riley, M.; Bull, F. Global trends in insufficient physical activity among adolescents: A pooled analysis of 298 population-based surveys with 1·6 million participants. Lancet Child Adolesc. Health 2019, 4, 23–35. [Google Scholar] [CrossRef]
- Sudholz, B.; Timperio, A.; Ridgers, N.; Dunstan, D.; Baldock, R.; Holland, B.; Salmon, J. The Impact and Feasibility of Introducing Height-Adjustable Desks on Adolescents’ Sitting in a Secondary School Classroom. AIMS Public Health 2016, 3, 274–287. [Google Scholar] [CrossRef] [PubMed]
- Ucci, M.; Law, S.; Andrews, R.; Fisher, A.; Smith, L.; Sawyer, A.; Marmot, A. Indoor school environments, physical activity, sitting behaviour and pedagogy: A scoping review. Build. Res. Inf. 2015, 43, 566–581. [Google Scholar] [CrossRef]
- Parrish, A.; Okely, A.; Stanley, R.; Ridgers, N. The effect of school recess interventions on physical activity: A systematic review. Sport Med. 2013, 43, 287–299. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, M.; Carson, V.; Chaput, J.-P.; Gorber, S.C.; Dinh, T.; Duggan, M.; Faulkner, G.; Gray, C.E.; Gruber, R.; Janson, K.; et al. Canadian 24-h movement guidelines for children and youth: An Integration of Physical Activity, Sedentary Behaviour, and Sleep. Appl. Physiol. Nutr. Metab. 2016, 41, S311–S327. [Google Scholar] [CrossRef] [PubMed]
- Salmon, J.; Tremblay, M.S.; Marshall, S.J.; Hume, C. Health risks, correlates, and interventions to reduce sedentary behavior in young people. Am. J. Prev. Med. 2011, 41, 197–206. [Google Scholar] [CrossRef]
- Carson, V.; Hunter, S.; Kuzik, N.; Gray, C.E.; Poitras, V.J.; Chaput, J.-P.; Saunders, T.J.; Katzmarzyk, P.T.; Okely, A.D.; Gorber, S.C.; et al. Systematic review of sedentary behaviour and health indicators in school-aged children and youth: An update. Appl. Physiol. Nutr. Metab. 2016, 41, S240–S265. [Google Scholar] [CrossRef]
- Healy, G.; Dunstan, D.; Salmon, J.; Cerin, E.; Shaw, J.; Zimmet, P.; Owen, N. Breaks in sedentary time: Beneficial associations with metabolic risk. Diabetes Care 2008, 31, 661–666. [Google Scholar] [CrossRef] [Green Version]
- Drenowatz, C.; Eisenmann, J.; Pfeiffer, K.; Welk, G.; Heelan, K.; Gentile, D.; Walsh, D. Influence of socio-economic status on habitual physical activity and sedentary behaviorin 8- to 11-year old children. BMC Public Health 2010, 10, 214. [Google Scholar] [CrossRef] [Green Version]
- Salmon, J. Novel strategies to promote children’s physical activities and reduce sedentary behavior. Phys. Act. Health 2010, 7 (Suppl. S3), S299–S306. [Google Scholar] [CrossRef] [PubMed]
- Haapala, E.; Väistö, J.; Lintu, N.; Westgate, K.; Ekelund, U.; Poikkeus, A.-M.; Brage, S.; Lakka, T. Physical activity and sedentary time in relation to academic achievement in children. J. Sci. Med. Sport 2017, 20, 583–589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lanningham-Foster, L.; Foster, R.C.; McCrady, S.K.; Manohar, C.U.; Jensen, T.B.; Mitre, N.G.; Hill, J.O.; Levine, J.A. Changing the school environment to increase physical activity in children. Obesity 2008, 16, 1849–1853. [Google Scholar] [CrossRef] [PubMed]
- Lopes, L.; Santos, R.; Mota, J.; Pereira, B.; Lopes, V. Objectively measured sedentary time and academic achievement in schoolchildren. J. Sports Sci. 2017, 35, 463–469. [Google Scholar] [CrossRef] [Green Version]
- Colley, R.; Garriguet, D.; Janssen, I.; Craig, C.L.; Clarke, J.; Tremblay, M.S. Physical activity of Canadian children and youth: Accelerometer results from the 2007 to 2009 Canadian Health Measures Survey. Health Rep. 2011, 22, 15–23. [Google Scholar] [PubMed]
- Giurgiu, M.; Koch, E.; Ottenbacher, J.; Plotnikoff, R.C.; Ebner-Priemer, U.W.; Reichert, M. Sedentary behavior in everyday life relates negatively to mood: An Ambulatory Assessment study. Scand. J. Med. Sci. Sports 2019, 29, 1340–1351. [Google Scholar] [CrossRef] [PubMed]
- Minges, K.; Chao, A.; Irwin, M.; Park, C.; Whittemore, R.; Salmon, J. Classroom Standing Desks and Sedentary Behavior: A Systematic Review. Pediatrics 2016, 137, e20153087. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Tolfrey, K.; Pearson, N.; Bingham, D.; Edwardson, C.; Cale, L.; Dunstan, D.; Barber, S.; Clemes, S. Stand Out in Class: Investigating the Potential Impact of a Sit–Stand Desk Intervention on Children’s Sitting and Physical Activity during Class Time and after School. Int. J. Environ. Res. Public Health 2021, 18, 4759. [Google Scholar] [CrossRef]
- Koskelo, R.; Vuorikari, K.; Hänninen, O. Sitting and standing postures are corrected by adjustable furniture with lowered muscle tension in high-school students. Ergonomics 2007, 50, 1643–1656. [Google Scholar] [CrossRef]
- Kromeyer-Hauschild, K.; Wabitsch, M.; Kunze, D.; Geller, F.; Geiß, H.C.; Hesse, V.; von Hippel, A.; Jaeger, U.; Johnsen, D.; Korte, W.; et al. Perzentile fuür den Body-mass-Index fuür das Kindes- und Jugendalter unter Heranziehung verschiedener deutscher Stichproben. Mon. Kinderheilkd 2001, 149, 807–818. [Google Scholar] [CrossRef] [Green Version]
- Bös, K. Deutscher Motorik-Test 6-18 (DMT 6-18); Feldhaus: Hamburg, Germany, 2016; ISBN 978-3-88020-643-4. [Google Scholar]
- Movisens GmbH. FZI Forschungszentrum Informatik, Karlsruhe. Move 3 Sensor. 2018. Available online: www.movisens.com (accessed on 19 April 2022).
- Movisens GmbH. FZI Forschungszentrum Informatik, Karlsruhe. Sensor Manager. Version 1.15.7. Available online: www.movisens.com (accessed on 19 April 2022).
- Movisens GmbH. FZI Forschungszentrum Informatik, Karlsruhe. UnisensViewer. GPL 3.0 license. Available online: www.movisens.com (accessed on 19 April 2022).
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- IBM Corp. Released 2020. IBM SPSS Statistics, Version 27.0.0 Armonk, NY: IBM Corp91022091USEN-04. Available online: www.ibm.com/support/pages/downloading-ibm-spss-statistics-27 (accessed on 19 April 2022).
- Mayring, P. Qualitative Inhaltsanalyse. In Grundlagen und Techniken, 12th ed.; Beltz Verlag: Weinheim, Germany; Basel, Switzerland, 2015. [Google Scholar]
- Kuckartz, U. Qualitative Inhaltsanalyse. In Methoden, Praxis, Computerunterstützung; Beltz Verlag: Weinheim, Germany; Basel, Switzerland, 2012. [Google Scholar]
- Clemes, S.; Barber, S.; Bingham, D.; Ridgers, N.; Fletcher, E.; Pearson, N.; Salmon, J.; Dunstan, D. Reducing children’s classroom sitting time using sit-to-stand desks: Findings from pilot studies in UK and Australian primary schools. J. Public Health 2015, 38, 526–533. [Google Scholar] [CrossRef] [PubMed]
- Verloigne, M.; Ridgers, N.; De Bourdeaudhuij, I.; Cardon, G. Effect and process evaluation of implementing standing desks in primary and secondary schools in Belgium: A cluster-randomised controlled trial. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 94. [Google Scholar] [CrossRef] [PubMed]
- Blake, J.; Benden, M.; Wendel, M. Using stand/sit workstations in classrooms: Lessons learned from a pilot study in Texas. J. Public Health Manag. Pract. 2012, 18, 412–415. [Google Scholar] [CrossRef] [PubMed]
- Hinckson, E.; Aminian, S.; Ikeda, E.; Stewart, T.; Oliver, M.; Duncan, S.; Schofield, G. Acceptability of standing workstations in elementary schools: A pilot study. Prev. Med. 2013, 56, 82–85. [Google Scholar] [CrossRef]
- Gabel, L.; Ridgers, N.; Della Gatta, P.; Arundell, L.; Cerin, E.; Robinson, S.; Daly, E.M.; Dunstan, D.W.; Salmon, J. Associations of sedentary time patterns and TV viewing time with inflammatory and endothelial function biomarkers in children. Pediatr. Obes. 2015, 11, 194–201. [Google Scholar] [CrossRef]
- Mehta, R.; Shortz, A.; Benden, M. Standing Up for Learning: A Pilot Investigation on the Neurocognitive Benefits of Stand-Biased School Desks. Int. J. Environ. Res. Public Health 2015, 13, 59. [Google Scholar] [CrossRef] [Green Version]
- Mazzoli, E.; Teo, W.; Salmon, J.; Pesce, C.; He, J.; Ben-Soussan, T.; Barnett, L. Associations of Class-Time Sitting, Stepping and Sit-to-Stand Transitions with Cognitive Functions and Brain Activity in Children. Int. J. Environ. Res. Public Health 2019, 16, 1482. [Google Scholar] [CrossRef] [Green Version]
- Syvaoja, H.; Tammelin, T.H.; Ahonen, T.; Kankaanpää, A.; Kantomaa, M.T. The Associations of Objectively Measured Physical Activity and Sedentary Time with Cognitive Functions in School-Aged Children. PLoS ONE 2014, 9, e103559. [Google Scholar] [CrossRef] [Green Version]
- Aminian, S.; Hinckson, E.; Stewart, T. Modifying the classroom enviroment to increase standing and reducing sitting. Build. Res. Inf. 2015, 43, 631–645. [Google Scholar] [CrossRef]
- Hinckson, E.; Salmon, J.; Benden, M.; Clemes, S.A.; Sudholz, B.; Barber, S.; Ridgers, N. Standing classrooms: Research and lessons learned from around the world. Sports Med. 2016, 46, 977–987. [Google Scholar] [CrossRef] [PubMed]
- Erwin, H.; Beighle, A.; Routen, A.; Montemayor, B. Perceptions of Using Sit-to-Stand Desks in a Middle School Classroom. Youth Health 2018, 19, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Kirschner, M.; Golsteijn, R.H.J.; Sijben, S.M.; Singh, A.S.; Savelberg, H.H.C.M.; de Groot, R.H.M. A Qualitative Study of the Feasibility and Acceptability of Implementing ‘Sit-To-Stand’ Desks in Vocational Education and Training. Int. J. Environ. Res. Public Health 2021, 18, 849. [Google Scholar] [CrossRef] [PubMed]
- Ayala, A.; Salmon, J.; Timperio, A.; Sudholz, B.; Ridgers, N.; Sethi, P.; Dunstan, D. Impact of an 8-Month Trial Using Height-Adjustable Desks on Children’s Classroom Sitting Patterns and Markers of Cardio-Metabolic and Musculoskeletal Health. Int. J. Environ. Res. Public Health 2016, 13, 1227. [Google Scholar] [CrossRef] [PubMed]
- Swartz, A.; Tokarek, N.; Lisdahl, K.; Maeda, H.; Strath, S.; Cho, C. Do Stand-Biased Desks in the Classroom Change School-Time Activity and Sedentary Behavior? Int. J. Environ. Res. Public Health 2019, 16, 933. [Google Scholar] [CrossRef] [Green Version]
- Krampen, G. Kaseler-Konzentrations-Aufgabe für 3- bis 8-Jährige, KKA; Hogrefe Verlag: Göttingen, Germany, 2007. [Google Scholar]
- Brickenkamp, R.; Schmidt-Atzert, L.; Liepmann, D. Aufmerksamkeits- und Konzentrationstest, d2-r; Hogrefe Verlag: Göttingen, Germany, 2010. [Google Scholar]



| School | Number of Participating Children Per School (n) | Primary School (P) Secondary School (S) | Location: Munich (M) Metropolitan Area (MA) | Number of Classes Participating in Study (n) | Schools Included in Nested Study (P) | Allocation to IG and CG *: Mixed Classes (M) Separated Classes (S) | Number of Interviewed Teachers from Intervention Classes (n) |
|---|---|---|---|---|---|---|---|
| 1 | 31 | P | M | 2 | P | S | 1 |
| 2 | 34 | P | M | 2 | P | S | 1 |
| 3 | 29 | P | M | 2 | P | S | 1 |
| 4 | 34 | P, S | M | 3 | P | M | 3 |
| 5 | 16 | S | MA | 1 | P | M | 1 |
| 6 | 14 | S | MA | 1 | - | M | 2 |
| 7 | 32 | S | MA | 2 | - | M | 3 |
| 8 | 21 | P | MA | 1 | - | M | 1 |
| Total | 211 | 5 primary classes (n = 139 children) 4 secondary classes (n = 72 children) | 4 schools in Munich (n = 128 children) 4 schools in metropolitan area of Munich (n = 83 children) | 14 | 5 schools taking part in nested study | 3 schools with one intervention and one control class 5 schools with mixed classes ** | 13 |
| Characteristics | All | Intervention | Control | |||
|---|---|---|---|---|---|---|
| N (211) | %/Mean (SD) | n (98) | %/Mean (SD) | n (113) | %/Mean (SD) | |
| Sex | ||||||
| Female | 89 | 42.2 | 40 | 40.8 | 49 | 43.4 |
| Male | 122 | 57.8 | 58 | 59.2 | 63 | 56.6 |
| Age | 9.06 (1.70) | 8.85 (1.79) | 9.24 (1.61) | |||
| 7 | 39 | 18.5 | 25 | 25.5 | 14 | 12.4 |
| 8 | 69 | 32.7 | 32 | 32.7 | 37 | 32.7 |
| 9 | 21 | 10.0 | 11 | 11.2 | 10 | 8.8 |
| 10 | 34 | 16.1 | 9 | 9.2 | 25 | 22.1 |
| 11 | 26 | 12.3 | 9 | 9.2 | 17 | 15.0 |
| 12 | 15 | 7.1 | 8 | 8.2 | 7 | 6.2 |
| 13 | 7 | 3.3 | 4 | 4.1 | 3 | 2.7 |
| Schools | ||||||
| Primary School | 139 | 65.9 | 80 | 81.6 | 59 | 52.2 |
| Secondary School | 72 | 34.1 | 18 | 18.4 | 54 | 47.8 |
| Grade | ||||||
| 2 | 75 | 35.5 | 51 | 52.0 | 24 | 21.2 |
| 3 | 52 | 24.6 | 17 | 17.3 | 35 | 31.0 |
| 4 | 12 | 5.7 | 12 | 12.2 | 0 | 0 |
| 5 | 49 | 23.2 | 10 | 10.2 | 39 | 34.5 |
| 6 | 23 | 10.9 | 8 | 8.2 | 15 | 13.3 |
| BMI Percentiles | ||||||
| Extreme Underweight (<3) | 5 | 2.4 | 0 | 0 | 5 | 4.4 |
| Underweight (3–15) | 18 | 8.5 | 10 | 10.2 | 8 | 7.1 |
| Normal weight (15–85) | 128 | 60.7 | 58 | 59.2 | 70 | 61.9 |
| Overweight (85–97) | 33 | 15.6 | 13 | 13.3 | 20 | 17.7 |
| Obesity (>97) | 27 | 12.8 | 17 | 17.3 | 10 | 8.8 |
| Sport activities (outside the school setting) | ||||||
| No | 76 | 36.0 | 47 | 48.0 | 29 | 25.7 |
| Yes | 135 | 64.0 | 51 | 52.0 | 84 | 74.3 |
| Fitness Level * | ||||||
| Low (<30) | 16 | 7.6 | 14 | 14.3 | 2 | 1.8 |
| Normal (30–70) | 173 | 82.0 | 76 | 77.6 | 97 | 85.8 |
| High (>70) | 22 | 10.4 | 8 | 8.2 | 14 | 12.4 |
| School | Grade | Intervention Group | Control Group | t-test (a) | ||||
|---|---|---|---|---|---|---|---|---|
| n | M (SD) | n | M (SD) | 95%-CI | p-Value | |||
| 1 | 3 | Time sitting | 17 | 35.75 (3.73) | 14 | 42.30 (1.11) | 4.56, 8.54 | <0.001 |
| Time standing | 9.61 (3.78) | 2.91 (1.10) | −8.71, −4.68 | <0.001 | ||||
| 2 | 2 | Time sitting | 22 | 32.26 (3.68) | 12 | 40.97 (3.26) | 6.12, 11.30 | <0.001 |
| Time standing | 13.25 (3.69) | 4.36 (3.23) | −11.47, −6.30 | <0.001 | ||||
| 3 | 3 | Time sitting | 17 | 35.65 (2.81) | 12 | 40.15 (1.23) | 2.91, 6.09 | <0.001 |
| Time standing | 9.64 (2.83) | 5.25 (1.19) | −5.97, −2.80 | <0.001 | ||||
| 4 | 2 | Time sitting | 11 | 37.58 (2.26) | 8 | 40.27 (1.61) | 1.11, 4.48 | 0.003 |
| Time standing | 7.70 (2.20) | 5.17 (1.60) | −4.06, −0.83 | 0.006 | ||||
| 4 | Time sitting | 9 | 37.87 (1.51) | 8 | 41.53 (1.68) | 1.63, 5.16 | 0.001 | |
| Time standing | 7.55 (1.48) | 3.91 (1.88) | −4.95, −1.38 | 0.002 | ||||
| 5 | Time sitting | 10 | 37.57 (2.53) | 10 | 44.36 (0.95) | 5.16, 8.24 | <0.001 | |
| Time standing | 7.76 (2.58) | 1.13 (0.92) | −8.11, −5.01 | <0.001 | ||||
| 5 | 6 | Time sitting | 5 | 32.94 (7.57) | 8 | 44.91 (0.47) | 2.57, 21.37 | 0.024 |
| Time standing | 13.12 (6.93) | 0.44 (0.48) | −21.28, −4.10 | 0.015 | ||||
| Primary Schools | 2, 3, 4 | Time sitting | 76 | 35.82 (3.89) | 54 | 41.04 (2.21) | 4.54, 6.81 | <0.001 |
| Time standing | 9.55 (3.95) | 4.32 (2.22) | −6.90, −4.60 | <0.001 | ||||
| Secondary Schools | 5, 6 | Time sitting | 15 | 35.26 (1.60) | 18 | 44.64 (0.71) | 7.12, 10.30 | <0.001 |
| Time standing | 10.44 (1.60) | 0.79 (0.70) | −10.74; −7.42 | <0.001 | ||||
| Total | 2–6 | Time sitting | 91 | 35.54 (3.96) | 72 | 42.84 (2.21) | 6.05, 8.26 | <0.001 |
| Time standing | 9.99 (4.01) | 2.55 (2.22) | −8.35, −6.12 | <0.001 | ||||
| Intervention Group | Control Group | t-test (a) | |||||
|---|---|---|---|---|---|---|---|
| n | M (SD) | n | M (SD) | 95%-CI | p-Value | ||
| Sex | |||||||
| Female | Time sitting | 34 | 36.02 (3.58) | 16 | 41.35 (2.42) | (−1.75, 1.23) | 0.72 |
| Time standing | 9.34 (3.63) | 3.93 (2.40) | (−1.20, 1.80) | 0.68 | |||
| Male | Time sitting | 52 | 36.05 (4.23) | 22 | 41.09 (2.10) | (−1.71, 1.79) | 0.97 |
| Time standing | 9.34 (4.27) | 4.23 (2.14) | (−1.77, 1.77) | 0.99 | |||
| BMI Percentiles | |||||||
| Extreme Underweight (<3) | Time sitting | 0 | - | 2 | 40.60 (0.75) | (−5.42, 2.96) | 0.46 |
| Time standing | - | 5.05 (0.26) | (−1.35, 4.64) | 0.19 | |||
| Underweight (3–15) | Time sitting | 8 | 36.80 (3.33) | 4 | 41.83 (1.96) | - | - |
| Time standing | 8.58 (3.40) | 3.40 (1.92) | - | - | |||
| Normal weight (15–85) | Time sitting | 51 | 35.78 (3.96) | 24 | 40.99 (2.30) | (−2.40, 2.37) | 0.99 |
| Time standing | 9.59 (4.01) | 4.28 (2.33) | (−2.48, 2.34) | 0.95 | |||
| Overweight (85–97) | Time sitting | 11 | 37.12 (3.15) | 5 | 41.01 (2.72) | (−3.89, 1.22) | 0.30 |
| Time standing | 8.25 (3.19) | 4.35 (2.68) | (−1.25, 3.92) | 0.31 | |||
| Obesity (>97) | Time sitting | 16 | 35.74 (4.85) | 3 | 42.73 (1.83) | - | - |
| Time standing | 9.66 (4.87) | 2.61 (1.85) | - | - | |||
| Sport activities (outside the school setting) | fx | ||||||
| No | Time sitting | 44 | 36.47 (3.55) | 8 | 41.96 (2.48) | (−0.82, 2.74) | 0.28 |
| Time standing | 8.92 (3.60) | 3.37 (2.55) | (−2.72, 0.86) | 0.30 | |||
| Yes | Time sitting | 42 | 35.59 (4.35) | 30 | 40.10 (2.13) | (−0.83, 2.57) | 0.31 |
| Time standing | 9.78 (4.40) | 4.30 (2.13) | (−2.57, 0.87) | 0.33 | |||
| Fitness Level | |||||||
| Low (<30) | Time sitting | 12 | 39.49 (2.01) | 1 | 44.52 (0.0) | (−1.25, 7.79) | 0.15 |
| Time standing | 5.87 (1.95) | 0.81 (0.0) | (−7.79, 1.31) | 0.16 | |||
| Normal (30–70) | Time sitting | 67 | 35.81 (3.72) | 33 | 41.25 (2.18) | (−1.00, 3.64) | 0.001 |
| Time standing | 9.57 (3.76) | 4.06 (2.20) | (−3,64, 1.04) | 0.001 | |||
| High (>70) | Time sitting | 7 | 32.36 (4.8) | 4 | 39.94 (1.86) | (0.42, 6.46) | 0.026 |
| Time standing | 13.11 (4.86) | 5.35 (1.93) | (−6.61, −0.49) | 0.024 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schwenke, P.; Coenen, M. Influence of Sit-Stand Tables in Classrooms on Children’s Sedentary Behavior and Teacher’s Acceptance and Feasibility: A Mixed-Methods Study. Int. J. Environ. Res. Public Health 2022, 19, 6727. https://doi.org/10.3390/ijerph19116727
Schwenke P, Coenen M. Influence of Sit-Stand Tables in Classrooms on Children’s Sedentary Behavior and Teacher’s Acceptance and Feasibility: A Mixed-Methods Study. International Journal of Environmental Research and Public Health. 2022; 19(11):6727. https://doi.org/10.3390/ijerph19116727
Chicago/Turabian StyleSchwenke, Paula, and Michaela Coenen. 2022. "Influence of Sit-Stand Tables in Classrooms on Children’s Sedentary Behavior and Teacher’s Acceptance and Feasibility: A Mixed-Methods Study" International Journal of Environmental Research and Public Health 19, no. 11: 6727. https://doi.org/10.3390/ijerph19116727