
The Cycle to Respectful Care: A Qualitative Approach to the Creation of an Actionable Framework to Address Maternal Outcome Disparities

 ,
,
Abstract
:1. Introduction
2. Shifts in Policy and Practice
3. Taking Action to Address Maternal Outcome Disparities
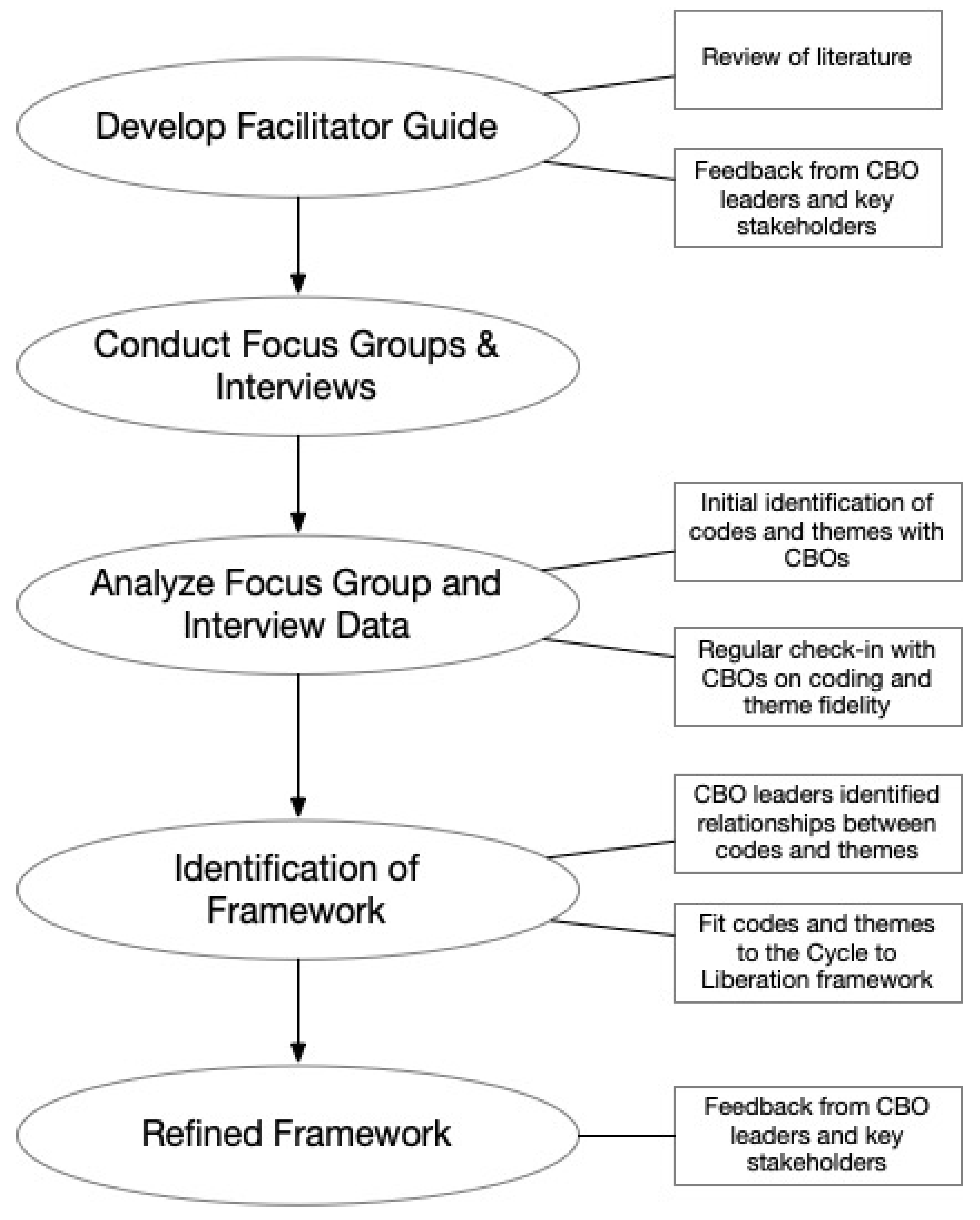
4. Methods
5. Data Collection
6. Data Analysis
7. Creating the Framework
8. Participant Recruitment
9. Framework Development
10. Results
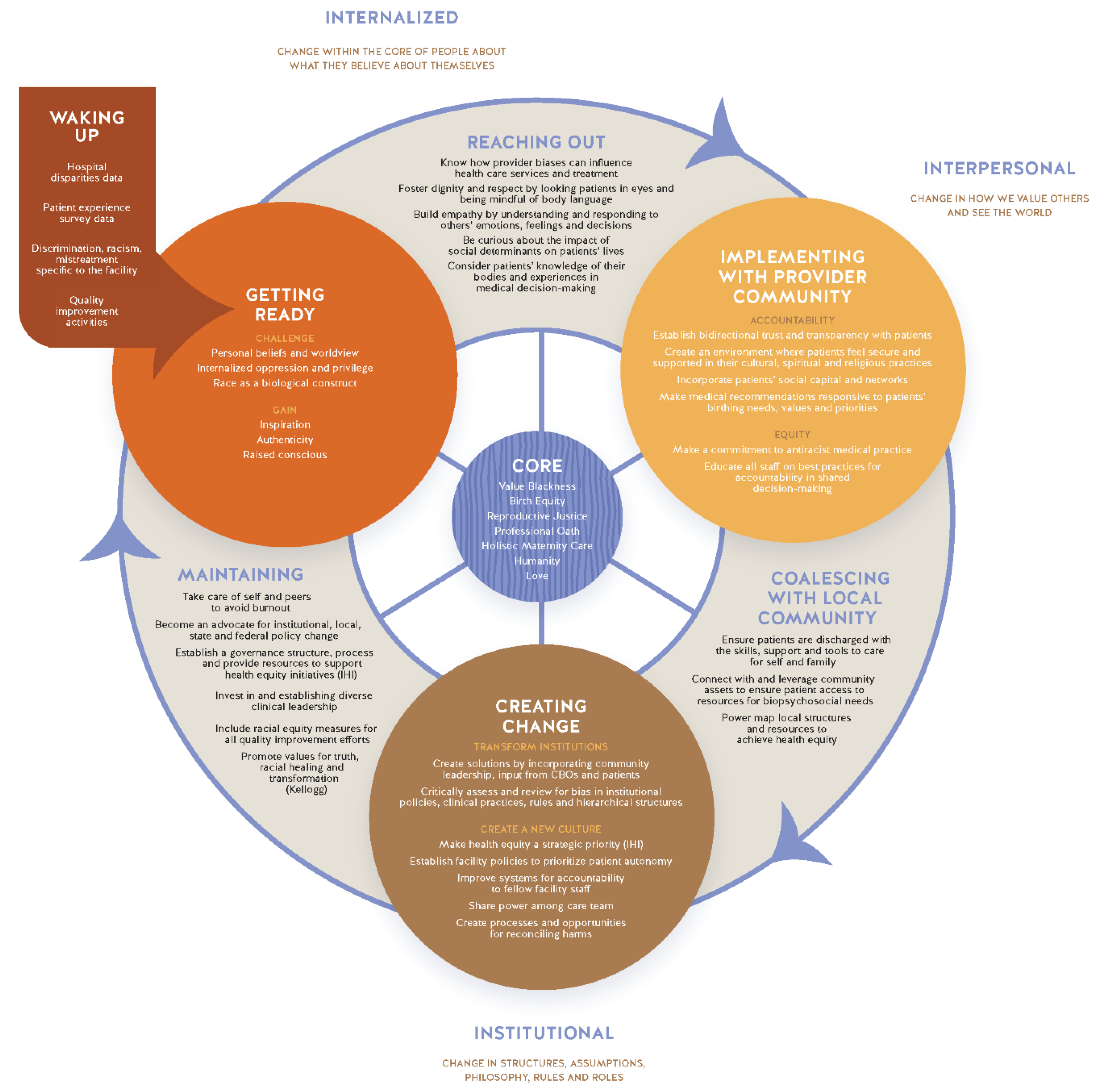
11. The Core of the Cycle to Respectful Care
12. Discussion
13. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McLemore, M.R.; Altman, M.R.; Cooper, N.; Williams, S.; Rand, L.; Franck, L. Health care experiences of pregnant, birthing and postnatal women of color at risk for preterm birth. Soc. Sci. Med. 2018, 201, 127–135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fridman, M.; Korst, L.M.; Chow, J.; Lawton, E.; Mitchell, C.; Gregory, K.D. Trends in maternal morbidity before and during pregnancy in California. Am. J. Public Health 2014, 104, S49–S57. [Google Scholar] [CrossRef] [PubMed]
- Petersen, E.E.; Davis, N.L.; Goodman, D.; Cox, S.; Syverson, C.; Seed, K.; Shapiro-Mendoza, C.; Callaghan, W.M.; Barfield, W. Racial/ethnic disparities in pregnancy-related deaths—United States, 2007–2016. Morb. Mortal. Wkly. Rep. 2019, 68, 762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakala, C.; Declercq, E.; Turon, J.; Corry, M. Listening to Mothers in California: A Population-Based Survey of Women’s Childbearing Experiences; National Partnership for Women & Families: Washington, DC, USA, 2018. [Google Scholar]
- Vedam, S.; Stoll, K.; Taiwo, T.K.; Rubashkin, N.; Cheyney, M.; Strauss, N.; McLemore, M.; Cadena, M.; Nethery, E.; Rushton, E. The Giving Voice to Mothers study: Inequity and mistreatment during pregnancy and childbirth in the United States. Reprod. Health 2019, 16, 77. [Google Scholar] [CrossRef] [Green Version]
- Petersen, E.E.; Davis, N.L.; Goodman, D.; Cox, S.; Mayes, N.; Johnston, E.; Syverson, C.; Seed, K.; Shapiro-Mendoza, C.K.; Callaghan, W.M. Vital signs: Pregnancy-related deaths, United States, 2011–2015, and strategies for prevention, 13 states, 2013–2017. Morb. Mortal. Wkly. Rep. 2019, 68, 423. [Google Scholar] [CrossRef] [Green Version]
- Amutah-Onukagha, N.; Howell, E.; Crear-Perry, J.A.; Underwood, L. A Path to Reproductive Justice: Research, Practice and Policies. In Advancing Racial Equity; American Public Health Association: Washington, DC, USA, 2020. [Google Scholar]
- World Health Organization. WHO Recommendations on Intrapartum Care for a Positive Childbirth Experience; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- McWilliams, J.M. Professionalism Revealed: Rethinking Quality Improvement in the Wake of a Pandemic. NEJM Catal. Innov. Care Deliv. 2020, 1. [Google Scholar] [CrossRef]
- Crear-Perry, J.; Maybank, A.; Keeys, M.; Mitchell, N.; Godbolt, D. Moving towards anti-racist praxis in medicine. Lancet 2020, 396, 451–453. [Google Scholar] [CrossRef]
- Tervalon, M.; Murray-Garcia, J. Cultural humility versus cultural competence: A critical distinction in defining physician training outcomes in multicultural education. J. Health Care Poor Underserved 1998, 9, 117–125. [Google Scholar] [CrossRef]
- Reproductive Justice. Available online: https://www.sistersong.net/reproductive-justice/ (accessed on 10 September 2020).
- Jolivétte, A. Research Justice: Methodologies for Social Change; Policy Press: Bristol, UK, 2015. [Google Scholar]
- Scott, K.A.; Britton, L.; McLemore, M.R. The ethics of perinatal care for black women: Dismantling the structural racism in “mother blame” narratives. J. Perinat. Neonatal Nurs. 2019, 33, 108–115. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. Ecological Systems Theory; Jessica Kingsley Publishers: London, UK, 1992. [Google Scholar]
- Balogun-Mwangi, O.; Matsumoto, A.; Ballou, M.; Faver, L.; Todorova, I. Women’s Pain, Women’s Voices: Using the Feminist Ecological Model and a Participatory Action Research Approach in Developing a Group Curriculum for Chronic Pain. J. Ethnogr. Qual. Res. 2016, 11, 1–16. [Google Scholar]
- Maslow, A.; Lewis, K. Maslow’s Hierarchy of Needs; Salenger Incorporated: Glenarm, IL, USA, 1987; Volume 14, p. 987. [Google Scholar]
- Harro, B. The cycle of liberation. Read. Divers. Soc. Justice 2000, 2, 52–58. [Google Scholar]
- Bobbie, H.; Maurianne, A. The cycle of socialization. In Reading for Diversity and Social Justice; Adams, M., Blumenfeld, W.J., Castaneda, R., Hackman, H.W., Peters, M.L., Zuniga, X., Eds.; Routledge: New York, NY, USA, 2000. [Google Scholar]
- Ross, L.; Solinger, R. Reproductive Justice: An Introduction; University of California Press: Berkeley, CA, USA, 2017; Volume 1. [Google Scholar]
- Muse, S.; Gay, E.D.; Aina, A.D.; Green, C.; Crear-Perry, J.; Roach, J.; Tesfa, H.; Matthews, K.; Harris, T.L. Black Paper: Setting the Standard for Holistic Care of and for Black Women; Black Mamas Matter Alliance: Atlanta, GA, USA, 2018. [Google Scholar]
- Lipscomb, B.N.; Taylor, J.K.; Gay, E.D.; Aina, A.D.; Crear-Perry, J.; Roach, J.; Porcchia-Albert, C.; Nedhari, A.; Scott, C.; Williams, A.N.; et al. Advancing Holistic Maternal Care for Black Women through Policy; Black Mamas Matter Alliance: Atlanta, GA, USA, 2018. [Google Scholar]
- UN General Assembly. Universal Declaration of Human Rights; UN General Assembly: New York, NY, USA, 1948; Volume 302. [Google Scholar]
- Giordano, L.A.; Elliott, M.N.; Goldstein, E.; Lehrman, W.G.; Spencer, P.A. Development, implementation, and public reporting of the HCAHPS survey. Med. Care Res. Rev. 2010, 67, 27–37. [Google Scholar] [CrossRef]
- Mahoney, J. The alliance for innovation in maternal health care: A way forward. Clin. Obstet. Gynecol. 2018, 61, 400–410. [Google Scholar] [CrossRef] [PubMed]
- Kendi, I.X. How to Be an Antiracist; One world: London, UK, 2019. [Google Scholar]
- A Roadmap for Promoting Health Equity and Eliminating Disparities: The Four I’s for Health Equity; National Quality Forum: Washington, DC, USA, 2017; pp. 1–119.
- Wyatt, R.; Laderman, M.; Botwinick, L.; Mate, K.; Whittington, J. Achieving Health Equity: A Guide for Health Care Organizations; IHI White Paper; Institute for Healthcare Improvement: Cambridge, MA, USA, 2016. [Google Scholar]
- Reduction of Peripartum Racial/Ethnic Disparities (+AIM). Available online: https://safehealthcareforeverywoman.org/patient-safety-bundles/reduction-of-peripartum-racialethnic-disparities/#link_acc-1-5-d (accessed on 10 September 2020).
- Crear-Perry, J.; Correa-de-Araujo, R.; Lewis Johnson, T.; McLemore, M.R.; Neilson, E.; Wallace, M. Social and structural determinants of health inequities in maternal health. J. Women’s Health 2020, 30, 230–235. [Google Scholar] [CrossRef]
- Howell, E.A.; Brown, H.; Brumley, J.; Bryant, A.S.; Caughey, A.B.; Cornell, A.M.; Grant, J.H.; Gregory, K.D.; Gullo, S.M.; Kozhimannil, K.B. Reduction of peripartum racial and ethnic disparities: A conceptual framework and maternal safety consensus bundle. J. Obstet. Gynecol. Neonatal Nurs. 2018, 47, 275–289. [Google Scholar] [CrossRef]
- Aina, A.D.; Asiodu, I.V.; Castillo, P.; Denson, J.; Drayton, C.; Aka-James, R.; Mahdi, I.K.; Mitchell, N.; Morgan, I.; Robinson, A. Black Maternal Health Research Re-Envisioned: Best Practices for the Conduct of Research with, for, and by Black Mamas. Harv. Law Policy Rev. 2019, 14, 393. [Google Scholar]
- Griffith, D.; Jegede, B.; Weir, S.; Canady, R. Practices to Reduce Infant Mortality through Equity: Recommendations for State Public Health Departments; Michigan Department of Community Health: Lansing, MI, USA, 2015. [Google Scholar]
- Hogan, V.; Rowley, D.L.; White, S.B.; Faustin, Y. Dimensionality and R4P: A health equity framework for research planning and evaluation in African American populations. Matern. Child Health J. 2018, 22, 147–153. [Google Scholar] [CrossRef]
- Wallace, M.; Crear-Perry, J.; Richardson, L.; Tarver, M.; Theall, K. Separate and unequal: Structural racism and infant mortality in the US. Health Place 2017, 45, 140–144. [Google Scholar] [CrossRef]
- Chambers, B.D.; Arabia, S.E.; Arega, H.A.; Altman, M.R.; Berkowitz, R.; Feuer, S.K.; Franck, L.S.; Gomez, A.M.; Kober, K.; Pacheco-Werner, T. Exposures to structural racism and racial discrimination among pregnant and early post-partum Black women living in Oakland, California. Stress Health 2020, 36, 213–219. [Google Scholar] [CrossRef] [Green Version]
- Hacker, K. Community-Based Participatory Research; Sage Publications: Thousand Oaks, CA, USA, 2013. [Google Scholar]
- Hunt, P.; Backman, G. Health systems and the right to the highest attainable standard of health. Health Hum. Rights 2008, 10, 81–92. [Google Scholar] [CrossRef]
- Jones, C.P. Levels of racism: A theoretic framework and a gardener’s tale. Am. J. Public Health 2000, 90, 1212. [Google Scholar]
- Nuru-Jeter, A.; Dominguez, T.P.; Hammond, W.P.; Leu, J.; Skaff, M.; Egerter, S.; Jones, C.P.; Braveman, P. “It’s the skin you’re in”: African-American women talk about their experiences of racism. An exploratory study to develop measures of racism for birth outcome studies. Matern. Child Health J. 2009, 13, 29. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | n (%) |
|---|---|
| Location | |
| Atlanta | 11 (22%) |
| Baltimore | 7 (14%) |
| Chicago | 9 (18%) |
| Dallas | 6 (12%) |
| Houston | 9 (18%) |
| Tulsa | 8 (16%) |
| Insurance | |
| Public | 25 (50%) |
| Private | 16 (32%) |
| Both (Public and Private) | 7 (14%) |
| Decline to state/Unsure | 2 (4%) |
| Annual Household Income | |
| <$25,000 | 16 (32%) |
| $25,000–$49,999 | 18 (36%) |
| $50,000–$74,999 | 7 (14%) |
| $75,000–$99,999 | 4 (8%) |
| $100,000+ | 5 (10%) |
| Education | |
| Some High School | 3 (6%) |
| High School Graduate/GED | 6 (12%) |
| Trade School | 1 (2%) |
| Some College | 17 (34%) |
| Bachelor’s Degree or Higher | 23 (46%) |
| Core Value | Description |
|---|---|
| Black Intersectionality * | Valuing the Black experience rather than the physical dark skin. Maternal experiences from Black identifying mothers are rich with data about bias and racism negatively affecting their births. It is imperative that making strides in quality improvement efforts to value the culture and experiences of being Black. Any quality improvement in maternal experiences are hypothesized to impact Black women most directly; therefore, any solutions developed must explicitly center Black women [1]. |
| Birth Equity * | The assurance of the conditions of optimal births and wellbeing for all people with a willingness of systems to address racial and social inequities in a sustained effort. |
| Reproductive Justice | Capacious envisioning of reproductive possibilities that requires the use of intersectionality, the perspective that allows us to comprehend how race, class, ethnicity, and sexuality together construct gendered implications of motherhood and citizenship, sex and reproduction [12,20]. |
| Professional Pledge/Oath | The commitment and promise of each profession. This is included in the core to remind hospital staff of the reasons why they practice and the foundational values of their profession. This could include the Hippocratic Oath, Imhotep Oath, Nightingale Pledge, etc. [5]. |
| Holistic Maternity Care | Black Mamas Matter Alliance’s (BMMA’s) holistic maternity care concept is anchored in: addressing gaps in care and ensures continuity of care, is confidential, safe and trauma-informed, is culturally informed and includes traditional practices, respects spirituality and spiritual health, and lastly is provided by culturally competent and culturally congruent providers [21,22]. |
| Humanity | Characterized by the United Nations treaty for Human Rights. From the perspective of mothers, being treated with humanity is being seen and regarded equally on the same level as another person you are interacting with, kindness, courtesy and politeness [23]. |
| Love of self and others * | Respectful care is the practice of love. It is developing a sense of self as a care provider so that they can love others who are different than themself. |
| Cycle Stage | Physician | Nurse | Black Patient |
|---|---|---|---|
| Waking-Up | A physician does not believe themselves to be personally are racist, but the data from their medical director shows disparities in HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) [24] and C-section rates for Black patients. | A nurse views countless news stories on police brutality and the Black Lives Matter Movement, and thus, she begins to reflect upon her role in contributing to racism. | A patient realizes she gets different types of questions from her doctor than the White mothers in her mom group. Questions such as whether she plans to terminate or continue the pregnancy and questions about her relationship with the baby’s father. |
| Getting Ready | A physician is required to take implicit bias training but is uncertain on how the training will impact their medical practice. | A certified nurse midwife (CNM), continues to raise her consciousness and educate herself on privilege and the construction of racism in the U.S. | A patient begins to educate herself on her birthing options and the hospital policies. |
| Reaching Out | A physician recognizes the ways in which their biases influence patient care and seeks to identify ways in which their practice might be more holistic by asking patients about their experiences at home, at work, and with family. | A nurse midwife could start with practicing new approaches with her patient interactions, such as looking patients in the eyes when she’s speaking with them, showing patients they have her full attention with the positioning of her body, and making a conscious effort to listen to patients while checking her own biases. | A patient communicates her birthing needs and priorities with her care team. |
| Implementing with the Provider Community | A physician is, perhaps, now aware of the patient’s support system and considers the patient’s knowledge of their body in medical decision-making. | A nurse midwife becomes her department’s champion for educating the staff on best practices for accountability and decision-making. | A patient asserts her knowledge of her body and experiences to create a birthing plan where she would feel most safe and supported. |
| Coalescing with the Local Community | A physician ensures patients are discharged with all that they need to care for themselves and their family by connecting with and leveraging community assets. | A nurse midwife leads a power mapping exercise, starting with her network of local CMNs, to identify structure and processes for health equity. | When a patient shares her birth plan, the nurse provides resources to complement the birth plan and to meet the patient’s biopsychosocial needs. |
| Creating Change | A physician might suggest at quality improvement meetings with all hospital staff to create a system of accountability and leveled hierarchies among all hospital staff. | A nurse midwife builds relationships with local Women, Infants, and Children (WIC) offices and CBOs and creates a transparent process for patients to report harms, mistreatment or complaints. | A patient is educated on ways to report harms and complaints, and they are invited to participate in a department-wide maternal mortality review committee as a patient liaison. |
| Maintaining | A physician advocates for institutional policy and on-going workshops/medical education to minimize risk of burnout. | A nurse midwife engages with her statewide professional organization to establish policies for investment and promotion of diverse hiring practices. | A patient is introduced to services at health systems and hospitals that have shown a commitment to racial equity, made possible by the strength of community-hospital partnerships |
| Cycle Phase | Definition | Actions |
|---|---|---|
| Waking Up | In the Cycle to Respectful Care, this waking up might include a critical incident of racism, discrimination, or mistreatment in the healthcare facility. Providers are made aware of the incident through patient reports, disparities data, or mandates to address disparate outcomes through implicit bias training or a quality improvement initiative. The American College of Obstetrics and Gynecologists (ACOG) ACOG AIM Patient Safety Bundles [25] and quality improvement initiatives are resources for hospitals and health systems that may illuminate racist and discriminatory care in order to prompt this Waking-Up phase. | Due to the urgency of growing maternal inequities in the United States, hospitals, healthcare systems, and policy makers have taken action to mandate implicit bias training thereby initiating the Waking-Up process rather than waiting for maternal care staff to Wake-Up on their own. The Cycle to Respectful Care begins when an individual observes or experiences the world differently than s/he has in the past. |
| Getting Ready | Getting Ready is the point at which individuals move from exclusively internal work to application in how they interact with and speak to others. This can be achieved through reviewing evidence-based research, attending anti-racist workshops, training on various topics, and building connections with others. This phase can include challenging beliefs in our worldview, medical education, and consciousness raising. | In preparation of the practice of valuing Black mothers more intensely, healthcare providers become conscious and make note of thoughts, language, and actions to see if they are consistent with newly established beliefs or they can be dismantled [18]. This intrapersonal section requires us to develop a repertoire of skills and tools that will serve us throughout the rest of the Cycle. These skills are built with others in Reaching Out. |
| Reaching Out | Reaching Out describes the ways in which an individual solidifies a new understanding of Respectful Care. Providers, who are educated about their biases, can identify the behaviors they exhibit that influence care and treatment for patients they are biased towards. Communication and information sharing become more important to the provider, to show themselves more trustworthy [5]. Overall, curiosity about the impact of social determinants on patients’ lives can help providers build empathy and understand others. Small shifts in behavior communicate a level of respect to Black mothers, that impacts their experience. This Reaching Out phase moves us from the internal work to the truly interpersonal within the provider community. | In this phase, a person begins to incorporate their new ideals and knowledge into their everyday interactions, observing the response of others in their life to their new perspective. It is imperative to practice the new skills with others, test expressing new views, vocalize uncertainty instead of staying silent, and examine ideals through reflection and introspection, and seek out a greater range of differences than before. This Reaching Out phase provides strategies to practice the ways in which new worldviews will be met by patients. |
| Implementing with Provider Community | The Provider Community phase of the Cycle to Liberation contains two components: conversing with those who possess similar social identities and those who are different to build coalitions [18]. The interpersonal phase of the respectful care process is marked by a change in the value of others. This phase is characterized by the creation of an ongoing dialogue where views are exchanged, people are listened to and valued, and the process of seeing others’ points of view as making sense and having integrity, even if they are very different from our own, begins. An integral part of this dialogue is exploring differences, clarifying them, erasing assumptions, and replacing them with firsthand contact and good listening. Building a solid provider community for respectful care means that small groups within institutions come to a common understanding of respectful care for Black mothers. These individuals will begin to conduct themselves differently in ways that impact their colleagues. | Addressing the provider community consists of two steps: (1) dialoguing with people who are like us for support and (2) dialoguing with people who are different from us for gaining understanding about oppression. Patients’ culture, religion, fears, and hopes for their birth experience, must be discussed. It is useful to collectively create guidelines on normalizing best practices that are not standardized, like visitation policies or emerging anti-racism tools [26]. The Black mothers in the study suggested that provider accountability is shown either to the health system itself or to the patient. It is socialized in the provider community to build trust with the patient, such that the patient adheres to clinical guidance. It is not socialized in the provider community to be responsive to the knowledge, words, birthing needs, and priorities of the patient as an autonomous decisionmaker in the birthing experience [27]. The Institute for Healthcare Improvement (IHI) Framework [28] and AIM Patient Safety Bundle Reduction of Peripartum Racial/Ethnic Disparities are resources for organizational self-evaluation for accountability and equity of care to guide health systems and hospitals through this phase. |
| Coalescing with Local Community | The Coalescing phase is where the actions of the organized coalitions and groups begin to disrupt oppressive systems and create change [18]. It is vital during this phase to realize the collective work of the cohesive group is greater than individual actions. Once obstacles have been ameliorated, one can address factors that maintain racial inequities by joining forces with the broader community beyond that of the hospital facility or healthcare system [27]. | Working in a true collaborative manner means that providers are culpable in ensuring patients are well when they are outside of the direct care and oversight of the care facility. Providers, who have coalesced with their patients’ communities are able to ensure patients leave with access to resources to meet biopsychosocial needs. This may require large systems to power map structures and processes for health equity in their locations. This phase is intended to disrupt the status quo and for members of coalitions to take a stand with their beliefs. Consistent with existing quality improvement efforts, this phase also aligns with the IHI Framework sections four and five [28], National Quality Forum’s domains of health equity [27] and the ACOG AIM Patient AIM Patient Safety Bundle Reduction of Peripartum Racial/Ethnic Disparities [29]. The actions in this phase of the Cycle lead to collective work to create change in structures, assumptions, philosophy, rules, and roles |
| Creating Change | The Creating Change phase of the cycle includes redesigning health services to create new culture and norms that reflect the public’s collective identity [30], resulting in new assumptions, new structures, new roles, and new rules consistent with birth equity. Establishing health equity as a strategic priority and challenging structures, greatly enhances efforts to critically transform systems. Another way to create a culture of respectful care is to improve methods of accountability so that providers can have critical conversations amongst themselves, this involves taking leadership risks and becoming a beacon of change. Critical transformation takes place when organizations make conscious collective decisions for all policies for a collaborative structure rather than hierarchical. The new assumptions, rules, roles and structures must be cultivated. | Creating Change for respectful care means transforming institutions and creating a new culture [31]. Centering the voices and experiences of the group most impacted by the inequity is of greatest importance. Institutional change also depends on an assessment of institutional policies, clinical practices, and structures undergirding the system. Mentorship from identified birth equity champions within the facility or dismantling structures of power in and around quality improvement projects are legitimate activities to create change [5,32]. Tools for assessments include the Institute for Healthcare Improvement tools, National Quality Forum’s health equity domains [27], AIM tools and the strategy of applying the Brooks Equity Typology assessment [33] described in the R4P framework [34]. |
| Maintaining | Maintaining is a phase where all the previous changes become routines in the life of the person, and that people in this phase of the system support each other, to hold one another accountable for maintenance of the change [18]. Moving towards a respectful and anti-racist practice necessitates that institutions challenge structural racism and other intersecting oppressive systems (e.g., ableism, classism, ethnocentrism, homophobia, sexism, transphobia- and shift power in resources, leadership, and policies) [10]. In order to succeed, change needs to be strengthened, monitored, and integrated into the ritual of daily life. Just like anything new, it needs to be nurtured, learned again “debugged,” and modified as needed. Maintaining includes a paradigm shift in medical training and competencies for respectful and anti-racist care models [10]. There must be an ongoing commitment and investment of resources from leadership and systems to maintain Respectful Maternity Care initiatives. | Providers are under extreme pressure and responsibility. Taking care of themselves and others on the care team helps them to avoid burnout and desensitization from repeated issues. Individual providers can help maintain systems change by advocating for institutional, local, state, and federal policies that impact social determinants [30], structural racism [35,36] and healthcare overall. They may be trained to advocate or exercise their inherent knowledge of the administrative or legislative process. Advocacy within the healthcare facility would be helping establish a governance structure and process for health equity, including hiring a diverse staff. Quality improvement efforts of any kind must address racial equity and bias to impact care. The Institute for Healthcare Improvement Achieving Health Equity: A Guide for Health Care Organizations provides guidance on this process [28]. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Green, C.L.; Perez, S.L.; Walker, A.; Estriplet, T.; Ogunwole, S.M.; Auguste, T.C.; Crear-Perry, J.A. The Cycle to Respectful Care: A Qualitative Approach to the Creation of an Actionable Framework to Address Maternal Outcome Disparities. Int. J. Environ. Res. Public Health 2021, 18, 4933. https://doi.org/10.3390/ijerph18094933
Green CL, Perez SL, Walker A, Estriplet T, Ogunwole SM, Auguste TC, Crear-Perry JA. The Cycle to Respectful Care: A Qualitative Approach to the Creation of an Actionable Framework to Address Maternal Outcome Disparities. International Journal of Environmental Research and Public Health. 2021; 18(9):4933. https://doi.org/10.3390/ijerph18094933
Chicago/Turabian StyleGreen, Carmen L., Susan L. Perez, Ashlee Walker, Tracey Estriplet, S. Michelle Ogunwole, Tamika C. Auguste, and Joia A. Crear-Perry. 2021. "The Cycle to Respectful Care: A Qualitative Approach to the Creation of an Actionable Framework to Address Maternal Outcome Disparities" International Journal of Environmental Research and Public Health 18, no. 9: 4933. https://doi.org/10.3390/ijerph18094933