
Winter Air Pollution from Domestic Coal Fired Heating in Ulaanbaatar, Mongolia, Is Strongly Associated with a Major Seasonal Cyclic Decrease in Successful Fecundity

Abstract
:1. Introduction
2. Materials and Methods
3. Results
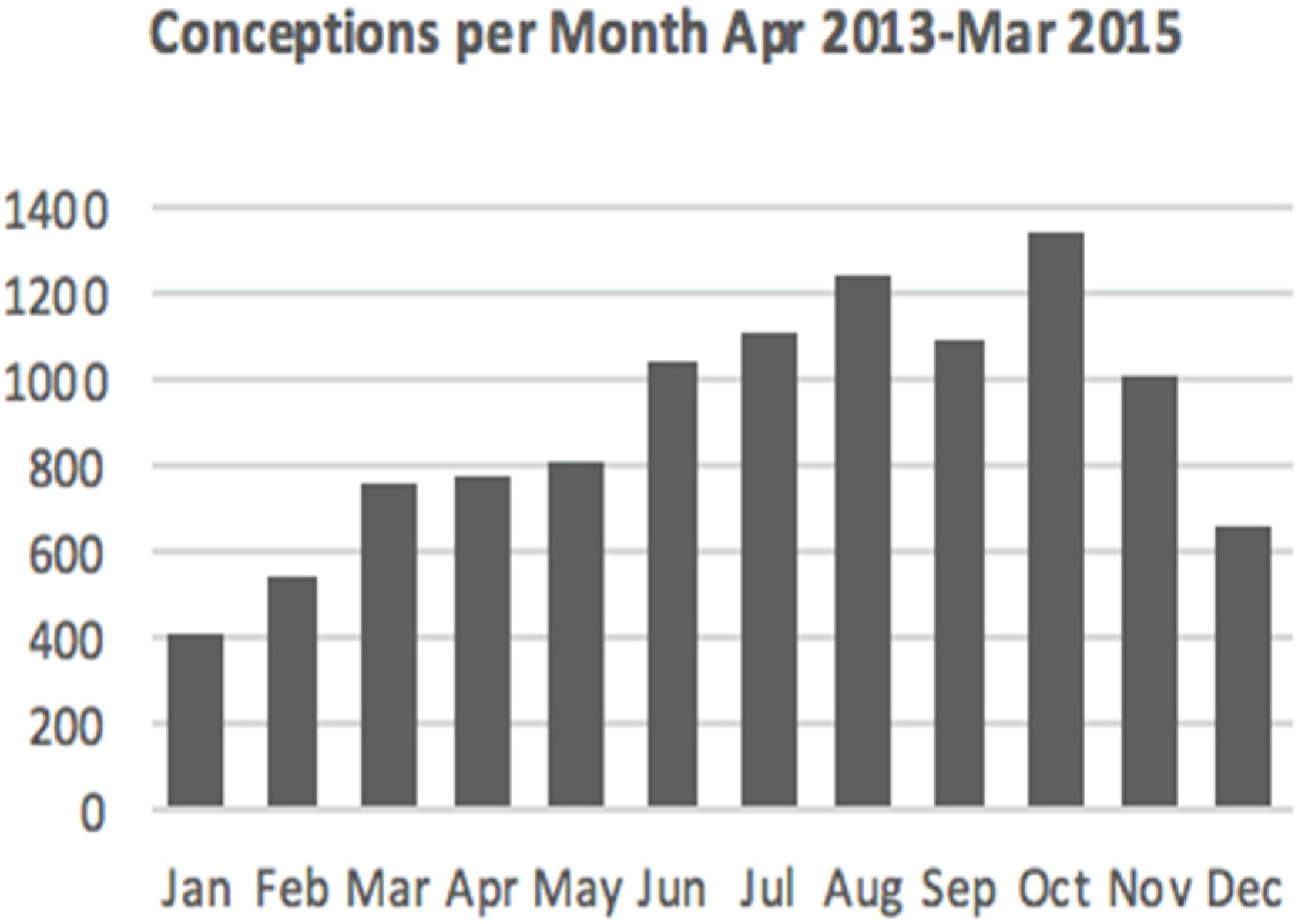
3.1. Birth Data
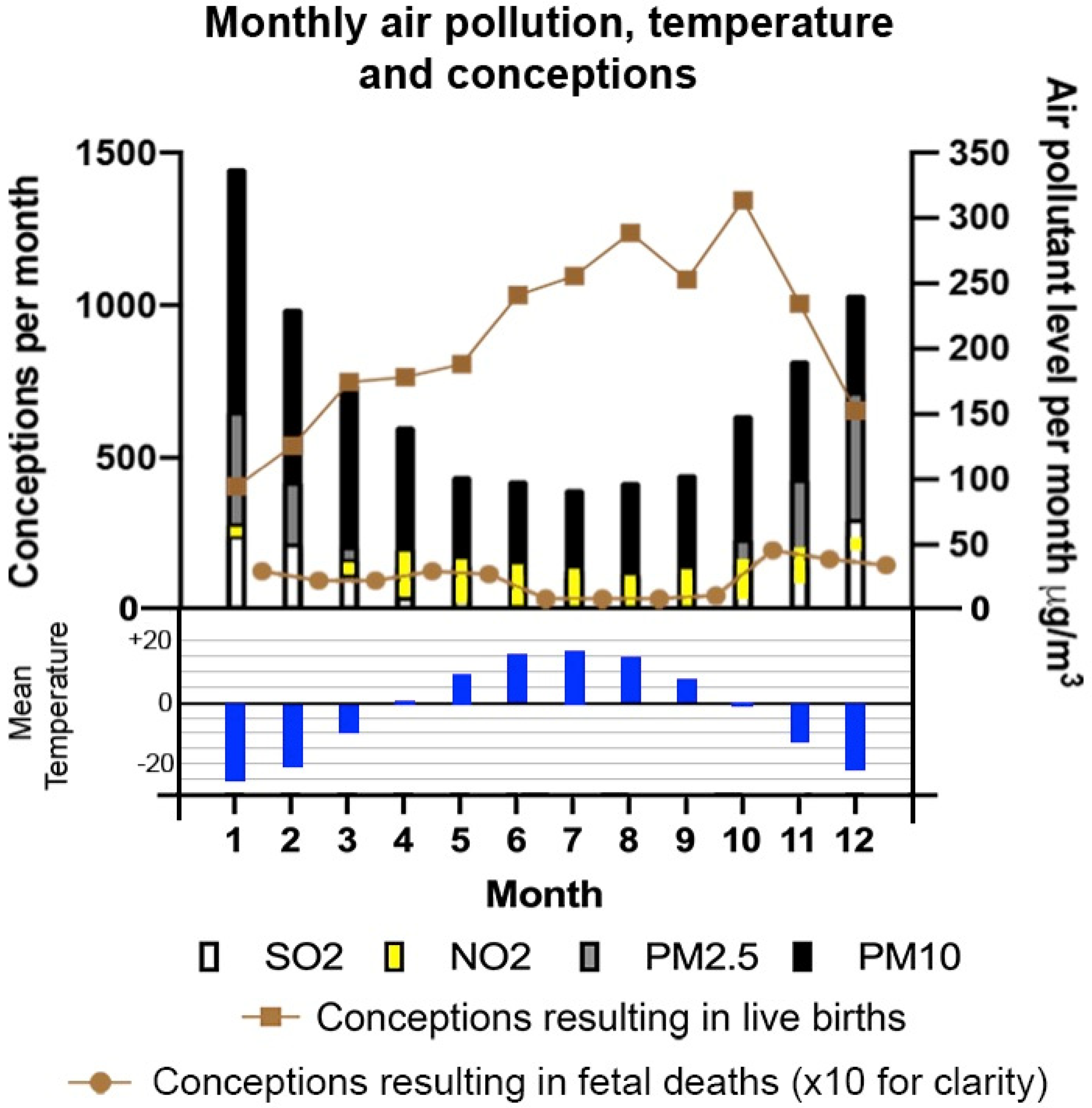
3.2. Conception, Spontaneous Abortion, Winter Temperatures and Air Pollution
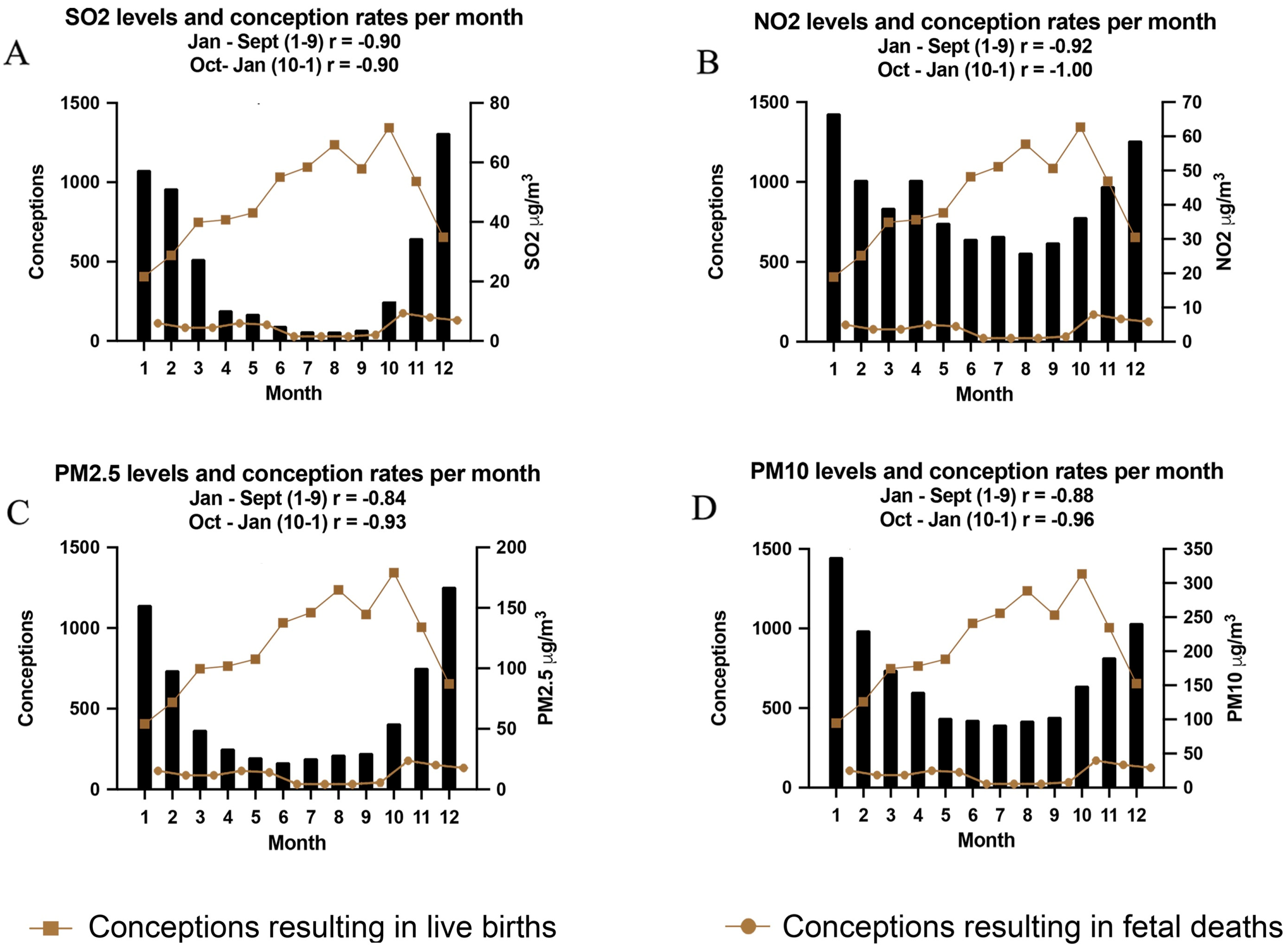
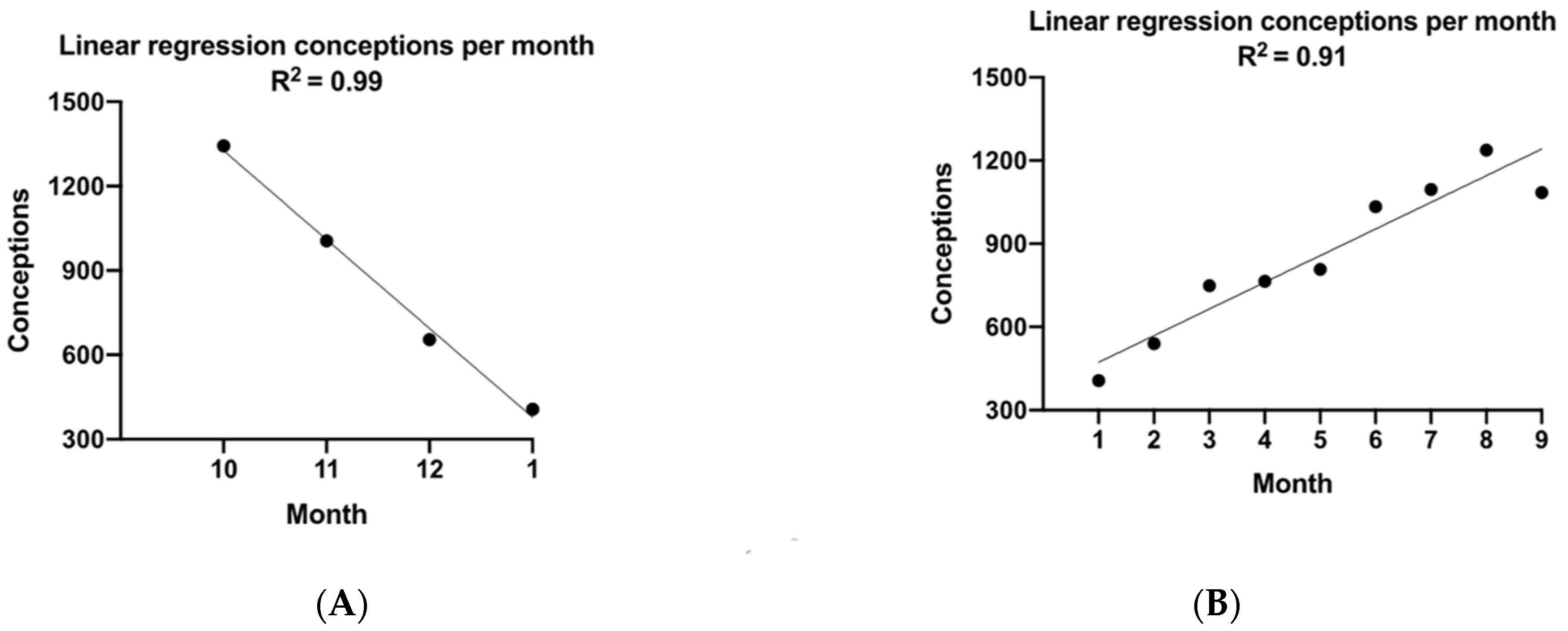
3.3. Conception and SO2 Pollution
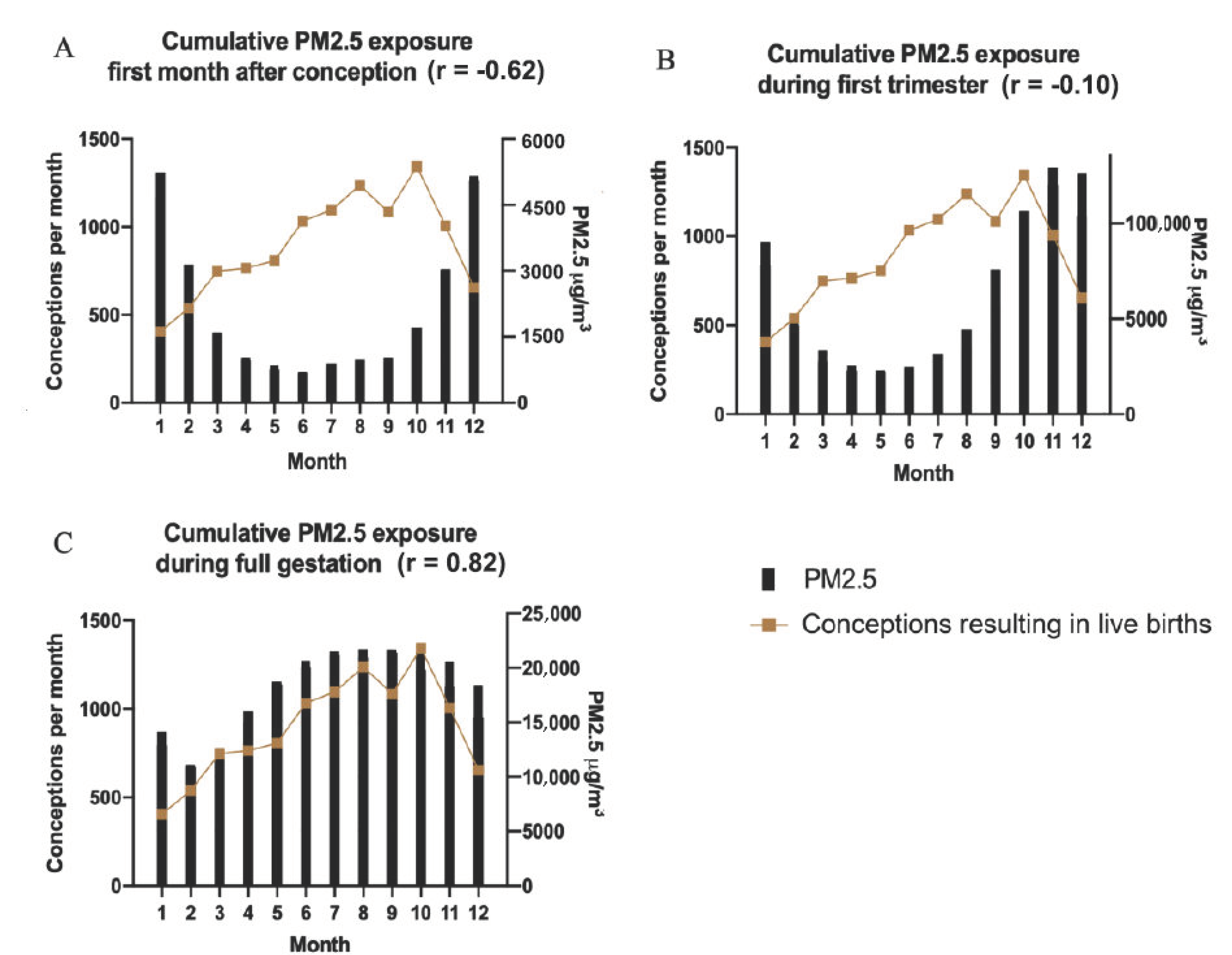
3.4. Conception and PM2.5 Exposure
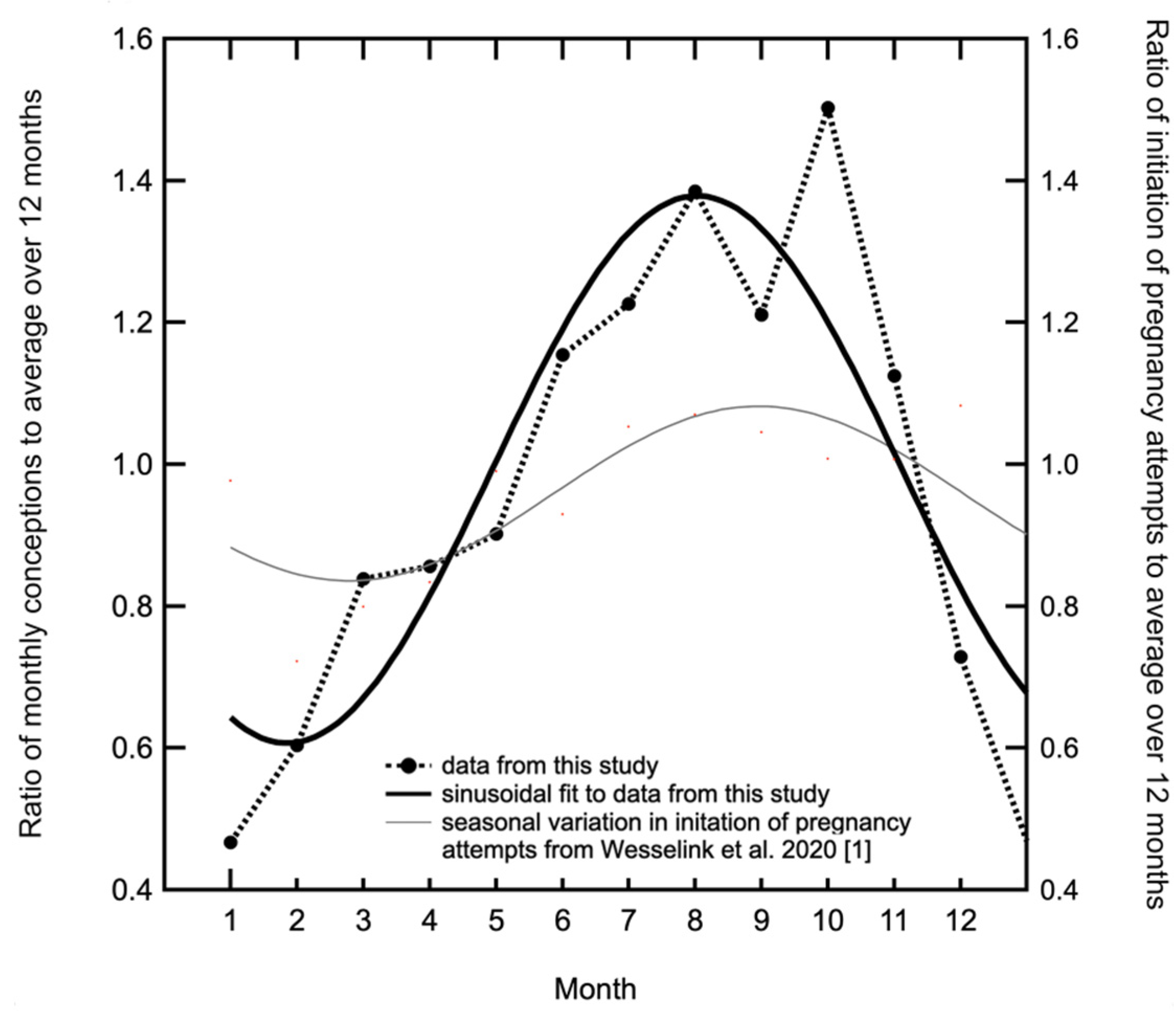
3.5. Seasonal Patterns in Successful Conceptions in UB Compared with Those in North America and Denmark
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wesselink, A.K.; Wise, L.A.; Hatch, E.E.; Mikkelsen, E.M.; Sørensen, H.T.; Riis, A.H.; McKinnon, K.J.; Rothman, K.J. Seasonal patterns in fecundability in North America and Denmark: A preconception cohort study. Hum. Reprod. 2020, 35, 565–572. [Google Scholar] [CrossRef]
- World Health Organization. Ambient (Outdoor) Air Quality and Health; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Boogaard, H.; Walker, K.; Cohen, A.J. Air pollution: The emergence of a major global health risk factor. Int. Health 2019, 11, 417–421. [Google Scholar] [CrossRef]
- Schraufnagel, D.E.; Balmes, J.R.; De Matteis, S.; Hoffman, B.; Kim, W.J.; Perez-Padilla, R.; Rice, M.; Sood, A.; Vanker, A.; Wuebbles, D.J. Health Benefits of Air Pollution Reduction. Ann. Am. Thorac. Soc. 2019, 16, 1478–1487. [Google Scholar] [CrossRef] [PubMed]
- Hoek, G.; Krishnan, R.M.; Beelen, R.; Peters, A.; Ostro, B.; Brunekreef, B.; Kaufman, J. Long-term air pollution exposure and cardio- respiratory mortality: A review. Environ. Health 2013, 12, 43. [Google Scholar] [PubMed] [Green Version]
- Vanker, A.; Wuebbles, D.J. Air Pollution and Noncommunicable Diseases: A Review by the Forum of International Respiratory Societies’ Environmental Committee, Part 2: Air Pollution and Organ Systems. CHEST 2019, 155, 417–426. [Google Scholar]
- Turner, M.; Gracia-Lavedan, M.; Cirac, M.; Castaño-Vinyals, G.; Malats, N.; Tardon, A.; Garcia-Closas, R.; Serra, C.; Carrato, A.; Jones, R.R.; et al. Ambient air pollution and incident bladder cancer risk: Updated analysis of the Spanish Bladder Cancer Study. Int. J. Cancer 2019, 145, 894–900. [Google Scholar] [CrossRef] [PubMed]
- Filippini, T.; Hatch, E.E.; Rothman, K.J.; Heck, J.E.; Park, A.; Crippa, A.; Orsini, N.; Vinceti, M. Association between Outdoor Air Pollution and Childhood Leukemia: A Systematic Review and Dose–Response Meta-Analysis. Environ. Health Perspect. 2019, 127, 046002-1. [Google Scholar] [CrossRef]
- Dashdendev, B.; Fukushima, L.K.; Woo, M.S.; Ganbaatar, E.; Warburton, D. Carbon monoxide pollution and lung function in urban compared with rural Mongolian children. Respirology 2011, 16, 653–658. [Google Scholar] [CrossRef] [PubMed]
- Yoshihara, S.; Munkhbayarlakh, S.; Makino, S.; Ito, C.; Logii, N.; Dashdemberel, S.; Sagara, H.; Fukuda, T.; Arisaka, O. Prevalence of childhood asthma in Ulaanbaatar, Mongolia in 2009. Allergol. Int. 2016, 65, 62–67. [Google Scholar] [CrossRef] [Green Version]
- Shah, P.S.; Balkhaira, T.; on behalf of Knowledge Synthesis Group on Determinants of Preterm/LBW Births. Air pollution and birth outcomes: A systematic Review. Environ. Int. 2011, 37, 498–516. [Google Scholar] [CrossRef] [PubMed]
- Conforti, A.; Mascia, M.; Cioffi, G.; De Angelis, C.; Coppola, G.; De Rosa, P.; Pivonello, R.; Alviggi, C.; De Placido, G. Air pollution and female fertility: A systematic review of literature. Reprod. Biol. Endocrinol. 2018, 16, 117. [Google Scholar] [CrossRef] [PubMed]
- Enkhmaa, D.; Warburton, N.; Javzandulam, B.; Uyanga, J.; Khishigsuren, Y.; Lodoysamba, S.; Enkhtur, S.; Warburton, D. Seasonal ambient air pollution correlates strongly with spontaneous abortion in Mongolia. BMC Pregnancy Childbirth 2014, 14, 146. [Google Scholar] [CrossRef] [Green Version]
- Warburton, D.; Gilliland, F.; Dashdendev, B. Environmental pollution in Mongolia: Effects across the lifespan. Environ. Res. 2013, 124, 65–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warburton, D.; Warburton, N.; Wigfall, C.; Chimedsuren, O.; Lodoisamba, D.; Lodoysamba, S.; Jargalsaikhan, B. Impact of Seasonal Winter Air Pollution on Health across the Lifespan in Mongolia and Some Putative Solutions. Ann. Am. Thorac. Soc. 2018, 15 (Suppl. 2), S86–S90. [Google Scholar] [CrossRef]
- Ganbat, G.; Soyol-Erdene, T.-O.; Jadamba, B. Recent Improvement in Particulate Matter (PM) Pollution in Ulaanbaatar, Mongolia. Aerosol Air Qual. Res. 2020, 20, 2280–2288. [Google Scholar] [CrossRef]
- Hasenkopf, C.A.; Veghte, D.P.; Schill, G.P.; Lodoysamba, S.; Freedman, M.A.; Tolbert, M.A. Ice nucleation, shape, and composition of aerosol particles in one of the most polluted cities in the world: Ulaanbaatar, Mongolia. Atmos. Environ. 2016, 139, 222–229. [Google Scholar] [CrossRef]
- Batmunkh, T.; Kim, Y.J.; Jung, J.S.; Park, K.; Tumendemberel, B. Chemical characteristics of fine particulate matters measured during severe winter haze events in Ulaanbaatar, Mongolia. J. Air Waste Manag. Assoc. 2013, 63, 659–670. [Google Scholar] [CrossRef] [PubMed]
- WHO. Air pollution in Mongolia. Bull. World Health Organ. 2019, 97, 79–80. [Google Scholar] [CrossRef]
- Nieuwenhuijsen, M.J.; Basagana, X.; Dadvand, P.; Martinez, D.; Cirach, M.; Beelen, R.; Jacquemin, B. Air pollution and human fertility rates. Environ. Int. 2014, 70, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Mahalingaiah, S.; Hart, J.E.; Laden, F.; Farland, L.V.; Hewlett, M.M.; Chavarro, J.; Aschengrau, A.; Missmer, S.A. Adult air pollution exposure and risk of infertility in the Nurses’ Health Study II. Hum. Reprod. 2016, 31, 638–647. [Google Scholar] [CrossRef]
- Broughton, D.E.; Moley, K.H. Obesity and female infertility: Potential mediators of obesity’s impact. Fertil. Steril. 2017, 107, 840–847. [Google Scholar] [CrossRef] [Green Version]
- Panopoulou, G.; Tsaklogou, P. Fertility and economic development: Theoretical considerations and cross-country evidence. Appl. Econ. 1999, 31, 1337–1351. [Google Scholar] [CrossRef]
- Pizzorno, J. Environmental Toxins and Infertility. Integr. Med. 2018, 17, 8–11. [Google Scholar]
- Gug, C.; Rațiu, A.; Navolan, D.; Drăgan, I.; Groza, I.M.; Păpurică, M.; Vaida, M.A.; Mozoș, I.; Jurcă, M.C. Incidence and spectrum of chromosome disorders: A retrospective study of 330 cases. Cytogenet. Genome Res. 2019, 158, 171–183. [Google Scholar] [CrossRef]
- Rojansky, N.; Brzezinski, A.; Schenker, J.G. Seasonality in human reproduction: An update. Hum. Reprod. 1992, 7, 735–745. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Liu, L.; Chen, Y.; Yao, C.; Che, Z.; Cao, J. Maternal exposure to particulate matter (PM2.5) and pregnancy outcomes: A meta-analysis. Environ. Sci. Pollut. Res. 2015, 22, 3383–3396. [Google Scholar] [CrossRef] [PubMed]
- Zhu, N.; Ji, X.; Geng, X.; Yue, H.; Li, G.; Sang, N. Maternal PM2.5 exposure and abnormal placental nutrient transport. Ecotoxicol. Environ. Saf. 2021, 207, 111281. [Google Scholar] [CrossRef] [PubMed]
- Yue, H.; Ji, X.; Zhang, Y.; Li, G.; Sang, N. Gestational exposure to PM2.5 impairs vascularization of the placenta. Sci. Total Environ. 2019, 665, 153–161. [Google Scholar] [PubMed]
- Blum, J.L.; Chen, L.-C.; Zelikoff, J.T. Exposure to Ambient Particulate Matter during Specific Gestational Periods Produces Adverse Obstetric Consequences in Mice. Environ. Health Perspect. 2017, 125, 7077020-1. [Google Scholar] [CrossRef] [Green Version]
- Rojansky, N.; Benshushan, A.; Meirsdorf, S.; Lewin, A.; Laufer, N.; Safran, A. Seasonal variability in fertilization and embryo quality rates in women undergoing IVF. Fertil. Steril. 2000, 74, 476–481. [Google Scholar] [CrossRef]
- Becker, S. Seasonal patterns of birth and conception throughout the world. In Temperature and Environmental Effects on the Testis; Zorgniotti, A.W., Ed.; Springer: Boston, MA, USA, 1991; pp. 59–72. [Google Scholar]
- Roenneberg, T.; Ashoff, J. Environmental correlations. J. Biol. Rhythm. 1990, 5, 217. [Google Scholar] [CrossRef] [Green Version]
- Ashary, N.; Tiwari, A.; Modi, D. Embryo Implantation: War in Times of Love. Endocrinology 2018, 159, 1188–1198. [Google Scholar]
- Zeyneloglu, H.B.; Onalan, G. Remedies for Implantation failure. Semin. Reprod. Med. 2014, 32, 297–305. [Google Scholar]
- The, W.-T.; McBain, J.; Rogers, P. What is the contribution of embryo-endometrial asynchrony to implantation failure? J. Assist. Reprod. Genet. 2016, 33, 1419–1430. [Google Scholar]
- Lafuente, R.; García-Blaquez, N.; Jacquemin, B.; Checa, M.A. Outdoor air pollution and sperm quality. Fertil. Steril. 2016, 106, 880–896. [Google Scholar] [CrossRef] [Green Version]
- Guana, Q.; Chena, S.; Wanga, S.; Douc, X.; Luc, Y.; Liangc, J.; Nic, R.; Yang, C.; Wang, H.; Baktash, M.B.; et al. Effects of particulate matter exposure on semen quality: A retrospective cohort study. Ecotoxicol. Environ. Saf. 2020, 193, 110319. [Google Scholar] [CrossRef] [PubMed]
- Clermont, Y. Kinetics of Spermatogenesis in Mammmals. Physiol. Rev. 1972, 52, 198–236. [Google Scholar] [CrossRef] [PubMed]
- Griswold, M. Spermatogenesis: The Commitment to Meiosis. Physiol. Rev. 2016, 96, 1–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gestational Age (weeks) | Number of Births (Male/ Female) | Percentage of Total |
|---|---|---|
| ≤35 | 158 (64/94) | 1 |
| 36 | 180 (71/109) | 2 |
| 37 | 394 (218/176) | 4 |
| 38 | 989 (528/461) | 9 |
| 39 | 2383 (1303/1080) | 22 |
| 40 | 4042 (2069/1973) | 38 |
| 41 | 2569 (1214/1355) | 24 |
| Total | 10715 | 100 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Badarch, J.; Harding, J.; Dickinson-Craig, E.; Azen, C.; Ong, H.; Hunter, S.; Pannaraj, P.S.; Szepesi, B.; Sereenendorj, T.; Davaa, S.; et al. Winter Air Pollution from Domestic Coal Fired Heating in Ulaanbaatar, Mongolia, Is Strongly Associated with a Major Seasonal Cyclic Decrease in Successful Fecundity. Int. J. Environ. Res. Public Health 2021, 18, 2750. https://doi.org/10.3390/ijerph18052750
Badarch J, Harding J, Dickinson-Craig E, Azen C, Ong H, Hunter S, Pannaraj PS, Szepesi B, Sereenendorj T, Davaa S, et al. Winter Air Pollution from Domestic Coal Fired Heating in Ulaanbaatar, Mongolia, Is Strongly Associated with a Major Seasonal Cyclic Decrease in Successful Fecundity. International Journal of Environmental Research and Public Health. 2021; 18(5):2750. https://doi.org/10.3390/ijerph18052750
Chicago/Turabian StyleBadarch, Jargalsaikhan, James Harding, Emma Dickinson-Craig, Colleen Azen, Hilary Ong, Samantha Hunter, Pia S. Pannaraj, Brigitta Szepesi, Tegshjargal Sereenendorj, Sumiya Davaa, and et al. 2021. "Winter Air Pollution from Domestic Coal Fired Heating in Ulaanbaatar, Mongolia, Is Strongly Associated with a Major Seasonal Cyclic Decrease in Successful Fecundity" International Journal of Environmental Research and Public Health 18, no. 5: 2750. https://doi.org/10.3390/ijerph18052750