
Effects of Kangaroo Mother Care in the NICU on the Physiological Stress Parameters of Premature Infants: A Meta-Analysis of RCTs

 , , and
, , and
Abstract
:1. Background
2. Patients and Methods
2.1. Search Strategy and Selection Criteria
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Risk of Bias Assessment
2.5. Statistical Analysis
3. Results
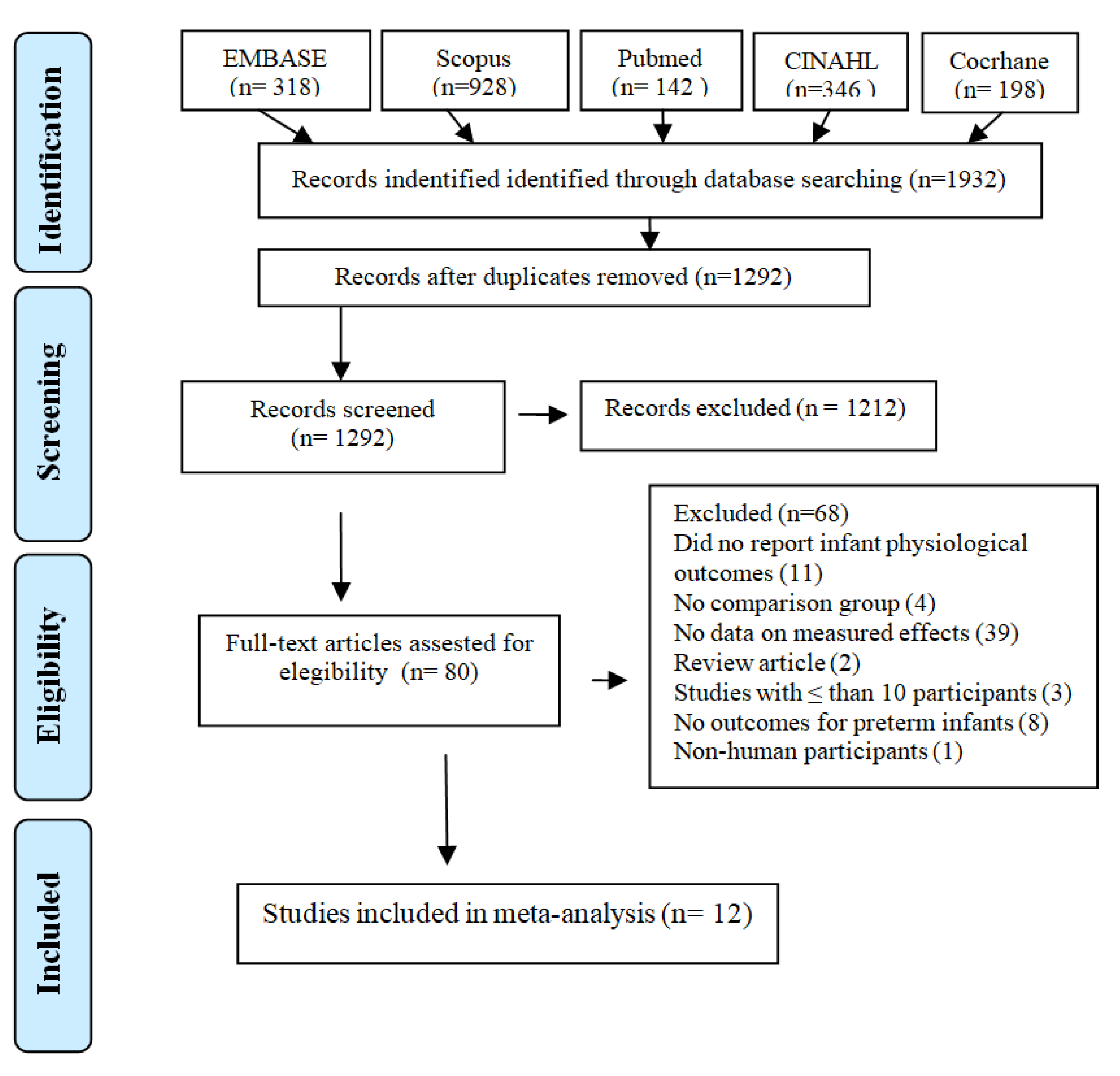
3.1. Study Selection
3.2. Characteristics of Included Studies
3.3. Risk of Bias Assessment
3.4. Meta-Analyses
3.5. Heart Rate
3.6. Respiratory Rate
3.7. Oxygen Saturation
3.8. Temperature
4. Discussion
Implications for Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gao, H.; Xu, G.; Gao, H.; Dong, R.; Fu, H.; Wang, D.; Zhang, H.; Zhang, H. Effect of repeated Kangaroo Mother Care on repeated procedural pain in preterm infants: A randomized controlled trial. Int. J. Nurs. Stud. 2015, 52, 1157–1165. [Google Scholar] [CrossRef]
- Cong, X.; Wu, J.; Vittner, D.; Xu, W.; Hussain, N.; Galvin, S.; Fitzsimons, M.; McGrath, J.; Henderson, W. The impact of cumulative pain/stress on neurobehavioral development of preterm infants in the NICU. Early Hum. Dev. 2017, 108, 9–16. [Google Scholar] [CrossRef] [Green Version]
- Blume-Peytavi, U.; Lavender, T.; Jenerowicz, D.; Ryumina, I.; Stalder, J.; Torrelo, A.; Cork, M. Recommendations from a European Roundtable Meeting on Best Practice Healthy Infant Skin Care. Pediatric Dermatol. 2016, 33, 311–321. [Google Scholar] [CrossRef] [Green Version]
- Medina, I.M.F.; Granero-Molina, J.; Fernández-Sola, C.; Hernández-Padilla, J.M.; Avila, M.C.; Rodríguez, M.D.M.L. Bonding in neonatal intensive care units: Experiences of extremely preterm infants’ mothers. Women Birth 2018, 31, 325–330. [Google Scholar] [CrossRef]
- Cho, E.-S.; Kim, S.-J.; Kwon, M.S.; Cho, H.; Kim, E.H.; Jun, E.-M.; Lee, S. The Effects of Kangaroo Care in the Neonatal Intensive Care Unit on the Physiological Functions of Preterm Infants, Maternal–Infant Attachment, and Maternal Stress. J. Pediatric Nurs. 2016, 31, 430–438. [Google Scholar] [CrossRef]
- Chan, G.J.; Valsangkar, B.; Kajeepeta, S.; Boundy, E.O.; Wall, S. What is kangaroo mother care? Systematic review of the literature. J. Glob. Health 2016, 6, 010701. [Google Scholar] [CrossRef] [PubMed]
- Nyqvist, K.H.; Anderson, G.C.; Bergman, N.; Cattaneo, A.; Charpak, N.; DaVanzo, R.; Ewald, U.; Ibe, O.; Ludington-Hoe, S.; Mendoza, S.; et al. Towards universal Kangaroo Mother Care: Recommendations and report from the First European conference and Seventh International Workshop on Kangaroo Mother Care. Acta Paediatr. 2010, 99, 820–826. [Google Scholar] [CrossRef] [PubMed]
- Moore, E.R.; Anderson, G.C.; Bergman, N.; Dowswell, T. Early skin-to-skin contact for mothers and their healthy newborn infants. Cochrane Database Syst. Rev. 2012, 5, CD003519. [Google Scholar] [CrossRef] [Green Version]
- Luong, K.C.; Nguyen, T.L.; Thi, D.H.H.; Carrara, H.P.; Bergman, N.J. Newly born low birthweight infants stabilise better in skin-to-skin contact than when separated from their mothers: A randomised controlled trial. Acta Paediatr. 2015, 105, 381–390. [Google Scholar] [CrossRef] [PubMed]
- Ionio, C.; Ciuffo, G.; Landoni, M. Parent–Infant Skin-to-Skin Contact and Stress Regulation: A Systematic Review of the Literature. Int. J. Environ. Res. Public Health 2021, 18, 4695. [Google Scholar] [CrossRef]
- De Almeida, H.; Venancio, S.I.; Sanches, M.T.C.; Onuki, D. The impact of kangaroo care on exclusive breastfeeding in low birth weight newborns. J. Pediatrics 2010, 86, 250–253. [Google Scholar] [CrossRef] [Green Version]
- Bieleninik, Ł.; Ettenberger, M.; Epstein, S.; Elefant, C.; Arnon, S. Potential Psychological and Biological Mechanisms Underlying the Effectiveness of Neonatal Music Therapy during Kangaroo Mother Care for Preterm Infants and Their Parents. Int. J. Environ. Res. Public Health 2021, 18, 8557. [Google Scholar] [CrossRef] [PubMed]
- Bera, A.; Ghosh, J.; Singh, A.K.; Hazra, A.; Som, T.; Munian, D. Effect of Kangaroo mother care on vital physiological parameters of the low birth weight newborn. Indian J. Community Med. 2014, 39, 245–249. [Google Scholar] [CrossRef] [PubMed]
- Pados, B.F. Physiology of Stress and Use of Skin-to-Skin Care as a Stress-Reducing Intervention in the NICU. Nurs. Women’s Health 2019, 23, 59–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charpak, N.; Tessier, R.; Ruiz, J.G.; Hernandez, J.T.; Uriza, F.; Villegas, J.; Nadeau, L.; Mercier, C.; Maheu, F.; Marin, J.; et al. Twenty-year Follow-up of Kangaroo Mother Care Versus Traditional Care. Pediatrics 2017, 139, e20162063. [Google Scholar] [CrossRef] [Green Version]
- Campbell-Yeo, M.; Johnston, C.C.; Benoit, B.; Disher, T.; Caddell, K.; Vincer, M.; Walker, C.-D.; Latimer, M.; Streiner, D.L.; Inglis, D. Sustained efficacy of kangaroo care for repeated painful procedures over neonatal intensive care unit hospitalization: A single-blind randomized controlled trial. Pain 2019, 160, 2580–2588. [Google Scholar] [CrossRef] [PubMed]
- Mekonnen, A.G.; Yehualashet, S.S.; Bayleyegn, A.D. The effects of kangaroo mother care on the time to breastfeeding initiation among preterm and LBW infants: A meta-analysis of published studies. Int. Breastfeed. J. 2019, 14, 12. [Google Scholar] [CrossRef]
- Boundy, E.O.; Dastjerdi, R.; Spiegelman, D.; Fawzi, W.W.; Missmer, S.A.; Lieberman, E.; Kajeepeta, S.; Wall, S.; Chan, G.J. Kangaroo Mother Care and Neonatal Outcomes: A Meta-analysis. Pediatrics 2016, 137, e20152238. [Google Scholar] [CrossRef] [Green Version]
- Conde-Agudelo, A.; Belizán, J.M. Kangaroo mother care to reduce morbidity and mortality in low birthweight infants. Cochrane Database Syst. Rev. 2003, 2, CD002771. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miltersteiner, A.R.; Miltersteiner, D.R.; Rech, V.V.; Molle, L.D. Respostas fisiológicas da Posição Mãe-Canguru em bebês pré-termos, de baixo peso e ventilando espontaneamente. Rev. Bras. Saúde Matern. Infant. 2003, 3, 447–455. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Bang, K.-S. The Effects of Kangaroo Care on Maternal Self-esteem and Premature Infants’ Physiological Stability. Korean J. Women Health Nurs. 2011, 17, 454–462. [Google Scholar] [CrossRef] [Green Version]
- Ludington-Hoe, S.M.; Anderson, G.C.; Swinth, J.Y.; Thompson, C.; Hadeed, A.J. Randomized Controlled Trial of Kangaroo Care: Cardiorespiratory and Thermal Effects on Healthy Preterm Infants. Neonatal Netw. 2004, 23, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Forde, D.; Deming, D.D.; Tan, J.B.; Phillips, R.M.; Fry-Bowers, E.K.; Barger, M.K.; Bahjri, K.; Angeles, D.M.; Boskovic, D.S. Oxidative Stress Biomarker Decreased in Preterm Neonates Treated With Kangaroo Mother Care. Biol. Res. Nurs. 2020, 22, 188–196. [Google Scholar] [CrossRef]
- Kadam, S.; Binoy, S.; Kanbur, W.; Mondkar, J.A.; Fernandez, A. Feasibility of kangaroo mother care in Mumbai. Indian J. Pediatrics 2005, 72, 35–38. [Google Scholar] [CrossRef]
- Maastrup, R.; Greisen, G. Extremely preterm infants tolerate skin-to-skin contact during the first weeks of life. Acta Paediatr. 2010, 99, 1145–1149. [Google Scholar] [CrossRef]
- Bloch-Salisbury, E.; Zuzarte, I.; Indic, P.; Bednarek, F.; Paydarfar, D. Kangaroo care: Cardio-respiratory relationships between the infant and caregiver. Early Hum. Dev. 2014, 90, 843–850. [Google Scholar] [CrossRef]
- Legault, M.; Goulet, C. Comparison of Kangaroo Traditional Methods of Removing Preterm Infants From Incubators. J. Obstet. Gynecol. Neonatal Nurs. 1995, 24, 501–506. [Google Scholar] [CrossRef]
- Lorenz, L.; Dawson, J.; Jones, H.; Jacobs, S.E.; Cheong, J.; Donath, S.; Davis, P.G.; Kamlin, C.O.F. Skin-to-skin care in preterm infants receiving respiratory support does not lead to physiological instability. Arch. Dis. Child. Fetal Neonatal Ed. 2017, 102, F339–F344. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, L.; Marulli, A.; Dawson, J.; Owen, L.S.; Manley, B.J.; Donath, S.M.; Davis, P.G.; Kamlin, C.O.F. Cerebral oxygenation during skin-to-skin care in preterm infants not receiving respiratory support. Arch. Dis. Child. Fetal Neonatal Ed. 2017, 103, F137–F142. [Google Scholar] [CrossRef] [PubMed]
- Özdel, D.; Sarı, H.Y. Effects of the prone position and kangaroo care on gastric residual volume, vital signs and comfort in preterm infants. Jpn. J. Nurs. Sci. 2020, 17, e12287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pados, B.; Hess, F. Systematic Review of the Effects of Skin-to-Skin Care on Short-Term Physiologic Stress Outcomes in Preterm Infants in the Neonatal Intensive Care Unit. Adv. Neonatal Care 2020, 20, 48–58. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Country | KMC and Comparison Group | N | Gestational Age Mean (SD) or Median (IQR) | Birth Weight (g) | KMC Duration | Physiologic Parameter Measured |
|---|---|---|---|---|---|---|---|
| Legault, 1995 | Canada | KMC compared traditional method | 61 | 30 (24–35) | 1225 (685–1835) | 30 min | HR, BR O2sat, Tº |
| Miltersteiner, 2003 | Brazil | KMC compared incubator | 23 | 34.1 ± 1.88 | 1740 ± 280.04 | 60 min | HR, BR O2sat, Tº |
| Ludington-Hoe, 2004 | USA | KMC compared to standard care | 24 | (KMC) 33.55 ± 1.57 | 1467 ± 228 | 180 min | HR, BR O2sat, Tº |
| (CC) 34.42 ± 1.08 | 14,611 ± 217 | ||||||
| Kadam, 2005 | India | KMC compared to conventional method of care | 89 | (KMC) 33.3 ± 2.1 | 1467 ± 228 | 9.8 ± 3.7 h | BR, O2sat |
| (CC) 34 ± 1.7 | 14,611± 217 | ||||||
| Maastrup, 2010 | Denmark | Skin-to-skin-contact | 22 | 25 (23–27) | 735 (460–1050) | 98 (51–387) min | HR, RR O2sat, Tº |
| Lee, 2011 | South Korea | KMC compared to Conventional Care | 34 | (KMC) 27.50 ± 2.89 | 990 ± 360 | 30 min | HR, RR O2sat, Tº |
| (CC) 29.87 ± 3.25 | 1180 ± 450 | ||||||
| Bloch-Salisbury, 2014 | USA | Compared with control group in incubator | 11 | 29.87 ± 2.74 | 1393 ± 127 | 41.3 ± 21.2 min | HR, RR O2sat, Tº |
| Cho, 2016 | South Korea | KC compare with routine care | 40 | (KMC) 30.12 ± 16.29 | 1660.00 ± 225.20 | 30 min | HR, RR O2sat, Tº |
| (CC) 28.81 ± 20.63 | 1442.00 ± 128.00 | ||||||
| Lorenz, 2017 | Australia | SSC compared with incubator | 40 | 27.6 (26.0–28.9) | 969 (817–1263) | 90 min | HR O2sat |
| Lorenz, 2018 | Australia | SSC compared with incubator | 40 | 30.6 (29.1–31.7) | 1370 (1062–1572) | 90 min | HR O2sat |
| Forde, 2020 | USA | KMC versus incubator care | 51 | (KMC) 32.00 ± 2.6 | 1827 ± 492 | 60 min | Tº |
| (CC) 31.40 ± 2.1 | 1642 ± 545 | ||||||
| Özdel, 2020 | Turkey | Prone position and kangaroo care | 30 | 30.20 ± 2.63 | 1455.43 ± 607.85 (593–3080) | 180 min | HR, RR O2sat, Tº |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cristóbal Cañadas, D.; Bonillo Perales, A.; Galera Martínez, R.; Casado-Belmonte, M.d.P.; Parrón Carreño, T. Effects of Kangaroo Mother Care in the NICU on the Physiological Stress Parameters of Premature Infants: A Meta-Analysis of RCTs. Int. J. Environ. Res. Public Health 2022, 19, 583. https://doi.org/10.3390/ijerph19010583
Cristóbal Cañadas D, Bonillo Perales A, Galera Martínez R, Casado-Belmonte MdP, Parrón Carreño T. Effects of Kangaroo Mother Care in the NICU on the Physiological Stress Parameters of Premature Infants: A Meta-Analysis of RCTs. International Journal of Environmental Research and Public Health. 2022; 19(1):583. https://doi.org/10.3390/ijerph19010583
Chicago/Turabian StyleCristóbal Cañadas, Delia, Antonio Bonillo Perales, Rafael Galera Martínez, María del Pilar Casado-Belmonte, and Tesifón Parrón Carreño. 2022. "Effects of Kangaroo Mother Care in the NICU on the Physiological Stress Parameters of Premature Infants: A Meta-Analysis of RCTs" International Journal of Environmental Research and Public Health 19, no. 1: 583. https://doi.org/10.3390/ijerph19010583