
Health Literacy as a Major Contributor to Health-Promoting Behaviors among Korean Teachers


Abstract
:1. Introduction
2. Methods
2.1. Data Collection and Samples
2.2. Measures
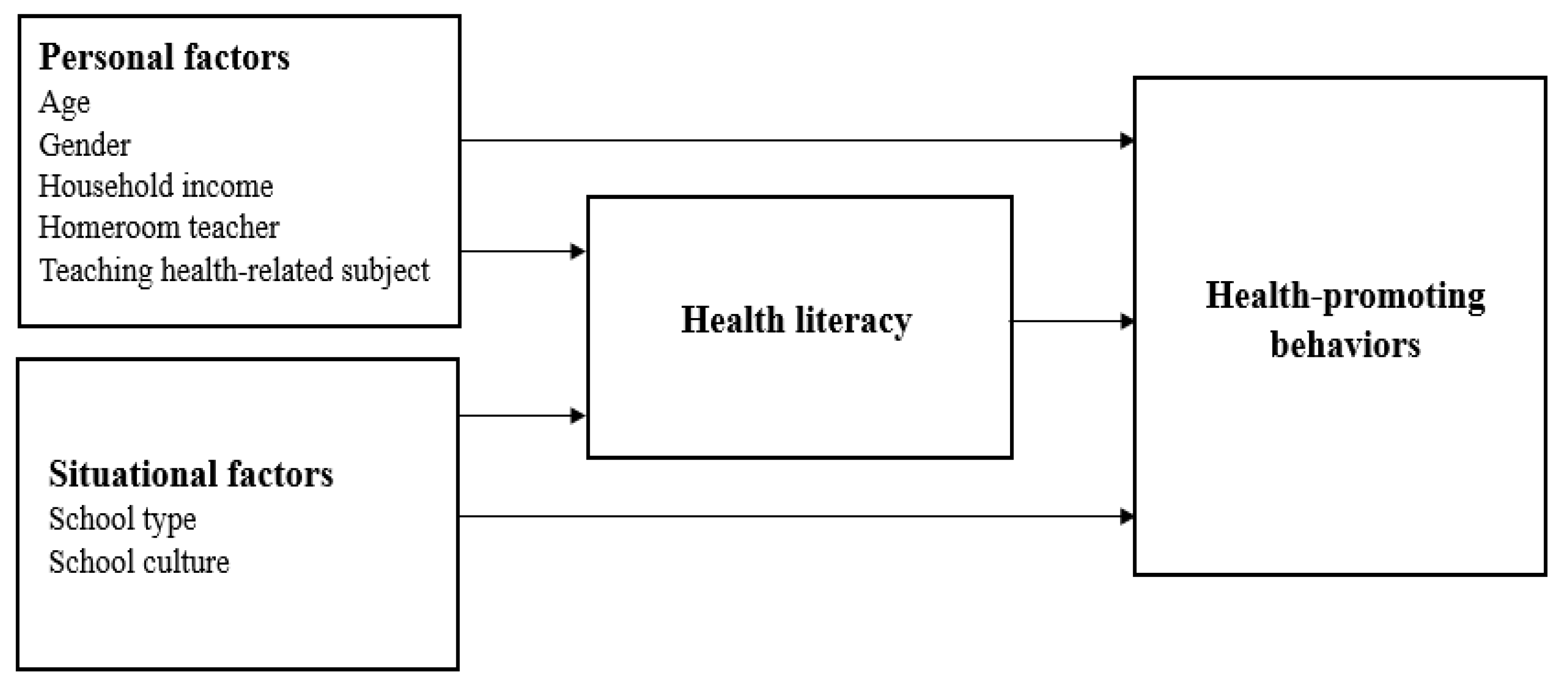
2.2.1. Personal Factors
2.2.2. Situational Factors
2.2.3. Health Literacy
2.2.4. Health-Promoting Behaviors
2.3. Data Analysis
3. Results
3.1. Sample Characteristics
3.2. Correlation of Variables
3.3. Regression Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A


Appendix B

{kind=link}
{kind=link}
{kind=link}
| Predictor | Overall 2 | Health Responsibility | Physical Activity | Nutrition | Spiritual Growth | Interpersonal Relations | Stress Management | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | p | β | p | β | p | β | p | β | p | β | p | β | p | |
| Personal factors | ||||||||||||||
| Age | −0.01 | 0.778 | −0.07 | 0.148 | 0.03 | 0.496 | 0.20 | <0.001 | −0.02 | 0.749 | −0.19 | <0.001 | −0.04 | 0.444 |
| Gender (ref. male) | −0.001 | 0.986 | 0.04 | 0.382 | −0.10 | 0.028 | 0.11 | 0.013 | −0.02 | 0.738 | 0.04 | 0.333 | −0.05 | 0.231 |
| Household income 1 | 0.04 | 0.395 | 0.01 | 0.762 | −0.03 | 0.543 | 0.06 | 0.235 | 0.06 | 0.189 | 0.08 | 0.094 | 0.01 | 0.814 |
| Teaching Health-related subject | 0.01 | 0.852 | 0.03 | 0.582 | 0.01 | 0.787 | 0.03 | 0.571 | 0.02 | 0.738 | −0.07 | 0.144 | 0.03 | 0.593 |
| Homeroom teacher | 0.03 | 0.578 | 0.01 | 0.836 | 0.07 | 0.154 | 0.03 | 0.560 | -0.01 | 0.788 | −0.01 | 0.868 | 0.03 | 0.555 |
| Situational factors | ||||||||||||||
| School type (ref. secondary school) | 0.09 | 0.057 | 0.03 | 0.452 | 0.10 | 0.044 | 0.12 | 0.010 | −0.01 | 0.864 | 0.03 | 0.540 | 0.15 | 0.001 |
| School culture | 0.11 | 0.010 | 0.05 | 0.192 | 0.05 | 0.274 | 0.05 | 0.232 | 0.08 | 0.069 | 0.16 | <0.001 | 0.13 | 0.002 |
| HC-HL | 0.40 | <0.001 | 0.43 | <0.001 | 0.22 | <0.001 | 0.30 | <0.001 | 0.29 | <0.001 | 0.36 | <0.001 | 0.30 | <0.001 |
| R2 | 0.211 | 0.219 | 0.081 | 0.185 | 0.109 | 0.230 | 0.165 | |||||||
| Adjusted R2 | 0.197 | 0.206 | 0.065 | 0.171 | 0.094 | 0.217 | 0.150 | |||||||
| F (p) | 15.55 (<0.001) | 16.31 (<0.001) | 5.13 (<0.001) | 13.20 (<0.001) | 7.11 (<0.001) | 17.39 (<0.001) | 11.45 (<0.001) | |||||||
| Predictor | Overall 2 | Health Responsibility | Physical Activity | Nutrition | Spiritual Growth | Interpersonal Relations | Stress Management | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | p | β | p | β | p | β | p | β | p | β | p | β | p | |
| Personal factors | ||||||||||||||
| Age | −0.04 | 0.357 | −0.10 | 0.024 | 0.02 | 0.630 | 0.18 | <0.001 | -0.04 | 0.466 | −0.21 | <0.001 | −0.06 | 0.213 |
| Gender (ref. male) | 0.01 | 0.781 | 0.05 | 0.222 | −0.10 | 0.036 | 0.12 | 0.006 | −0.01 | 0.886 | 0.05 | 0.204 | −0.05 | 0.310 |
| Household income 1 | 0.02 | 0.609 | 0.001 | 0.987 | −0.04 | 0.355 | 0.05 | 0.322 | 0.05 | 0.291 | 0.06 | 0.157 | −0.001 | 0.985 |
| Teaching Health-related subject | −0.003 | 0.939 | 0.02 | 0.672 | −0.001 | 0.991 | 0.02 | 0.649 | 0.01 | 0.909 | −0.08 | 0.084 | 0.02 | 0.713 |
| Homeroom teacher | 0.03 | 0.466 | 0.02 | 0.708 | 0.08 | 0.127 | 0.03 | 0.484 | −0.01 | 0.858 | −0.002 | 0.969 | 0.03 | 0.479 |
| Situational factors | ||||||||||||||
| School type (ref. secondary school) | 0.06 | 0.179 | 0.01 | 0.867 | 0.08 | 0.101 | 0.10 | 0.029 | -0.03 | 0.522 | 0.003 | 0.950 | 0.13 | 0.005 |
| School culture | 0.11 | 0.007 | 0.06 | 0.144 | 0.04 | 0.322 | 0.05 | 0.204 | 0.08 | 0.068 | 0.16 | <0.001 | 0.13 | 0.002 |
| DP-HL | 0.48 | <0.001 | 0.48 | <0.001 | 0.31 | <0.001 | 0.34 | <0.001 | 0.37 | <0.001 | 0.43 | <0.001 | 0.36 | <0.001 |
| R2 | 0.282 | 0.269 | 0.124 | 0.213 | 0.155 | 0.282 | 0.202 | |||||||
| Adjusted R2 | 0.269 | 0.257 | 0.109 | 0.199 | 0.140 | 0.270 | 0.188 | |||||||
| F (p) | 22.78 (<0.001) | 21.42 (<0.001) | 8.22 (<0.001) | 15.73 (<0.001) | 10.66 (<0.001) | 22.85 (<0.001) | 14.72 (<0.001) | |||||||
| Predictor | Overall 2 | Health Responsibility | Physical Activity | Nutrition | Spiritual Growth | Interpersonal Relations | Stress Management | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | p | β | p | β | p | β | p | β | p | β | p | β | p | |
| Personal Factors | ||||||||||||||
| Age | −0.01 | 0.775 | −0.08 | 0.081 | 0.05 | 0.262 | 0.19 | <0.001 | −0.02 | 0.743 | −0.19 | <0.001 | −0.03 | 0.529 |
| Gender (ref. male) | 0.01 | 0.878 | 0.05 | 0.263 | −0.10 | 0.022 | 0.12 | 0.008 | -0.01 | 0.816 | 0.05 | 0.240 | −0.05 | 0.239 |
| Household income 1 | 0.02 | 0.667 | 0.001 | 0.995 | −0.06 | 0.221 | 0.05 | 0.285 | 0.05 | 0.297 | 0.06 | 0.146 | −0.01 | 0.794 |
| Teaching Health-related subject | 0.05 | 0.247 | 0.074 | 0.092 | 0.03 | 0.547 | 0.06 | 0.180 | 0.05 | 0.325 | −0.28 | 0.524 | 0.05 | 0.237 |
| Homeroom teacher | 0.03 | 0.545 | 0.01 | 0.807 | 0.07 | 0.139 | 0.03 | 0.537 | −0.01 | 0.780 | −0.01 | 0.877 | 0.03 | 0.541 |
| Situational Factors | ||||||||||||||
| School type (ref. secondary school) | 0.01 | 0.736 | −0.03 | 0.464 | 0.04 | 0.413 | 0.08 | 0.094 | −0.06 | 0.194 | −0.03 | 0.492 | 0.09 | 0.052 |
| School culture | 0.10 | 0.012 | 0.05 | 0.184 | 0.03 | 0.531 | 0.05 | 0.204 | 0.07 | 0.087 | 0.15 | <0.001 | 0.12 | 0.004 |
| HP-HL | 0.54 | <0.001 | 0.51 | <0.001 | 0.42 | <0.001 | 0.33 | <0.001 | 0.40 | <0.001 | 0.44 | <0.001 | 0.46 | <0.001 |
| R2 | 0.335 | 0.295 | 0.195 | 0.206 | 0.175 | 0.292 | 0.276 | |||||||
| Adjusted R2 | 0.324 | 0.283 | 0.181 | 0.192 | 0.160 | 0.280 | 0.264 | |||||||
| F (p) | 29.30 (<0.001) | 24.31 (<0.001) | 14.10 (<0.001) | 15.068 (<0.001) | 12.30 (<0.001) | 24.02 (<0.001) | 22.182 | |||||||
References
- Pender, N.; Murdaugh, C.L.; Parsons, M.A. Health Promotion in Nursing Practice, 6th ed.; Pearson Education: Upper Saddle River, NJ, USA, 2011. [Google Scholar]
- Warburton, D.E.; Bredin, S.S. Health benefits of physical activity: A systematic review of current systematic reviews. Curr. Opin. Cardiol. 2017, 32, 541–556. [Google Scholar] [CrossRef]
- Zhang, X.; Devlin, H.M.; Smith, B.; Imperatore, G.; Thomas, W.; Lobelo, F.; Ali, M.K.; Norris, K.; Gruss, S.; Bardenheier, B.; et al. Effect of lifestyle interventions on cardiovascular risk factors among adults without impaired glucose tolerance or diabetes: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0176436. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Bogensberger, B.; Hoffmann, G. Diet quality as assessed by the healthy eating index, alternate healthy eating index, dietary approaches to stop hypertension score, and health outcomes: An updated systematic review and meta-analysis of cohort studies. J. Acad. Nutr. Diet. 2018, 118, 74–100. [Google Scholar] [CrossRef] [Green Version]
- Kyu, H.H.; Bachman, V.F.; Alexander, L.T.; Mumford, J.E.; Afshin, A.; Estep, K.; Veerman, J.L.; Delwiche, K.; Iannarone, M.L.; Moyer, M.L.; et al. Physical activity and risk of breast cancer, colon cancer, diabetes, ischemic heart disease, and ischemic stroke events: Systematic review and dose-response meta-analysis for the Global Burden of Disease Study 2013. BMJ (Clin. Res. Ed.) 2016, 354, i3857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelly, J.T.; Palmer, S.C.; Wai, S.N.; Ruospo, M.; Carrero, J.J.; Campbell, K.L.; Strippoli, G.F. Healthy dietary patterns and risk of mortality and ESRD in CKD: A meta-analysis of cohort studies. Clin. J. Am. Soc. Nephrol. 2017, 12, 272–279. [Google Scholar] [CrossRef]
- Khaw, K.T.; Wareham, N.; Bingham, S.A.; Welch, A.; Luben, R.; Day, D. Combined impact of health behaviours and mortality in men and women: The EPIC-Norfolk prospective population study. PLoS Med. 2008, 5, 39–47. [Google Scholar] [CrossRef] [Green Version]
- Mo, P.K.; Winnie, W.M. The influence of health promoting practices on the quality of life of community adults in Hong Kong. Soc. Indic. Res. 2010, 95, 503–517. [Google Scholar] [CrossRef]
- Lee, M.K.; Oh, J. health-related quality of life in older adults: Its association with health literacy, self-efficacy, social support, and health-promoting behavior. Healthc. Multidiscip. Digit. Publ. Inst. 2020, 8, 407. [Google Scholar] [CrossRef]
- Laguna, M.C.; Hecht, A.A.; Ponce, J.; Jue, T.; Brindis, C.D.; Patel, A.I. Teachers as healthy beverage role models: Relationship of student and teacher beverage choices in elementary schools. J. Community Health 2020, 45, 121–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, L.; Zhai, Y.; Engelgau, M.; Li, W.; Qian, H.; Si, X.; Gao, X.; Sereny, M.; Liang, J.; Zhu, X.; et al. Association of children’s eating behaviors with parental education, and teachers’ health awareness, attitudes and behaviors: A national school-based survey in China. Eur. J. Public Health 2014, 24, 880–887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smuka, I. Teacher role model and students’ physical activity. Pol. J. Sport Tour. 2012, 19, 281–286. [Google Scholar] [CrossRef] [Green Version]
- Lewallen, T.C.; Hunt, H.; Potts-Datema, W.; Zaza, S.; Giles, W. The whole school, whole community, whole child model: A new approach for improving educational attainment and healthy development for students. J. Sch. Health 2015, 85, 729–739. [Google Scholar] [CrossRef] [Green Version]
- Sørensen, K.; Van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H. Health literacy and public health: A systematic review and integration of definitions and models. Bmc Public Health 2012, 12, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peerson, A.; Saunders, M. Health literacy revisited: What do we mean and why does it matter? Health Promot Int. 2009, 24, 285–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suka, M.; Odajima, T.; Okamoto, M.; Sumitani, M.; Igarashi, A.; Ishikawa, H.; Kusama, M.; Yamamoto, M.; Nakayama, T.; Sugimori, H. Relationship between health literacy, health information access, health behavior, and health status in Japanese people. Patient Educ. Couns. 2015, 98, 660–668. [Google Scholar] [CrossRef] [PubMed]
- HLS-EU Consortium. Comparative Report of Health Literacy in Eight EU Member States. European Health Literacy Survey HLS-EU. 2012. Available online: http://cpme.dyndns.org:591/adopted/2015/Comparative_report_on_health_literacy_in_eight_EU_member_states.pdf (accessed on 29 November 2020).
- Levin-Zamir, D.; Baron-Epel, O.B.; Cohen, V.; Elhayany, A. The association of health literacy with health behavior, socioeconomic indicators, and self-assessed health from a national adult survey in Israel. J. Health Commun. 2016, 21 (Suppl. 2), 61–68. [Google Scholar] [CrossRef]
- Aygun, O.; Cerim, S. The relationship between general health behaviors and general health literacy levels in the Turkish population. Health Promot. Int. 2020, 1–15. [Google Scholar] [CrossRef]
- Nagler, E.M.; Sinha, D.N.; Pednekar, M.S.; Stoddard, A.M.; Gupta, P.C.; Mathur, N.; Lando, H.; Aghi, M.; Shulman Cordeira, L.; Viswanath, K.; et al. Social contextual factors and tobacco use among Indian teachers: Insights from the Bihar School Teachers’ Study. Prev. Med. 2015, 74, 24–30. [Google Scholar] [CrossRef] [Green Version]
- Park, H.; Jung, H.S.; Lee, J.H. Effects of Self-Efficacy on Health Promotion Lifestyle in Teachers. Korean Soc. Sch. Health 2009, 22, 183–191. [Google Scholar]
- Lee, J.; Lee, J. A survey on competencies of teachers of guidance using importance-performance analysis. J. Yeolin Educ. 2013, 21, 53–76. [Google Scholar]
- Lee, J.H.; Jung, H.S.; Choi, E.S. Health promotion lifestyle profile of the teachers of health-related disciplines and not-health-related disciplines in middle and high school. Korean J. Occup. Health Nurs. 2003, 12, 123–133. [Google Scholar]
- Peltzer, K.; Pengpid, S.; Yung, T.K.; Aounallah-Skhiri, H.; Rehman, R. Comparison of health risk behavior, awareness, and health benefit beliefs of health science and non-health science students: An international study. Nurs. Health Sci. 2016, 18, 180–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mikkonen, K.; Ojala, T.; Sjögren, T.; Piirainen, A.; Koskinen, C.; Koskinen, M.; Koivula, M.; Sormunen, M.; Saaranen, T.; Salminen, L.; et al. Competence areas of health science teachers–A systematic review of quantitative studies. Nurse Educ. Today 2018, 70, 77–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, E.T.; Venta, A. Lack of implementation of eating disorder education and prevention programs in high schools: Data from incoming college freshmen. Eat. Disord. 2018, 26, 430–447. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.Y.; Choi, B.Y.; Sohn, A.R.; Ahn, D.H. Evaluating of health promoting school by school characteristics. Korean Soc. Health Educ. Promot. 2009, 26, 85–96. [Google Scholar]
- Institute of Medicine. The Future of the Public’s Health in the 21st Century; National Academies Press: Washington, DC, USA, 2003. [Google Scholar]
- McNeill, L.H.; Kreuter, M.W.; Subramanian, S.V. Social environment and physical activity: A review of concepts and evidence. Soc. Sci. Med. 2006, 63, 1011–1022. [Google Scholar] [CrossRef]
- Shin, J.H.; Y, Y.; Choi, H.S. Predictive relations of teacher efficacy to school cultures. J. Child Educ. 2007, 16, 47–56. [Google Scholar]
- World Health Organization. Shanghai declaration on promoting health in the 2030 Agenda for Sustainable Development. Health Promot. Int. 2017, 32, 7–8. [Google Scholar] [CrossRef] [Green Version]
- Hong, E.; Kang, Y.S.; Ha, Y. Factors affecting on health promoting behaviors among teachers with middle-aged women experiencing menopause. Korean J. Occup. Health Nurs. 2013, 66–74. [Google Scholar] [CrossRef]
- Jung, S.H.; Kim, D.H. Health perception, health status, and health promoting behaviors of elementary school teacher. J. Korean Soc. Sch. Health 2017, 30, 355–364. [Google Scholar] [CrossRef]
- Cohen, J. Statical Power Analysis for the Behavioral Sciences, 2nd ed.; Hillsdale, N.J., Ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar]
- Soper, D. Hierarchical Multiple Regression Sample Size Calculator [Software]. 2021. Available online: https://www.danielsoper.com/statcalc (accessed on 29 November 2020).
- Roscoe, J.T. Fundamental Research Statistics for the Behavioral Sciences, 2nd ed.; Holt, Rinehart and Winston: New York, NY, USA, 1975. [Google Scholar]
- Hill, R. What sample size is “enough” in internet survey research. Interpers. Comput. Technol. Electron. J. 21st Century 1998, 6, 1–12. [Google Scholar]
- Sørensen, K.; Van den Broucke, S.; Pelikan, J.M.; Fullam, J.; Doyle, G.; Slonska, Z.; Kondilis, B.; Stoffels, V.; Osborne, R.H.; Brand, H. Measuring health literacy in populations: Illuminating the design and development process of the European Health Literacy Survey Questionnaire (HLS-EU-Q). BMC Public Health 2013, 13, 948. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.H.; Park, C.Y.; Kang, S.H. A survey on the level and related factors of health literacy in Korean people. Health Policy Manag. 2019, 29, 146–159. [Google Scholar] [CrossRef]
- Walker, S.N.; Hill-Polerecky, D.M. Psychometric Evaluation of the Health-Promoting Lifestyle Profile II; Unpublished manuscript; University of Nebraska Medical Center: Omaha, NV, USA, 1996; Volume 13, pp. 120–126. [Google Scholar]
- Yun, S.N.; Kim, J.H. Health-promoting behaviors of the women workers at the manufacturing industry - based on the Pender’s health promotion model. Korean J. Occup. Health Nurs. 1999, 8, 130–140. [Google Scholar]
- Sebert, D.M.; Montgomery, D.C.; Rollier, D.A. A clustering algorithm for identifying multiple outliers in linear regression. Comput. Stat. Data Anal. 1998, 27, 461–484. [Google Scholar] [CrossRef]
- Montgomery, D.C.; Peck, E.A.; Vining, G.G. Introduction to Linear Regression Analysis, 5th ed.; John Wiley & Sons: Hoboken, NJ, USA, 2012. [Google Scholar]
- Petrocelli, J.V. Hierarchical multiple regression in counseling research: Common problems and possible remedies. Meas. Eval. Couns. Dev. 2003, 36, 9–22. [Google Scholar] [CrossRef]
- Hickey, G.L.; Kontopantelis, E.; Takkenberg, J.J.; Beyersdorf, F. Statistical primer: Checking model assumptions with regression diagnostics. Interact. Cardiovasc. Thorac. Surg. 2019, 28, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Dobbins, M.; Husson, H.; DeCorby, K.; LaRocca, R.L. School-based physical activity programs for promoting physical activity and fitness in children and adolescents aged 6 to 18. Cochrane Database Syst. Rev. 2013, 2, CD007651. [Google Scholar] [CrossRef]
- Woynarowska-Sołdan, M. Implementation trial of school staff health promotion: Polish experiences. Health Promot. Int. 2019, 34, e47–e58. [Google Scholar] [CrossRef]
- Shepherd, J.; Dewhirst, S.; Pickett, K.; Byrne, J.; Speller, V.; Grace, M.; Almond, P.; Hartwell, D.; Roderick, P. Factors facilitating and constraining the delivery of effective teacher training to promote health and well-being in schools: A survey of current practice and systematic review. J. Public Health Res. 2013, 1. [Google Scholar] [CrossRef] [Green Version]
- Rueda-Medina, B.; Gómez-Urquiza, J.L.; Tapia-Haro, R.; Casas-Barragán, A.; Aguilar-Ferrándiz, M.E.; Correa-Rodríguez, M. Assessing health science students’ health literacy and its association with health behaviours. Health Soc. Care Community 2020, 28, 2134–2139. [Google Scholar] [CrossRef] [PubMed]
- de Buhr, E.; Ewers, M.; Tannen, A. Potentials of school nursing for strengthening the health literacy of children, parents and teachers. Int. J. Environ. Res. Public Health 2020, 17, 2577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenglass, E.R. The contribution of social support to coping strategies. Appl. Psychol. 1993, 42, 323–340. [Google Scholar] [CrossRef]
- Leung, S.S.; Wah Mak, Y.; Yu Chui, Y.; Chiang, V.C.; Lee, A.C. Occupational stress, mental health status and stress management behaviors among secondary school teachers in Hong Kong. Health Educ. J. 2009, 68, 328–343. [Google Scholar] [CrossRef]
- Lee, H.H.; Heo, J.; Kim, J.M.; Jung, B.W.; Oh, S.A. A Study on the Actual Condition of Teacher Job Stress and Management Plan; Korean Educational Development Institute: Jinchon, Korea, 2017; Available online: https://www.kedi.re.kr/khome/main/research/selectPubForm.do?plNum0=11617 (accessed on 29 November 2020).

| Variables | Category | N (%) or M ± SD |
|---|---|---|
| Gender | Male | 103 (21.7) |
| Female | 371 (78.3) | |
| Age | 42.63 ± 9.24 | |
| ≤30 | 53 (11.2) | |
| 31–40 | 148 (31.2) | |
| 41–50 | 158 (33.3) | |
| ≥51 | 115 (24.3) | |
| Household income (monthly, 10,000 KRW) | 668.82 ± 323.69 | |
| ≤ 50 | 82 (17.3) | |
| 360–500 | 112 (23.6) | |
| 510–700 | 107 (22.6) | |
| 710–900 | 75 (15.8) | |
| ≥910 | 98 (20.7) | |
| Health-related subject teacher | Yes | 93 (19.6) |
| No | 381 (80.4) | |
| Homeroom teacher | Yes | 246 (51.9) |
| No | 228 (48.1) | |
| School type | Primary school | 200 (42.2) |
| Secondary school | 274 (57.8) | |
| School culture (20–100) | 70.33 ± 10.75 | |
| General health literacy (index, 0–50) | 31.00 ± 7.59 | |
| Healthcare health literacy (index, 0–50) | 30.87 ± 7.87 | |
| Disease prevention health literacy (index, 0–50) | 31.44 ± 8.26 | |
| Health promotion health literacy (index, 0–50) | 30.40 ± 8.78 | |
| Health-promoting behaviors (52–208) | 130.73 ± 22.81 | |
| Overall (1–4) | 2.51 ± 0.43 | |
| Health responsibility (1–4) | 2.27 ± 0.51 | |
| Physical activity (1–4) | 2.22 ± 0.71 | |
| Nutrition (1–4) | 2.57 ± 0.52 | |
| Spiritual growth (1–4) | 2.74 ± 0.59 | |
| Interpersonal relations (1–4) | 2.79 ± 0.52 | |
| Stress management (1–4) | 2.45 ± 0.52 |
| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|
| 1. Gender | - | ||||||||
| 2. Age | −0.02 | - | |||||||
| 3. Household income | 0.15 | 0.29 | - | ||||||
| 4. Teaching health-related subject | 0.07 | 0.15 | 0.05 | - | |||||
| 5. Homeroom teacher | −0.02 | −0.25 | −0.06 | −0.41 | - | ||||
| 6. School type | 0.30 | −0.07 | 0.11 | 0.08 | 0.19 | - | |||
| 7. School culture | −0.08 | 0.05 | −0.04 | 0.01 | 0.04 | 0.06 | - | ||
| 8. Health literacy | 0.07 | −0.09 | 0.12 | 0.16 | 0.004 | 0.18 | 0.17 | - | |
| 9. Health-promoting behaviors | 0.05 | −0.06 | 0.09 | 0.07 | 0.05 | 0.15 | 0.18 | 0.54 | - |
| Predictor | Model 1 | Model 2 | Model 3 | Model 3(a) | Model 3(b) | Model 3(c) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | p | β | p | β | p | β | p | β | p | β | p | |
| Personal factors | ||||||||||||
| Age | −0.09 | 0.071 | −0.10 | 0.056 | −0.01 | 0.835 | −0.01 | 0.788 | −0.04 | 0.357 | −0.01 | 0.775 |
| Gender (ref. male) | 0.03 | 0.565 | 0.01 | 0.788 | 0.004 | 0.917 | −0.001 | 0.986 | 0.01 | 0.781 | 0.01 | 0.878 |
| Household income 1 | 0.10 | 0.039 | 0.09 | 0.073 | 0.02 | 0.731 | 0.04 | 0.395 | 0.02 | 0.609 | 0.02 | 0.667 |
| Teaching health-related subject | 0.11 | 0.024 | 0.09 | 0.080 | −0.004 | 0.933 | 0.01 | 0.852 | −0.003 | 0.939 | 0.05 | 0.247 |
| Homeroom teacher | 0.08 | 0.130 | 0.04 | 0.481 | 0.03 | 0.535 | 0.03 | 0.578 | 0.03 | 0.466 | 0.03 | 0.545 |
| Situational factors | ||||||||||||
| School type(ref. secondary school) | 0.11 | 0.027 | 0.05 | 0.250 | 0.09 | 0.057 | 0.06 | 0.179 | 0.01 | 0.736 | ||
| School culture | 0.18 | <0.001 | 0.09 | 0.021 | 0.11 | 0.010 | 0.11 | 0.007 | 0.10 | 0.012 | ||
| Health literacy | ||||||||||||
| General HL | 0.52 | <0.001 | ||||||||||
| HC-HL | 0.40 | <0.001 | ||||||||||
| DP-HL | 0.48 | <0.001 | ||||||||||
| HP-HL | 0.54 | <0.001 | ||||||||||
| R2 | 0.026 | 0.070 | 0.308 | 0.211 | 0.282 | 0.335 | ||||||
| Adjusted R2 | 0.016 | 0.056 | 0.296 | 0.197 | 0.269 | 0.324 | ||||||
| F (p) | 2.49 (0.030) | 4.99 (<0.001) | 25.89 (<0.001) | 15.55 (<0.001) | 22.78 (<0.001) | 29.30 (<0.001) | ||||||
| Δ R2 | 0.026 | 0.044 | 0.238 | 0.141 | 0.212 | 0.265 | ||||||
| Predictor | Overall 2 | Health Responsibility | Physical Activity | Nutrition | Spiritual Growth | Interpersonal Relations | Stress Management | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | p | β | p | β | p | β | p | β | p | β | p | β | p | |
| Personal factors | ||||||||||||||
| Age | −0.01 | 0.835 | −0.07 | 0.118 | 0.05 | 0.354 | 0.20 | <0.001 | −0.01 | 0.801 | −0.19 | <0.001 | −0.03 | 0.492 |
| Gender (ref. male) | 0.004 | 0.917 | 0.04 | 0.286 | −0.10 | 0.026 | 0.12 | 0.009 | −0.01 | 0.791 | 0.05 | 0.259 | −0.05 | 0.244 |
| Household income 1 | 0.02 | 0.731 | −0.01 | 0.868 | −0.05 | 0.290 | 0.04 | 0.366 | 0.05 | 0.336 | 0.06 | 0.194 | −0.01 | 0.844 |
| Teaching Health-related subject | −0.004 | 0.933 | 0.02 | 0.675 | −0.002 | 0.965 | 0.02 | 0.624 | 0.01 | 0.890 | −0.08 | 0.085 | 0.01 | 0.759 |
| Homeroom teacher | 0.03 | 0.535 | 0.01 | 0.795 | 0.07 | 0.142 | 0.03 | 0.532 | −0.01 | 0.793 | −0.01 | 0.885 | 0.03 | 0.530 |
| Situational factors | ||||||||||||||
| School type (ref. secondary school) | 0.05 | 0.250 | −0.002 | 0.959 | 0.07 | 0.131 | 0.10 | 0.039 | −0.04 | 0.438 | −0.01 | 0.915 | 0.12 | 0.008 |
| School culture | 0.09 | 0.021 | 0.04 | 0.296 | 0.03 | 0.475 | 0.04 | 0.308 | 0.07 | 0.119 | 0.14 | <0.001 | 0.12 | 0.005 |
| General HL | 0.52 | <0.001 | 0.52 | <0.001 | 0.34 | <0.001 | 0.36 | <0.001 | 0.39 | <0.001 | 0.45 | <0.001 | 0.40 | <0.001 |
| R2 | 0.308 | 0.298 | 0.140 | 0.220 | 0.165 | 0.297 | 0.228 | |||||||
| Adjusted R2 | 0.296 | 0.285 | 0.125 | 0.207 | 0.151 | 0.284 | 0.215 | |||||||
| F (p) | 25.89 (<0.001) | 24.62 (<0.001) | 9.44 (<0.001) | 16.42 (<0.001) | 11.49 (<0.001) | 24.50 (<0.001) | 17.21 (<0.001) | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bae, E.J.; Yoon, J.Y. Health Literacy as a Major Contributor to Health-Promoting Behaviors among Korean Teachers. Int. J. Environ. Res. Public Health 2021, 18, 3304. https://doi.org/10.3390/ijerph18063304
Bae EJ, Yoon JY. Health Literacy as a Major Contributor to Health-Promoting Behaviors among Korean Teachers. International Journal of Environmental Research and Public Health. 2021; 18(6):3304. https://doi.org/10.3390/ijerph18063304
Chicago/Turabian StyleBae, Eun Jung, and Ju Young Yoon. 2021. "Health Literacy as a Major Contributor to Health-Promoting Behaviors among Korean Teachers" International Journal of Environmental Research and Public Health 18, no. 6: 3304. https://doi.org/10.3390/ijerph18063304