
Depressive Symptoms and Healthy Behavior Frequency in Polish Postmenopausal Women from Urban and Rural Areas

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Group
2.2. Severity of Depressive Symptoms
2.3. Healthy Behavior Frequency
2.4. Statistical Methods
- Pearson’s chi-square test to compare the categorical variables between rural and urban women;
- Student’s t-test was used to compare continuous variables between rural and urban women, and to compare the severity of depressive symptoms and healthy behavior frequency, and to distinguish between the two categories of marital status and between the two categories of education level in urban women;
- F test of analysis of variance to compare the severity of depressive symptoms and healthy behavior frequency between the three categories of the level of education in rural women;
- Pearson’s correlation coefficient r to correlate the severity of depression and healthy behavior frequency with continuous characteristics.
3. Results
3.1. General Characteristics of Rural and Urban Women
3.2. Severity of Deprresive Symtoms—Comparison between Rural and Urban Women
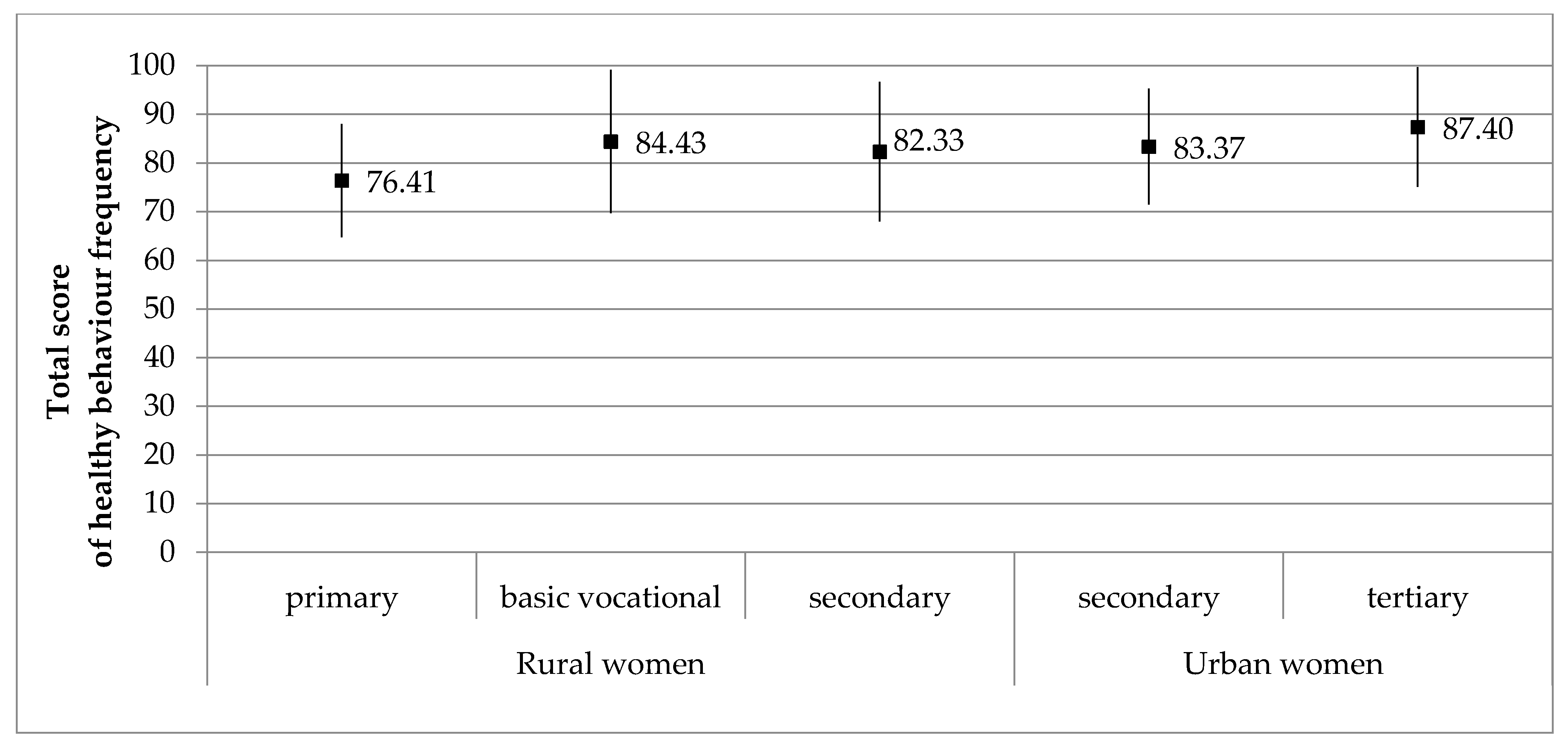
3.3. Comparison of Health Behavior Frequency in Rural and Urban Women
3.4. Correlation between Severity of Depressive Symptoms and Healthy Behavior Frequency in Rural and Urban Women
- healthy behavior frequency, especially psychological attitudes in both rural and urban women;
- frequency of recommended nutritional habits and health practices only in urban women, but not in rural ones (Table 6).
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Harlow, S.D.; Gass, M.; Hall, J.E.; Lobo, R.; Maki, P.; Rebar, R.W.; Sherman, S.; Sluss, P.M.; de Villiers, T.J. STRAW + 10 Collaborative Group. Executive summary of the Stages of Reproductive Aging Workshop + 10: Addressing the unfinished agenda of staging reproductive aging. Fertil Steril. 2012, 97, 843–851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneider, H.P.G.; Birkhäuser, M. Quality of life in climacteric women. Climacteric 2017, 20, 187–194. [Google Scholar] [CrossRef]
- Tang, R.; Luo, M.; Li, J.; Peng, Y.; Wang, Y.; Liu, B.; Liu, G.; Wang, Y.; Lin, S.; Chen, R. Symptoms of anxiety and depression among Chinese women transitioning through menopause: Findings from a prospective community-based cohort study. Fertil Steril. 2019, 112, 1160–1171. [Google Scholar] [CrossRef]
- Zimny, M.; Starczewska, M.; Szkup, M.; Karakiewicz-Krawczyk, K.; Grochans, E.; Sipak-Szmigiel, O. Analysis of the Impact of Type 2 Diabetes on the Psychosocial Functioning and Quality of Life of Perimenopausal Women. Int. J. Environ. Res. Public Health 2020, 17, 4349. [Google Scholar] [CrossRef]
- Azizi, M.; Fooladi, E.; Masoumi, M.; Orimi, T.G.; Elyasi, F.; Davis, S.R. Depressive symptoms and their risk factors in midlife women in the Middle East: A systematic review. Climacteric 2018, 21, 13–21. [Google Scholar] [CrossRef]
- Sassarini, D.J. Depression in midlife women. Maturitas 2016, 94, 149–154. [Google Scholar] [CrossRef] [Green Version]
- Mauas, V.; Kopala-Sibley, D.C.; Zuroff, D.C. Depressive symptoms in the transition to menopause: The roles of irritability, personality vulnerability, and self-regulation. Arch. Womens Ment. Health 2014, 17, 279–289. [Google Scholar] [CrossRef] [PubMed]
- Timur, S.; Sahin, N.H. The prevalence of depression symptoms and influencing factors among perimenopausal and postmenopausal women. Menopause 2010, 17, 545–551. [Google Scholar] [CrossRef]
- Colvin, A.; Richardson, G.A.; Cyranowski, J.M.; Youk, A.; Bromberger, J.T. The role of family history of depression and menopausal transition in the development of major depression in midlife women: Study of women’s health across the nation Mental Health study (SWAN MHS). Depress Anxiety 2017, 34, 826–835. [Google Scholar] [CrossRef] [PubMed]
- Lipińska-Szałek, A.; Sobczuk, A.; Pertyński, T.; Stetkiewicz, T.; Szymczak, W. Biological and psychosocial factors influence on psychical issues of perimenopause. Przegląd Menopauzalny 2003, 2, 55–56. [Google Scholar]
- Zalewska-Juzka, A.; Częstochowska, E. Depresja w okresie okołomenopauzalnym. Pol. Merk. Lek. 2003, 14, 261–264. [Google Scholar]
- Bielawska-Batorowicz, E. Menopausal symptoms in women and men aged 45–55. Przegląd Menopauzalny 2005, 1, 53–60. [Google Scholar]
- Makara-Studzińska, M.; Wdowiak, A.; Bakalczuk, G.; Bakalczuk, S. The effect of hormone therapy on the level of depression and quality of life in women in perimenopausal age, living in the countryside. Przegląd Menopauzalny 2009, 5, 284–289. [Google Scholar]
- Bromberger, J.T.; Epperson, C.N. Depression During and After the Perimenopause: Impact of Hormones, Genetics, and Environmental Determinants of Disease. Obstet Gynecol. Clin. N. Am. 2018, 45, 663–678. [Google Scholar] [CrossRef] [PubMed]
- Worsley, R.; Bell, R.; Kulkarni, J.; Davis, S.R. The association between vasomotor symptoms and depression during perimenopause: A systematic review. Maturitas 2014, 77, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Ensan, A.; Babazadeh, R.; Aghamohammadian, H.; Afzal Aghaei, M. Effect of Training Based on Choice Theory on Health-Promoting Lifestyle Behaviors among Menopausal Women. J. Midwifery Reprod. Health 2018, 6, 1253–1263. [Google Scholar] [CrossRef]
- Godycki-Cwirko, M.; Panasiuk, L.; Brotons, C.; Bulc, M.; Zakowska, I. Perception of preventive care and readiness for lifestyle change in rural and urban patients in Poland: A questionnaire study. Ann. Agric. Environ. Med. 2017, 24, 732–738. [Google Scholar] [CrossRef]
- Barros, M.B.A.; Lima, M.G.; Azevedo, R.C.S.; Medina, L.B.P.; Lopes, C.S.; Menezes, P.R.; Malta, D.C. Depression and health behaviors in Brazilian adults—PNS 2013. Rev. Saude Publica 2017, 51 (Suppl. 1), 8s. [Google Scholar] [CrossRef] [Green Version]
- Peltzer, K.; Pengpid, S. High prevalence of depressive symptoms in a national sample of adults in Indonesia: Childhood adversity, sociodemographic factors, and health risk behaviour. Asian J. Psychiatry 2018, 33, 52–59. [Google Scholar] [CrossRef]
- Pilewska-Kozak, A.B.; Dobrowolska, B.; Stadnicka, G.; Drop, B.; Jędrych, M. Place of residence and age as variables differentiating health behaviours and perception of health by women past menopause. Ann. Agric. Environ. Med. 2019, 26, 165–173. [Google Scholar] [CrossRef]
- Rural, Regional and Remote Health: Mortality Trends -2003; Australian Institute of Health and Welfare: Canberra, Australia, 2006. Available online: https://lccn.loc.gov/2006462132 (accessed on 4 December 2020).
- Kaczmarek, M.; Pacholska-Bogalska, J.; Kwaśniewski, W.; Kotarski, J.; Halerz-Nowakowska, B.; Goździcka-Józefiak, A. The association between socioeconomic status and health-related quality of life among Polish postmenopausal women from urban and rural communities. Homo 2017, 68, 42–50. [Google Scholar] [CrossRef]
- Bojar, I.; Raczkiewicz, D.; Sarecka-Hujar, B. Depression, Metabolic Syndrome, Serum TSH, and Vitamin D Concentrations in Rural and Urban Postmenopausal Women. Medicina 2020, 56, 511. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A.; Ball, R.; Ranieri, W.F. Comparison of Beck Depression Inventories -IA and -II in psychiatric outpatients. J. Pers. Assess 1996, 67, 588–797. [Google Scholar] [CrossRef]
- Juczyński, Z. Measurement Tools in Health Promotion and Psychology; Psychological Test Laboratory: Warsaw, Poland, 2001; pp. 110–116. [Google Scholar]
- Soares, C.N. Depression and Menopause: Current Knowledge and Clinical Recommendations for a Critical Window. Psychiatr. Clin. N. Am. 2017, 40, 239–254. [Google Scholar] [CrossRef]
- Malacara, J.M.; Canto de Cetina, T.; Bassol, S.; González, N.; Cacique, L.; Vera-Ramírez, M.L.; Nava, L.E. Symptoms at pre- and postmenopause in rural and urban women from three States of Mexico. Maturitas 2002, 43, 11–19. [Google Scholar] [CrossRef]
- Żołnierczuk-Kieliszek, D.; Kulik, T.B.; Jarosz, M.J.; Stefanowicz, A.; Pacian, A.; Pacian, J.; Janiszewska, M. Quality of life in peri- and post-menopausal Polish women living in Lublin Province--differences between urban and rural dwellers. Ann. Agric. Environ. Med. 2012, 19, 129–133. [Google Scholar]
- Onya, O.N.; Otorkpa, C. Biological and Environmental Correlates of Post-Menopausal Depression Among Gopd Attendees in Fmc, Lokoja, Nigeria. West Afr. J. Med. 2018, 35, 153–157. [Google Scholar]
- Deveci, S.E.; Açik, Y.; Dag, D.G.; Tokdemir, M.; Gündoğdu, C. The frequency of depression and menopause-related symptoms in postmenopausal women living in a province in Eastern Turkey, and the factors that affect depressive status. Med. Sci. Monit. 2010, 16, PH40–PH47. [Google Scholar]
- Pérez-López, F.R.; Pérez-Roncero, G.; Fernández-Iñarrea, J.; Fernández-Alonso, A.M.; Chedraui, P.; Llaneza, P. MARIA (MenopAuse RIsk Assessment) Research Group. Resilience, depressed mood, and menopausal symptoms in postmenopausal women. Menopause 2014, 21, 159–164. [Google Scholar] [CrossRef]
- Unsal, A.; Tozun, M.; Ayranci, U. Prevalence of depression among postmenopausal women and related characteristics. Climacteric 2011, 14, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.L.; Booth-LaForce, C.; Tang, S.M.; Wu, W.R.; Chen, C.H. Depressive symptoms in Taiwanese women during the peri- and post-menopause years: Associations with demographic, health, and psychosocial characteristics. Maturitas 2013, 75, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Barnaś, E.; Krupińska, A.; Kraśnianin, E.; Raś, R. Psychosocial and occupational functioning of women in menopause. Menopause Rev./Przegląd Menopauzalny 2012, 11, 296–304. [Google Scholar] [CrossRef]
- Bromberger, J.T.; Schott, L.L.; Matthews, K.A.; Kravitz, H.M.; Harlow, S.D.; Montez, J.K. Childhood socioeconomic circumstances and depressive symptom burden across 15 years of follow-up during midlife: Study of Women’s Health Across the Nation (SWAN). Arch. Womens Ment. Health 2017, 20, 495–504. [Google Scholar] [CrossRef]
- Mitchell, E.S.; Woods, N.F. Depressed mood during the menopausal transition: Is it reproductive aging or is it life? Womens Midlife Health 2017, 3, 11. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Zhao, X.; Leonhart, R.; Nadig, M.; Wang, J.; Zhao, Y.; Wirsching, M.; Fritzsche, K. A Cross-Cultural Comparison of Climacteric Symptoms, Health-Seeking Behavior, and Attitudes towards Menopause Among Mosuo Women and Han Chinese Women in Yunnan, China. Transcult Psychiatry 2019, 56, 287–301. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.J.; Shin, A.; Kang, D. Menarche age, menopause age and other reproductive factors in association with post-menopausal onset depression: Results from Health Examinees Study (HEXA). J. Affect. Disord. 2015, 187, 127–135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Uffelen, J.G.; van Gellecum, Y.R.; Burton, N.W.; Peeters, G.; Heesch, K.C.; Brown, W.J. Sitting-time, physical activity, and depressive symptoms in mid-aged women. Am. J. Prev. Med. 2013, 45, 276–281. [Google Scholar] [CrossRef] [Green Version]
- Hickey, M.; Schoenaker, D.A.; Joffe, H.; Mishra, G.D. Depressive symptoms across the menopause transition: Findings from a large population-based cohort study. Menopause 2016, 23, 1287–1293. [Google Scholar] [CrossRef]
- Amore, M.; Di Donato, P.; Papalini, A.; Berti, A.; Palareti, A.; Ferrari, G.; Chirico, C.; De Aloysio, D. Psychological status at the menopausal transition: An Italian epidemiological study. Maturitas 2004, 48, 115–124. [Google Scholar] [CrossRef]


{kind=link}
| Variable, Parameter | Rural Women (n = 239) | Urban Women (n = 157) | Comparison between Rural and Urban Women | |
|---|---|---|---|---|
| Test 1 | p | |||
| Age (years), M ± SD | 56.82 ± 4.40 | 56.38 ± 3.34 | 1.072 | 0.285 |
| Age at last menstruation (years), M ± SD | 48.95 ± 4.22 | 50.27 ± 4.08 | −3.016 | 0.003 |
| BMI (kg/m2), M ± SD | 28.83 ± 5.01 | 26.36 ± 4.36 | 5.045 | <0.001 |
| normal weight | 56 (23.43) | 65 (41.40) | 21.271 | <0.001 |
| overweight | 96 (40.17) | 64 (40.76) | ||
| obesity | 87 (36.40) | 28 (17.83) | ||
| Level of education, n (%) | ||||
| primary | 27 (11.29) | 1 (0.64) | 168.621 | <0.001 |
| basic vocational | 104 (43.51) | 5 (3.18) | ||
| secondary | 97 (40.59) | 65 (41.40) | ||
| tertiary | 11 (4.60) | 86 (54.78) | ||
| Marital status, n (%) | ||||
| married | 204 (85.36) | 128 (81.53) | 24.504 | <0.001 |
| never married | 3 (1.26) | 7 (4.46) | ||
| divorced | 4 (1.67) | 16 (10.19) | ||
| widowed | 28 (11.72) | 6 (3.82) | ||
| Having children, n (%) | 228 (95.40) | 144 (91.72) | 2.251 | 0.134 |
| Depressive Symptoms | Rural Women (n = 239) | Urban Women (n = 157) | Comparison between Rural and Urban Women | |
|---|---|---|---|---|
| t or Chi-Square Test 1 | p | |||
| Total score, M ± SD | 11.82 ± 8.43 | 10.29 ± 7.07 | 1.879 | 0.061 |
| lack or minimal, n (%) | 110 (46.03) | 88 (56.05) | 6.013 | 0.049 |
| moderate, n (%) | 118 (49.37) | 67 (42.68) | ||
| severe, n (%) | 11 (4.60) | 2 (1.27) | ||
| Variable | Severity of Depressive Symptoms in Rural Women (n = 239) | Severity of Depressive Symptoms in Urban Women (n = 157) | ||||
|---|---|---|---|---|---|---|
| Test | p | Test | p | |||
| Age (years) | r | −0.034 | 0.600 | r | −0.174 | 0.029 |
| Age at last menstruation (years) | r | −0.046 | 0.491 | r | −0.103 | 0.207 |
| BMI (kg/m2) | r | −0.002 | 0.976 | r | 0.106 | 0.186 |
| Level of education | F (primary, basic vocational or secondary) | 0.994 | 0.372 | t (secondary vs. tertiary) | −0.357 | 0.721 |
| Marital status | t (married vs. widowed) | −0.076 | 0.939 | NA | ||
| Healthy Behavior Frequency | Rural Women (n = 239) | Urban Women (n = 157) | Comparison between Rural and Urban Women | |
|---|---|---|---|---|
| t or Chi-Square Test | p | |||
| Total score, M ± SD | 82.46 ± 14.42 | 85.62 ± 12.13 | −2.268 | 0.024 |
| low, n (%) | 88 (36.82) | 38 (24.20) | 7.062 | 0.029 |
| average, n (%) | 88 (36.82) | 67 (42.68) | ||
| high, n (%) | 63 (26.36) | 52 (33.12) | ||
| Recommended nutritional habits, M ± SD | 3.31 ± 0.73 | 3.51 ± 0.73 | −2.697 | 0.007 |
| Preventive behaviors, M ± SD | 3.63 ± 0.74 | 3.76 ± 0.69 | −1.772 | 0.077 |
| Psychological attitudes, M ± SD | 3.55 ± 0.72 | 3.65 ± 0.67 | −1.481 | 0.139 |
| Health practices, M ± SD | 3.25 ± 0.74 | 3.34 ± 0.58 | −1.244 | 0.214 |
| Variable | Total Score of Healthy Behavior Frequency in Rural Women (n = 239) | Total Score of Healthy Behavior Frequency in Urban Women (n = 157) | ||||
|---|---|---|---|---|---|---|
| test | p | test | p | |||
| Age (years) | r | −0.169 | 0.009 | r | 0.166 | 0.038 |
| Age at last menstruation (years) | r | 0.039 | 0.568 | r | 0.154 | 0.058 |
| BMI (kg/m2) | r | 0.020 | 0.765 | r | −0.073 | 0.366 |
| Level of education | F (primary, basic, vocational or secondary) | 3.436 | 0.034 | t (secondary vs. tertiary) | −2.018 | 0.045 |
| Marital status | t (married vs. widowed) | 0.731 | 0.465 | NA | ||
| Covariate | Severity of Depressive Symptoms in Rural Women (n = 239) | Severity of Depressive Symptoms in Urban Women (n = 157) | ||||||
|---|---|---|---|---|---|---|---|---|
| Univariate Models | Multivariate Model | Univariate Models | Multivariate Model | |||||
| b | p | b | p | b | p | b | p | |
| Total score of healthy behavior frequency | −1.89 | 0.038 | NA | - | −5.10 | <0.001 | NA | - |
| Recommended nutritional habits | −0.96 | 0.205 | −0.02 | 0.988 | −2.91 | <0.001 | −0.98 | 0.221 |
| Preventive behaviors | −0.95 | 0.202 | 1.02 | 0.341 | −1.03 | 0.208 | 2.36 | 0.007 |
| Psychological attitudes | −2.54 | 0.001 | −3.58 | 0.001 | −4.92 | <0.001 | −5.34 | <0.001 |
| Health practices | −0.70 | 0.346 | 0.66 | 0.473 | −2.83 | 0.004 | −0.91 | 0.357 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gujski, M.; Raczkiewicz, D.; Humeniuk, E.; Sarecka-Hujar, B.; Wdowiak, A.; Bojar, I. Depressive Symptoms and Healthy Behavior Frequency in Polish Postmenopausal Women from Urban and Rural Areas. Int. J. Environ. Res. Public Health 2021, 18, 2967. https://doi.org/10.3390/ijerph18062967
Gujski M, Raczkiewicz D, Humeniuk E, Sarecka-Hujar B, Wdowiak A, Bojar I. Depressive Symptoms and Healthy Behavior Frequency in Polish Postmenopausal Women from Urban and Rural Areas. International Journal of Environmental Research and Public Health. 2021; 18(6):2967. https://doi.org/10.3390/ijerph18062967
Chicago/Turabian StyleGujski, Mariusz, Dorota Raczkiewicz, Ewa Humeniuk, Beata Sarecka-Hujar, Artur Wdowiak, and Iwona Bojar. 2021. "Depressive Symptoms and Healthy Behavior Frequency in Polish Postmenopausal Women from Urban and Rural Areas" International Journal of Environmental Research and Public Health 18, no. 6: 2967. https://doi.org/10.3390/ijerph18062967