
Parental Feeding, Child Eating and Physical Activity: Differences in Children Living with and without Asthma


Abstract
:1. Introduction
- Establish whether differences between parental attitudes to feeding and activity or child eating and activity levels exist in children living with and without asthma.
- Explore any differences in the relationship between child BMI scores with parental feeding practices, parental attitudes toward physical activity, child eating behaviors and child activity levels in children living with asthma compared to healthy controls.
- Explore whether asthma control moderates any relationships between child BMI scores with parental attitudes to feeding and activity, or child eating and activity levels.
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measures
2.2.1. Parental Feeding Behaviors
2.2.2. Parental Practices around Child Activity
2.2.3. Perceptions of Child Weight
2.2.4. Child Eating
2.2.5. Child Activity
2.2.6. Asthma Control
2.3. Statistical Analysis
3. Results
3.1. Demographic Information
3.2. Differences between Parental Attitudes toward Feeding and Exercise and Child Eating and Exercise Behaviors
3.3. Relationships between Parental Attitudes toward Feeding and Exercise and Child Eating and Exercise Behaviors with Child Weight
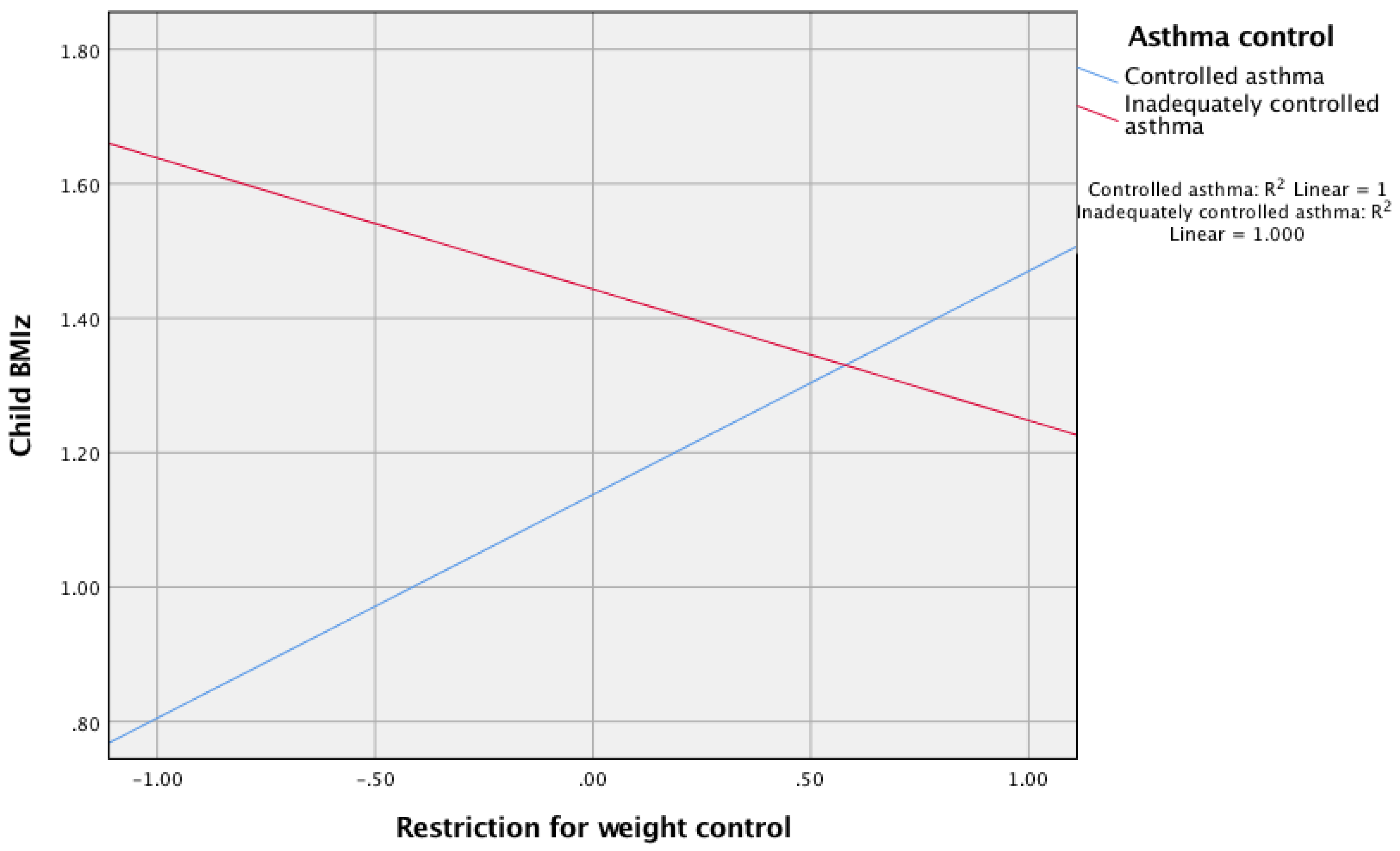
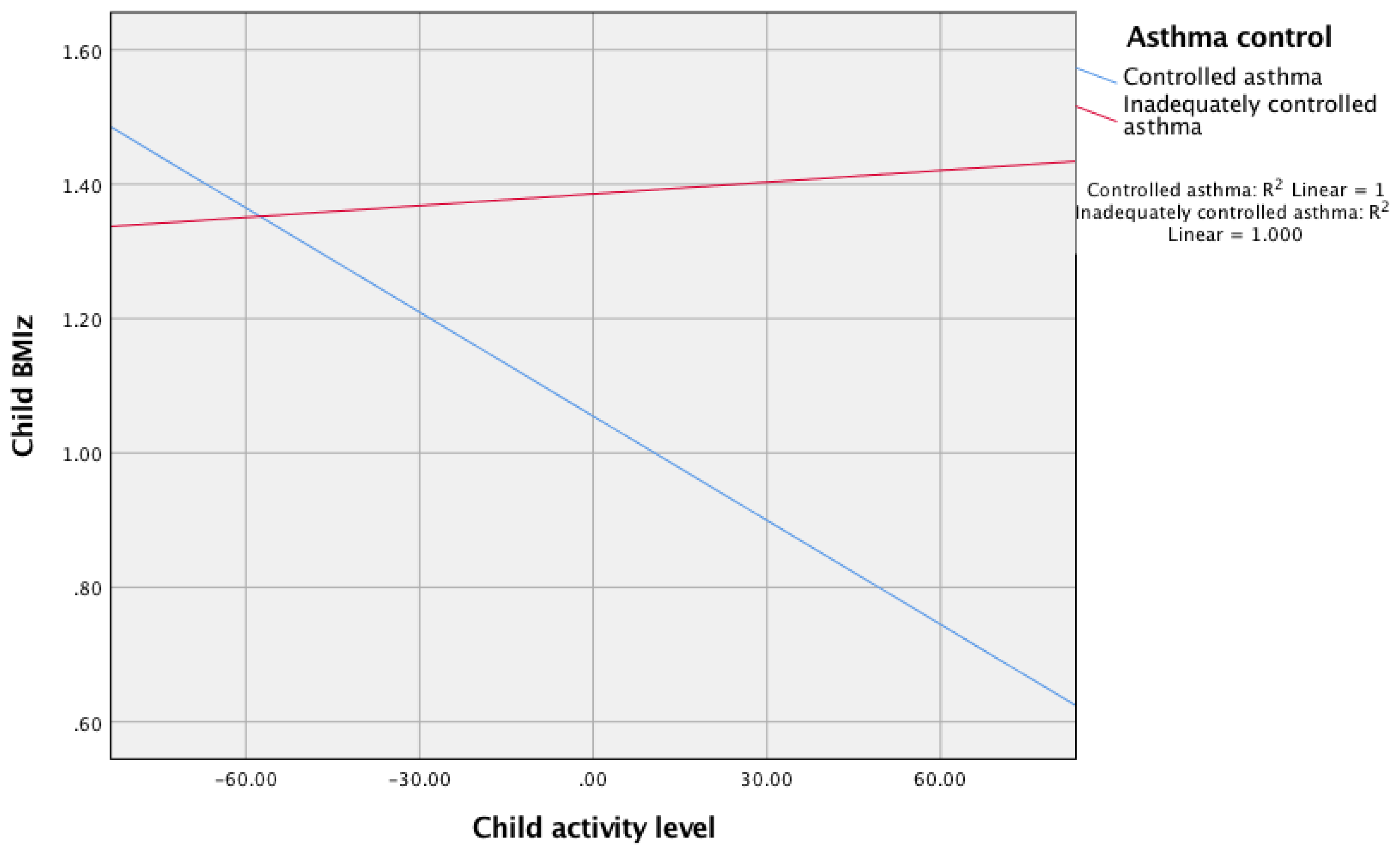
3.4. Asthma Control as a Moderator to the Relationship between Restriction for Weight Control and Child Activity Level with Child BMIz
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Asthma Key Facts. Available online: https://www.who.int/respiratory/asthma/en/ (accessed on 29 July 2020).
- Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention. Available online: https://ginasthma.org/gina-reports/ (accessed on 1 May 2020).
- Nunes, C.; Pereira, A.M.; Morais-Almeida, M. Asthma costs and social impact. Asthma Res. Pract. 2017, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keeble, E.; Kosarova, L. Focus on: Emergency Hospital Care for Children and Young People. QualityWatch. Available online: https://www.nuffieldtrust.org.uk/files/2018-10/1540142848_qualitywatch-emergency-hospital-care-children-and-young-people-full.pdf (accessed on 10 August 2020).
- Sundbom, F.; Malinovschi, A.; Lindberg, E.; Alving, K.; Janson, C. Effects of poor asthma control, insomnia, anxiety and depression on quality of life in young asthmatics. J. Asthma 2016, 53, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Baffi, C.W.; Winnica, D.E.; Holguin, F. Asthma and obesity: Mechanisms and clinical implications. Asthma Res. Pract. 2015, 1, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gross, E.; Lee, D.S.; Hotz, A.; Ngo, K.C.; Rastogi, D. Impact of obesity on asthma morbidity during a hospitalization. Hosp. Pediatrics 2018, 8, 538–546. [Google Scholar] [CrossRef] [Green Version]
- Carpaij, O.A.; van den Berge, M. The asthma-obesity relationship: Underlying mechanisms and treatment implications. Curr. Opin. Pulm. Med. 2018, 24, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Forno, E.; Celedón, J.C. The effect of obesity, weight gain, and weight loss on asthma inception and control. Curr. Opin. Allergy Clin. Immunol. 2017, 17, 123–130. [Google Scholar] [CrossRef]
- Sahoo, K.; Sahoo, B.; Choudhury, A.K.; Sofi, N.Y.; Kumar, R.; Bhadoria, A.S. Childhood obesity: Causes and consequences. J. Fam. Med. Prim. Care 2015, 4, 187–192. [Google Scholar]
- Farrow, C.F.; Haycraft, E.; Blissett, J.M. Teaching our children when to eat: How parental feeding practices inform the development of emotional eating: A longitudinal experiment design. Am. J. Clin. Nutr. 2015, 101, 908–913. [Google Scholar] [CrossRef] [Green Version]
- Scaglioni, S.; De Cosmi, V.; Ciappolino, V.; Parazzini, F.; Bramilla, P.; Agostoni, C. Factors influencing children’s eating behaviours. Nutrients 2018, 10, 706. [Google Scholar] [CrossRef] [Green Version]
- Kral, T.V.E.; Souders, M.C.; Thompkins, V.H.; Remiker, A.M.; Eriksen, W.T.; Pinto-Martin, J.A. Child eating behaviours and caregiver feeding practices in children with autism spectrum disorders. Public Health Nurs. 2015, 32, 488–497. [Google Scholar] [CrossRef] [PubMed]
- Allen, H.A.; Chambers, A.; Blissett, J.; Chechlacz, M.; Barrett, T.; Higgs, S.; Nouwen, A. Relationships between parental feeding practices and neural responses to food cues in adolescents. PLoS ONE 2016, 11, e0157037. [Google Scholar]
- Castro-Rodriguez, J.A.; Garcia-Marcos, L. What are the effects of a Mediterranean diet on allergies and asthma in children? Front. Pediatrics 2017, 5, 330–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borhani, R.; Asadi, N.; Mohsenpour, M. The experiences of mothers with asthmatic children: A content analysis. J. Caring Sci. 2012, 1, 115–121. [Google Scholar]
- Moreau, D.; Kalaboka, S.; Choquet, M.; Annesi-Maesano, I. Asthma, obesity, and eating behaviors according to the Diagnostic and Statistical Manual of Mental Disorders IV in a large population-based sample of adolescents. Am. J. Clin. Nutr. 2009, 89, 1292–1298. [Google Scholar] [CrossRef] [PubMed]
- Groth, S.; Rhee, H.; Kitzman, H. Relationships among obesity, physical activity and sedentary behaviour in young adolescents with and without lifetime asthma. J. Asthma 2016, 53, 19–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhatia, R.; Abu-Hasan, M.; Weinberger, M. Exercise-induced dyspnea in children and adolescents: Differential diagnosis. Pediatrics Ann. 2019, 48, e121–e127. [Google Scholar] [CrossRef]
- Park, S.J.; Sawyer, S.M.; Glaun, D.E. Childhood asthma complicated by anxiety: An application of cognitive behavioural therapy. J. Pediatric Child Health 1996, 32, 183–187. [Google Scholar] [CrossRef]
- Sicouri, G.; Sharpe, L.; Hudson, J.L.; Dudeney, J.; Jaffe, A.; Selvadurai, H.; Lorimer, S.; Hunt, C. Threat interpretation and parental influences for children with asthma and anxiety. Behav. Res. Ther. 2017, 89, 14–23. [Google Scholar] [CrossRef]
- Bruzzese, J.M.; Reigada, L.C.; Lamm, A.; Wang, J.; Li, M.; Zandieh, S.O.; Klein, R.G. Association of youth and caregiver anxiety and asthma care among urban young adolescents. Acad. Pediatrics 2016, 16, 792–798. [Google Scholar] [CrossRef] [Green Version]
- Kornblit, A.; Cain, A.; Bauman, L.J.; Brown, N.M.; Reznik, M. Parental perspectives of barriers to physical activity in urban schoolchildren with asthma. Acad. Pediatrics 2018, 18, 310–316. [Google Scholar] [CrossRef]
- Koinis-Mitchell, D.; Kopel, S.J.; Esteban, C.A.; Seifer, R.; Vehse, N.W.; Chau, S.; Jelalian, E. Asthma status and physical activity in urban children. Am. J. Respir. Crit. Care Med. 2017, 195, A2993. [Google Scholar]
- Guillenminault, L.; Williams, E.J.; Scott, H.A.; Berthon, B.S.; Jensen, M.; Wood, L.G. Diet and asthma: Is it time to adapt our message? Nutrients 2017, 9, 1227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freeman, J.V.; Cole, T.J.; Chinn, S.; Jones, P.R.; White, E.M.; Preece, M.A. Cross sectional stature and weight reference curves for the UK, 1990. Arch. Dis. Child. 1995, 73, 17–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Musher-Eizenman, D.; Holub, S. Comprehensive feeding practices questionnaire: Validation of a new measure of parental feeding practices. J. Pediatric Psychol. 2007, 32, 960–972. [Google Scholar] [CrossRef] [PubMed]
- Mais, L.A.; Warkentin, S.; Latorre, M.R.D.O.; Carnell, S.; Taddei, J.A.D.A.C. Validation of the comprehensive feeding practices questionnaire among Brazilian families of school-aged children. Front. Nutr. 2015, 2, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Fleary, S.A.; Ettienne, R. The Relationship between food parenting practices, parental diet and their adolescents’ diet. Appetite 2019, 135, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Haycraft, E.; Powell, F.; Meyer, C. Activity-related parenting practices: Development of the parenting related to activity measure (PRAM) and links with mothers’ eating psychopathology and compulsive exercise beliefs. Eur. Eat. Disord. Rev. 2015, 23, 51–61. [Google Scholar] [CrossRef] [Green Version]
- Birch, L.L.; Fisher, J.O.; Grimm-Thomas, K.; Markey, C.N.; Sawyer, R.; Johnson, S.L. Confirmatory factor analysis of the child feeding questionnaire: A measure of parental attitudes, beliefs and practices about child feeding and obesity proneness. Appetite 2001, 36, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Ek, A.; Sorjonen, K.; Eli, K.; Lindberg, L.; Nyman, J.; Marcus, C.; Nowicka, P. Associations between parental concerns about pre-schoolers’ weight and eating and parental feeding practices: Results from analyses of the child eating behaviour questionnaire, the child feeding questionnaire, and the lifestyle behaviour checklist. PLoS ONE 2016, 11, e0147257. [Google Scholar]
- Loth, K.A.; MacLehose, R.F.; Larson, N.; Berge, J.M.; Neumark-Sztainer, D. Food availability, modelling and restriction: How are these different aspects of the family eating environment related to adolescent dietary intake? Appetite 2016, 96, 80–86. [Google Scholar] [CrossRef] [Green Version]
- Wardle, J.; Guthrie, C.A.; Sanderson, S.; Rapoport, L. Development of the children’s eating behaviour questionnaire. J. Child Psychol. Psychiatry 2007, 42, 963–970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quah, P.L.; Fries, L.R.; Chan, M.J.; Fogel, A.; McCrickerd, K.; Goh, A.T.; Aris, I.A.; Lee, Y.S.; Pang, W.W.; Basnyat, I. Validation of the Children’s Eating Questionnaire in 5 and 6 year-old children: The GUSTO cohort study. Front. Psychol. 2019, 10, 824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mallan, K.M.; Daniels, L.A.; Nicholson, J.M. Obesogenic eating behaviours mediate the relationships between psychological problems and BMI in children. Obesity 2017, 25, 928–934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dos Passos, D.R.; Gigante, D.P.; Maciel, F.V.; Matijasevich, A. Children’s eating behaviour: Comparison between normal and overweight children from a school in Pelotas, Rio Grande do Sul, Brazil. Rev. Paul. Pediatr. 2015, 33, 42–49. [Google Scholar]
- de Groot, C.J.; van den Akker, E.L.T.; Rings, E.H.H.M.; Delemarre-van de Waal, H.A.; van der Grond, J. Brain structure, executive function and appetitive traits in adolescent obesity. Pediatric Obes. 2016, 12, 33–36. [Google Scholar] [CrossRef]
- Godin, G.; Shepard, R.J. A simple method to assess exercise behaviour in the community. Can. J. Appl. Sport Sci. 1985, 10, 141–146. [Google Scholar]
- Suorsa, K.I.; Cushing, C.C.; Mullins, A.J.; Meier, E.; Tackett, A.P.; Junghans, A.; Chaney, J.M.; Mullins, L.L. Adolescents and young adults with asthma and allergies: Physical activity, self-efficacy, social support, and subsequent psychosocial outcomes. Child. Health Care 2016, 45, 414–427. [Google Scholar] [CrossRef]
- Juniper, E.F.; O’Bryne, P.M.; Guyatt, G.H.; Ferrie, P.J.; King, D.R. Development and validation of a questionnaire to measure asthma control. Eur. Respir. J. 2001, 14, 902–907. [Google Scholar] [CrossRef]
- Olaguibel, J.M.; Quirce, S.; Juliá, B.; Fernández, C.; Fortuna, A.M.; Molina, J.; Plaza, V.; MAGIC Study Group. Measurement of asthma control according to global initiative for asthma guidelines: A comparison with the asthma control questionnaire. Respir. Res. 2012, 13, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, J.M.; Holbrook, J.T.; Wei, C.Y.; Gerald, L.B.; Teague, W.G.; Wise, R.A. Validation and psychometric properties of the Asthma Control Questionnaire among Children. J. Allergy Clin. Immunol. 2014, 133, 91–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juniper, E.F.; Gruffyd-Jones, K.; Ward, S.; Svensson, K. Asthma control questionnaire in children: Validation, measurement properties, interpretation. Eur. Respir. J. 2010, 36, 1410–1416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis, 2nd ed.; A Regression-Based Approach; Guilford Publications: New York, NY, USA, 2017. [Google Scholar]
- Faul, F.; Erdfelder, S.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freitas, F.R.; Moraes, D.E.B.; Warkentin, S.; Mais, L.A.; Ivers, J.F.; Taddei, J.A.A.C. Maternal restrictive feeding practices for child weight control and associated characteristics. J. Pediatr. 2019, 95, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Wood, L.G. Diet, obesity, and asthma. Ann. Am. Thorac. 2017, 14, S332–S338. [Google Scholar] [CrossRef]
- Douros, K.; Thanopoulou, M.I.; Boutopoulou, B.; Papadopoulou, A.; Papadimitriou, A.; Fretzayas, A.; Priftis, K.N. Adherence to the Mediterranean diet and inflammatory markers in children with asthma. Allergol. Immunopathol. 2019, 47, 209–213. [Google Scholar] [CrossRef]
- Jensen, M.E.; Gibson, P.G.; Collins, C.E.; Hilton, J.M.; Wood, L.G. Diet-induced weight loss in obese children with asthma: A randomized controlled trial. Clin. Exp. Allergy 2013, 775–784. [Google Scholar] [CrossRef]
- Luna-Pech, J.A.; Torres-Mendoza, B.M.; Luna-Pech, J.A.; Garcia-Cobas, C.Y.; Navarrete-Navarro, S.; Elizalde-Lozano, A.M. Normacarloric diet improves asthma related quality of life in obese pubertal adolescents. Int. Arch. Allergy Immunol. 2014, 163, 252–258. [Google Scholar] [CrossRef]
- Van Leeuwen, J.C.; Hoogstrate, M.; Duiverman, E.J.; Thio, B.J. Effects of dietary induced weight loss on exercise-induced bronchoconstriction in overweight and obese children. Pediatric Pulmonol. 2014, 49, 1155–1159. [Google Scholar] [CrossRef]
- Bhutta, Z.A.; Guerrant, R.L. Neurodevelopment, nutrition, and inflammation: The evolving global child health landscape. Pediatrics 2017, 139, 12–22. [Google Scholar] [CrossRef] [Green Version]
- Prescott, S.L. Early nutrition as a major determinant of ‘immune health’: Implications for allergy, obesity and other noncommunicable diseases. In Preventive Aspects of Early Nutrition; Fewtrell, M.S., Haschke, F., Prescott, S.L., Eds.; Vevey/S. Kager AG: Basel, Switzerland, 2016; pp. 1–17. [Google Scholar]
- Shaw, M.R.; Katz, J.; Benavides-Vaello, S.; Oneal, G.; Holliday, C. Views on exercise: A grounded theory exploration of the creation of exercise perceptions in Hispanic children with asthma. Hisp. Health Care Int. 2017, 15, 71–78. [Google Scholar] [CrossRef]
- Moonie, S.; Hogan, M.B. Challenges for the clinician: Physical activity among severe asthmatic patients with comorbid obesity. J. Allergy Clin. Immunol. 2018, 6, 823–824. [Google Scholar] [CrossRef]
- Lang, J.E.; Hossain, J.; Smith, K.; Lima, J.J. Asthma severity, exacerbation risk, and controller treatment burden in underweight and obese children. J. Asthma 2012, 49, 456–463. [Google Scholar] [CrossRef]
- Fredberg, J.J. Airway smooth muscle in asthma: Flirting with disaster. Eur. Respir. J. 1998, 12, 1252–1256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lövström, L.; Emtner, M.; Alving, K.; Nordall, L.; Borres, M.P.; Janson, C.; Malinovschi, A. High levels of physical activity are associated with poorer control asthma in young females but not males. Respirology 2015, 21, 79–87. [Google Scholar] [CrossRef] [Green Version]
- Toennensen, L.L.; Meteran, H.; Hostrup, M.; Geiker, N.R.W.; Jensen, C.B.; Porsbjerg, C.; Astrup, A.; Bangsbo, J.; Parker, D.; Backer, V. Effects of exercise and diet in nonobese asthma patients—A randomized controlled trial. J. Allergy Clin. Immunol. Pract. 2018, 6, 808–811. [Google Scholar]
- Sly, P.D.; Holt, P.G. Predicting steroid responsiveness in asthmatic children: Are we there yet? J. Allergy Clin. Immunol. 2019, 143, 927–929. [Google Scholar] [CrossRef] [Green Version]
- Han, J.; Nguyen, J.; Kim, Y.; Geng, B.; Romanowski, G.; Alejandro, L.; Proudfoot, J.; Xu, R.; Leibel, S. Effect of inhaled corticosteroid use on weight (BMI) in pediatric patients with moderate-severe asthma. J. Asthma 2019, 56, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Klok, T.; Kaptein, A.A.; Brand, P.L.P. Non-adherence in children with asthma reviewed: The need for improvement of asthma care and medical education. Pediatric Allergy Immunol. 2015, 26, 197–205. [Google Scholar] [CrossRef]
- Longo, C.; Bartlett, G.; Schuster, T.; Ducharme, F.M.; MacGibbon, B.; Barnett, T.A. Weight status and nonadherence to asthma maintenance therapy among children enrolled in a public drug insurance plan. J. Asthma 2019, 26, 1–11. [Google Scholar] [CrossRef]
- Selby, L.; Beresford, F.; Saglani, S. Emotional distress in children with problematic severe asthma is associated with parental anxiety and depression. Eur. Respir. J. 2018, 52, 1280. [Google Scholar]
- Steinsbekk, S.; Barker, E.D.; Llewellyn, C.; Fildes, A. Emotional feeding and emotional eating: Reciprocal processes and the influence of negative affectivity. Child Dev. 2017, 89, 1234–1246. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Asthma (n = 310) | No Asthma (n = 311) | |
|---|---|---|
| Parent age (mean, SD) | 41.24 (8.11) | 42.21 (8.21) |
| Parent gender (% female) | 66.1 | 75.6 |
| Parent BMI (mean, SD) | 27.44 (8.58) | 26.18 (7.03) |
| Parent marital status (%) | ||
| Single | 13.5 | 11.3 |
| Married | 61.3 | 54.7 |
| Co-habiting | 16.8 | 21.2 |
| Divorced | 6.8 | 8 |
| Widowed | 0.3 | 1.9 |
| Other | 1.3 | 2.9 |
| Parent education status (%) | ||
| To age 16 | 17.7 | 22.2 |
| AS-Level/A-Level/Other equivalent | 30.6 | 32.5 |
| Apprenticeship | 7.4 | 7.1 |
| Bachelor’s degree | 27.7 | 25.4 |
| Postgraduate degree | 14.2 | 9 |
| Education level not specified | 2.3 | 3.9 |
| Parent employment status (%) | ||
| Unemployed | 5.2 | 2.6 |
| Homemaker | 17.4 | 24.1 |
| Full time employment | 52.6 | 40.2 |
| Part time employment | 14.5 | 18 |
| Self-employed | 6.1 | 9.6 |
| Retired | 0.6 | 1.3 |
| Student | 0.6 | 0.6 |
| Other | 2.9 | 3.5 |
| Parent ethnicity (%) | ||
| White British | 87.4 | 85.5 |
| Other | 12.6 | 14.6 |
| Household income (%) | ||
| Less than £10,000 | 3.2 | 2.6 |
| £10,000–£19,999 | 16.1 | 21.2 |
| £20,000–£29,999 | 22.9 | 26 |
| £30,000–£39,999 | 16.8 | 18.6 |
| £40,000–£49,999 | 13.5 | 11.3 |
| £50,000–£74,999 | 17.1 | 11.9 |
| £75,000–£99,999 | 5.5 | 3.9 |
| Over £100,000 | 2.6 | 1 |
| Prefer not to say | 2.3 | 3.5 |
| Asthma | No Asthma | |
|---|---|---|
| Child age (mean, SD) | 12.89 (1.94) | 12.52 (1.94) |
| Child gender (% female) | 41.6 | 48.6 |
| Child BMI z-score (mean, SD) (n = 198 vs. 194) | 1.21 (1.25) | 0.89 (1.18) |
| Child Comorbidities (%) | 25.5 | 14.1 |
| Children with Asthma—Mean (SD) | Children without Asthma—Mean (SD) | Mann–Whitney U Test | |
|---|---|---|---|
| Parental Feeding | |||
| Child Control | 2.8 (0.71) | 2.79 (0.68) | 47,968 |
| Emotion Regulation | 2.21 (0.87) | 2.02 (0.7) | 43,273 * |
| Encourage balance and variety | 4.42 (0.57) | 4.42 (0.55) | 48,150 |
| Environment | 3.59 (0.77) | 3.65 (0.73) | 45,599 |
| Restriction for weight control | 3.08 (0.79) | 2.88 (0.79) | 41,602 ** |
| Food as a reward | 2.63 (1.1) | 2.54 (1.09) | 45,766 |
| Restriction for health | 3.55 (1.02) | 3.52 (0.72) | 47,876 |
| Teaching about nutrition | 4.53 (0.72) | 4.43 (0.81) | 45,242 |
| Parenting Practices of Child Activity | |||
| Responsibility/monitoring | 3.52 (0.82) | 3.34 (0.83) | 42,521 * |
| Pressure to exercise | 3.73 (0.85) | 3.53 (0.91) | 42,131 ** |
| Control of active behaviours | 2.35 (1.09) | 2.05 (1.03) | 40,002 ** |
| Perceptions of Child Weight | |||
| Concerns about child overweight | 2.76 (1.3) | 2.45 (1.33) | 41,697 ** |
| Perceived child overweight | 3.1 (0.58) | 3.05 (0.48) | 47,020 |
| Child Eating | |||
| Enjoyment of food | 3.84 (0.77) | 3.89 (8) | 46,243 |
| Emotional overeating | 2.47 (1.04) | 2.17 (0.82) | 40,491 ** |
| Desire to drink | 2.84 (1.08) | 2.63 (1.04) | 42,855 * |
| Food responsiveness | 2.81 (1.08) | 2.66 (1) | 44,701 |
| Child Activity | |||
| Activity Score | 65.36 (61.21) | 65.78 (59.25) | 47,785 |
| Activity frequency | 1.75 (0.66) | 1.81 (0.69) | 45,909 |
| Child BMIz Score | ||
|---|---|---|
| Children with Asthma (n = 198)—R | Children without Asthma (n = 194)—R | |
| Parental Feeding | ||
| Child Control | −0.03 | 0.12 |
| Emotion Regulation | 0.12 | 0.14 * |
| Encourage balance and variety | −0.06 | −0.16 * |
| Environment | −0.03 | −0.10 |
| Restriction for weight control | 0.16 * | 0.31 ** |
| Food as a reward | 0.08 | 0.16 * |
| Restriction for health | 0.08 | 0.24 ** |
| Teaching about nutrition | −0.13 * | −0.02 |
| Parenting Practices of Child Activity | ||
| Responsibility/monitoring | 0.01 | 0.09 |
| Pressure to exercise | 0.03 | 0.21 ** |
| Control of active behaviours | 0.06 | 0.05 |
| Perceptions of child weight | ||
| Concerns about child overweight | 0.24 ** | 0.37 ** |
| Perceived child overweight | 0.28 ** | 0.35 ** |
| Child Eating | ||
| Enjoyment of food | 0.08 | 0.05 |
| Emotional overeating | 0.19 ** | 0.29 ** |
| Desire to drink | 0.10 | 0.19 ** |
| Food responsiveness | 0.13 * | 0.30 ** |
| Child Activity | ||
| Activity Score | −0.16 * | −0.14 * |
| Activity frequency | 0.09 | 0.21 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Clarke, R.; Heath, G.; Nagakumar, P.; Pattison, H.; Farrow, C. Parental Feeding, Child Eating and Physical Activity: Differences in Children Living with and without Asthma. Int. J. Environ. Res. Public Health 2021, 18, 3452. https://doi.org/10.3390/ijerph18073452
Clarke R, Heath G, Nagakumar P, Pattison H, Farrow C. Parental Feeding, Child Eating and Physical Activity: Differences in Children Living with and without Asthma. International Journal of Environmental Research and Public Health. 2021; 18(7):3452. https://doi.org/10.3390/ijerph18073452
Chicago/Turabian StyleClarke, Rebecca, Gemma Heath, Prasad Nagakumar, Helen Pattison, and Claire Farrow. 2021. "Parental Feeding, Child Eating and Physical Activity: Differences in Children Living with and without Asthma" International Journal of Environmental Research and Public Health 18, no. 7: 3452. https://doi.org/10.3390/ijerph18073452