
Characteristics of Hospitals Employing Dentists, and Utilization of Dental Care Services for Hospitalized Patients in Japan: A Nationwide Cross-Sectional Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
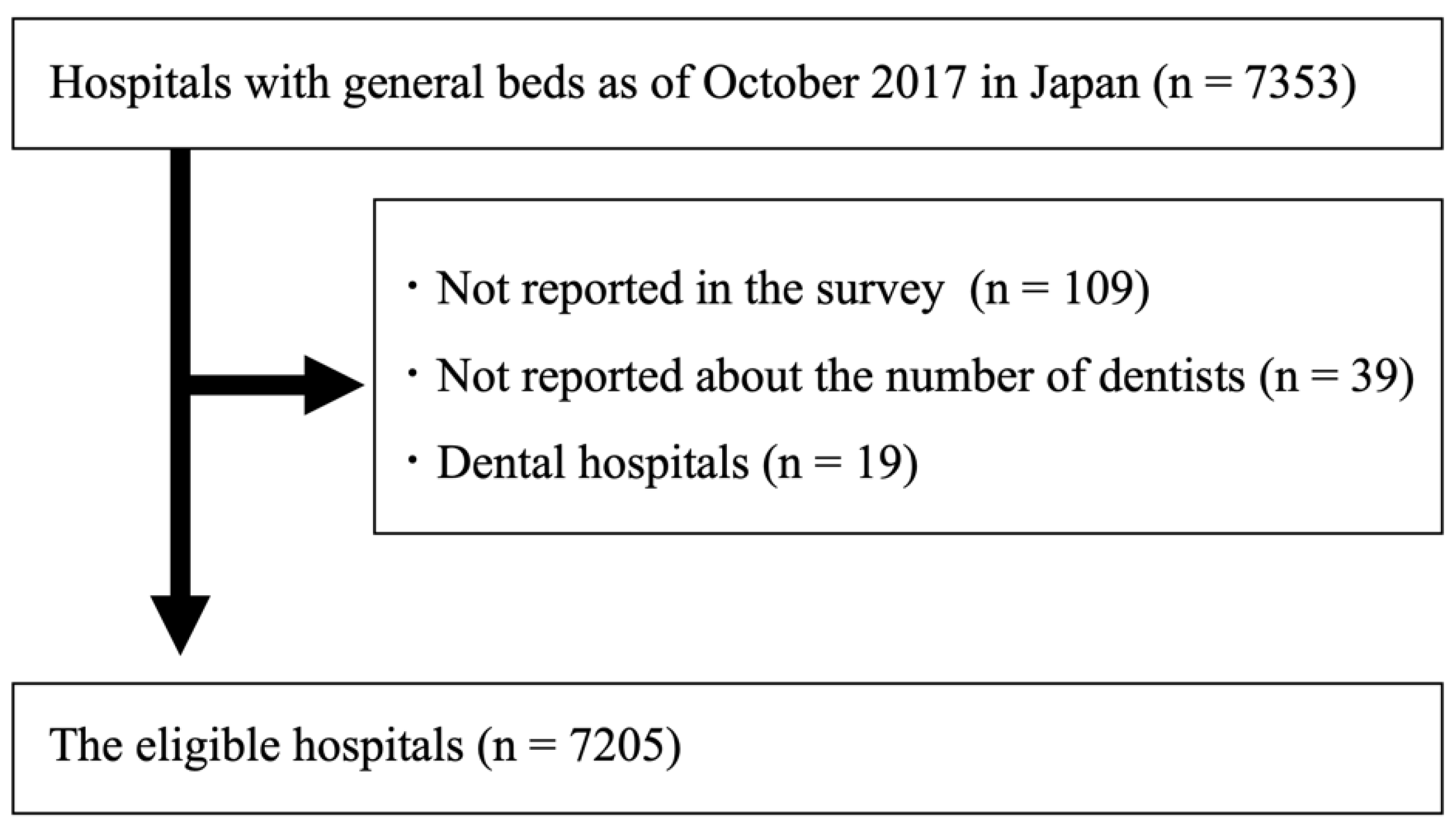
2.2. Inclusion and Exclusion Criteria
2.3. Variables
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ishimaru, M.; Matsui, H.; Ono, S.; Hagiwara, Y.; Morita, K.; Yasunaga, H. Preoperative Oral Care and Effect on Postoperative Complications after Major Cancer Surgery. Br. J. Surg. 2018, 105, 1688–1696. [Google Scholar] [CrossRef] [PubMed]
- Bergan, E.H.; Tura, B.R.; Lamas, C.C. Impact of Improvement in Preoperative Oral Health on Nosocomial Pneumonia in a Group of Cardiac Surgery Patients: A Single Arm Prospective Intervention Study. Intensive Care Med. 2014, 40, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Bellissimo-Rodrigues, W.T.; Menegueti, M.G.; Gaspar, G.G.; Nicolini, E.A.; Auxiliadora-Martins, M.; Basile-Filho, A.; Martinez, R.; Bellissimo-Rodrigues, F. Effectiveness of a Dental Care Intervention in the Prevention of Lower Respiratory Tract Nosocomial Infections among Intensive Care Patients: A Randomized Clinical Trial. Infect. Control Hosp. Epidemiol. 2014, 35, 1342–1348. [Google Scholar] [CrossRef] [PubMed]
- Abbott, C.A.; Dremsa, T.; Stewart, D.W.; Mark, D.D.; Swift, C.C. Adoption of a Ventilator-Associated Pneumonia Clinical Practice Guideline. Worldviews Evid. Based Nurs. 2006, 3, 139–152. [Google Scholar] [CrossRef] [PubMed]
- Hua, F.; Xie, H.; Worthington, H.V.; Furness, S.; Zhang, Q.; Li, C. Oral Hygiene Care for Critically Ill Patients to Prevent Ventilator-Associated Pneumonia. Cochrane Database Syst. Rev. 2016, 10, CD008367. [Google Scholar] [CrossRef] [PubMed]
- Shiraishi, A.; Yoshimura, Y.; Wakabayashi, H.; Tsuji, Y.; Yamaga, M.; Koga, H. Hospital Dental Hygienist Intervention Improves Activities of Daily Living, Home Discharge and Mortality in Post-Acute Rehabilitation. Geriatr. Gerontol. Int. 2019, 19, 189–196. [Google Scholar] [CrossRef] [PubMed]
- The Japan Dental Association. The Survey of the Collaboration between Medical and Dental Care in Hospitals. Available online: https://www.jda.or.jp/jda/research_organization/pdf/kikou_chousa20180316.pdf?180409 (accessed on 30 March 2020).
- Koike, K.; Shiba, M.; Kamata, T.; Nakahara, H.; Isomura, E.; Hamada, S. Survey Research Concerning the Current Status of Oral Functions and Oral Healthcare Management Targeting Inpatients in General Hospitals. J. Jpn. Stomatol. Soc. 2020, 69, 179–189. [Google Scholar]
- Rozenfeld, M.; Bodas, M.; Shani, M.; Radomislensky, I.; Israel, A.; Israeli, A.; Peleg, K. Introduction of hospital quality measures may lead to a temporary decrease in patient outcomes. Public Health 2021, 200, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Salampessy, B.H.; Portrait, F.R.M.; van der Hijden, E.; Klink, A.; Koolman, X. On the correlation between outcome indicators and the structure and process indicators used to proxy them in public health care reporting. Eur. J. Health Econ. 2021, 22, 1239–1251. [Google Scholar] [CrossRef] [PubMed]
- The Administrative Reports on Hospital Bed Function in 2017. The Ministry of Health, Labour, and Welfare; (In Japanese). Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/open_data_00002.html (accessed on 20 May 2020).
- Okamoto, E. An Analysis of the Conversion of Wards into Different Functions Using the Administrative Reports on Hospital Bed Function by Ward Matching Technique. J. Jpn. Assoc. Health Care Admin. 2020, 14, 29–36. [Google Scholar]
- Yasunaga, H. Real World Data in Japan: Chapter II The Diagnosis Procedure Combination Database. Ann. Clin. Epidemiol. 2019, 1, 76–79. [Google Scholar] [CrossRef]
- Hayashida, K.; Murakami, G.; Matsuda, S.; Fushimi, K. History and Profile of Diagnosis Procedure Combination (DPC): Development of a Real Data Collection System for Acute Inpatient Care in Japan. J. Epidemiol. 2021, 31, 1–11. [Google Scholar] [CrossRef]
- Morioka, N.; Tomio, J.; Seto, T.; Kobayashi, Y. The Association between Higher Nurse Staffing Standards in the Fee Schedules and the Geographic Distribution of Hospital Nurses: A Cross-Sectional Study Using Nationwide Administrative Data. BMC Nurs. 2017, 16, 25. [Google Scholar] [CrossRef] [Green Version]
- Sekiya, H.; Kurasawa, Y.; Maruoka, Y.; Mukohyama, H.; Negishi, A.; Shigematsu, S.; Sugizaki, J.; Ohashi, M.; Hasegawa, S.; Kobayashi, Y.; et al. Cost-Effectiveness Analysis of Perioperative Oral Management after Cancer Surgery and an Examination of the Reduction in Medical Costs Thereafter: A Multicenter Study. Int. J. Environ. Res. Public Health 2021, 18, 7453. [Google Scholar] [CrossRef]
- Toyokawa, S.; Kobayashi, Y. Increasing Supply of Dentists Induces Their Geographic Diffusion in Contrast with Physicians in Japan. Soc. Sci. Med. 2010, 71, 2014–2019. [Google Scholar] [CrossRef]
- Morita, T.; Tanimoto, T.; Morita, M.; Tsubokura, M.; Kami, M. Trend in Unequal Geographical Distribution of Doctors by Age and Sex in Japan from 2004 to 2014. Public Health 2018, 159, 95–98. [Google Scholar] [CrossRef] [PubMed]
- Length of Hospital Stay. OECD Health Data, 2020. Available online: https://data.oecd.org/healthcare/length-of-hospital-stay.htm (accessed on 20 May 2022).
- Admission, Number 1. The Ministry of Health, Labour, and Welfare; (In Japanese). Available online: https://www.mhlw.go.jp/content/12404000/000823126.pdf (accessed on 20 May 2022).
- Moore, L.; Lavoie, A.; Bourgeois, G.; Lapointe, J. Donabedian’s structure-process-outcome quality of care model: Validation in an integrated trauma system. J. Trauma Acute Care Surg. 2015, 78, 1168–1175. [Google Scholar] [CrossRef]
- Hibbert, P.D.; Molloy, C.J.; Wiles, L.K.; Cameron, I.D.; Gray, L.C.; Reed, R.L.; Kitson, A.; Georgiou, A.; Gordon, S.J.; Westbrook, J.; et al. Designing clinical indicators for common residential aged care conditions and processes of care: The CareTrack Aged development and validation study. Int. J. Qual. Health Care 2022, 34, mzac033. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hospital with Dentists | Hospital without Dentists | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Total | Nutrition Support Team Including Dentists | Nutrition Support Team Including Dentists | |||||||
| N | n | (%) | n | (%) | N | (%) | n | (%) | |
| N | 7205 | 1584 | (22.0) | 324 | (20.5) | 5621 | (78.0) | 50 | (0.9) |
| Hospital factors | |||||||||
| DPC type (%) | |||||||||
| Group I | 82 | 82 | (100.0) | 37 | (45.1) | 0 | (0.0) | - | - |
| Group II | 140 | 113 | (80.7) | 55 | (48.7) | 27 | (19.3) | 2 | (7.4) |
| Group III | 1442 | 595 | (41.3) | 198 | (33.3) | 847 | (58.7) | 37 | (4.4) |
| Non-DPC | 5541 | 794 | (14.3) | 34 | (4.3) | 4747 | (85.7) | 11 | (0.2) |
| Establisher of hospitals (%) | |||||||||
| The Japanese government | 226 | 133 | (58.8) | 32 | (24.1) | 93 | (41.2) | 3 | (3.2) |
| University | 162 | 127 | (78.4) | 43 | (33.9) | 35 | (21.6) | 0 | 0.0 |
| Public organizations | 1166 | 486 | (41.7) | 146 | (30.0) | 680 | (58.3) | 10 | (1.5) |
| Social insurance-related organizations | 53 | 26 | (49.1) | 8 | (30.8) | 27 | (50.9) | 3 | (11.1) |
| Medical corporations | 4722 | 605 | (12.8) | 63 | (10.4) | 4117 | (87.2) | 27 | (0.7) |
| Other corporations | 577 | 165 | (28.6) | 25 | (15.2) | 412 | (71.4) | 4 | (1.0) |
| Others | 299 | 42 | (14.0) | 7 | (16.7) | 257 | (86.0) | 3 | (1.2) |
| Regional medical care support hospital | 554 | 342 | (61.7) | 147 | (43.0) | 212 | (38.3) | 13 | (6.1) |
| Emergency hospital | 3770 | 1073 | (28.5) | 299 | (27.9) | 2697 | (71.5) | 46 | (1.7) |
| Recovery rehabilitation hospital | 735 | 114 | (15.5) | 6 | (5.3) | 621 | (84.5) | 1 | (0.2) |
| Long-term care hospital | 1729 | 238 | (13.8) | 3 | (1.3) | 1491 | (86.2) | 2 | (0.1) |
| Number of dentists working in a hospital (mean (SD)) | 1.4 (13.5) | 6.3 | (28.2) | 7.0 | (19.6) | - | - | - | - |
| Regional factors | |||||||||
| Having dental colleges or faculty of dentistry (%) | 1437 | 310 | (21.6) | 66 | (21.3) | 1127 | (78.4) | 11 | (1.0) |
| Number of dental clinics per 10,000 population (mean (SD)) | 53.5(15.4) | 53.9 | (20.9) | 55.6 | (24.5) | 53.5 | (15.36) | 53.96 | (11.61) |
| Regional divisions (%) | |||||||||
| Hokkaido | 489 | 88 | (18.0) | 11 | (12.5) | 401 | (82.0) | 3 | (0.7) |
| Tohoku | 476 | 135 | (28.4) | 19 | (14.1) | 341 | (71.6) | 4 | (1.2) |
| Kanto | 1758 | 438 | (24.9) | 79 | (18.0) | 1320 | (75.1) | 17 | (1.3) |
| Chubu | 1007 | 292 | (29.0) | 65 | (22.3) | 715 | (71.0) | 6 | (0.8) |
| Kinki | 1217 | 256 | (21.0) | 68 | (26.6) | 961 | (79.0) | 8 | (0.8) |
| Chugoku/Shikoku | 955 | 186 | (19.5) | 41 | (22.0) | 769 | (80.5) | 4 | (0.5) |
| Kyushu/Okinawa | 1303 | 189 | (14.5) | 41 | (21.7) | 1114 | (85.5) | 8 | (0.7) |
| Surgery Hospitals | With Dentists | Without Dentists | |||||
|---|---|---|---|---|---|---|---|
| Perioperative Oral Care | Perioperative Oral Care | ||||||
| N | N | n | (%) | N | n | (%) | |
| N | 3279 | 1076 | 598 | (55.6) | 2203 | 91 | (4.1) |
| Hospital factors | |||||||
| DPC type (%) | |||||||
| Group I | 82 | 82 | 74 | (90.2) | - | - | - |
| Group II | 139 | 112 | 94 | (83.9) | 27 | 8 | (29.6) |
| Group III | 1373 | 583 | 377 | (64.7) | 790 | 70 | (8.9) |
| Non-DPC | 1685 | 299 | 53 | (17.7) | 1386 | 13 | (0.9) |
| Establisher of hospitals (%) | |||||||
| The Japanese government | 171 | 101 | 57 | (56.4) | 70 | 7 | (10.0) |
| University | 148 | 117 | 94 | (80.3) | 31 | 1 | (3.2) |
| Public organizations | 827 | 423 | 285 | (67.4) | 404 | 40 | (9.9) |
| Social insurance-related organizations | 48 | 24 | 21 | (87.5) | 24 | 6 | (25.0) |
| Medical corporations | 1681 | 295 | 84 | (28.5) | 1386 | 26 | (1.9) |
| Other corporations | 292 | 90 | 39 | (43.3) | 202 | 7 | (3.5) |
| Others | 112 | 26 | 18 | (69.2) | 86 | 4 | (4.7) |
| Regional medical care support hospital | 543 | 338 | 254 | (75.1) | 205 | 44 | (21.5) |
| Emergency hospital | 2713 | 948 | 560 | (59.1) | 1765 | 86 | (4.9) |
| Recovery rehabilitation hospital | 43 | 8 | 0 | 0.0 | 35 | 0 | 0.0 |
| Long-term care hospital | 33 | 13 | 0 | 0.0 | 20 | 0 | 0.0 |
| Number of dentists working in a hospital (mean (SD)) | 2.3(15.5) | 7.0(26.5) | 9.1 | (29.2) | - | - | - |
| Regional factors | |||||||
| Having dental colleges or faculty of dentistry (%) | 665 | 209 | 139 | (66.5) | 456 | 21 | (4.6) |
| Number of dental clinics per 10,000 population (mean (SD)) | 54.6(19.8) | 52.4 (17.4) | 56.7 | (27.0) | 54.49 (18.0) | 53.55 | (12.3) |
| Regional divisions (%) | |||||||
| Hokkaido | 200 | 51 | 28 | (54.9) | 149 | 2 | (1.3) |
| Tohoku | 210 | 86 | 41 | (47.7) | 124 | 8 | (6.5) |
| Kanto | 902 | 306 | 162 | (52.9) | 596 | 15 | (2.5) |
| Chubu | 463 | 217 | 135 | (62.2) | 246 | 11 | (4.5) |
| Kinki | 626 | 183 | 114 | (62.3) | 443 | 25 | (5.6) |
| Chugoku/Shikoku | 374 | 116 | 67 | (57.8) | 258 | 14 | (5.4) |
| Kyushu/Okinawa | 504 | 117 | 51 | (43.6) | 387 | 16 | (4.1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ishimaru, M.; Taira, K.; Zaitsu, T.; Inoue, Y.; Kino, S.; Takahashi, H.; Tamiya, N. Characteristics of Hospitals Employing Dentists, and Utilization of Dental Care Services for Hospitalized Patients in Japan: A Nationwide Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 6448. https://doi.org/10.3390/ijerph19116448
Ishimaru M, Taira K, Zaitsu T, Inoue Y, Kino S, Takahashi H, Tamiya N. Characteristics of Hospitals Employing Dentists, and Utilization of Dental Care Services for Hospitalized Patients in Japan: A Nationwide Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(11):6448. https://doi.org/10.3390/ijerph19116448
Chicago/Turabian StyleIshimaru, Miho, Kento Taira, Takashi Zaitsu, Yuko Inoue, Shiho Kino, Hideto Takahashi, and Nanako Tamiya. 2022. "Characteristics of Hospitals Employing Dentists, and Utilization of Dental Care Services for Hospitalized Patients in Japan: A Nationwide Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 11: 6448. https://doi.org/10.3390/ijerph19116448