
Spatial and Temporal Characteristics of Hand-Foot-and-Mouth Disease and Their Influencing Factors in Urumqi, China


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Area
2.2. Data Acquisition
2.3. Statistical Methods
2.3.1. Center of Gravity
2.3.2. Geographical Detector
3. Results
3.1. Spatial and Temporal Distributions of HFMD
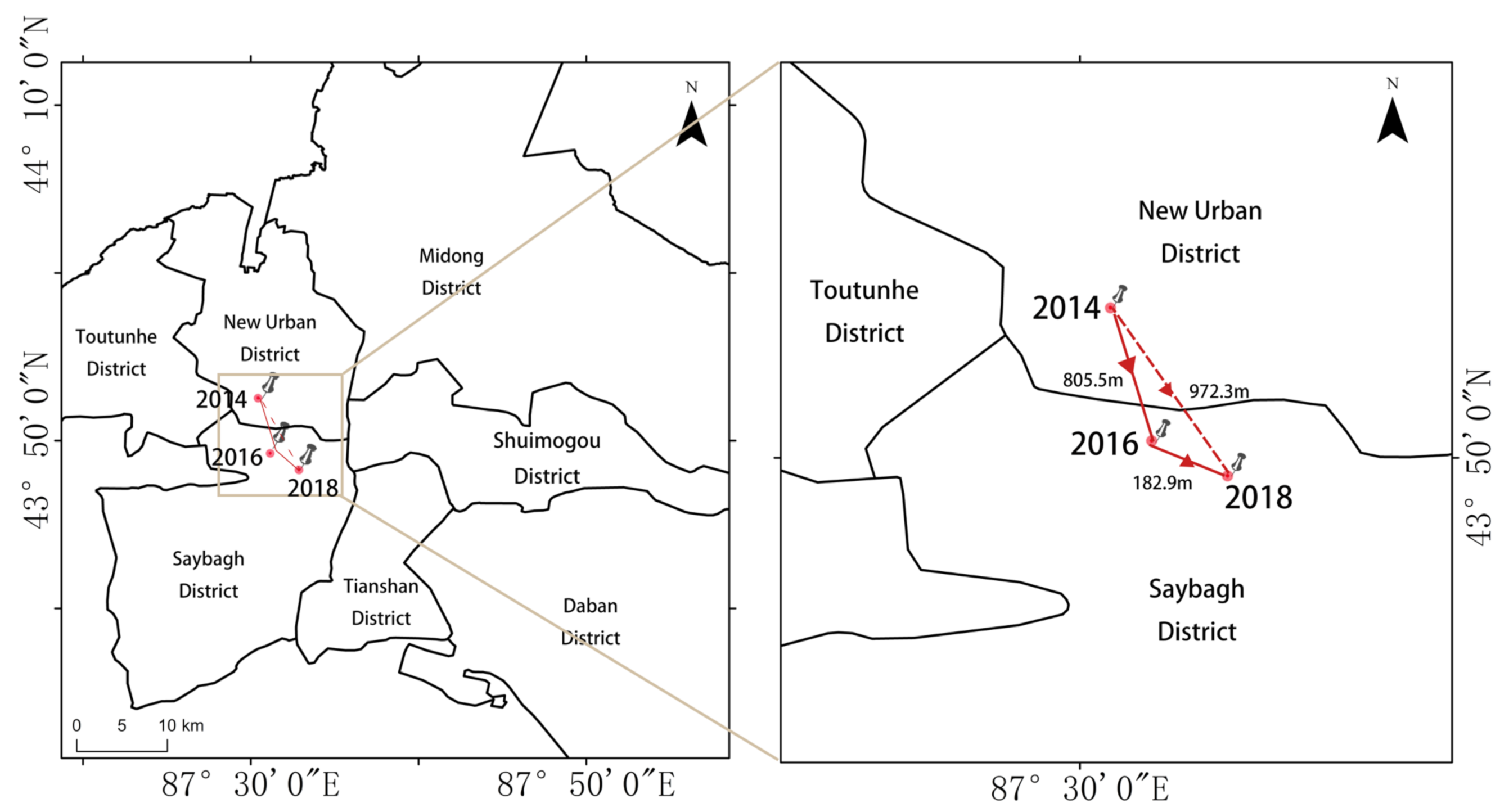
3.2. Change of the Center of Gravity of HFMD
3.3. Analysis of the Driving Factors of HFMD
- (1)
- Factor detector is mainly used to detect influencing factors’ explanatory powers. Each driving factor has a different degree of influence. The top 5 driving factors of HFMD were ranked by the q-value (Table 4) as follows: population density (X2) > road density (X3) > GDP (X1) > temperature (X4) > precipitation (X5) > wind speed (X6).
- (2)
- Interaction detector is mainly used to calculate the interactions among different factors. The analysis results showed a high degree of consistency with the previous section. Furthermore, indicated that the influence of any two factors on the HFMD cases was enhanced under their interaction. Table 5, Table 6 and Table 7 show the results of the interactions of population density (X2) with other factors: X2∩X3 (0.878) > X2∩X6 (0.830) > X2∩X1 (0.829) > X2∩X4 (0.826) > X2∩X5 (0.825). The results showed that the interaction between population density∩ road density had the strongest effect on the spatial distribution of HFMD in 2014. Similarly, the interaction between population density∩ road density (q = 0.881) had the strongest effect on the spatial distribution of HFMD in 2016, the interaction between population density∩ road density (q = 0.859) also had the strongest effect on the spatial distribution of HFMD in 2018. This phenomenon shows that socioeconomic factors such as “fortifiers” can strengthen the explanatory powers of other factors regarding HFMD spatial heterogeneity.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Qi, H.; Chen, Y.; Xu, D.; Su, H.; Zhan, L.; Xu, Z.; Huang, Y.; He, Q.; Hu, Y.; Lynn, H.; et al. Impact of meteorological factors on the incidence of childhood hand, foot, and mouth disease (HFMD) analyzed by DLNMs-based time series approach. Infect. Dis. Poverty 2018, 7, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Z.; Meng, Y.; Xiang, H.; Lu, Y.; Liu, S. Association of Short-Term Exposure to Meteorological Factors and Risk of Hand, Foot, and Mouth Disease: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Heal. 2020, 17, 8017. [Google Scholar] [CrossRef] [PubMed]
- Ooi, M.H.; Wong, S.C.; Lewthwaite, P.; Cardosa, M.J.; Solomon, T. Clinical features, diagnosis, and management of enterovirus 71. Lancet Neurol. 2010, 9, 1097–1105. [Google Scholar] [CrossRef]
- Wu, J.T.; Jit, M.; Zheng, Y.; Leung, K.; Xing, W.; Yang, J.; Liao, Q.; Cowling, B.J.; Yang, B.; Lau, E.H.Y.; et al. Routine Pediatric Enterovirus 71 Vaccination in China: A Cost-Effectiveness Analysis. PLoS Med. 2016, 13, e1001975. [Google Scholar] [CrossRef]
- Park, S.K.; Park, B.; Ki, M.; Kim, H.; Lee, K.; Jung, C.; Sohn, Y.M.; Choi, S.-M.; Kim, D.-K.; Lee, D.S.; et al. Transmission of Seasonal Outbreak of Childhood Enteroviral Aseptic Meningitis and Hand-foot-mouth Disease. J. Korean Med Sci. 2010, 25, 677–683. [Google Scholar] [CrossRef]
- Gui, J.; Liu, Z.; Zhang, T.; Hua, Q.; Jiang, Z.; Chen, B.; Gu, H.; Lv, H.; Dong, C. Epidemiological Characteristics and Spatial-Temporal Clusters of Hand, Foot, and Mouth Disease in Zhejiang Province, China, 2008-2012. PLoS ONE 2015, 10, e0139109. [Google Scholar] [CrossRef] [Green Version]
- Yan, S.; Wei, L.; Duan, Y.; Li, H.; Liao, Y.; Lv, Q.; Zhu, F.; Wang, Z.; Lu, W.; Yin, P.; et al. Short-Term Effects of Meteorological Factors and Air Pollutants on Hand, Foot and Mouth Disease among Children in Shenzhen, China, 2009–2017. Int. J. Environ. Res. Public Heal. 2019, 16, 3639. [Google Scholar] [CrossRef] [Green Version]
- Peng, D.; Ma, Y.; Liu, Y.; Lv, Q.; Yin, F. Epidemiological and aetiological characteristics of hand, foot, and mouth disease in Sichuan Province, China, 2011–2017. Sci. Rep. 2020, 10, 6117. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Qiu, W.; Xu, C.; Wang, J. A spatiotemporal mixed model to assess the influence of environmental and socioeconomic factors on the incidence of hand, foot and mouth disease. BMC Public Heal. 2018, 18, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Lai, Y.; Du, Z.; Zhang, W.; Feng, C.; Li, R.; Hao, Y. Spatiotemporal Distribution of Hand, Foot, and Mouth Disease in Guangdong Province, China and Potential Predictors, 2009–2012. Int. J. Environ. Res. Public Heal. 2019, 16, 1191. [Google Scholar] [CrossRef] [Green Version]
- Hu, M.; Li, Z.; Wang, J.; Jia, L.; Liao, Y.; Lai, S.; Guo, Y.; Zhao, D.; Yang, W. Determinants of the Incidence of Hand, Foot and Mouth Disease in China Using Geographically Weighted Regression Models. PLoS ONE 2012, 7, e38978. [Google Scholar] [CrossRef]
- Hong, Z.; Hao, H.; Li, C.; Du, W.; Wei, L.; Wang, H. Exploration of potential risks of Hand, Foot, and Mouth Disease in Inner Mongolia Autonomous Region, China Using Geographically Weighted Regression Model. Sci. Rep. 2018, 8, 17707. [Google Scholar] [CrossRef]
- Lin, H.; Zou, H.; Wang, Q.; Liu, C.; Lang, L.; Hou, X.; Li, Z. Short-Term Effect of El Niño-Southern Oscillation on Pediatric Hand, Foot and Mouth Disease in Shenzhen, China. PLoS ONE 2013, 8, e65585. [Google Scholar] [CrossRef]
- Cao, C.; Li, G.; Zheng, S.; Cheng, J.; Lei, G.; Tian, K.; Wu, Y.; Xie, X.; Xu, M.; Ji, W. Research on the environmental impact factors of Hand-Foot-Mouth Disease in Shenzhen, China using RS and GIS technologies. In Proceedings of the 2012 IEEE International Geoscience and Remote Sensing Symposium, Munich, Germany, 22–27 July 2012; 2012; pp. 7240–7243. [Google Scholar]
- Huang, J.; Chen, S.; Wu, Y.; Tong, Y.; Wang, L.; Zhu, M.; Hu, S.; Guan, X.; Wei, S. Quantifying the influence of temperature on hand, foot and mouth disease incidence in Wuhan, Central China. Sci. Rep. 2018, 8, 1934. [Google Scholar] [CrossRef] [Green Version]
- Fu, T.; Chen, T.; Dong, Z.-B.; Luo, S.-Y.; Miao, Z.; Song, X.-P.; Huang, R.-T.; Sun, J.-M. Development and comparison of forecast models of hand-foot-mouth disease with meteorological factors. Sci. Rep. 2019, 9, 15691. [Google Scholar] [CrossRef]
- Cheng, J.; Wu, J.; Xu, Z.; Zhu, R.; Wang, X.; Li, K.; Wen, L.; Yang, H.; Su, H. Associations between extreme precipitation and childhood hand, foot and mouth disease in urban and rural areas in Hefei, China. Sci. Total. Environ. 2014, 497–498, 484–490. [Google Scholar] [CrossRef]
- Yang, B.; Lau, E.H.Y.; Wu, P.; Cowling, B.J. Transmission of Hand, Foot and Mouth Disease and Its Potential Driving Factors in Hong Kong. Sci. Rep. 2016, 6, 27500. [Google Scholar] [CrossRef] [Green Version]
- Li, T.; Yang, Z.; Liu, X.; Kang, Y.; Wang, M. Hand-foot-and-mouth disease epidemiological status and relationship with me-teorological variables in Guangzhou, southern China, 2008–2012. Rev. Inst. Med. Trop. Sao Paulo 2014, 56, 533–539. [Google Scholar] [CrossRef]
- Deng, T.; Huang, Y.; Yu, S.; Gu, J.; Huang, C.; Xiao, G.; Hao, Y. Spatial-Temporal Clusters and Risk Factors of Hand, Foot, and Mouth Disease at the District Level in Guangdong Province, China. PLoS ONE 2013, 8, e56943. [Google Scholar] [CrossRef] [Green Version]
- National Bureau of Statistics, State Council of the Republic of China. Statistical Bulletin of Urumqi National Economic and Social Development 2019. Available online: http://www.xinjiang.gov.cn/ (accessed on 1 March 2021).
- Dai, L.; Zhang, Y.; Wang, L.; Zheng, S.; Xu, W. Assessment of Carbon Density in Natural Mountain Forest Ecosystems at Northwest China. Int. J. Environ. Res. Public Heal. 2021, 18, 2098. [Google Scholar] [CrossRef]
- Abduwaiti, A.; Liu, X.; Yan, C.; Xue, Y.; Jin, T.; Wu, H.; He, P.; Bao, Z.; Liu, Q. Testing Biodegradable Films as Alternatives to Plastic-Film Mulching for Enhancing the Yield and Economic Benefits of Processed Tomato in Xinjiang Region. Sustain 2021, 13, 3093. [Google Scholar] [CrossRef]
- Fu, R.; Zhang, X.; Yang, D.; Cai, T.; Zhang, Y. The Relationship between Urban Vibrancy and Built Environment: An Empirical Study from an Emerging City in an Arid Region. Int. J. Environ. Res. Public Heal. 2021, 18, 525. [Google Scholar] [CrossRef]
- Liu, Y. Sustainable Development in Urban Areas: Contributions from Generalized Trade. Sustain. Cities Soc. 2020, 61, 102312. [Google Scholar] [CrossRef]
- Song, C.; Yang, X.; Shi, X.; Bo, Y.; Wang, J. Estimating missing values in China’s official socioeconomic statistics using progressive spatiotemporal Bayesian hierarchical modeling. Sci. Rep. 2018, 8, 10055. [Google Scholar] [CrossRef]
- Bo, Y.-C.; Song, C.; Wang, J.-F.; Li, X.-W. Using an autologistic regression model to identify spatial risk factors and spatial risk patterns of hand, foot and mouth disease (HFMD) in Mainland China. BMC Public Heal. 2014, 14, 358. [Google Scholar] [CrossRef] [Green Version]
- Du, Z.; Huang, Y.; Lawrence, W.R.; Xu, J.; Yang, Z.; Lu, J.; Zhang, Z.; Hao, Y. Leading Enterovirus Genotypes Causing Hand, Foot, and Mouth Disease in Guangzhou, China: Relationship with Climate and Vaccination against EV71. Int. J. Environ. Res. Public Heal. 2021, 18, 292. [Google Scholar] [CrossRef]
- Fan, F.; Fan, W. Understanding spatial-temporal urban expansion pattern (1990–2009) using impervious surface data and landscape indexes: a case study in Guangzhou (China). J. Appl. Remote. Sens. 2014, 8, 083609. [Google Scholar] [CrossRef] [Green Version]
- Peng, T.; Sun, C.; Feng, S.; Zhang, Y.; Fan, F. Temporal and Spatial Variation of Anthropogenic Heat in the Central Urban Area: A Case Study of Guangzhou, China. ISPRS Int. J. Geo-Information 2021, 10, 160. [Google Scholar] [CrossRef]
- Wang, J.F.; Li, X.H.; Christakos, G.; Liao, Y.L.; Zhang, T.; Gu, X.; Zheng, X.Y. Geographical detectors-based health risk assessment and its application in the neural tube defects study of the Heshun region, China. Int. J. Geogr. Inf. Sci. 2010, 24, 107–127. [Google Scholar] [CrossRef]
- Ju, H.; Zhang, Z.; Zuo, L.; Wang, J.; Zhang, S.; Wang, X.; Zhao, X. Driving forces and their interactions of built-up land expansion based on the geographical detector—A case study of Beijing, China. Int. J. Geogr. Inf. Sci. 2016, 30, 2188–2207. [Google Scholar] [CrossRef]
- Qi, X.; Si, Z.; Zhong, T.; Huang, X.; Crush, J. Spatial determinants of urban wet market vendor profit in Nanjing, China. Habitat Int. 2019, 94, 102064. [Google Scholar] [CrossRef]
- Xie, W.; Li, X.; Jian, W.; Yang, Y.; Liu, H.; Robledo, L.; Nie, W. A Novel Hybrid Method for Landslide Susceptibility Mapping-Based GeoDetector and Machine Learning Cluster: A Case of Xiaojin County, China. ISPRS Int. J. Geo-Inf. 2021, 10, 93. [Google Scholar] [CrossRef]
- Zhang, J.; Yu, L.; Li, X.; Zhang, C.; Shi, T.; Wu, X.; Yang, C.; Gao, W.; Li, Q.; Wu, G. Exploring Annual Urban Expansions in the Guangdong-Hong Kong-Macau Greater Bay Area: Spatiotemporal Features and Driving Factors in 1986–2017. Remote. Sens. 2020, 12, 2615. [Google Scholar] [CrossRef]
- Wang, J.; Hu, T.; Sun, D.; Ding, S.; Carr, M.J.; Xing, W.; Li, S.; Wang, X.; Shi, W. Epidemiological characteristics of hand, foot, and mouth disease in Shandong, China, 2009–2016. Sci. Rep. 2017, 7, 8900. [Google Scholar] [CrossRef] [Green Version]
- Qi, L.; Tang, W.; Zhao, H.; Ling, H.; Su, K.; Zhao, H.; Li, Q.; Shen, T. Epidemiological Characteristics and Spatial-Temporal Distribution of Hand, Foot, and Mouth Disease in Chongqing, China, 2009–2016. Int. J. Environ. Res. Public Heal. 2018, 15, 270. [Google Scholar] [CrossRef] [Green Version]
- Song, C.; He, Y.; Bo, Y.; Wang, J.; Ren, Z.; Yang, H. Risk Assessment and Mapping of Hand, Foot, and Mouth Disease at the County Level in Mainland China Using Spatiotemporal Zero-Inflated Bayesian Hierarchical Models. Int. J. Environ. Res. Public Heal. 2018, 15, 1476. [Google Scholar] [CrossRef] [Green Version]
- Tian, L.; Liang, F.; Xu, M.; Jia, L.; Pan, X.; Clements, A.C.A. Spatio-temporal analysis of the relationship between meteorological factors and hand-foot-mouth disease in Beijing, China. BMC Infect. Dis. 2018, 18, 158. [Google Scholar] [CrossRef] [Green Version]
- Yi, S.; Wang, H.; Yang, S.; Xie, L.; Gao, Y.; Ma, C. Spatial and Temporal Characteristics of Hand-Foot-and-Mouth Disease and Its Response to Climate Factors in the Ili River Valley Region of China. Int. J. Environ. Res. Public Heal. 2021, 18, 1954. [Google Scholar] [CrossRef]
- Huang, J.; Wang, J.; Bo, Y.; Xu, C.; Hu, M.; Huang, D. Identification of Health Risks of Hand, Foot and Mouth Disease in China Using the Geographical Detector Technique. Int. J. Environ. Res. Public Heal. 2014, 11, 3407–3423. [Google Scholar] [CrossRef]
- Bie, Q.; Qiu, D.; Hu, H.; Ju, B. Spatial and Temporal Distribution Characteristics of Hand-Foot-Mouth Disease in China. J. Geo-Inf. Sci. 2010, 12, 380–384. [Google Scholar] [CrossRef]
- Zhu, Q.; Hao, Y.T.; Yu, S.C. Epidemiology Characteristic and Spatial Time Analysis of Hand, Foot, and Mouth Disease in Guangdong Province from 2008 to 2010. Mod. Prev. Med. 2011, 38, 1824–1831. [Google Scholar]
- Huang, J.-X.; Wang, J.-F.; Li, Z.-J.; Wang, Y.; Lai, S.-J.; Yang, W.-Z. Visualized Exploratory Spatiotemporal Analysis of Hand-Foot-Mouth Disease in Southern China. PLoS ONE 2015, 10, e0143411. [Google Scholar] [CrossRef]
- Kim, B.I.; Ki, H.; Park, S.; Cho, E.; Chun, B.C. Effect of Climatic Factors on Hand, Foot, and Mouth Disease in South Korea, 2010-2013. PLoS ONE 2016, 11, e0157500. [Google Scholar] [CrossRef]
- Yi, X.; Chang, Z.; Zhao, X.; Ma, Y.; Liu, F.; Xiao, X. The temporal characteristics of the lag-response relationship and related key time points between ambient temperature and hand, foot and mouth disease: A multicity study from mainland China. Sci. Total. Environ. 2020, 749, 141679. [Google Scholar] [CrossRef]
- Chen, C.; Lin, H.; Li, X.; Lang, L.; Xiao, X.; Ding, P.; He, P.; Zhang, Y.; Wang, M.; Liu, Q. Short-term effects of meteorological factors on children hand, foot and mouth disease in Guangzhou, China. Int. J. Biometeorol. 2013, 58, 1605–1614. [Google Scholar] [CrossRef]
- Huang, Y.; Deng, T.; Yu, S.; Gu, J.; Huang, C.; Xiao, G.; Hao, Y. Effect of meteorological variables on the incidence of hand, foot, and mouth disease in children: a time-series analysis in Guangzhou, China. BMC Infect. Dis. 2013, 13, 134. [Google Scholar] [CrossRef] [Green Version]
- Liao, Y.; Ouyang, R.; Wang, J.; Xu, B. A study of spatiotemporal delay in hand, foot and mouth disease in response to weather variations based on SVD: a case study in Shandong Province, China. BMC Public Heal. 2015, 15, 71. [Google Scholar] [CrossRef] [Green Version]
- Bo, Z.; Ma, Y.; Chang, Z.; Zhang, T.; Liu, F.; Zhao, X.; Long, L.; Yi, X.; Xiao, X.; Li, Z. The spatial heterogeneity of the associations between relative humidity and pediatric hand, foot and mouth disease: Evidence from a nation-wide multicity study from mainland China. Sci. Total. Environ. 2020, 707, 136103. [Google Scholar] [CrossRef]
- Luo, C.; Ma, Y.; Liu, Y.; Lv, Q.; Yin, F. The burden of childhood hand-foot-mouth disease morbidity attributable to relative humidity: a multicity study in the Sichuan Basin, China. Sci. Rep. 2020, 10, 19394. [Google Scholar] [CrossRef]
- Dong, W.; Li, X.; Yang, P.; Liao, H.; Wang, X.; Wang, Q. The Effects of Weather Factors on Hand, Foot and Mouth Disease in Beijing. Sci. Rep. 2016, 6, 19247. [Google Scholar] [CrossRef] [Green Version]
- Yin, F.; Zhang, T.; Liu, L.; Lv, Q.; Li, X. The Association between Ambient Temperature and Childhood Hand, Foot and Mouth Disease in Chengdu, China: A Distributed Lag Non-linear Analysis. Sci. Rep. 2016, 6, 27305. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number | National Code of Current Address | Address Longitude and Latitude | Case Classification | Date of Accident | Reporting Unit |
|---|---|---|---|---|---|
| 1 | 650100000 | 88.209° E 43.363° N | clinically diagnosed cases | 2014/1/1 | Tianshan District Hospital |
| 2 | 650100001 | 88.119° E 43.463° N | clinically diagnosed cases | 2016/1/1 | Midong District Hospital |
| N | 650100002 | 88.129° E 43.553° N | clinically diagnosed cases | 2018/1/1 | Tianshan District Hospital |
| Graphical Representation | Relationship | Interaction |
|---|---|---|
 | q(X1∩X2) < Min(q(X1), q(X2)) | Nonlinear weakening |
 | Min(q(X1), q(X2)) < q(X1∩X2) < Max(q(X1)), q(X2)) | Single-factor nonlinear weakening |
 | q(X1∩X2) > Max(q(X1), q(X2)) | Double-factor enhancement |
 | q(X1∩X2) = q(X1) + q(X2) | Independent |
 | q(X1∩X2) > q(X1) + q(X2) | Nonlinear enhancement |
| Year | 2014 | 2015 | 2018 | Average Number of Cases | Average Growth Rate (%) |
|---|---|---|---|---|---|
| District | |||||
| Tianshan | 423 | 846 | 1123 | 797 | 66.37 |
| Shayibuck | 675 | 774 | 883 | 777 | 14.37 |
| Toutunhe | 223 | 327 | 289 | 280 | 17.5 |
| New Urban | 664 | 793 | 1059 | 839 | 26.4 |
| Shuimogou | 292 | 593 | 586 | 490 | 50.95 |
| Midong | 247 | 295 | 435 | 326 | 33.45 |
| Daban | 4 | 33 | 43 | 27 | 377 |
| Urumqi | 25 | 28 | 65 | 39 | 72.07 |
| Sum | 2553 | 3689 | 4483 |
| Level of Impact (q-Value) | Gross Domestic Product (GDP) X1 | Population Density X2 | Road Density X3 | Temperature X4 | Precipitation X5 | Wind Speed X6 |
|---|---|---|---|---|---|---|
| 2014 | 0.598 | 0.569 | 0.623 | 0.462 | 0.368 | 0.194 |
| 2016 | 0.451 | 0.552 | 0.449 | 0.495 | 0.414 | 0.151 |
| 2018 | 0.450 | 0.540 | 0.558 | 0.546 | 0.408 | 0.147 |
| Mean Value | 0.500 | 0.554 | 0.544 | 0.501 | 0.397 | 0.164 |
| Variable | GDP X1 | Population Density X2 | Road Density X3 | Temperature X4 | Precipitation X5 | Wind Speed X6 |
|---|---|---|---|---|---|---|
| X1 | 0.598 | |||||
| X2 | 0.829 | 0.569 | ||||
| X3 | 0.776 | 0.878 | 0.623 | |||
| X4 | 0.637 | 0.826 | 0.667 | 0.462 | ||
| X5 | 0.677 | 0.825 | 0.665 | 0.577 | 0.368 | |
| X6 | 0.594 | 0.830 | 0.625 | 0.834 | 0.362 | 0.194 |
| Variable | GDP X1 | Population Density X2 | Road Density X3 | Temperature X4 | Precipitation X5 | Wind Speed X6 |
|---|---|---|---|---|---|---|
| X1 | 0.451 | |||||
| X2 | 0.849 | 0.552 | ||||
| X3 | 0.580 | 0.881 | 0.449 | |||
| X4 | 0.626 | 0.667 | 0.619 | 0.495 | ||
| X5 | 0.601 | 0.665 | 0.472 | 0.572 | 0.414 | |
| X6 | 0.411 | 0.619 | 0.575 | 0.571 | 0.594 | 0.151 |
| Variable | GDP X1 | Population Density X2 | Road Density X3 | Temperature X4 | Precipitation X5 | Wind Speed X6 |
|---|---|---|---|---|---|---|
| X1 | 0.450 | |||||
| X2 | 0.805 | 0.540 | ||||
| X3 | 0.589 | 0.859 | 0.558 | |||
| X4 | 0.634 | 0.818 | 0.669 | 0.546 | ||
| X5 | 0.592 | 0.799 | 0.667 | 0.567 | 0.408 | |
| X6 | 0.612 | 0.609 | 0.573 | 0.624 | 0.577 | 0.147 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gao, Y.; Wang, H.; Yi, S.; Wang, D.; Ma, C.; Tan, B.; Wei, Y. Spatial and Temporal Characteristics of Hand-Foot-and-Mouth Disease and Their Influencing Factors in Urumqi, China. Int. J. Environ. Res. Public Health 2021, 18, 4919. https://doi.org/10.3390/ijerph18094919
Gao Y, Wang H, Yi S, Wang D, Ma C, Tan B, Wei Y. Spatial and Temporal Characteristics of Hand-Foot-and-Mouth Disease and Their Influencing Factors in Urumqi, China. International Journal of Environmental Research and Public Health. 2021; 18(9):4919. https://doi.org/10.3390/ijerph18094919
Chicago/Turabian StyleGao, Yibo, Hongwei Wang, Suyan Yi, Deping Wang, Chen Ma, Bo Tan, and Yiming Wei. 2021. "Spatial and Temporal Characteristics of Hand-Foot-and-Mouth Disease and Their Influencing Factors in Urumqi, China" International Journal of Environmental Research and Public Health 18, no. 9: 4919. https://doi.org/10.3390/ijerph18094919