
Rare Diseases in the Educational Field: Knowledge and Perceptions of Spanish Teachers

 ,
,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instrument
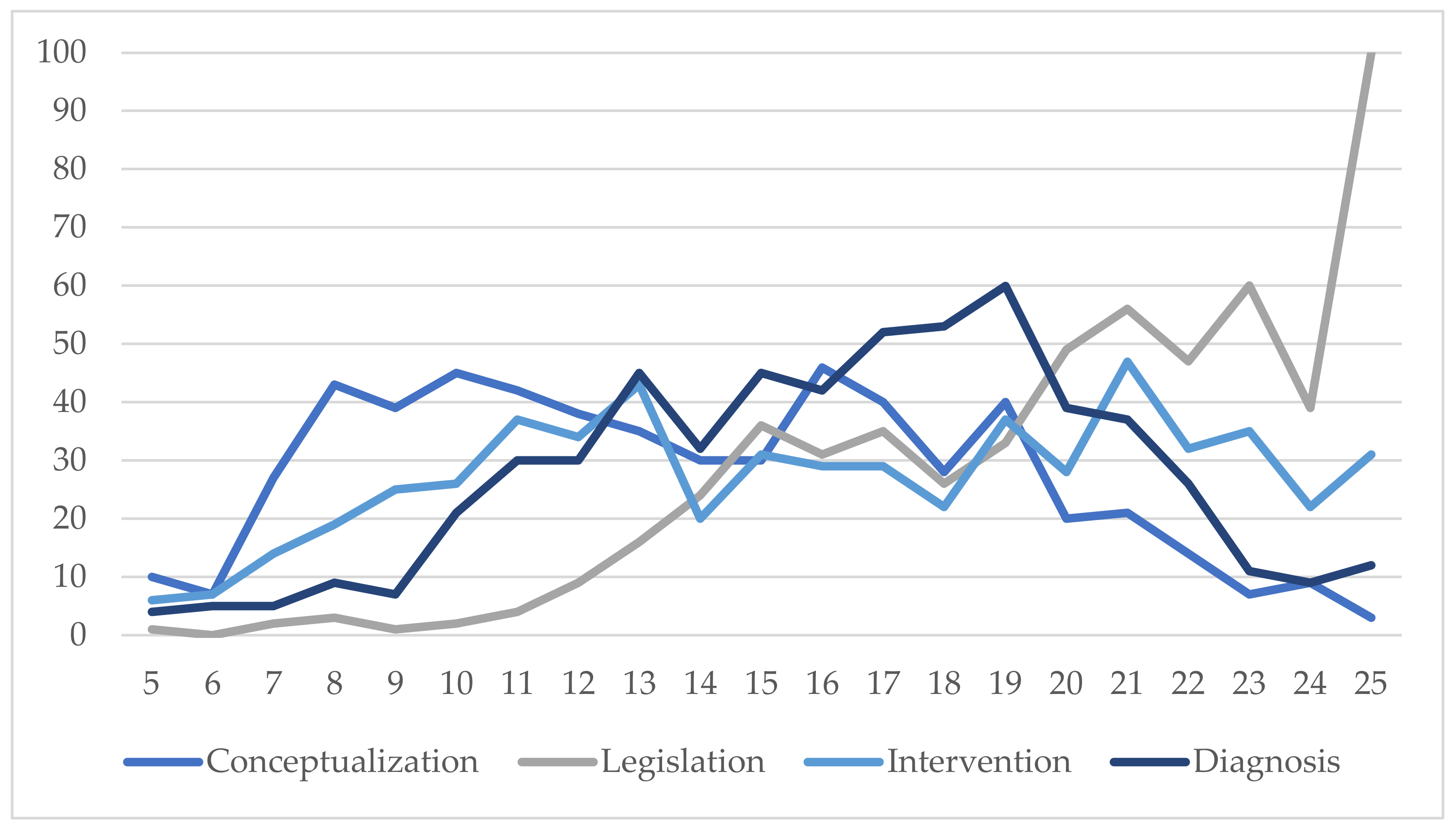
- Conceptualization: key aspects allowing understanding of rare diseases, from definitions to characteristics, prevalence, and types;
- Legislation: legislative frameworks influencing the educational response to these students that teachers should be aware of;
- Intervention: practical aspects affecting teaching and learning processes with these students in schools;
- Diagnosis: content related to identifying these students, warning signs, characteristics, and procedures, as well as assessment of the level of awareness about detection and research in the field.
- The structure of the instrument is given below (Table 1).
2.3. Procedure and Data Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Arnaiz, P. La Educación Inclusiva: Mejora Escolar y Retos para el Siglo XXI. Particip. Educ. 2019, 6, 41–54. Available online: https://cutt.ly/kPPDI97 (accessed on 6 November 2021).
- González-Gil, F.; Pastor-Martín, M.E. Educación para todos: Formación docente, género y atención a la diversidad. Cuest. Género Igual. Difer. 2014, 9, 11–28. [Google Scholar] [CrossRef]
- Espada, R.M.; Gallego, M.; González-Montesino, R.H. Diseño Universal del Aprendizaje e inclusión en la Educación Básica. Alteridad 2019, 14, 207–218. [Google Scholar] [CrossRef] [Green Version]
- Ministerio de Educación y Formación Profesional. Ley Orgánica 3/2020, de 29 de diciembre, por la que se modifica la Ley Orgánica 2/2006, de 3 de mayo, de Educación. Boletín Of. Estado 2020, 340, 122868–122953. Available online: https://cutt.ly/vPPD7j3 (accessed on 9 December 2021).
- Junta de Comunidades de Castilla-La Mancha. Decreto 85/2018, de 20 de noviembre, por el que se regula la inclusión educativa del alumnado en la comunidad de Castilla-La Mancha. D. Of. Castilla-La Mancha 2018, 229, 32231–32246. Available online: https://cutt.ly/tPPDBZb (accessed on 10 December 2021).
- Ahedo, Y.; Cabrejas, M.; Santamaría, A. Enfermedades Raras en la Escuela: Guía de Apoyo; Centro de Referencia Estatal de Atención a Personas con Enfermedades Raras y sus Familias: Burgos, Spain, 2021; Available online: https://cutt.ly/3AqfSa5 (accessed on 22 November 2021).
- Charco, J.M.; Barrio, T.; Eraña, H. Enfermedades priónicas: Historia, diversidad e importancia socioeconómica como paradigma de las Enfermedades Raras. Araucaria. Rev. Iberoam. Filos. Política Humanid. Relac. Int. 2021, 23, 429–451. [Google Scholar] [CrossRef]
- Orphanet. Prevalencia de las enfermedades raras: Datos bibliográficos. Inf. Periód. Orphanet. Ser. Enferm. Raras 2022, 1, 1–94. Available online: https://cutt.ly/rPP1jBl (accessed on 10 March 2022).
- Richter, T.; Nestler-Parr, S.; Babela, R.; Khan, Z.M.; Tesoro, T.; Molsen, E.; Hughes, D.A. Rare Disease Terminology and Definitions-A Systematic Global Review: Report of the ISPOR Rare Disease Special Interest Group. Value Health 2015, 18, 906–914. [Google Scholar] [CrossRef] [Green Version]
- Valdez, R.; Ouyang, L.; Bolen, J. Public Health and Rare Diseases: Oxymoron No More. Prev. Chronic Dis. 2016, 13, E05. [Google Scholar] [CrossRef] [Green Version]
- Nguengang-Wakap, S.; Lambert, D.M.; Olry, A.; Rodwell, C.; Gueydan, C.; Lanneau, V.; Murphy, D.; Le Cam, Y.; Rath, A. Estimating cumulative point prevalence of rare diseases: Analysis of the Orphanet database. Eur. J. Hum. Genet. EJHG 2020, 28, 165–173. [Google Scholar] [CrossRef] [Green Version]
- Walker, C.E.; Mahede, T.; Davis, G.; Miller, L.J.; Girschik, J.; Brameld, K.; Sun, W.; Rath, A.; Aymé, S.; Zubrick, S.R.; et al. The collective impact of rare diseases in Western Australia: An estimate using a population-based cohort. Genet. Med. Off. J. Am. Coll. Med. Genet. 2017, 19, 546–552. [Google Scholar] [CrossRef] [Green Version]
- Seco, M.O.; Ruiz, R. Las enfermedades raras en España. Un enfoque social. Prism. Soc. 2016, 17, 373–395. Available online: https://cutt.ly/2PF0ioY (accessed on 22 October 2021).
- Monzón, J.; Aróstegui, I.; Ozerinjauregi, N. Alumnado con Enfermedades poco Frecuentes y Escuela Inclusiva; Octaedro Editorial: Barcelona, Spain, 2017. [Google Scholar]
- Pérez, J.; Santos, M.T.; Meso, K. Las asociaciones de enfermedades raras: Estructura de sus redes e identificación de los líderes de opinión mediante la técnica del análisis de redes sociales. Rev. Lat. Comun. Soc. 2021, 79, 175–205. [Google Scholar] [CrossRef]
- García-Toledano, E.; Palomares-Ruiz, A.; Serrano-Marugán, I. Enfermedades raras que precisan respuesta social y educativa. In Investigación y Respuestas Socioeducativas del Profesorado en el Siglo XXI.; Palomares-Ruiz, A., Ed.; Editorial Síntesis: Madrid, Spain, 2020; pp. 145–154. [Google Scholar]
- González, B.; González, J.O. Enfermedades raras en edad pediátrica en el contexto de la COVID-19. Rev. Finlay 2021, 11, 1–3. Available online: https://cutt.ly/OPFDv0g (accessed on 17 November 2021).
- Wasilewska, E.; Sobierajska-Rek, A.; Śledzińska, K.; Małgorzewicz, S.; Jassem, E.; Wierzba, J. Morbidity, Clinical Course and Vaccination against SARS-CoV-2 Virus in Patients with Duchenne Muscular Dystrophy: A Patient Reported Survey. Int. J. Environ. Res. Public Health 2022, 19, 406. [Google Scholar] [CrossRef]
- Rath, A.; Olry, A.; Dhombres, F.; Brandt, M.M.; Urbero, B.; Ayme, S. Representation of rare diseases in health information systems: The Orphanet approach to serve a wide range of end users. Hum. Mutat. 2012, 33, 803–808. [Google Scholar] [CrossRef]
- EURORDIS. Rare Diseases: Understanding This Public Health Priority; EURORDIS: Paris, France, 2011; Available online: https://cutt.ly/TPATXaQ (accessed on 16 November 2021).
- Rodwell, C.; Aymé, S. Rare disease policies to improve care for patients in Europe. Biochim. Biophys. Acta 2015, 1852, 2329–2335. [Google Scholar] [CrossRef] [Green Version]
- Federación Española de Enfermedades Raras. Misión, Visión y Valores; Federación Española de Enfermedades Raras: Madrid, Spain, 2022; Available online: https://cutt.ly/tPFWgAN (accessed on 23 February 2022).
- González-Gil, F.; Pastor-Martín, M.E.; Poy, R. Educación inclusiva: Barreras y facilitadores para su desarrollo. Un estudio desde la percepción del profesorado. Profr. Rev. Currículum Form. Profr. 2019, 23, 243–263. [Google Scholar] [CrossRef]
- Pérez-Gutiérrez, R.; Casado-Muñoz, R.; Rodríguez-Conde, M. Evolución del profesorado de apoyo hacia la educación inclusiva: Una perspectiva legislativa autonómica en España. Rev. Complut. Educ. 2021, 32, 285–295. [Google Scholar] [CrossRef]
- Perlado, I.; Muñoz, Y.; Torrego, J.C. Implicaciones de la formación del profesorado en aprendizaje cooperativo para la educación inclusiva. Profr. Rev. Currículum Form. Profr. 2019, 23, 128–151. [Google Scholar] [CrossRef] [Green Version]
- Federación Española de Enfermedades Raras. Estudio Sobre Situación de Necesidades Sociosanitarias de las Personas con Enfermedades Raras en España. Estudio ENSERio Datos 2016–2017; FEDER: Madrid, Spain; CREER: Burgos, Spain, 2018; Available online: https://cutt.ly/vPFJ2zb (accessed on 20 December 2021).
- Ministerio de Educación y Formación Profesional. Estadísticas del Profesorado y Otro Personal; Ministerio de Educación y Formación Profesional: Madrid, Spain, 2022. Available online: https://cutt.ly/bGGRbeB (accessed on 11 March 2022).
- Álvarez-Castillo, J.; Buenestado-Fernández, M. Predictores de las actitudes hacia la inclusión de alumnado con necesidades educativas especiales en futuros profesionales de la educación. Rev. Complut. Educ. 2015, 26, 627–645. [Google Scholar] [CrossRef]
- Sharma, U.; Dt Kate, J. Predicting in-service educators’ intentions to teach in inclusive classrooms in India and Australia. Teach. Teach. Educ. 2016, 55, 13–23. [Google Scholar] [CrossRef]
- Colmenero, M.J.; Pantoja, A.; Pegajalar, M.C. Percepciones sobre atención a la diversidad en la formación inicial del profesorado en Educación Secundaria. Rev. Complut. Educ. 2015, 26, 101–120. [Google Scholar] [CrossRef]
- Collado-Sanchís, A.; Tárraga-Mínguez, R.; Lacruz-Pérez, I.; Sanz-Cervera, P. Analysis of teachers’ attitudes and perceived self-efficacy towards inclusive education. Educar 2020, 56, 509–523. [Google Scholar] [CrossRef]
- Falla, D.; Alejandres, C.; Gil del Pino, C. Engagement en la formación docente como impulsor de actitudes inclusivas. Educ. XX1 2022, 25, 251–271. [Google Scholar] [CrossRef]
- Florian, L.; Camedda, D. Enhancing teacher education for inclusion. Eur. J. Teach. Educ. 2020, 43, 4–8. [Google Scholar] [CrossRef]
- Quesada, M.I. Metodologías inclusivas y emergentes para la formación docente en inclusión educativa. Rev. Int. Apoyo A Inclusión Logop. Soc. Y Multicult. 2021, 7, 110–117. [Google Scholar] [CrossRef]
- Gallegos, M. La Inclusión de las TIC en la Educación de Personas con Discapacidad. Relatos de Experiencias; Editorial Universitaria Abya-Yala: Quito, Ecuador, 2018. [Google Scholar]
- García-Perales, R.; Palomares-Ruiz, A. Education in Programming and Mathematical Learning: Functionality of a Programming Language in Educational Processes. Sustainability 2020, 12, 10129. [Google Scholar] [CrossRef]
- Palomares-Ruiz, A.; García-Perales, R. Math Performance and Sex: The Predictive Capacity of Self-Efficacy, Interest and Motivation for Learning Mathematics. Front. Psychol. 2020, 11, 1879. [Google Scholar] [CrossRef]
- López-Fernández, O. Emerging Health and Education Issues Related to Internet Technologies and Addictive Problems. Int. J. Environ. Res. Public Health 2021, 18, 321. [Google Scholar] [CrossRef]
- García-Perales, R.; Almeida, L. Programa de enriquecimiento para alumnado con alta capacidad: Efectos positivos para el currículum. Comunicar 2019, 60, 39–48. [Google Scholar] [CrossRef]
- Cejudo, J.; Losada, L.; Feltrero, R. Promoting Social and Emotional Learning and Subjective Well-Being: Impact of the “Aislados” Intervention Program in Adolescents. Int. J. Environ. Res. Public Health 2020, 17, 609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palomares-Ruiz, A.; García-Perales, R.; Cebrián-Martínez, A.; Martín-García, M.I. Bullying and Cyberbullying in Primary School: The Impact of Gender and Student Academic Performance. Sustainability 2021, 13, 7316. [Google Scholar] [CrossRef]
- Orphanet. Estimación de la Prevalencia Puntual Acumulada de Enfermedades Raras: Análisis de la Base de Datos de Orphanet; Orphanet: Paris, France, 2020; Available online: https://cutt.ly/8AqRodO (accessed on 22 November 2021).
- Jaffe, A.; Zurynski, Y.; Beville, L.; Elliott, E. Call for a national plan for rare diseases. J. Paediatr. Child Health 2010, 46, 2–4. [Google Scholar] [CrossRef]
- Schieppati, A.; Henter, J.I.; Daina, E.; Aperia, A. Why rare diseases are an important medical and social issue. Lancet 2008, 371, 2039–2041. [Google Scholar] [CrossRef]
- Tambuyzer, E. Rare diseases, orphan drugs and their regulation: Questions and misconceptions. Nat. Rev. Drug Discov. 2010, 9, 921–929. [Google Scholar] [CrossRef]
- Song, P.; Gao, J.; Inagaki, Y.; Kokudo, N.; Tang, W. Rare diseases, orphan drugs, and their regulation in Asia: Current status and future perspectives. Intractable Rare Dis. Res. 2012, 1, 3–9. [Google Scholar] [CrossRef] [Green Version]
- Navarro-Montaño, M.; López-Martínez, A.; Rodríguez-Gallego, M. Research on Quality Indicators to Guide Teacher Training to Promote an Inclusive Educational Model. Rev. Electrón. Educ. 2021, 25, 182–200. [Google Scholar] [CrossRef]
- Arnaiz, P.; Guirao, J.M. La autoevaluación de centros en España para la atención a la diversidad desde una perspectiva inclusiva: ACADI. Rev. Electrón. Interuniv. Form. Profr. 2015, 18, 45–101. [Google Scholar] [CrossRef] [Green Version]
- Oriola-Requena, S.; Cascales-Ribera, J. Liderazgo y legislación educativa como fundamentos para la acción directiva escolar. Un estudio descriptivo en el contexto de Cataluña. Profr. Rev. Currículum Form. Profr. 2019, 23, 41–58. [Google Scholar] [CrossRef]
- Berrocal-Acedo, M.; Benito-Lozano, J.; Alonso-Ferreira, V.; Vilches-Arenas, A. Retraso diagnóstico en enfermedades raras: Revisión sistemática. Rev. Esp. Salud Pública 2022, 96, e1–e16. Available online: https://cutt.ly/wGKL2Iw (accessed on 18 February 2022).




{kind=link}
{kind=link}
{kind=link}
| Dimension | Items |
|---|---|
| Conceptualization | 1. I know what a rare disease is 2. I know the categories that the different types of rare diseases fall into 3. I know how prevalent the rare diseases I have dealt with in my school are at a national or international level. 4. When I have had a student with a rare disease in my class, I knew what their main characteristics were 5. I have maintained contact from the school with patient advocacy groups that deal with rare diseases |
| Legislation | 6. I know the educational inclusion legislation in our region 7. I know the content of the most recent education legislation, especially about student educational needs 8. I have read and understand the article in the Spanish Constitution which describes the right to education for all 9. I understand the importance of there being a law aimed at educational inclusion 10. Within my teaching, I believe inclusive education to be important, and therefore the principles of inclusion must be applied in the classroom |
| Intervention | 11. I have had, or still have, a student in my class with a rare disease 12. I have educated myself about the signs and symptoms students may exhibit if they suffer from a rare disease 13. I think the family-school relationship is essential for proper intervention for students with rare diseases 14. I know specific activities to do with these students15. I am able to advise and guide other teachers about activities with these students |
| Diagnosis | 16. I know the warning signs a student with a possible rare disease may present 17. I educate myself and try to contact other diagnosed cases in order to improve the education I give to students with rare diseases that I might encounter as a teacher 18. I know how to clinically diagnose a rare disease 19. I think the relationship between the school and the families is essential in order to be able to properly detect and help an initial diagnosis 20. I am aware of the need for more research to help diagnosis and treatment |
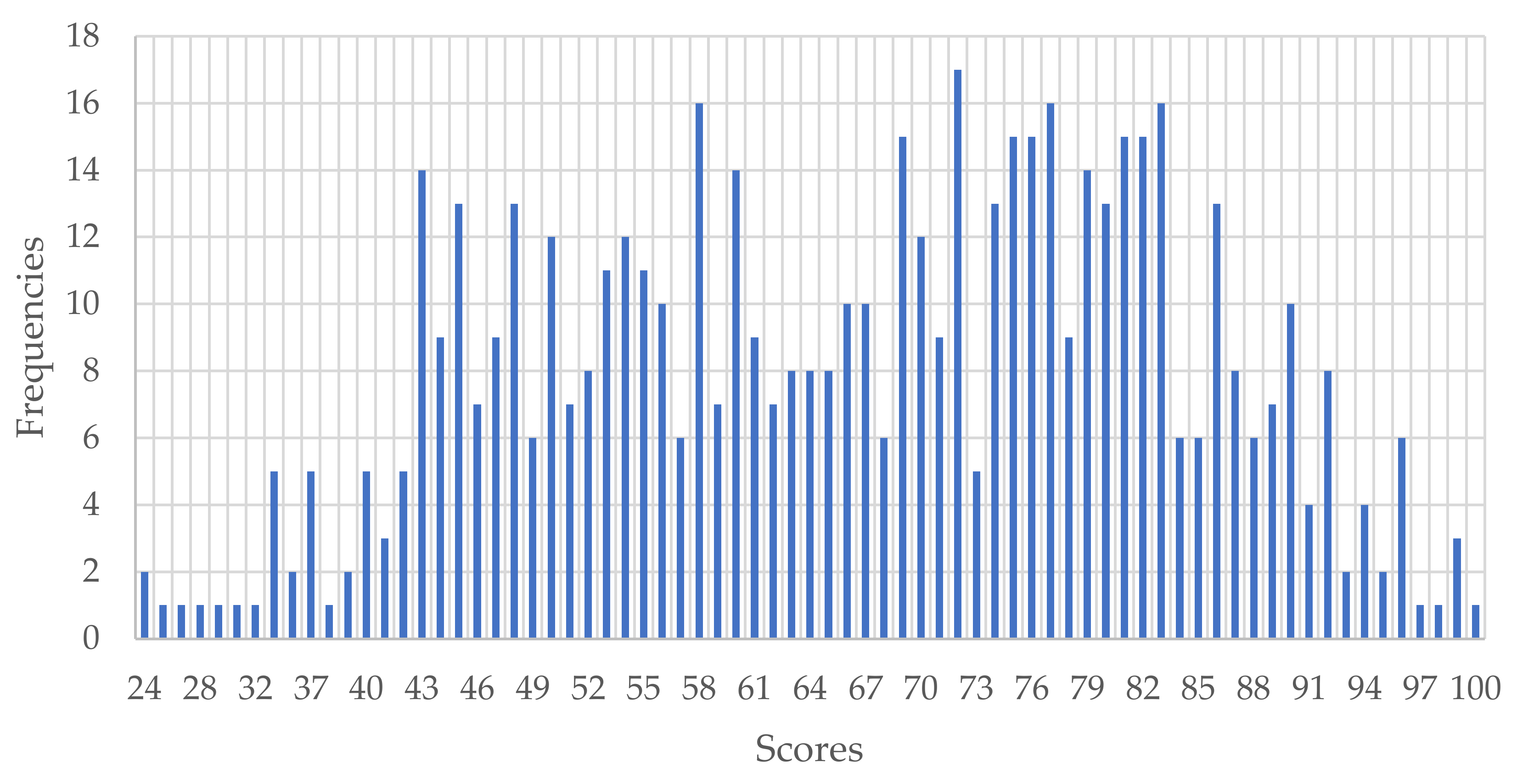
| Minimum | Maximum | M | SD | Asymmetry | Kurtosis |
|---|---|---|---|---|---|
| 24 | 100 | 66.49 | 16.41 | −0.19 | −0.82 |
| Item | Scores | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | ||||||
| F | % | f | % | f | % | f | % | f | % | |
| IT1 | 14 | 2.44 | 74 | 12.89 | 125 | 21.78 | 174 | 30.31 | 187 | 32.58 |
| IT2 | 246 | 42.86 | 147 | 25.61 | 114 | 19.86 | 51 | 8.89 | 16 | 2.79 |
| IT3 | 228 | 39.72 | 133 | 23.17 | 107 | 18.64 | 65 | 11.32 | 41 | 7.14 |
| IT4 | 66 | 11.50 | 132 | 23.00 | 132 | 23.00 | 156 | 27.18 | 88 | 15.33 |
| IT5 | 146 | 25.44 | 129 | 22.47 | 117 | 20.38 | 119 | 20.73 | 63 | 10.98 |
| Item | M | SD | Asymmetry | Kurtosis |
|---|---|---|---|---|
| IT1 | 3.78 | 1.11 | −0.55 | −0.65 |
| IT2 | 2.03 | 1.11 | 0.82 | −0.25 |
| IT3 | 2.23 | 1.28 | 0.72 | −0.62 |
| IT4 | 3.12 | 1.25 | −0.11 | −1.04 |
| IT5 | 2.69 | 1.34 | 0.21 | −1.18 |
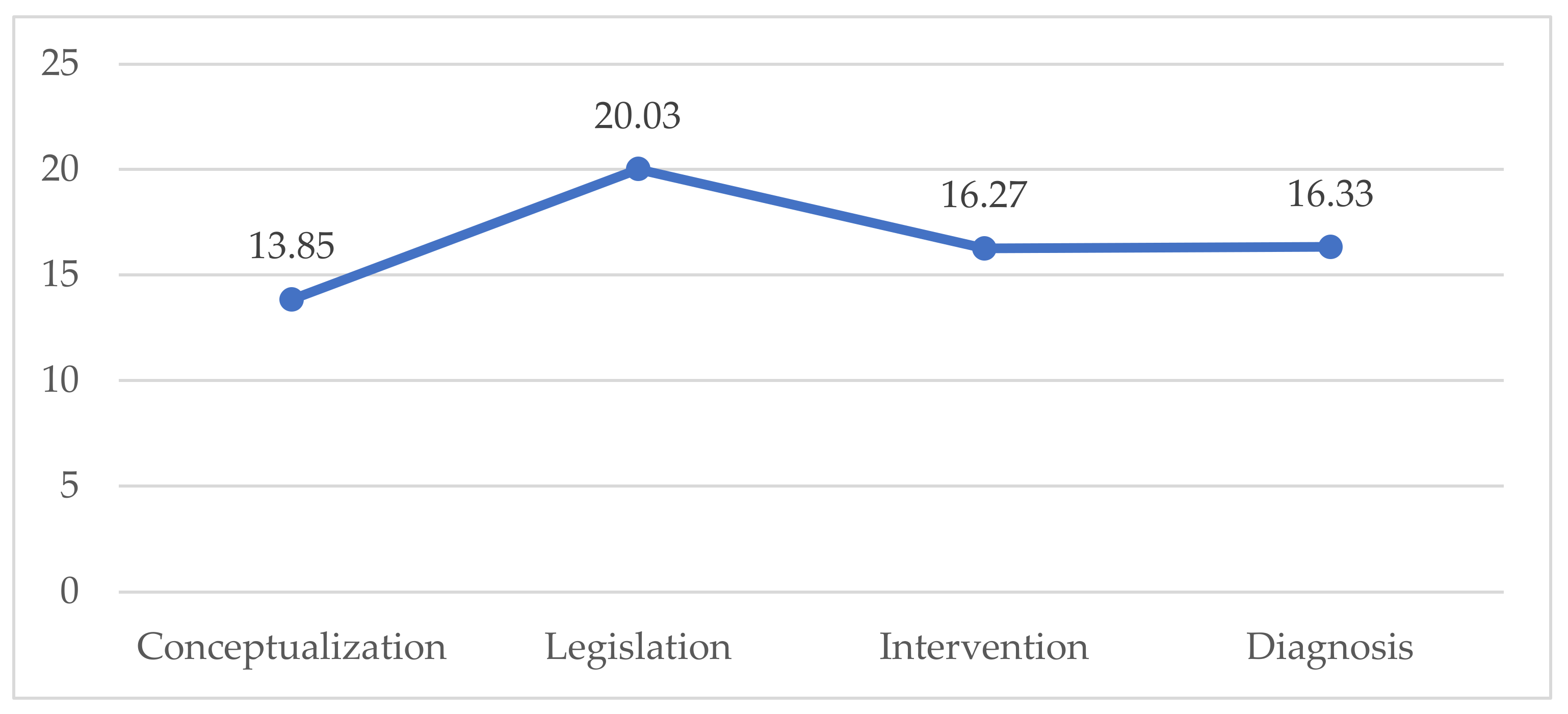
| Total | 13.85 | 4.74 | 0.20 | −0.88 |
| Item | Scores | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | ||||||
| F | % | f | % | f | % | f | % | f | % | |
| IT6 | 34 | 5.92 | 43 | 7.49 | 118 | 20.56 | 157 | 27.35 | 222 | 38.68 |
| IT7 | 118 | 20.56 | 80 | 13.94 | 97 | 16.90 | 134 | 23.34 | 145 | 25.26 |
| IT8 | 18 | 3.14 | 39 | 6.79 | 95 | 16.55 | 150 | 26.13 | 272 | 47.39 |
| IT9 | 6 | 1.05 | 9 | 1.57 | 57 | 9.93 | 135 | 23.52 | 367 | 63.94 |
| IT10 | 8 | 1.39 | 14 | 2.44 | 51 | 8.89 | 147 | 25.61 | 354 | 61.67 |
| Item | M | SD | Asymmetry | Kurtosis |
|---|---|---|---|---|
| IT6 | 3.85 | 1.19 | −0.84 | −0.15 |
| IT7 | 3.19 | 1.47 | −0.24 | −1.34 |
| IT8 | 4.08 | 1.09 | −1.06 | 0.31 |
| IT9 | 4.48 | 0.82 | −1.71 | 2.99 |
| IT10 | 4.44 | 0.86 | −1.73 | 3.03 |
| Total | 20.03 | 4.10 | −0.66 | −0.18 |
| Item | Scores | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | ||||||
| f | % | f | % | f | % | f | % | f | % | |
| IT11 | 191 | 33.28 | 127 | 22.13 | 82 | 14.29 | 61 | 10.63 | 113 | 19.69 |
| IT12 | 78 | 13.59 | 79 | 13.76 | 57 | 9.93 | 124 | 21.60 | 236 | 41.11 |
| IT13 | 10 | 1.74 | 19 | 3.31 | 39 | 6.79 | 112 | 19.51 | 394 | 68.64 |
| IT14 | 106 | 18.47 | 125 | 21.78 | 121 | 21.08 | 135 | 23.52 | 87 | 15.16 |
| IT15 | 201 | 35.02 | 86 | 14.98 | 111 | 19.34 | 105 | 18.29 | 71 | 12.37 |
| Item | M | SD | Asymmetry | Kurtosis |
|---|---|---|---|---|
| IT11 | 2.61 | 1.52 | 0.44 | −1.28 |
| IT12 | 3.63 | 1.47 | −0.64 | −1.06 |
| IT13 | 4.50 | 0.89 | −2.03 | 3.88 |
| IT14 | 2.95 | 1.34 | 0.01 | −1.20 |
| IT15 | 2.58 | 1.43 | 0.30 | −1.29 |
| Total | 16.27 | 5.40 | −0.10 | −1.11 |
| Item | Scores | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | ||||||
| f | % | f | % | f | % | f | % | f | % | |
| IT16 | 160 | 27.87 | 146 | 25.44 | 130 | 22.65 | 107 | 18.64 | 31 | 5.40 |
| IT17 | 106 | 18.47 | 127 | 22.13 | 121 | 21.08 | 144 | 25.09 | 76 | 13.24 |
| IT18 | 278 | 48.43 | 126 | 21.95 | 103 | 17.94 | 45 | 7.84 | 22 | 3.83 |
| IT19 | 24 | 4.18 | 41 | 7.14 | 53 | 9.23 | 113 | 19.69 | 343 | 59.76 |
| IT20 | 7 | 1.22 | 9 | 1.57 | 18 | 3.14 | 68 | 11.85 | 472 | 82.23 |
| Item | M | SD | Asymmetry | Kurtosis |
|---|---|---|---|---|
| IT16 | 2.48 | 1.23 | 0.33 | −0.99 |
| IT17 | 2.93 | 1.32 | 0.00 | −1.18 |
| IT18 | 1.97 | 1.15 | 0.98 | −0.00 |
| IT19 | 4.24 | 1.14 | −1.45 | 1.07 |
| IT20 | 4.72 | 0.71 | −3.18 | 10.99 |
| Total | 16.33 | 4.22 | −0.26 | −0.36 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Perales, R.; Palomares-Ruiz, A.; Ordóñez-García, L.; García-Toledano, E. Rare Diseases in the Educational Field: Knowledge and Perceptions of Spanish Teachers. Int. J. Environ. Res. Public Health 2022, 19, 6057. https://doi.org/10.3390/ijerph19106057
García-Perales R, Palomares-Ruiz A, Ordóñez-García L, García-Toledano E. Rare Diseases in the Educational Field: Knowledge and Perceptions of Spanish Teachers. International Journal of Environmental Research and Public Health. 2022; 19(10):6057. https://doi.org/10.3390/ijerph19106057
Chicago/Turabian StyleGarcía-Perales, Ramón, Ascensión Palomares-Ruiz, Lydia Ordóñez-García, and Eduardo García-Toledano. 2022. "Rare Diseases in the Educational Field: Knowledge and Perceptions of Spanish Teachers" International Journal of Environmental Research and Public Health 19, no. 10: 6057. https://doi.org/10.3390/ijerph19106057