
Chemical Mixtures in the EU Population: Composition and Potential Risks

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. HBM4EU-Aggregated Dataset
2.2. Derivation of Generic Mixtures
2.3. Individual Substance Risks
2.4. Characterisation of Mixture Risks
3. Results
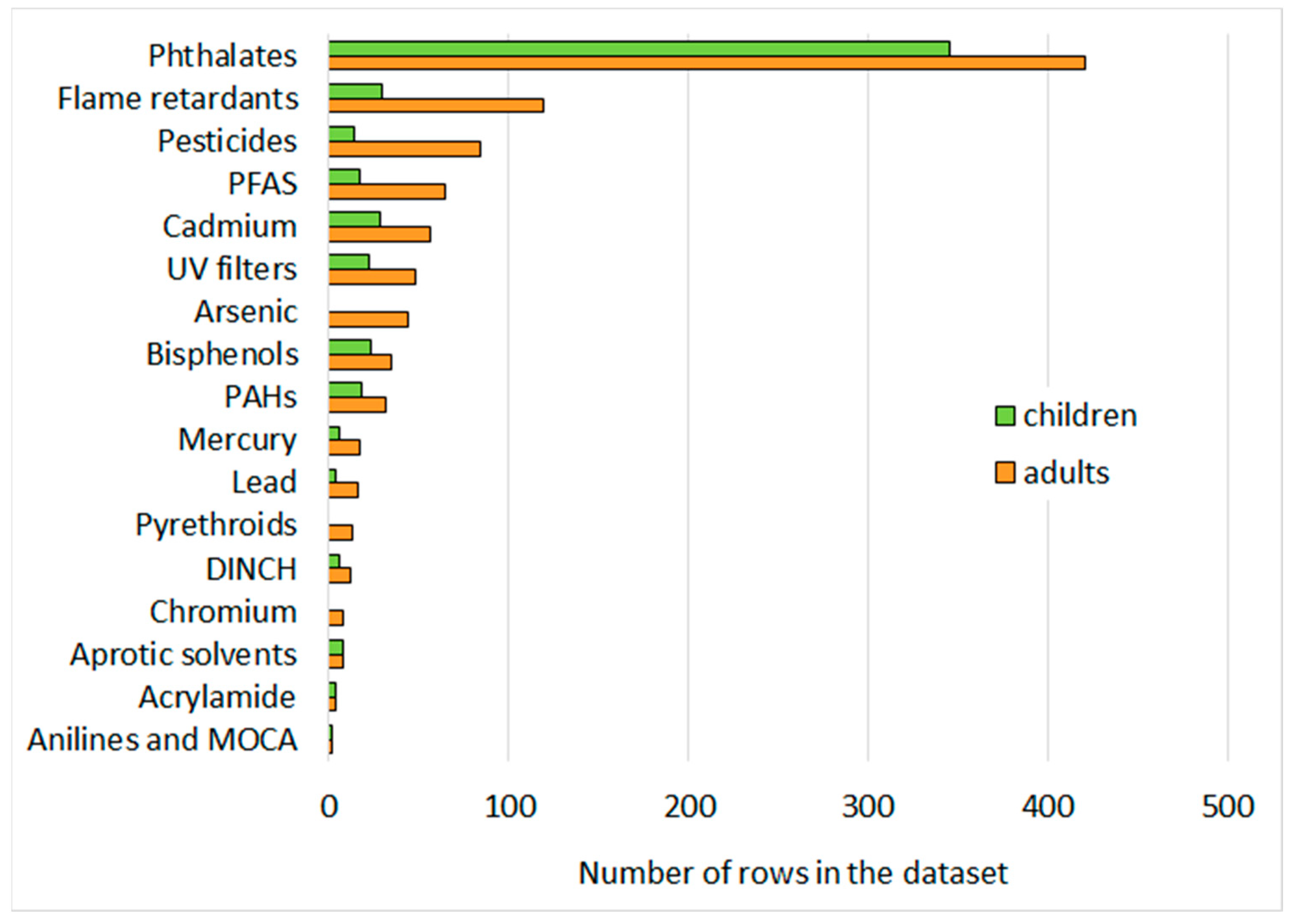
3.1. Composition of the Generic Mixtures
3.2. Single Substance Risks
3.3. Variability in Exposure Patterns of Toxicity Drivers
3.4. Mixtures Risk
4. Discussion
4.1. Building a Generic Mixture Representing Exposure in the European Population
4.2. Assumptions and Related Uncertainties in Mixture Risks Characterisation
4.3. Informing a Possible Mixture Assessment Factor
4.4. Towards Priority Mixtures of Concern
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kortenkamp, A. Low dose mixture effects of endocrine disrupters: Implications for risk assessment and epidemiology. Int. J. Androl. 2008, 312, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Bopp, S.K.; Kienzler, A.; Richarz, A.N.; van der Linden, S.C.; Paini, A.; Parissis, N.; Worth, A.P. Regulatory assessment and risk management of chemical mixtures: Challenges and ways forward. Crit. Rev. Toxicol. 2019, 492, 174–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Commission. Progress Report on the Assessment and Management of Combined Exposure to Multiple Chemicals (Chemical Mixtures) and Associated Risks. Staff Working Document SWD 250 Final. 2020. Available online: https://ec.europa.eu/environment/pdf/chemicals/2020/10/SWD_mixtures.pdf (accessed on 12 May 2022).
- Bopp, S.K.; Barouki, R.; Brack, W.; Dalla Costa, S.; Dorne, J.L.C.M.; Drakvik, P.E.; Faust, M.; Karjalainen, T.K.; Kephalopoulos, S.; van Klaveren, J.; et al. Current EU Research Activities on Combined Exposure to Multiple Chemicals; Environment International; Elsevier Ltd.: Amsterdam, The Netherlands, 2018; Volume 120, pp. 544–562. [Google Scholar]
- Drakvik, E.; Altenburger, R.; Aoki, Y.; Backhaus, T.; Bahadori, T.; Barouki, R.; Brack, W.; Cronin, M.T.D.; Demeneix, B.; Hougaard Bennekou, S.; et al. Statement on advancing the assessment of chemical mixtures and their risks for human health and the environment. Environ. Int. 2020, 134, 105267. [Google Scholar] [CrossRef] [PubMed]
- Swedish Government. Future Chemical Risk Management—Accounting for Combination Effects and Assessing Chemicals in Groups. 2019; p. 245. Available online: https://www.government.se/legal-documents/2019/11/sou-201945/ (accessed on 12 May 2022).
- European Commission. Chemical Strategy for Sustainability—Towards a Toxic Free Environment. Communication from the Commission to the Par-liament, the Council, the European Economic and Social Committee and the Committee of the Regions. COM(2020) 667 Final. 2020. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=COM%3A2020%3A667%3AFIN (accessed on 12 May 2022).
- Price, P.S.; Han, X. Maximum cumulative ratio (MCR) as a tool for assessing the value of performing a cumulative risk assessment. Int. J. Environ. Res. Public Health 2011, 86, 2212–2225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bopp, S.K.; Van der Linden, S.; Lamon, L.; Paini, A.; Parissis, N.; Richarz, A.N.; Triebe, J.; Worth, A. Review of Case Studies on the Human and Environmental Risk Assessment of Chemical Mixtures Identification of Priorities, Methodologies, Data Gaps, Future Needs; Publications Office of the European Union: Luxembourg, 2016; p. 87. [Google Scholar]
- Ganzleben, C.; Antignac, J.P.; Barouki, R.; Castaño, A.; Fiddicke, U.; Klánová, J.; Lebret, E.; Olea, N.; Sarigiannis, D.; Schoeters, G.R.; et al. Human biomonitoring as a tool to support chemicals regulation in the European Union. Int. J. Hyg. Environ. Health 2017, 220, 94–97. [Google Scholar] [CrossRef]
- Ougier, E.; Ganzleben, C.; Lecoq, P.; Bessems, J.; David, M.; Schoeters, G.; Lange, R.; Meslin, M.; Uhl, M.; Kolossa-Gehring, M.; et al. Chemical prioritisation strategy in the European Human Biomonitoring Initiative (HBM4EU)—Development and results. Int. J. Hyg. Environ. Health 2021, 236, 113778. [Google Scholar] [CrossRef]
- Vorkamp, K.; Castaño, A.; Antignac, J.P.; Boada, L.D.; Cequier, E.; Covaci, A.; Esteban López, M.; Haug, L.S.; Kasper-Sonnenberg, M.; Koch, H.M.; et al. Biomarkers, matrices and analytical methods targeting human exposure to chemicals selected for a European human biomonitoring initiative. Environ. Int. 2021, 146, 106082. [Google Scholar] [CrossRef]
- Poulson, O.M.; Holst, E.; Christensen, J.M. Calculation and application of coverage intervals for biological reference values (Technical Report). Pure Appl. Chem. 1997, 69, 1601–1612. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing, Vienna, Austria. 2021. Available online: https://www.R-project.org/ (accessed on 12 May 2022).
- Wickham, H.; Averick, M.; Bryan, J.; Chang, W.; McGowan, L.D.A.; François, R.; Grolemund, G.; Hayes, A.; Henry, L.; Hester, J.; et al. Welcome to the tidyverse. J. Open Source Softw. 2019, 4, 1686. [Google Scholar] [CrossRef]
- WHO. Human Biomonitoring: Facts and Figures; World Health Organization: Geneva, Switzerland, 2015; pp. 1–88. Available online: http://www.euro.who.int/__data/assets/pdf_file/0020/276311/Human-biomonitoring-facts-figures-en.pdf (accessed on 12 May 2022).
- Hays, S.M.; Nordberg, M.; Yager, J.W.; Aylward, L.L. Biomonitoring Equivalents (BE) dossier for cadmium (Cd) (CAS No. 7440-43-9). Regul. Toxicol. Pharmacol. 2008, 51 (Suppl. 3), 49–56. [Google Scholar] [CrossRef]
- Angerer, J.; Aylward, L.L.; Hays, S.M.; Heinzow, B.; Wilhelm, M. Human biomonitoring assessment values: Approaches and data requirements. Int. J. Hyg. Environ. Health 2011, 2145, 348–360. [Google Scholar] [CrossRef] [PubMed]
- Apel, P.; Rousselle, C.; Lange, R.; Sissoko, F.; Kolossa-Gehring, M.; Ougier, E. Human biomonitoring initiative (HBM4EU)—Strategy to derive human biomonitoring guidance values (HBM-GVs) for health risk assessment. Int. J. Hyg. Environ. Health 2020, 230, 113622. [Google Scholar] [CrossRef] [PubMed]
- Hölzer, J.; Lilienthal, H.; Schümann, M. Human Biomonitoring (HBM)-I values for perfluorooctanoic acid (PFOA) and perfluorooctane sulfonic acid (PFOS)—Description, derivation and discussion. Regul. Toxicol. Pharmacol. 2021, 121, 104862. [Google Scholar] [CrossRef] [PubMed]
- Lamkarkach, F.; Ougier, E.; Garnier, R.; Viau, C.; Kolossa-Gehring, M.; Lange, R.; Apel, P. Human biomonitoring initiative (HBM4EU): Human biomonitoring guidance values (HBM-GVs) derived for cadmium and its compounds. Environ. Int. 2021, 147, 106337. [Google Scholar] [CrossRef] [PubMed]
- EFSA. Guidance Document on Scientific criteria for grouping chemicals into assessment groups for human risk assessment of combined exposure to multiple chemicals. EFSA J. 2021, 19, e07033. [Google Scholar]
- Martin, O.; Scholze, M.; Ermler, S.; McPhie, J.; Bopp, S.K.; Kienzler, A.; Parissis, N.; Kortenkamp, A. Ten years of research on synergisms and antagonisms in chemical mixtures: A systematic review and quantitative reappraisal of mixture studies. Environ. Int. 2021, 146, 106206. [Google Scholar] [CrossRef] [PubMed]
- Swedish Chemicals Agency (KEMI). An Additional Assessment Factor (MAF)—A Suitable Approach for Improving the Regulatory Risk Assessment of Chemical Mixtures? 2015, Report 5/15. Available online: https://www.kemi.se/en/publications/reports/2015/report-5-15-an-additional-assessment-factor-maf---a-suitable-approach-for-improving-the-regulatory-risk-assessment-of-chemical-mixtures (accessed on 12 May 2022).
- Swedish Chemicals Agency (KEMI). Improving the Regulatory Assessment of Combination Effects: Steps towards Implementing the Mixture Assessment Factor (MAF) in Chemical Regulation. 2021, p. 59. Available online: https://www.kemi.se/en/publications/pms/2021/pm-8-21-improving-the-regulatory-assessment-of-combination-effects-steps-towards-implementing-the-mixture-assessment-factor-maf-in-chemical-regulation (accessed on 12 May 2022).
- UNEP. Second Global Monitoring Report: Global Monitoring Plan for Persistent Organic Pollutants. Unep/Pops/Cop.8/Inf/38. 2017. Available online: http://chm.pops.int/TheConvention/ConferenceoftheParties/Meetings/COP8/tabid/5309/Default.aspx (accessed on 12 May 2022).
- Bandow, N.; Conrad, A.; Kolossa-Gehring, M.; Murawski, A.; Sawal, G. Polychlorinated biphenyls (PCB) and organochlorine pesticides (OCP) in blood plasma—Results of the German environmental survey for children and adolescents 2014–2017 (GerES V). Int. J. Hyg. Environ. Health 2020, 224, 113426. [Google Scholar] [CrossRef]
- Colles, A.; Coertjens, D.; Morrens, B.; Den Hond, E.; Paulussen, M.; Bruckers, L.; Govarts, E.; Covaci, A.; Koppen, G.; Croes, K.; et al. Human biomonitoring data enables evidence-informed policy to reduce internal exposure to persistent organic compounds: A case study. Int. J. Environ. Res. Public Health 2021, 18, 5559. [Google Scholar] [CrossRef]
- Lassen, T.H.; Frederiksen, H.; Jensen, T.K.; Petersen, J.H.; Main, K.M.; Skakkebæk, N.E.; Jørgensen, N.; Kranich, S.K.; Andersson, A.M. Temporal variability in urinary excretion of bisphenol A and seven other phenols in spot, morning, and 24-h urine samples. Environ. Res. 2013, 126, 164–170. [Google Scholar] [CrossRef]
- Vernet, C.; Philippat, C.; Agier, L.; Calafat, A.M.; Ye, X.; Lyon-Caen, S.; Hainaut, P.; Siroux, V.; Schisterman, E.F.; Slama, R. An Empirical Validation of the Within-subject Biospecimens Pooling Approach to Minimize Exposure Misclassification in Biomarker-based Studies. Epidemiology 2019, 30, 756–767. [Google Scholar] [CrossRef]
- Buekers, J.; Verheyen, V.; Remy, S.; Covaci, A.; Colles, A.; Koppen, G.; Govarts, E.; Bruckers, L.; Leermakers, M.; St-Amand, A.; et al. Combined chemical exposure using exposure loads on human biomonitoring data of the 4th Flemish Environment and Health Study (FLEHS-4). Int. J. Hyg. Environ. Health 2021, 238, 113849. [Google Scholar] [CrossRef] [PubMed]
- Arrebola, J.P.; Castaño, A.; Esteban, M.; Bartolomé, M.; Pérez-Gómez, B.; Ramos, J.J. Differential contribution of animal and vegetable food items on persistent organic pollutant serum concentrations in Spanish adults. Data from BIOAMBIENT.ES project. Sci. Total Environ. 2018, 634, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Gilles, L.; Govarts, E.; Rambaud, L.; Vogel, N.; Castaño, A.; Esteban López, M.; Rodriguez Martin, L.; Koppen, G.; Remy, S.; Vrijheid, M.; et al. HBM4EU combines and harmonises human biomonitoring data across the EU, building on existing capacity—The HBM4EU survey. Int. J. Hyg. Environ. Health 2021, 237, 113809. [Google Scholar] [CrossRef] [PubMed]
- Pourchet, M.; Debrauwer, L.; Klanova, J.; Price, E.J.; Covaci, A.; Caballero-Casero, N.; Oberacher, H.; Lamoree, M.; Damont, A.; Fenaille, F.; et al. Suspect and non-targeted screening of chemicals of emerging concern for human biomonitoring, environmental health studies and support to risk assessment: From promises to challenges and harmonisation issues. Environ. Int. 2020, 139, 105545. [Google Scholar] [CrossRef] [PubMed]
- Franken, C.; Koppen, G.; Lambrechts, N.; Govarts, E.; Bruckers, L.; Den Hond, E.; Loots, I.; Nelen, V.; Sioen, I.; Nawrot, T.S.; et al. Environmental exposure to human carcinogens in teenagers and the association with DNA damage. Environ. Res. 2017, 152, 165–174. [Google Scholar] [CrossRef] [PubMed]
- Franken, C.; Lambrechts, N.; Govarts, E.; Koppen, G.; Den Hond, E.; Ooms, D.; Voorspoels, S.; Bruckers, L.; Loots, I.; Nelen, V.; et al. Phthalate-induced oxidative stress and association with asthma-related airway inflammation in adolescents. Int. J. Hyg. Environ. Health 2017, 2202, 468–477. [Google Scholar] [CrossRef]
- Verheyen, V.J.; Remy, S.; Govarts, E.; Colles, A.; Martin, L.R.; Koppen, G.; Voorspoels, S.; Bruckers, L.; Bijnens, M.; Vos, S.; et al. Urinary Polycyclic Aromatic Hydrocarbon Metabolites Are Associated with Biomarkers of Chronic Endocrine Stress, Oxidative Stress, and Inflammation in Adolescents: FLEHS-4 (2016–2020). Toxics 2021, 9, 245. [Google Scholar] [CrossRef]
- Zare Jeddi, M.; Hopf, N.B.; Viegas, S.; Price, A.B.; Paini, A.; van Thriel, C.; Benfenati, E.; Ndaw, S.; Bessems, J.; Behnisch, P.A.; et al. Towards a systematic use of effect biomarkers in population and occupational biomonitoring. Environ. Int. 2021, 146, 106257. [Google Scholar] [CrossRef]
- EFSA. Guidance on harmonised methodologies for human health, animal health and ecological risk assessment of combined exposure to multiple chemicals. EFSA J. 2019, 17, e05634. [Google Scholar]
- OECD. Considerations for Assessment of Risk from the Combined Exposure to Multiple Chemicals. Test Assess. 2018, 296, 119. Available online: https://www.oecd.org/chemicalsafety/considerations-for-assessing-the-risks-of-combined-exposure-to-multiple-chemicals-ceca15a9-en.htm (accessed on 12 May 2022).
- Meek, M.E.; Boobis, A.R.; Crofton, K.M.; HeineMeyer, G.; Van Raaij, M.; Vickers, C. Risk assessment of combined exposure to multiple chemicals: A WHO/IPCS framework. Regul. Toxicol. Pharmacol. 2011, 602, S1–S14. [Google Scholar]
- Kortenkamp, A.; Backhaus, T.; Faust, M. State of the Art Report of Mixture Toxicity. EU Commission Study Contract No. 070307/2007/485103/ETU/D.1. 2009. Available online: https://ec.europa.eu/environment/chemicals/effects/pdf/report_mixture_toxicity.pdf (accessed on 12 May 2022).
- Price, P.; Zaleski, R.; Hollnagel, H.; Ketelslegers, H.; Han, X. Assessing the safety of co-exposure to food packaging migrants in food and water using the maximum cumulative ratio and an established decision tree. Food Addit. Contam. Part A Chem. Anal. Control Expo. Risk Assess. 2014, 313, 414–421. [Google Scholar] [CrossRef] [PubMed]
- Han, X.; Price, P.S. Applying the maximum cumulative ratio methodology to biomonitoring data on dioxin-like compounds in the general public and two occupationally exposed populations. J. Expo. Sci. Environ. Epidemiol. 2013, 234, 343–349. [Google Scholar] [CrossRef] [PubMed]
- De Brouwere, K.; Cornelis, C.; Arvanitis, A.; Brown, T.; Crump, D.; Harrison, P.; Jantunen, M.; Price, P.; Torfs, R. Application of the maximum cumulative ratio (MCR) as a screening tool for the evaluation of mixtures in residential indoor air. Sci. Total Environ. 2014, 479, 267–276. [Google Scholar] [CrossRef]
- Faure, S.; Noisel, N.; Werry, K.; Karthikeyan, S.; Aylward, L.L.; St-Amand, A. Evaluation of human biomonitoring data in a health risk based context: An updated analysis of population level data from the Canadian Health Measures Survey. Int. J. Hyg. Environ. Health 2020, 2231, 267–280. [Google Scholar] [CrossRef]
- Hays, S.M.; Aylward, L.L.; Gagné, M.; Nong, A.; Krishnan, K. Biomonitoring Equivalents for inorganic arsenic. Regul. Toxicol. Pharmacol. 2010, 581, 1–9. [Google Scholar] [CrossRef]
- Ougier, E.; Fiore, K.; Rousselle, C.; Assunção, R.; Martins, C.; Buekers, J. Burden of osteoporosis and costs associated with human biomonitored cadmium exposure in three European countries: France, Spain and Belgium. Int. J. Hyg. Environ. Health 2021, 234, 113747. [Google Scholar] [CrossRef]
- Jain, R.B. Synergistic impact of co-exposures to toxic metals cadmium, lead, and mercury along with perfluoroalkyl substances on the healthy kidney function. Environ. Res. 2019, 169, 342–347. [Google Scholar] [CrossRef]
- European Chemical Agency. Committee for Risk Assessment (RAC) Committee for Socio-economic Analysis (SEAC) Opinion on four phthalates (DEHP, BBP, DBP, DIBP). 2017. Available online: https://echa.europa.eu/documents/10162/4080643e-4b56-c073-f902-bdc936034826 (accessed on 12 May 2022).
- Apel, P.; Angerer, J.; Wilhelm, M.; Kolossa-Gehring, M. New HBM values for emerging substances, inventory of reference and HBM values in force, and working principles of the German Human Biomonitoring Commission. Int. J. Hyg. Environ. Health 2017, 220, 152–166. [Google Scholar] [CrossRef] [Green Version]
- Arnold, S.M.; Morriss, A.; Velovitch, J.; Juberg, D.; Burns, C.J.; Bartels, M.; Aggarwal, M.; Poet, T.; Hays, S.; Price, P. Derivation of human biomonitoring guidance values for chlorpyrifos using a physiologically based pharmacokinetic and pharmacodynamic model of cholinesterase inhibition. Regul. Toxicol. Pharmacol. 2015, 71, 235–243. [Google Scholar] [CrossRef] [Green Version]
- Aylward, L.L.; Hays, S.M.; Gagné, M.; Krishnan, K. Derivation of Biomonitoring Equivalents for di-n-butyl phthalate (DBP), benzylbutyl phthalate (BzBP), and diethyl phthalate (DEP). Regul. Toxicol. Pharmacol. 2009, 55, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Aylward, L.L.; Irwin, K.; St-Amand, A.; Nong, A.; Hays, S.M. Screening-level Biomonitoring Equivalents for tiered interpretation of urinary 3-phenoxybenzoic acid (3-PBA) in a risk assessment context. Regul. Toxicol. Pharmacol. 2018, 92, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Bhat, V.S.; Durham, J.L.; English, J.C. Derivation of an oral reference dose (RfD) for the plasticizer, di-(2-propylheptyl)phthalate (Palatinol® 10-P). Regul. Toxicol. Pharmacol. 2014, 70, 65–74. [Google Scholar] [CrossRef] [PubMed]
- David, M.; Gerofke, A.; Lange, R.; Kolossa-Gehring, M.; Apel, P. The European Human Biomonitoring Initiative (HBM4EU): Human biomonitoring guidance values (HBM-GVs) for the aprotic solvents N-methyl-2-pyrrolidone (NMP) and N-ethyl-2-pyrrolidone (NEP). Int. J. Hyg. Environ. Health 2021, 238, 113856. [Google Scholar] [CrossRef] [PubMed]
- Hays, S.M.; Aylward, L.L.; Kirman, C.R.; Krishnan, K.; Nong, A. Biomonitoring Equivalents for di-isononyl phthalate (DINP). Regul. Toxicol. Pharmacol. 2011, 60, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, K.; Adamou, T.; Aylward, L.L.; Hays, S.M.; Kirman, C.R.; Nong, A. Biomonitoring Equivalents for 2,2′,4,4′,5-pentabromodiphenylether (PBDE-99). Regul. Toxicol. Pharmacol. 2011, 60, 165–171. [Google Scholar] [CrossRef]
- Lange, R.; Apel, P.; Rousselle, C.; Charles, S.; Sissoko, F.; Kolossa-Gehring, M.; Ougier, E. The European Human Biomonitoring Initiative (HBM4EU): Human biomonitoring guidance values for selected phthalates and a substitute plasticizer. Int. J. Hyg. Environ. Health 2021, 234, 113722. [Google Scholar] [CrossRef]
- Ougier, E.; Zeman, F.; Antignac, J.P.; Rousselle, C.; Lange, R.; Kolossa-Gehring, M.; Apel, P. Human biomonitoring initiative (HBM4EU): Human biomonitoring guidance values (HBM-GVs) derived for bisphenol A. Environ. Int. 2021, 154, 106563. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Options for Variable | |
|---|---|---|
| Population type |
| |
| Countries |
|
|
| Matrix |
| |
| Substance group |
|
|
| Age categories |
| |
| Urbanization degree |
| |
| Education |
| |
| Substance (Biomarker) | Unit and Related Matrix (U-Urine; B-Blood) | Adults | Children | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| HBM HBGV | P50 | P95 | RQ50 (RQ50,adj) | RQ95 (RQ95,adj) | HBM HBGV | P50 | P95 | RQ50 (RQ50,adj) | RQ95 (RQ95,adj) | ||
| Metals and metalloids | |||||||||||
| Cd | µg/g crt U | 1.0 | 0.21 | 0.55 | 0.206 | 0.548 | 1.0 | 0.12 | 0.24 | 0.115 | 0.237 |
| Hg | µg/L U | 7.0 | 0.73 | 4.79 | 0.105 | 0.684 | 7.0 | 0.24 | 1.22 | 0.035 | 0.174 |
| As (Σ(As(III) + As(V) + DMA + MMA)) | µg/L U | 6.4 | 4.15 | 12.61 | 0.648 | 1.970 (1.0) | - | - | - | - | - |
| Phthalates | |||||||||||
| BBzP (MBzP) | µg/L U | 3000 | 5.06 | 21.84 | 0.002 | 0.007 | 2000 | 7.37 | 34.00 | 0.004 | 0.017 |
| DEP (MEP) | µg/L U | 18,000 | 34.00 | 351.35 | 0.002 | 0.020 | 18,000 | 24.40 | 148.51 | 0.001 | 0.008 |
| DnBP (MnBP) | µg/L U | 190 | 23.50 | 86.72 | 0.124 | 0.456 | 120 | 38.90 | 130.10 | 0.324 | 1.084 (1.0) |
| DiDP (MiBP) | µg/L U | 230 | 28.01 | 106.4 | 0.122 | 0.463 | 160 | 45.54 | 185.4 | 0.285 | 1.159 (1.0) |
| DEHP (Σ(OH-MEHP, oxo-MEHP)) | µg/L U | 500 | 21.64 | 85.20 | 0.043 | 0.170 | 340 | 37.98 | 138.44 | 0.112 | 0.407 |
| DiNP (Σ(cx-MiNP, OH-MinP, oxo-MiNP) | µg/L U | 1800 | 13.22 | 69.29 | 0.007 | 0.038 | 1800 | 18.82 | 95.48 | 0.010 | 0.053 |
| DEHTP (5-cx MEPTP) | µg/L U | 2800 | 4.85 | 30.29 | 0.002 | 0.011 | 1800 | 11.01 | 70.01 | 0.006 | 0.039 |
| DPHP (Σ(OH-MPHP, oxo-MPHP)) | µg/L U | 500 | 0.60 | 2.93 | 0.001 | 0.006 | 330 | 0.65 | 4.67 | 0.002 | 0.014 |
| Other plasticizers | |||||||||||
| DINCH (Σ(OH-MINCH, cx-MINCH)) | µg/L U | 4500 | 1.65 | 20.95 | 0.0004 | 0.005 | 3000 | 4.81 | 28.38 | 0.002 | 0.009 |
| PFAS | |||||||||||
| PFOA | µg/L B | 2.0 | 1.62 | 3.68 | 0.810 | 1.840 (1.0) | 2.0 | 2.20 | 4.30 | 1.098 (1.0) | 2.150 (1.0) |
| PFOS | µg/L B | 5.0 | 6.26 | 14.21 | 1.252 (1.0) | 2.842 (1.0) | 5.0 | 4.07 | 8.43 | 0.815 | 1.685 (1.0) |
| Flame retardants | |||||||||||
| BDE-99 | µg/g lip B | 0.52 | 0.001 | 0.007 | 0.001 | 0.014 | 0.52 | 0.001 | 0.005 | 0.003 | 0.010 |
| Bisphenols | |||||||||||
| BPA (total BPA) | µg/L U | 230 | 2.09 | 9.50 | 0.009 | 0.041 | 135 | 2.09 | 9.50 | 0.015 | 0.070 |
| Pyrethroids insecticides | |||||||||||
| Various pyrethroid insecticides (3-PBA) | µg/L U | 87 | 0.34 | 2.44 | 0.004 | 0.028 | |||||
| Pesticides | |||||||||||
| Chlorpyripfos (TCPy) | µg/L U | 2100 | 1.95 | 9.94 | 0.001 | 0.005 | |||||
| Aprotic solvents | |||||||||||
| NEP Σ(5-HNEP, 2-HESI) | µg/L U | 15,000 | 8.95 | 276.20 | 0.001 | 0.018 | 10,000 | 6.80 | 121.33 | 0.001 | 0.012 |
| NMP (Σ (5-HNMP, 2-HMSI)) | µg/L U | 15,000 | 100.50 | 274.90 | 0.007 | 0.018 | 10,000 | 97.38 | 280.55 | 0.010 | 0.028 |
| Mixture Hazard Index (HI) Equation (1) | 3.35 (3.04) | 9.19 (5.38) | 2.84 (2.74) | 7.16 (5.1) | |||||||
| Max RQ | 1.25 (1.0) | 2.84 (1.0) | 1.10 (1.0) | 2.15 (1.0) | |||||||
| Maximum Cumulative Ratio (MCR) Equation (3) | 2.67 (3.09) | 3.23 (5.53) | 2.58 (2.74) | 3.33 (5.08) | |||||||
| Mixture allocation factor (MAFceiling) | 7.03 | 10.1 | 5.85 | 9.46 | |||||||
| Assumptions | Details | Effect on MAF Size |
|---|---|---|
| The GCM is built only considering monitored chemicals within the HBM4EU priority list. | The substances measured in HBM4EU are just a fraction of the entire array of chemicals present in European populations. | ↓ |
| The GCM used to calculate the mixture risk is formed by only 20 and 17 components for adults and children, respectively. | The mixture to calculate the mixture risk had to be narrowed down further based on the limited availability of HBM HBGVs to calculate the HI and MCR. This represents only a subset of the entire GCM. | ↓ |
| Combining co-exposure patterns from aggregated statistics of different study populations. | Using aggregated data, we assume a simultaneous exposure to all measured chemicals at P50 or P95, without knowing the real co-exposure patterns of the individuals. | At P50 ↓ or ↑ at P95 ↑ |
| All chemicals are considered to contribute to the combined risk assuming concentration addition. | No grouping was done for specific effects, assuming all chemicals will contribute to the overall combined risk independent of their Mode of Action. | ↑ |
| Pooling data across different data sets covering a relatively long time range from different European regions. | EU wide dataset, need to average across dataset regions and periods, assuming all of them equally represent a recent exposure scenario of the EU population. | ↓ or ↑ |
| HBM health based guidance values (HBGVs) | Absence of a fully standardized method for deriving HBM HBGVs (e.g., different uncertainty factors used) | ↓ or ↑ |
| Selection of population group | All persons ≥ 12 years were included in the “adult population” of the HBM4EU dataset All individuals < 12 years excluding infants were considered in the “children” group | ↓ or ↑ |
| Analytical accuracy | Intrinsic complexity of the individual datasets such as different analytical power and inter laboratory differences | ↓ or ↑ |
| Processing of non-detects | By replacing non-detects with zeros, it is likely that our calculated P50 underestimates the actual 50th percentile in some cases | ↓ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Socianu, S.; Bopp, S.K.; Govarts, E.; Gilles, L.; Buekers, J.; Kolossa-Gehring, M.; Backhaus, T.; Franco, A. Chemical Mixtures in the EU Population: Composition and Potential Risks. Int. J. Environ. Res. Public Health 2022, 19, 6121. https://doi.org/10.3390/ijerph19106121
Socianu S, Bopp SK, Govarts E, Gilles L, Buekers J, Kolossa-Gehring M, Backhaus T, Franco A. Chemical Mixtures in the EU Population: Composition and Potential Risks. International Journal of Environmental Research and Public Health. 2022; 19(10):6121. https://doi.org/10.3390/ijerph19106121
Chicago/Turabian StyleSocianu, Sebastian, Stephanie K. Bopp, Eva Govarts, Liese Gilles, Jurgen Buekers, Marike Kolossa-Gehring, Thomas Backhaus, and Antonio Franco. 2022. "Chemical Mixtures in the EU Population: Composition and Potential Risks" International Journal of Environmental Research and Public Health 19, no. 10: 6121. https://doi.org/10.3390/ijerph19106121