
Emotional Labor and Burnout of Public Health Nurses during the COVID-19 Pandemic: Mediating Effects of Perceived Health Status and Perceived Organizational Support


Abstract
:1. Introduction
1.1. Necessity of Study
1.2. Purpose
2. Methods
2.1. Study Design
2.2. Participants and Data Collection
2.3. Measures
2.3.1. General Characteristics of Participants
2.3.2. COVID-19 Pandemic-Related Psychological Burden
2.3.3. Burnout
2.3.4. Emotional Labor
2.3.5. PHS
2.3.6. POS
2.4. Data Analysis
3. Results
3.1. Psychological Burden, Burnout, and Related Factors
3.2. Correlations between Burnout and Related Factors
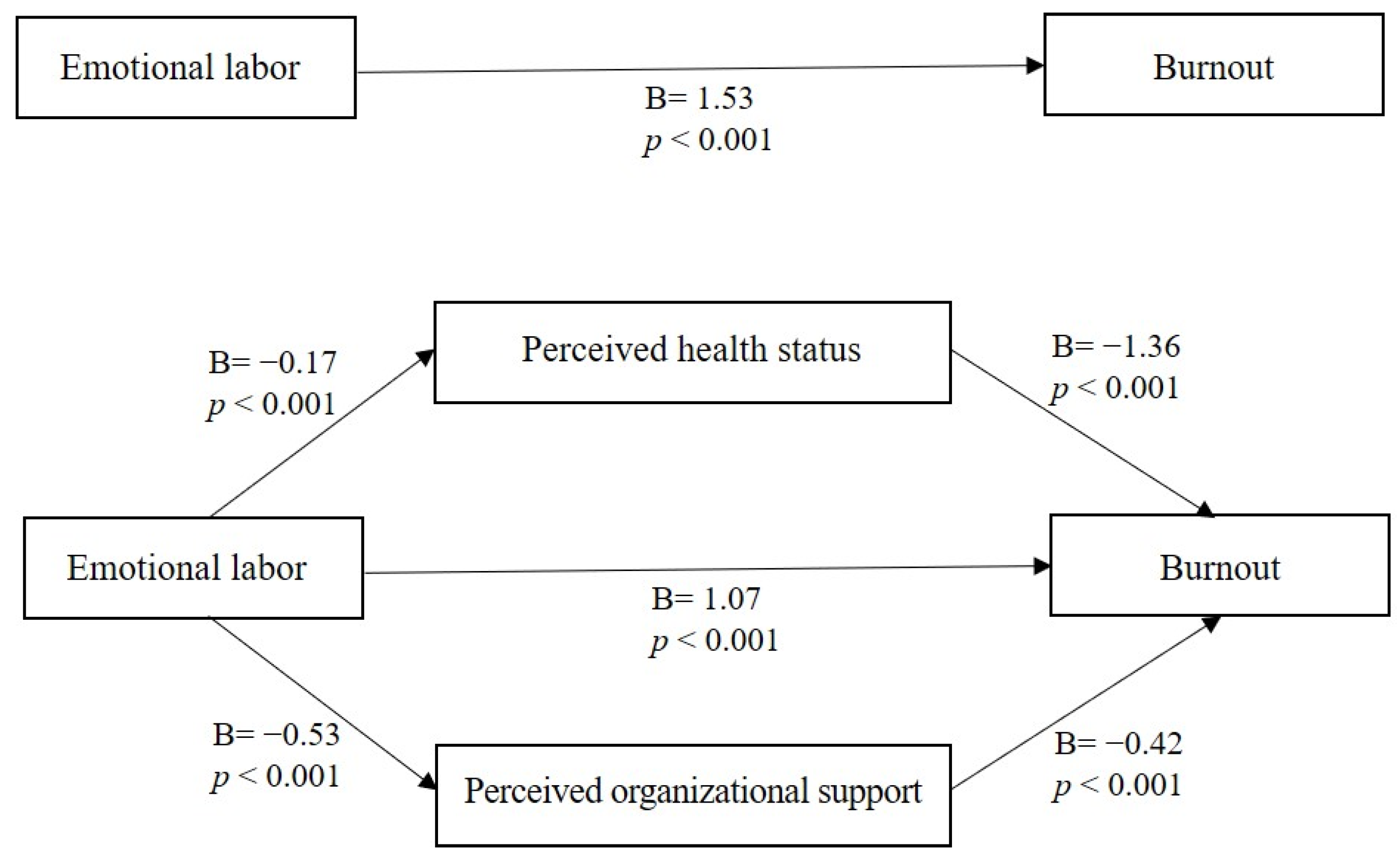
3.3. Mediating Effects of PHS and POS in the Association between Emotional Labor and Burnout
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Drevdahl, D.J.; Canales, M.K. Being a real nurse: A secondary qualitative analysis of how public health nurses rework their work identities. Nurs. Inq. 2020, 27, e12360. [Google Scholar] [CrossRef]
- Hayes, C.; Corrie, I.; Graham, Y. Paramedic emotional labour during COVID-19. J. Paramed. Pract. 2020, 12, 319–323. [Google Scholar] [CrossRef]
- Zhao, H.; He, Y.; Brister, F.; Yang, L.; Li, G.; Ling, Y.; Ying, Y. How Can Nursing Teams Respond to Large-Scale COVID-19 Screening? Front. Public Health 2021, 9, 681255. [Google Scholar] [CrossRef]
- Edmonds, J.K.; Kneipp, S.M.; Campbell, L. A call to action for public health nurses during the COVID-19 pandemic. Public Health Nurs. 2020, 37, 323–324. [Google Scholar] [CrossRef] [Green Version]
- Duarte, I.; Teixeira, A.; Castro, L.; Marina, S.; Ribeiro, C.; Jácome, C.; Martins, V.; Ribeiro-Vaz, I.; Pinheiro, H.C.; Silva, A.R.; et al. Burnout among Portuguese healthcare workers during the COVID-19 pandemic. BMC Public Health 2020, 20, 1885. [Google Scholar] [CrossRef]
- Stone, K.; Kintziger, K.; Jagger, M.; Horney, J. Public Health Workforce Burnout in the COVID-19 Response in the U.S. Int. J. Environ. Res. Public Health 2021, 18, 4369. [Google Scholar] [CrossRef]
- Hankyoreh News. Nurses at Public Health Centers after ‘Quarantine Burnout’ Increased by 1.5 Times. Available online: https://www.hani.co.kr/arti/society/health/1004767.html (accessed on 28 July 2021).
- Lee, N.; Lee, H.-J. South Korean Nurses’ Experiences with Patient Care at a COVID-19-Designated Hospital: Growth after the Frontline Battle against an Infectious Disease Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 9015. [Google Scholar] [CrossRef]
- Morgantini, L.A.; Naha, U.; Wang, H.; Francavilla, S.; Acar, Ö.; Flores, J.M.; Crivellaro, S.; Moreira, D.; Abern, M.; Eklund, M.; et al. Factors contributing to healthcare professional burnout during the COVID-19 pandemic: A rapid turnaround global survey. PLoS ONE 2020, 15, e0238217. [Google Scholar] [CrossRef]
- Aung, N.; Tewogbola, P. The impact of emotional labour on the health in the workplace: A narrative review of literature from 2013–2018. AIMS Public Health 2019, 6, 268–275. [Google Scholar] [CrossRef]
- Cao, X.; Chen, L.; Tian, L.; Diao, Y. The effect of perceived organisational support on burnout among community health nurses in China: The mediating role of professional self-concept. J. Nurs. Manag. 2015, 24, E77–E86. [Google Scholar] [CrossRef]
- Salvagioni, D.A.J.; Melanda, F.N.; Mesas, A.E.; González, A.D.; Gabani, F.L.; De Andrade, S.M. Physical, psychological and occupational consequences of job burnout: A systematic review of prospective studies. PLoS ONE 2017, 12, e0185781. [Google Scholar] [CrossRef]
- Søvold, L.E.; Naslund, J.A.; Kousoulis, A.A.; Saxena, S.; Qoronfleh, M.W.; Grobler, C.; Münter, L. Prioritizing the Mental Health and Well-Being of Healthcare Workers: An Urgent Global Public Health Priority. Front. Public Health 2021, 9, 679397. [Google Scholar] [CrossRef]
- Hanafin, S.; Cosgrove, J.; Hanafin, P.; Brady, A.-M.; Lynch, C. Burnout and its prevalence among public health nurses in Ireland. Br. J. Community Nurs. 2020, 25, 370–375. [Google Scholar] [CrossRef]
- Zaghini, F.; Biagioli, V.; Proietti, M.; Badolamenti, S.; Fiorini, J.; Sili, A. The role of occupational stress in the association between emotional labor and burnout in nurses: A cross-sectional study. Appl. Nurs. Res. 2020, 54, 151277. [Google Scholar] [CrossRef]
- Cho, K.S.; Kim, Y. Emotional Labor, Job Stress and Professional Quality of Life of Public Health Nurses according to the Employment Type. J. Korean Acad. Nurs. Adm. 2019, 25, 467–477. [Google Scholar] [CrossRef]
- Rose, S.; Hartnett, J.; Pillai, S. Healthcare worker’s emotions, perceived stressors and coping mechanisms during the COVID-19 pandemic. PLoS ONE 2021, 16, e0254252. [Google Scholar] [CrossRef]
- Kumar, S.; Shankar, B.; Singh, A.S.P. Emotional labor and health outcomes: An overview of literature and preliminary empirical evidences. Indian J. Soc. Sci. Res. 2010, 7, 83–89. [Google Scholar]
- Soto-Rubio, A.; Giménez-Espert, M.; Prado-Gascó, V. Effect of Emotional Intelligence and Psychosocial Risks on Burnout, Job Satisfaction, and Nurses’ Health during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 7998. [Google Scholar] [CrossRef]
- Yeh, S.C.J.; Chen, S.H.S.; Yuan, K.S.; Chou, W.; Wan, T.T.H. Emotional labor in health care: The moderating roles of per-sonality and the mediating role of sleep on job performance and satisfaction. Front. Psychol. 2020, 11, 574898. [Google Scholar] [CrossRef]
- Bukhari, S.R.; Alam, N.A.; Batool, A.; Hussain, Y.; Asim, S.; Khatttak, N.; Tabassum, S. Perceived Organizational Support Predicts Emotional Labor Among Nurses. Asian Soc. Sci. 2020, 16, 68. [Google Scholar] [CrossRef]
- Eisenberger, R.; Huntington, R. Perceived organizational support. J. Appl. Psychol. 1986, 71, 500–507. [Google Scholar] [CrossRef]
- Rhoades, L.; Eisenberger, R. Perceived organizational support: A review of the literature. J. Appl. Psychol. 2002, 87, 698–714. [Google Scholar] [CrossRef]
- Choi, Y. Perceived Organizational Support and Organizational Commitment in Hospital Nurses: Mediating and Moderating Effect of Resilience. Master’s Thesis, Yonsei University, Seoul, Korea, 2015. [Google Scholar]
- Lartey, J.K.S.; Amponsah-Tawiah, K.; Osafo, J. The moderating effect of perceived organizational support in the relationship between emotional labour and job attitudes: A study among health professionals. Nurs. Open 2019, 6, 990–997. [Google Scholar] [CrossRef]
- Kim, J. Emotional Labor Strategies, Stress, and Burnout among Hospital Nurses: A Path Analysis. J. Nurs. Sch. 2019, 52, 105–112. [Google Scholar] [CrossRef] [Green Version]
- Bobbio, A.; Bellan, M.; Manganelli, A.M. Empowering leadership, perceived organizational support, trust, and job burnout for nurses. Health Care Manag. Rev. 2012, 37, 77–87. [Google Scholar] [CrossRef]
- Grama, B.G.; Balas, M. Organizational support, emotional labor and burnout regarding the medical staff. Acta Med. Transilv. 2018, 23, 16–19. [Google Scholar]
- Pines, A.M.; Aronson, E.; Kafry, D. Burnout: From Tedium to Personal Growth; A Division of Macmilian Publishing Co., Inc.: New York, NY, USA, 1981. [Google Scholar]
- Morris, J.A.; Feldman, D.C. The Dimensions, Antecedents, and Consequences of Emotional Labor. Acad. Manag. Rev. 1996, 21, 986–1010. [Google Scholar] [CrossRef]
- Speake, D.L.; Cowart, M.E.; Pellet, K. Health perceptions and lifestyles of the elderly. Res. Nurs. Health 1989, 12, 93–100. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: Regression-Based Approach; Lee, H.K., Ed.; Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Cho, K.; Kim, B. The Psychological Responses of Nurses Caring for COVID-19 Patients: A Q Methodological Approach. Int. J. Environ. Res. Public Health 2021, 18, 3605. [Google Scholar] [CrossRef]
- Muz, G.; Yüce, G.E. Experiences of nurses caring for patients with COVID-19 in Turkey: A phenomenological enquiry. J. Nurs. Manag. 2021, 29, 1026–1035. [Google Scholar] [CrossRef]
- Dowell, J. What’s It Like Being a Public Health Nurse during the Pandemic? Available online: https://www.samuelmerritt.edu/news/whats-it-being-public-health-nurse-during-pandemic (accessed on 30 July 2021).
- Deng, H.; Wu, H.; Qi, X.; Jin, C.; Li, J. Stress Reactivity Influences the Relationship between Emotional Labor Strategies and Job Burnouts among Chinese Hospital Nurses. Neural Plast. 2020, 2020, 8837024. [Google Scholar] [CrossRef]
- Choi, H.; Ha, Y.; Yang, S. Relationships among emotional lab or, self-efficacy and burnout of employees in public health centers. Korean J. Occup Health Nurs. 2016, 25, 75–82. [Google Scholar] [CrossRef] [Green Version]
- Meier, K.J.; Mastracci, S.H.; Wilson, K. Gender and Emotional Labor in Public Organizations: An Empirical Examination of the Link to Performance. Public Adm. Rev. 2006, 66, 899–909. [Google Scholar] [CrossRef]
- Oh, Y.J.; Choi, Y.H. Effects of emotional labor, job stress and burnout on somatization in nurses: In convergence era. J. Digit. Converg. 2015, 13, 415–424. [Google Scholar] [CrossRef] [Green Version]
- Sohn, B.K.; Park, S.M.; Park, I.-J.; Hwang, J.Y.; Choi, J.-S.; Lee, J.-Y.; Jung, H.-Y. The Relationship between Emotional Labor and Job Stress among Hospital Workers. J. Korean Med. Sci. 2018, 33, e246. [Google Scholar] [CrossRef]
- Labrague, L.J.; de Los Santos, J.A.A. COVID-19 anxiety among front-line nurses: Predictive role of organisational support, personal resilience and social support. J. Nurs. Manag. 2020, 28, 1653–1661. Available online: https://onlinelibrary.wiley.com/doi/abs/10.1111/jonm.13121 (accessed on 8 July 2021). [CrossRef]
- Kang, J.; Jang, Y.Y.; Kim, J.; Han, S.-H.; Lee, K.R.; Kim, M.; Eom, J.S. South Korea’s responses to stop the COVID-19 pandemic. Am. J. Infect. Control 2020, 48, 1080–1086. [Google Scholar] [CrossRef]
- Burton, J. WHO Healthy Workplace Framework and Model: Background and Supportive Literature and Practices; World Health Organization: Geneva, Switzerland, 2010; Available online: https://www.who.int/occupational_health/healthy_workplace_framework.pdf (accessed on 28 July 2021).
- Latino, F.; Cataldi, S.; Fischetti, F. Effects of an 8-Week Yoga-Based Physical Exercise Intervention on Teachers’ Burnout. Sustainability 2021, 13, 2104. [Google Scholar] [CrossRef]
- Han, S.-S.; Han, J.-W.; Kim, Y.-H. Effect of Nurses’ Emotional Labor on Customer Orientation and Service Delivery: The Mediating Effects of Work Engagement and Burnout. Saf. Health Work 2018, 9, 441–446. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Categories | N (%) or M ± SD | Burnout | |
|---|---|---|---|---|
| M ± SD | t or F(p) Scheffe Test | |||
| Age | 37.4 ± 11.0 (22–59) | |||
| <30 | 76 (36.7) | 66.12 ± 14.36 | 5.44 (0.001) | |
| 30~39 | 51 (24.6) | 65.12 ± 14.29 | a, b, c > d | |
| 40~49 | 38 (18.4) | 62.82 ± 12.10 | ||
| ≥50 | 42 (20.3) | 56.36 ± 9.67 | ||
| Gender | Female | 199 (96.1) | 63.79 ± 13.18 | −2.71 (0.007) |
| male | 8 (3.9) | 50.75 ± 17.11 | ||
| Spouse | No | 93 (44.9) | 65.27 ± 13.71 | 1.92 (0.057) |
| Yes | 114 (55.1) | 61.67 ± 13.23 | ||
| Working institution | Public health care center | 181 (87.4) | 63.79 ± 13.59 | 1.42 (0.157) |
| Public health office | 26 (12.6) | 59.77 ± 12.81 | ||
| Employment type | Regular worker | 97 (46.9) | 64.84 ± 11.50 | 3.49 (<0.001) |
| Irregular workers | 110 (53.1) | 59.19 ± 11.70 | ||
| Total nurse career (years) | <5 | 101 (48.8) | 64.18 ± 13.90 | 1.11 (0.600) |
| ≥5 | 106 (51.2) | 62.43 ± 13.19 | ||
| Career of employment in healthcare center (year) | <3 | 90 (43.5) | 65.01 ± 14.01 | 1.62 (0.108) |
| ≥3 | 117 (56.5) | 61.96 ± 13.06 | ||
| Responsibilities * | Visiting nursing | 84 (40.6) | ||
| Infectious disease control | 66 (31.9) | |||
| Health promotion | 34 (16.4) | |||
| Vaccination | 31 (15.0) | |||
| Health administration | 26 (12.6) | |||
| Medical management | 7 (3.4) | |||
| Mental health | 12 (5.8) | |||
| Maternal and child health | 17(8.2) | |||
| Others | 37 (17.9) | |||
| Responsible business hours, Median (range) | 5.94 ± 3.01 (0–15) | |||
| <6 | 96 (46.4) | 65.25 ± 11.73 | 1.99 (0.048) | |
| ≥6 | 111 (53.6) | 61.59 ± 14.76 | ||
| COVID-19 related business hours, Median (range) | 4 (0–32) | |||
| <4 | 102 (48.3) | 60.07 ± 12.14 | −3.46 (<0.001) | |
| ≥4 | 105 (50.7) | 66.14 ± 14.13 | ||
| COVID-19 related complaints response time, Median (range) | 2 (0–55) | |||
| <2 | 75 (36.2) | 58.31 ± 14.17 | −4.14 (<0.001) | |
| ≥2 | 132 (63.8) | 66.11 ± 12.34 | ||
| Overtimes | 2 (0–24) | |||
| <2 | 83 (40.1) | 58.99 ± 13.88 | −3.86 (<0.001) | |
| ≥2 | 124 (59.9) | 66.16 ± 12.55 | ||
| Variables | M ± SD | Min-Max |
|---|---|---|
| COVID-19 pandemic related to psychological burden | ||
| Being stricter on one’s self than as required by the government with respect to social distancing and restrictions on personal life | 7.36 ± 2.37 | 0–10 |
| Overload of various work assigned additionally because of being a nurse | 7.09 ± 2.60 | 0–10 |
| Social expectations about sacrifice as a public servant and expectation of kind response | 6.84 ± 2.62 | 0–10 |
| Verbal and physical abuse from complaints | 6.06 ± 2.81 | 0–10 |
| Daily life of family members being restricted due to me | 6.65 ± 2.71 | 0–10 |
| Emotional labor | 31.55 ± 5.68 | 16–45 |
| Perceived health status | 9.09 ± 2.35 | 3–15 |
| Perceived organizational support | 32.82 ± 7.33 | 8–55 |
| Burnout | 63.29 ± 13.53 | 31–97 |
| Variables | Emotional Labor | Perceived Health Status | Perceived Organizational Support | Burnout |
|---|---|---|---|---|
| r (p) | r (p) | r (p) | r (p) | |
| Emotional labor | 1 | |||
| Perceived health status | −0.42 (<0.001) | 1 | ||
| Perceived organizational support | −0.41 (<0.001) | 0.38 (<0.001) | 1 | |
| Burnout | 0.64 (<0.001) | −0.51 (<0.001) | −0.51 (<0.001) | 1 |
| Variables | B | SE | t | p | 95% CI | |||
|---|---|---|---|---|---|---|---|---|
| Emotional labor→Perceived health status | −0.17 | 0.03 | −6.63 | <0.001 | −0.23~−0.12 | |||
| Emotional labor→Perceived organizational support | −0.53 | 0.08 | −6.49 | <0.001 | −0.69~0.37 | |||
| Emotional labor→Burnout | 1.07 | 0.13 | 8.03 | <0.001 | 0.81~1.33 | |||
| Perceived health status→Burnout | −1.36 | 0.32 | −4.31 | <0.001 | −1.99~−0.74 | |||
| Perceived organizational support→Burnout | −0.42 | 0.10 | −4.18 | <0.001 | −0.62~−0.22 | |||
| Variables | Directing effect | Indirect effect | ||||||
| B | Boot SE | 95% CI | B | Boot SE | 95% CI | |||
| Boot LLCI | Boot ULCI | Boot LLCI | Boot ULCI | |||||
| Emotional labor→Burnout | 1.07 | 0.13 | 0.81 | 1.33 | ||||
| Emotional labor →Perceived health status→Burnout | 0.24 | 0.07 | 0.11 | 0.39 | ||||
| Emotional labor→Perceived organizational support→Burnout | 0.23 | 0.09 | 0.07 | 0.42 | ||||
| Total | 0.46 | 0.10 | 0.29 | 0.68 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, M.-N.; Yoo, Y.-S.; Cho, O.-H.; Hwang, K.-H. Emotional Labor and Burnout of Public Health Nurses during the COVID-19 Pandemic: Mediating Effects of Perceived Health Status and Perceived Organizational Support. Int. J. Environ. Res. Public Health 2022, 19, 549. https://doi.org/10.3390/ijerph19010549
Kim M-N, Yoo Y-S, Cho O-H, Hwang K-H. Emotional Labor and Burnout of Public Health Nurses during the COVID-19 Pandemic: Mediating Effects of Perceived Health Status and Perceived Organizational Support. International Journal of Environmental Research and Public Health. 2022; 19(1):549. https://doi.org/10.3390/ijerph19010549
Chicago/Turabian StyleKim, Mi-Na, Yang-Sook Yoo, Ok-Hee Cho, and Kyung-Hye Hwang. 2022. "Emotional Labor and Burnout of Public Health Nurses during the COVID-19 Pandemic: Mediating Effects of Perceived Health Status and Perceived Organizational Support" International Journal of Environmental Research and Public Health 19, no. 1: 549. https://doi.org/10.3390/ijerph19010549