
Comparison between Cervical Ureaplasma spp. Colonization and the Intensity of Inflammatory Mediators in the Amniotic Fluid Retrieved during Cesarean Delivery in Preterm Birth


Abstract
:1. Introduction
2. Materials and Methods
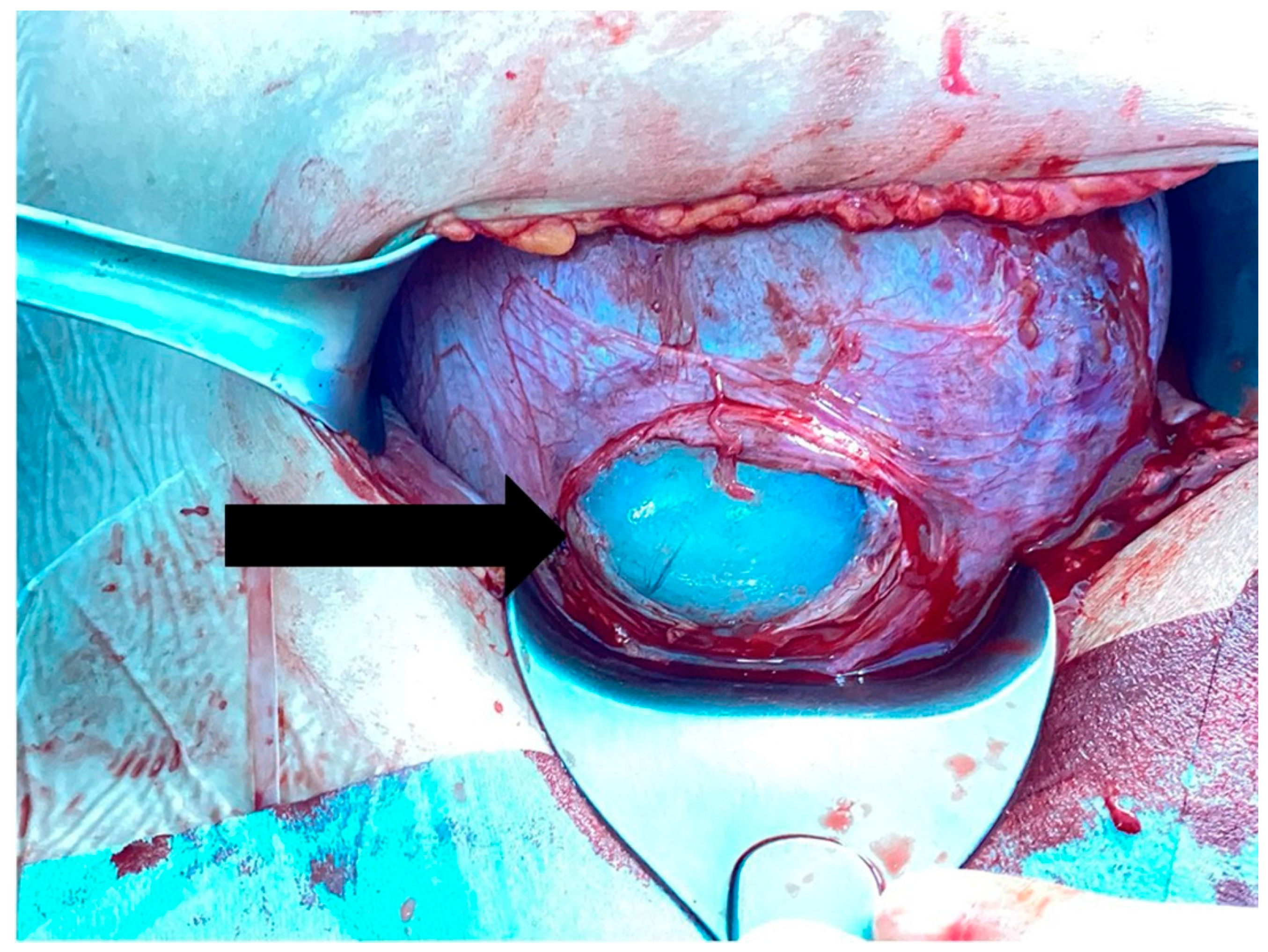
2.1. Collection of the Amniotic Fluids
2.2. Inclusion and Exclusion Criteria
2.3. Amniotic Fluid Analysis
2.4. Pathological Investigation of Placenta
2.5. Detection of Cervical Ureaplasma spp. Colonization
2.6. Statistical Analysis
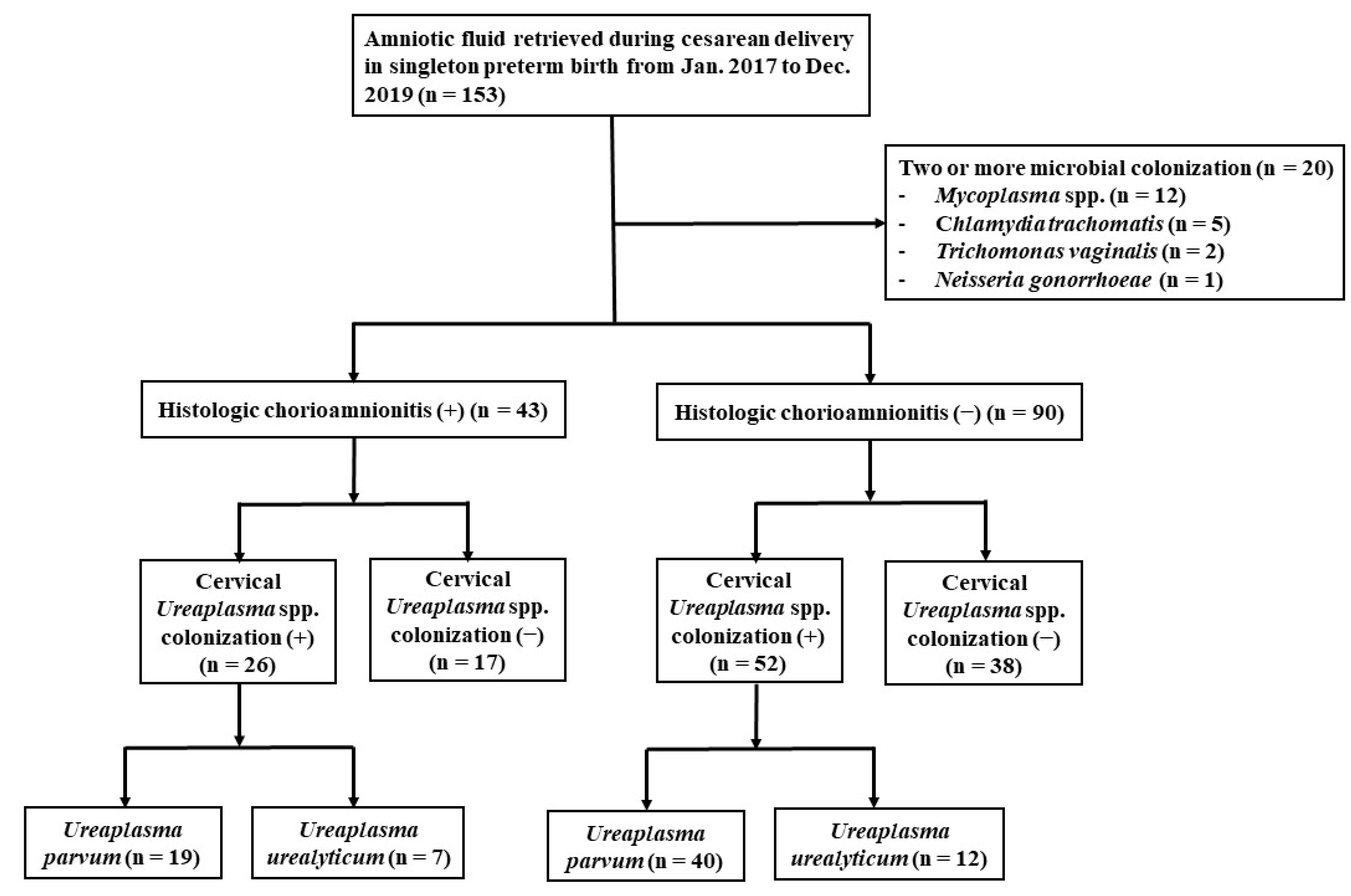
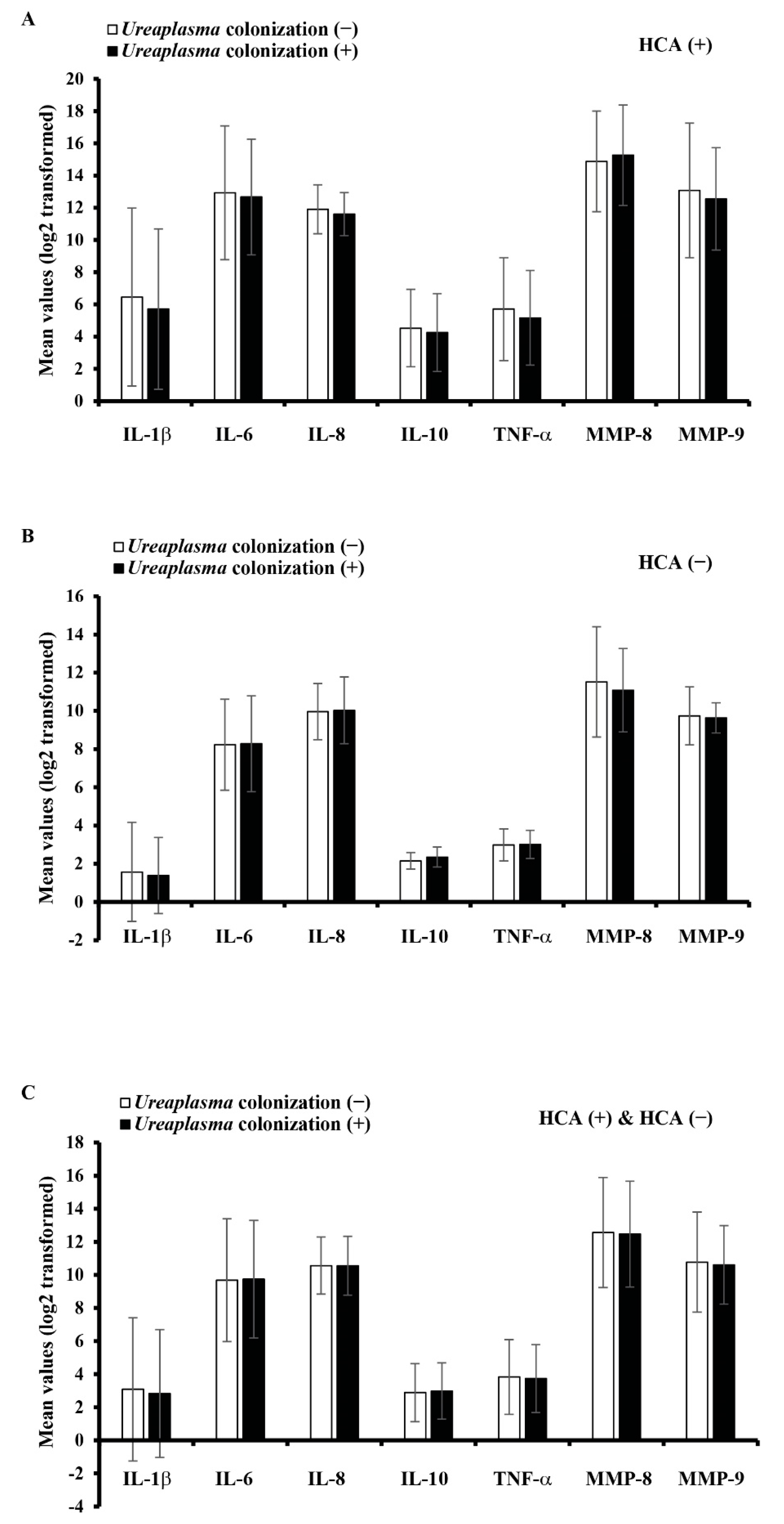
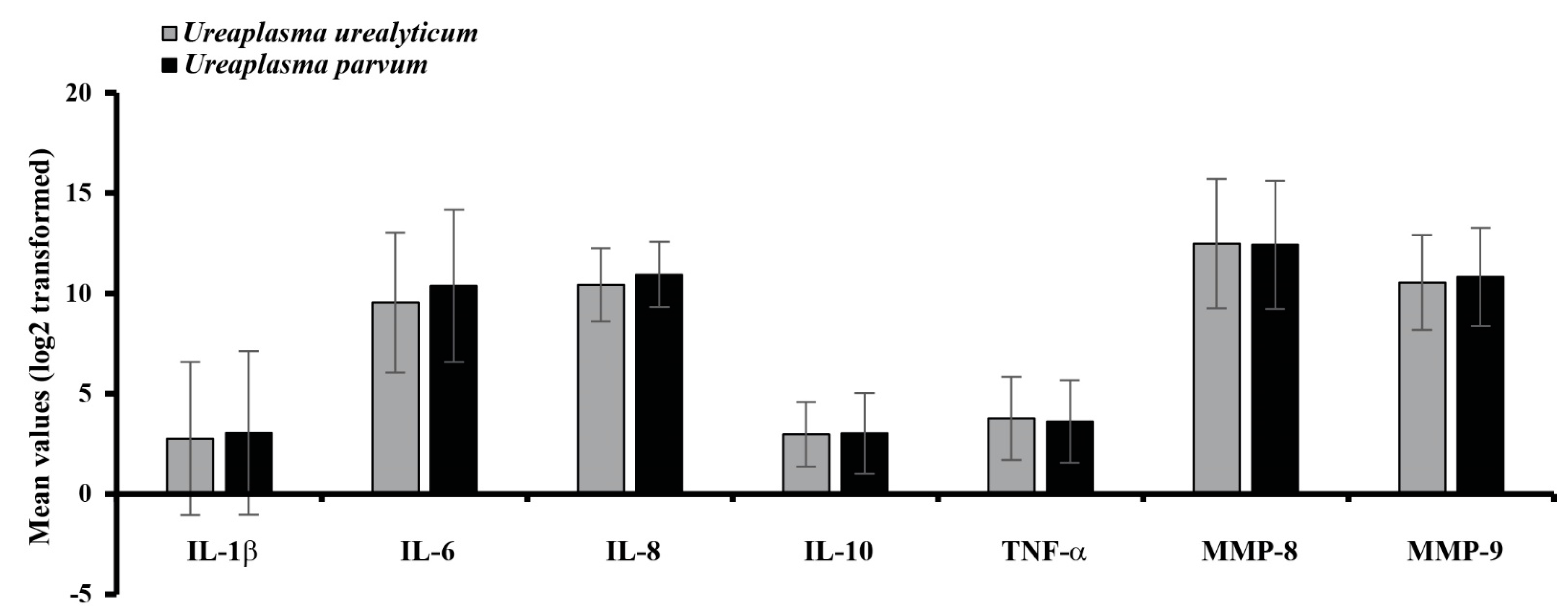
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chawanpaiboon, S.; Vogel, J.P.; Moller, A.-B.; Lumbiganon, P.; Petzold, M.; Hogan, D.; Landoulsi, S.; Jampathong, N.; Kongwattanakul, K.; Laopaiboon, M.; et al. Global, regional, and national estimates of levels of preterm birth in 2014: A systematic review and modelling analysis. Lancet Glob. Health 2019, 7, e37–e46. [Google Scholar] [CrossRef] [Green Version]
- Goldenberg, R.L.; Culhane, J.F.; Iams, J.D.; Romero, R. Epidemiology and causes of preterm birth. Lancet 2008, 371, 75–84. [Google Scholar] [CrossRef]
- Goldenberg, R.L.; Hauth, J.C.; Andrews, W.W. Intrauterine Infection and Preterm Delivery. N. Engl. J. Med. 2000, 342, 1500–1507. [Google Scholar] [CrossRef]
- Gotsch, F.; Romero, R.; Kusanovic, J.P.; Mazaki-Tovi, S.; Pineles, B.L.; Erez, O.; Espinoza, J.; Hassan, S.S. The Fetal Inflammatory Response Syndrome. Clin. Obstet. Gynecol. 2007, 50, 652–683. [Google Scholar] [CrossRef]
- Heine, R.P.; Puopolo, M.P.; Beigi, R.; Silverman, N.S.; El-sayed, Y.Y. Committee opinion No. 712: Intrapartum management of intraamniotic infection. Obstet. Gynecol. 2017, 130, e95–e101. [Google Scholar]
- Tita, A.T.; Andrews, W.W. Diagnosis and Management of Clinical Chorioamnionitis. Clin. Perinatol. 2010, 37, 339–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shim, S.S.; Romero, R.; Hong, J.S.; Park, C.W.; Jun, J.K.; Kim, B.I.; Yoon, B.H. Clinical significance of intra-amniotic inflammation in patients with preterm premature rupture of membranes. Am. J. Obstet. Gynecol. 2004, 191, 1339–1345. [Google Scholar] [CrossRef]
- Yoon, B.H.; Romero, R.; Bin Moon, J.; Shim, S.-S.; Kim, M.; Kim, G.; Jun, J.K. Clinical significance of intra-amniotic inflammation in patients with preterm labor and intact membranes. Am. J. Obstet. Gynecol. 2001, 185, 1130–1136. [Google Scholar] [CrossRef]
- Figueroa, R.; Garry, D.; Elimian, A.; Patel, K.; Sehgal, P.B.; Tejani, N. Evaluation of amniotic fluid cytokines in preterm labor and intact membranes. J. Matern. Fetal Neonatal Med. 2005, 18, 241–247. [Google Scholar] [CrossRef]
- Hagberg, H.; Wennerholm, U.-B.; Sävman, K. Sequelae of chorioamnionitis. Curr. Opin. Infect. Dis. 2002, 15, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Hillier, S.L.; Witkin, S.S.; Krohn, M.A.; Watts, D.H.; Kiviat, N.B.; Eschenbach, D.A. The relationship of amniotic fluid cytokines and preterm delivery, amniotic fluid infection, histologic chorioamnionitis, and chorioamnion infection. Obstet. Gynecol. 1993, 81, 941–948. [Google Scholar] [PubMed]
- Gotsch, F.; Romero, R.; Kusanovic, J.P.; Erez, O.; Espinoza, J.; Kim, C.J.; Vaisbuch, E.; Than, N.G.; Mazaki-Tovi, S.; Chaiworapongsa, T.; et al. The anti-inflammatory limb of the immune response in preterm labor, intra-amniotic infection/inflammation, and spontaneous parturition at term: A role for interleukin-10. J. Matern. Fetal Neonatal Med. 2008, 21, 529–547. [Google Scholar] [CrossRef] [Green Version]
- Maymon, E.; Romero, R.; Pacora, P.; Gomez, R.; Athayde, N.; Edwin, S.; Yoon, B.H. Human neutrophil collagenase (matrix metal-loproteinase 8) in parturition, premature rupture of the membranes, and intrauterine infection. Am. J. Obstet. Gynecol. 2000, 183, 94–99. [Google Scholar] [CrossRef]
- Locksmith, G.J.; Clark, P.; Duff, P.; Schultz, G.S. Amniotic Fluid Matrix Metalloproteinase-9 Levels in Women with Preterm Labor and Suspected Intra-amniotic Infection. Obstet. Gynecol. 1999, 94, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Gomez, R.; Ghezzi, F.; Romero, R.; Muñoz, H.; Tolosa, J.E.; Rojas, I. Premature Labor and Intra-Amniotic Infection: Clinical Aspects and Role of the Cytokines in Diagnosis and Pathophysiology. Clin. Perinatol. 1995, 22, 281–342. [Google Scholar] [CrossRef]
- Yoon, B.H.; Chang, J.W.; Romero, R. Isolation of Ureaplasma urealyticum from the amniotic cavity and adverse outcome in pre-term labor. Obstet. Gynecol. 1998, 92, 77–82. [Google Scholar] [CrossRef]
- Romero, R.; Yoon, B.H.; Mazor, M.; Gomez, R.; Gonzalez, R.; Diamond, M.P.; Baumann, P.; Araneda, H.; Kenney, J.S.; Cotton, D.B.; et al. A comparative study of the diagnostic performance of amniotic fluid glucose, white blood cell count, interleukin-6, and Gram stain in the detection of microbial invasion in patients with preterm premature rupture of membranes. Am. J. Obstet. Gynecol. 1993, 169, 839–851. [Google Scholar] [CrossRef]
- Kirchner, L.; Helmer, H.; Heinze, G.; Wald, M.; Brunbauer, M.; Weninger, M.; Zaknun, D. Amnionitis with Ureaplasma urealyticum or other microbes leads to increased morbidity and prolonged hospitalization in very low birth weight infants. Eur. J. Obstet. Gynecol. Reprod. Biol. 2007, 134, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Sweeney, E.L.; Kallapur, S.G.; Gisslen, T.; Lambers, D.S.; Chougnet, C.A.; Stephenson, S.-A.; Jobe, A.H.; Knox, C.L. Placental infection with Ureaplasma species is associated with histologic chorioamnionitis and adverse outcomes in moderately preterm and late-preterm infants. J. Infect. Dis. 2015, 213, 1340–1347. [Google Scholar] [CrossRef] [Green Version]
- Marovt, M.; Keše, D.; Kotar, T.; Kmet, N.; Miljković, J.; Šoba, B.; Matičič, M. Ureaplasma parvum and Ureaplasma urealyticum de-tected with the same frequency among women with and without symptoms of urogenital tract infection. Eur. J. Clin. Microbiol. Infect. Dis. 2015, 34, 1237–1245. [Google Scholar] [CrossRef]
- Hunjak, B.; Sabol, I.; Vojnović, G.; Fistonić, I.; Erceg, A.B.; Peršić, Z.; Grce, M. Ureaplasma urealyticum and Ureaplasma parvum in women of reproductive age. Arch. Gynecol. Obstet. 2014, 289, 407–412. [Google Scholar] [CrossRef] [Green Version]
- Sweeney, E.L.; Dando, S.J.; Kallapur, S.G.; Knox, C.L. The Human Ureaplasma Species as Causative Agents of Chorioamnionitis. Clin. Microbiol. Rev. 2017, 30, 349–379. [Google Scholar] [CrossRef] [Green Version]
- Lee, W.B. Biobank Regulation in South Korea. J. Law Med. Ethic 2016, 44, 342–351. [Google Scholar] [CrossRef]
- Lee, J.-E.; Kim, J.-H.; Hong, E.-J.; Yoo, H.S.; Nam, H.-Y.; Park, O. National Biobank of Korea: Quality control Programs of Collected-human Biospecimens. Osong Public Health Res. Perspect. 2012, 3, 185–189. [Google Scholar] [CrossRef] [Green Version]
- Kacerovsky, M.; Musilova, I.; Khatibi, A.; Skogstrand, K.; Hougaard, D.M.; Tambor, V.; Tosner, J.; Jacobsson, B. Intraamniotic in-flammatory response to bacteria: Analysis of multiple amniotic fluid proteins in women with preterm prelabor rupture of membranes. J. Matern. Fetal Neonatal Med. 2012, 25, 2014–2019. [Google Scholar] [CrossRef]
- Romero, R.; Miranda, J.; Chaemsaithong, P.; Chaiworapongsa, T.; Kusanovic, J.P.; Dong, Z.; Ahmed, A.I.; Shaman, M.; Lannaman, K.; Yoon, B.H.; et al. Sterile and microbial-associated intra-amniotic inflammation in preterm prelabor rupture of membranes. J. Matern. Fetal Neonatal Med. 2015, 28, 1394–1409. [Google Scholar] [CrossRef]
- Prince, A.L.; Ma, J.; Kannan, P.S.; Alvarez, M.; Gisslen, T.; Harris, R.A.; Sweeney, E.L.; Knox, C.L.; Lambers, D.S.; Jobe, A.H.; et al. The placental membrane microbiome is altered among subjects with spontaneous preterm birth with and without chorioamnionitis. Am. J. Obstet. Gynecol. 2016, 214, 627.e1–627.e16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldenberg, R.L.; Andrews, W.W.; Goepfert, A.R.; Faye-Petersen, O.; Cliver, S.P.; Carlo, W.A.; Hauth, J.C. The Alabama Preterm Birth Study: Umbilical cord blood Ureaplasma urealyticum and Mycoplasma hominis cultures in very preterm newborn infants. Am. J. Obstet. Gynecol. 2008, 198, 43.e1–43.e5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romero, R.; Espinoza, J.; Gonçalves, L.F.; Kusanovic, J.P.; Friel, L.A.; Nien, J.K. Inflammation in preterm and term labour and delivery. Semin. Fetal Neonatal Med. 2006, 11, 317–326. [Google Scholar] [CrossRef]
- Sprong, K.E.; Mabenge, M.; Wright, C.A.; Govender, S. Ureaplasma species and preterm birth: Current perspectives. Crit. Rev. Microbiol. 2020, 46, 169–181. [Google Scholar] [CrossRef] [PubMed]
- Kacerovsky, M.; Celec, P.; Vlkova, B.; Skogstrand, K.; Hougaard, D.M.; Cobo, T.; Jacobsson, B. Amniotic Fluid Protein Profiles of Intraamniotic Inflammatory Response to Ureaplasma spp. and Other Bacteria. PLoS ONE 2013, 8, e60399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- González Bosquet, E.; Gené, A.; Ferrer, I.; Borrás, M.; Lailla, J.M. Value of endocervical Ureaplasma species colonization as a mark-er of preterm delivery. Gynecol. Obstet. Invest. 2006, 61, 119–123. [Google Scholar] [CrossRef]
- Abele-Horn, M.; Scholz, M.; Wolff, C.; Kolben, M. High-density vaginal Ureaplasma urealyticum colonization as a risk factor for chorioamnionitis and preterm delivery. Acta Obstet. Gynecol. Scand. 2000, 79, 973–978. [Google Scholar]
- Choi, S.J.; Park, S.D.; Jang, I.H.; Uh, Y.; Lee, A. The Prevalence of Vaginal Microorganisms in Pregnant Women with Preterm Labor and Preterm Birth. Ann. Lab. Med. 2012, 32, 194–200. [Google Scholar] [CrossRef] [Green Version]
- Kwak, D.-W.; Cho, H.Y.; Kwon, J.-Y.; Park, Y.-W.; Kim, Y.-H. Usefulness of maternal serum C-reactive protein with vaginal Ureaplasma urealyticum as a marker for prediction of imminent preterm delivery and chorioamnionitis in patients with preterm labor or preterm premature rupture of membranes. J. Périnat. Med. 2015, 43, 409–415. [Google Scholar] [CrossRef] [PubMed]
- Vogel, I.; Thorsen, P.; Hogan, V.K.; Schieve, L.A.; Jacobsson, B.; Ferre, C.D. The joint effect of vaginal Ureaplasma urealyticum and bacterial vaginosis on adverse pregnancy outcomes. Acta Obstet. Gynecol. Scand. 2006, 85, 778–785. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, F.; Senat, M.-V. Multiple gestations and preterm birth. Semin. Fetal Neonatal Med. 2016, 21, 113–120. [Google Scholar] [CrossRef]
- Stock, S.; Norman, J. Preterm and term labour in multiple pregnancies. Semin. Fetal Neonatal Med. 2010, 15, 336–341. [Google Scholar] [CrossRef]
- Harmon, A.C.; Cornelius, D.C.; Amaral, L.M.; Faulkner, J.L.; Cunningham, M.W., Jr.; Wallace, K.; LaMarca, B. The role of inflammation in the pathology of preeclampsia. Clin. Sci. 2016, 130, 409–419. [Google Scholar] [CrossRef] [Green Version]
- Socha, M.; Malinowski, B.; Puk, O.; Dubiel, M.; Wiciński, M. The NLRP3 Inflammasome Role in the Pathogenesis of Pregnancy Induced Hypertension and Preeclampsia. Cells 2020, 9, 1642. [Google Scholar] [CrossRef]
- Reyes-Lagos, J.J.; Echeverría-Arjonilla, J.C.; Peña-Castillo, M.; Montiel-Castro, A.J.; Pacheco-López, G. Physiological, Immunological and Evolutionary Perspectives of Labor as an Inflammatory Process. Adv. Neuroimmune Biol. 2014, 5, 75–89. [Google Scholar] [CrossRef] [Green Version]
- Dubicke, A.; Fransson, E.; Centini, G.; Andersson, E.; Byström, B.; Malmström, A.; Petraglia, F.; Sverremark-Ekström, E.; Ekman-Ordeberg, G. Pro-inflammatory and anti-inflammatory cytokines in human preterm and term cervical ripening. J. Reprod. Immunol. 2010, 84, 176–185. [Google Scholar] [CrossRef] [Green Version]
- Reyes-Lagos, J.J.; Peña-Castillo, M.; Echeverría, J.C.; Pérez-Sánchez, G.; Álvarez-Herrera, S.; Becerril-Villanueva, E.; Pavón, L.; Ayala-Yáñez, R.; González-Camarena, R.; Pacheco-López, G. Women Serum Concentrations of the IL-10 Family of Cytokines and IFN-γ Decrease from the Third Trimester of Pregnancy to Active Labor. Neuroimmunomodulation 2017, 24, 162–170. [Google Scholar] [CrossRef]
- Seong, H.S.; Lee, S.E.; Kang, J.H.; Romero, R.; Yoon, B.H. The frequency of microbial invasion of the amniotic cavity and histologic chorioamnionitis in women at term with intact membranes in the presence or absence of labor. Am. J. Obstet. Gynecol. 2008, 199, 375.e1–375.e5. [Google Scholar] [CrossRef] [Green Version]
- Romero, R.; Nores, J.; Mazor, M.; Sepulveda, W.; Oyarzun, E.; Parra, M.; Insunza, A.; Montiel, F.; Behnke, E.; Cassell, G.H. Microbial invasion of the amniotic cavity during term labor. Prevalence and clinical significance. J. Reprod. Med. 1993, 38, 543–548. [Google Scholar]
- Locksmith, G.J.; Clark, P.; Duff, P.; Saade, G.R.; Schultz, G.S. Amniotic fluid concentrations of matrix metalloproteinase 9 and tissue inhibitor of metalloproteinase 1 during pregnancy and labor. Am. J. Obstet. Gynecol. 2001, 184, 159–164. [Google Scholar] [CrossRef]
- Zalud, I.; Janas, S. Risks of third-trimester amniocentesis. J. Reprod. Med. 2008, 53, 45–48. [Google Scholar] [PubMed]
- Stark, C.M.; Smith, R.S.; LaGrandeur, R.M.; Batton, D.G.; Lorenz, R.P. Need for Urgent Delivery After Third-Trimester Amniocentesis. Obstet. Gynecol. 2000, 95, 48–50. [Google Scholar] [CrossRef] [PubMed]
- Gordon, M.C.; Narula, K.; O’Shaughnessy, R.; Barth, W.H., Jr. Complications of third-trimester amniocentesis using continuous ultrasound guidance. Obstet. Gynecol 2002, 99, 255–259. [Google Scholar] [PubMed]
- Dudley, D.J.; Hunter, C.; Mitchell, M.D.; Varner, M.W. Amniotic fluid interleukin-10 (IL-10) concentrations during pregnancy and with labor. J. Reprod. Immunol. 1997, 33, 147–156. [Google Scholar] [CrossRef]
- Yoon, B.H.; Romero, R.; Kim, M.; Kim, E.-C.; Kim, T.; Park, J.S.; Jun, J.K. Clinical implications of detection of Ureaplasma urealyticum in the amniotic cavity with the polymerase chain reaction. Am. J. Obstet. Gynecol. 2000, 183, 1130–1137. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Histologic Chorioamnionitis (+) (n = 43) | Histologic Chorioamnionitis (−) (n = 90) | p-Value |
|---|---|---|---|
| Maternal age, years | 32.9 ± 4.1 | 33.4 ± 4.2 | 0.536 |
| Parity, times | 0.6 ± 0.7 | 0.6 ± 0.7 | 0.967 |
| Cerclage intervention, n (%) | 5 (11.6) | 9 (10.0) | 0.775 |
| Pregnancy-induced hypertension, n (%) | 11 (25.6) | 45 (50.0) | 0.008 |
| Gestational diabetes, n (%) | 4 (9.3) | 11 (12.2) | 0.619 |
| Cervical dilatation at admission, cm | 1.5 ± 1.8 | 0.8 ± 1.3 | 0.018 |
| Oligohydramnios, n (%) | 4 (9.3) | 10 (11.1) | 0.751 |
| Preterm labor with intact membrane, n (%) | 22 (51.2) | 24 (26.7) | 0.005 |
| Premature rupture of membrane, n (%) | 16 (37.2) | 15 (16.7) | 0.009 |
| Placenta previa, n (%) | 3 (7.0) | 7 (7.8) | 0.870 |
| Placenta abruptio, n (%) | 2 (4.7) | 6 (6.7) | 0.647 |
| Cervical Ureaplasma spp. colonization, n (%) | 26 (60.5) | 52 (57.8) | 0.768 |
| Gestational age at delivery, weeks | 30.1 ± 2.5 | 31.4 ± 2.2 | 0.008 |
| Birth weight, g | 1480 ± 472 | 1616 ± 562 | 0.170 |
| Apgar score, 1 min | 6.1 ± 1.5 | 6.1 ± 1.6 | 0.914 |
| Apgar score, 5 min | 8.0 ± 0.9 | 8.0 ± 0.8 | 0.781 |
| Inflammatory mediators (Logarithmically) | |||
| IL-1 ß | 6.0 ± 5.1 | 1.5 ± 2.3 | <0.001 |
| IL-6 | 12.8 ± 3.8 | 8.3 ± 2.4 | <0.001 |
| IL-8 | 11.7 ± 1.3 | 10.0 ± 1.6 | <0.001 |
| IL-10 | 4.4 ± 2.4 | 2.3 ± 0.5 | <0.001 |
| TNF-α | 5.4 ± 3.0 | 3.0 ± 0.8 | <0.001 |
| MMP-8 | 15.1 ± 3.1 | 10.0 ± 1.6 | <0.001 |
| MMP-9 | 12.8 ± 3.6 | 9.7 ± 1.1 | <0.001 |
| Variables | Gestational Age at Delivery (n = 133) | |
|---|---|---|
| Pearson’s Coefficient | p-Value | |
| IL-1β | −0.260 | 0.003 |
| IL-6 | −0.176 | 0.043 |
| IL-8 | −0.037 | 0.672 |
| IL-10 | −0.275 | 0.001 |
| TNF-α | −0.279 | 0.001 |
| MMP-8 | −0.268 | 0.002 |
| MMP-9 | −0.230 | 0.008 |
| Variables | Odds Ratios | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Cervical Ureaplasma spp. colonization | 1.110 | 0.483–2.550 | 0.806 |
| Preterm labor with intact membrane | 5.041 | 1.985–12.800 | 0.001 |
| Premature rupture of membrane | 7.217 | 2.559–20.357 | <0.001 |
| Pregnancy-induced hypertension | 1.002 | 0.312–3.217 | 0.998 |
| Cervical dilatation at admission | 1.126 | 0.854–1.484 | 0.400 |
| Gestational age at delivery | 0.776 | 0.651–0.926 | 0.005 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bae, J.; Kim, S.; Hwang, I.; Park, J. Comparison between Cervical Ureaplasma spp. Colonization and the Intensity of Inflammatory Mediators in the Amniotic Fluid Retrieved during Cesarean Delivery in Preterm Birth. Int. J. Environ. Res. Public Health 2022, 19, 107. https://doi.org/10.3390/ijerph19010107
Bae J, Kim S, Hwang I, Park J. Comparison between Cervical Ureaplasma spp. Colonization and the Intensity of Inflammatory Mediators in the Amniotic Fluid Retrieved during Cesarean Delivery in Preterm Birth. International Journal of Environmental Research and Public Health. 2022; 19(1):107. https://doi.org/10.3390/ijerph19010107
Chicago/Turabian StyleBae, Jingon, Shin Kim, Ilseon Hwang, and Jaehyun Park. 2022. "Comparison between Cervical Ureaplasma spp. Colonization and the Intensity of Inflammatory Mediators in the Amniotic Fluid Retrieved during Cesarean Delivery in Preterm Birth" International Journal of Environmental Research and Public Health 19, no. 1: 107. https://doi.org/10.3390/ijerph19010107