
Validity of DSM-5 Oppositional Defiant Disorder Symptoms in Children with Intellectual Disability


Abstract
:1. Introduction
1.1. Validity of the ODD Diagnosis in Children with Intellectual Disabilities
1.2. The Present Study
2. Materials and Methods
2.1. Participants
2.2. Measure
2.3. Data Analysis
2.3.1. Analytical Approach
2.3.2. Differential Item Functioning Analysis (DIF)
2.3.3. Analysis of the Impact of Differential Symptom Functioning
3. Results
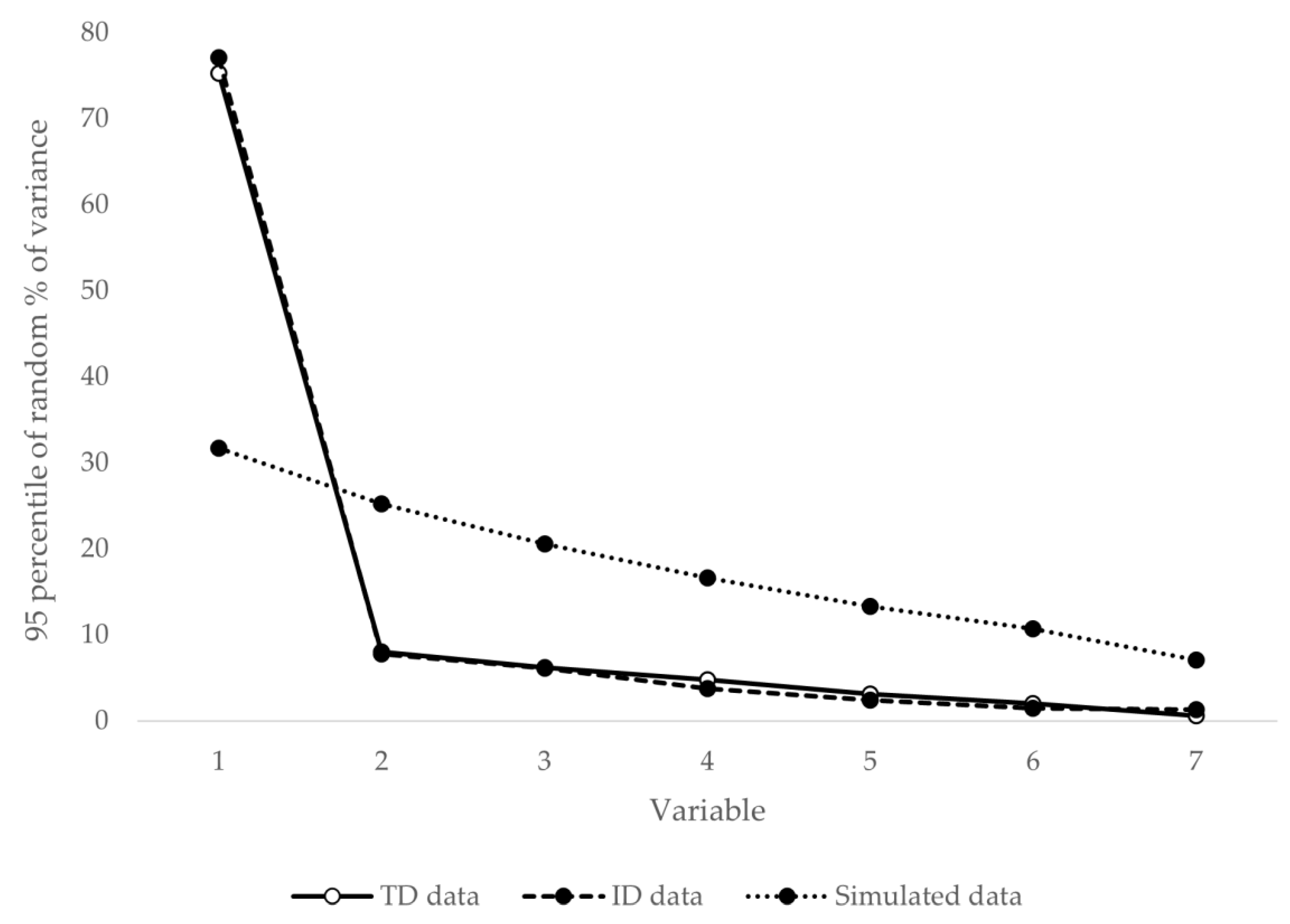
3.1. Unidimensionality and Local Independence
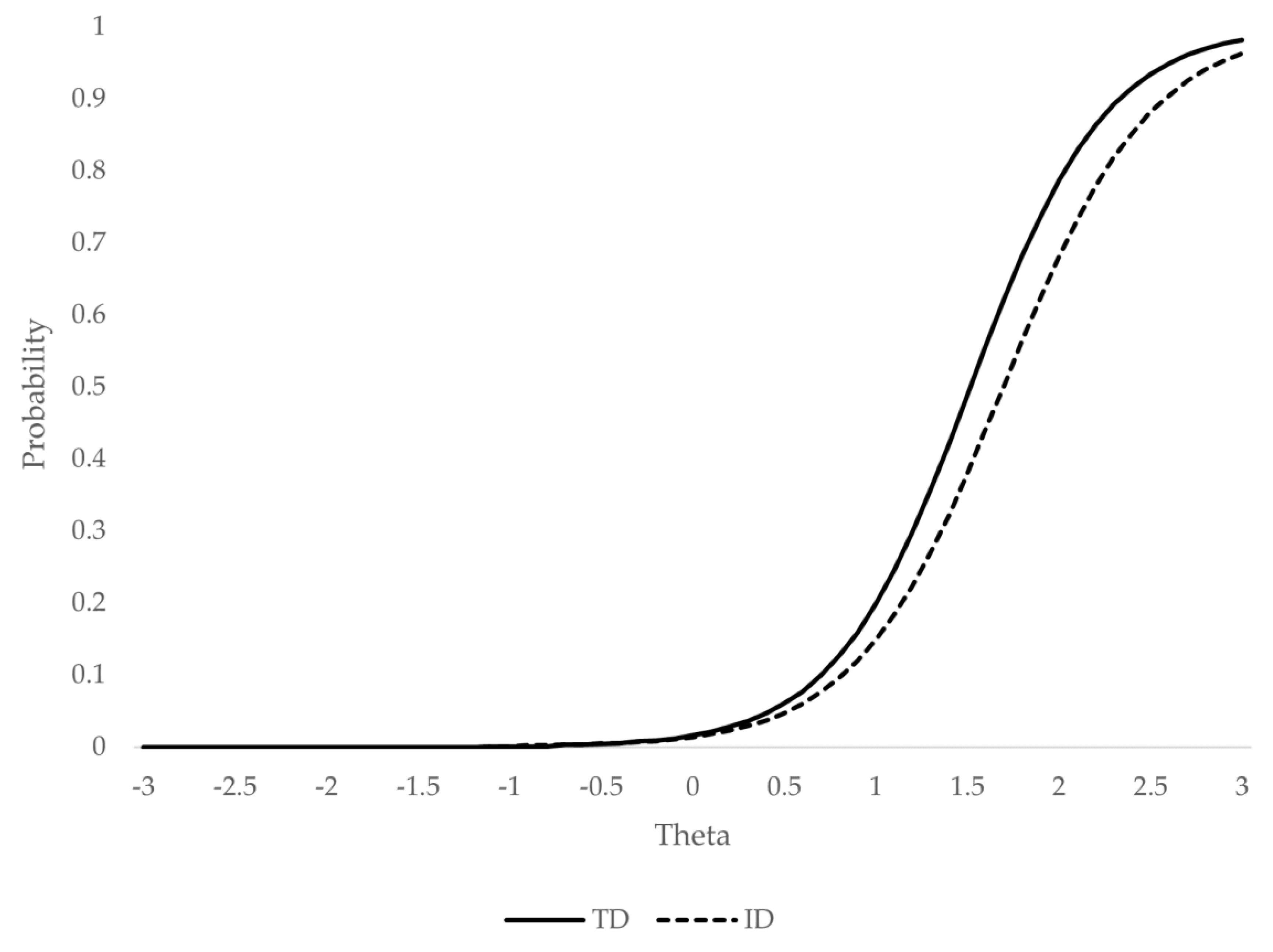
3.2. Analysis of the Differential Functioning of the Symptom
3.3. Analysis of the Size and Impact of Differential Item Functioning
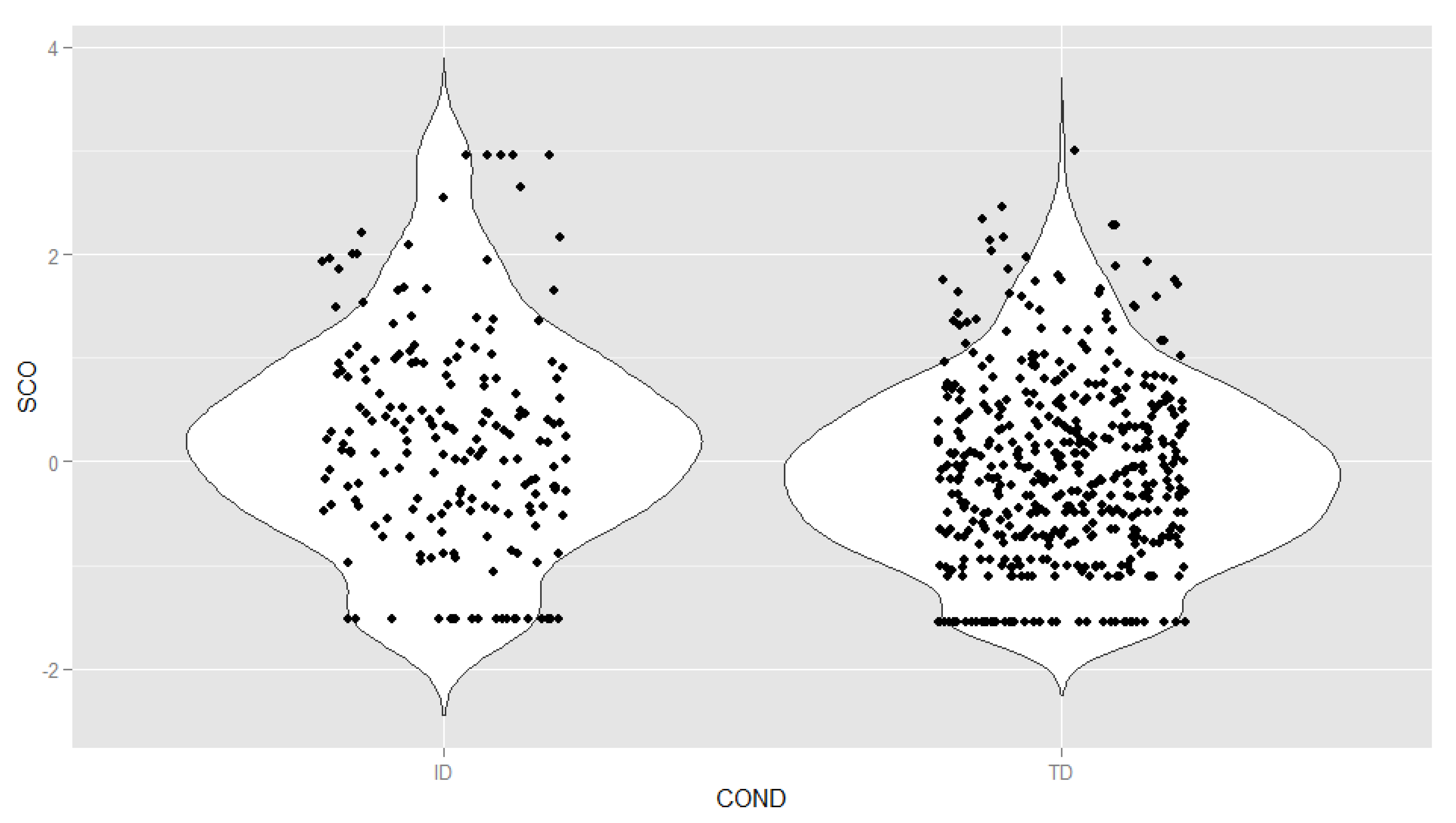
3.4. Distribution of Latent Oppositional Defiant Disorder Scores
4. Discussion
5. Conclusions, Limitations, and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- Dekker, M.C.; Koot, H.M. DSM-IV disorders in children with borderline to moderate intellectual disability. I: Prevalence and impact. J. Am. Acad. Child Adolesc. Psychiatry 2003, 42, 915–922. [Google Scholar] [CrossRef]
- Emerson, E.; Hatton, C. Mental health of children and adolescents with intellectual disabilities in Britain. Br. J. Psychiatry 2007, 191, 493–499. [Google Scholar] [CrossRef]
- Oeseburg, B.; Dijkstra, G.J.; Groothoff, J.W.; Reijneveld, S.A.; Jansen, D.E.M.C. Prevalence of of chronic health conditions in children with intellectual disability: A systematic literature review. Intellect. Dev. Disabil. 2011, 49, 59–85. [Google Scholar] [CrossRef] [Green Version]
- Neece, C.L.; Baker, B.L.; Blacher, J.; Crnic, K.A. Attention-deficit/hyperactivity disorder among children with and without intellectual disability: An examination across time. J. Intellect. Disabil. Res. 2011, 55, 623–635. [Google Scholar] [CrossRef]
- Ahuja, A.; Martin, J.; Langley, K.; Thapar, A. Intellectual disability in children with attention deficit hyperactivity disorder. J. Pediatr. 2013, 163, 890–895. [Google Scholar] [CrossRef] [Green Version]
- Dekker, M.C.; Koot, H.M.; van der Ende, J.; Verhulst, F.C. Emotional and behavioral problems in children and adolescents with and without intellectual disability. J. Child Psychol. Psychiatry 2002, 43, 1087–1098. [Google Scholar] [CrossRef]
- Christensen, L.; Baker, B.L.; Blacher, J. Oppositional defiant disorder in children with intellectual disabilities. J. Ment. Health Res. Intellect. Disabil. 2013, 6, 225–244. [Google Scholar] [CrossRef]
- Neece, C.L.; Christensen, L.; Berkovits, L.D.; Mayo, D. Psychopathology: ADHD, autism spectrum disorders, and other conditions present in early childhood. In Comorbid conditions in individuals with intellectual disabilities; Matson, J.L., Matson, M.L., Eds.; Springer International Publishing: Cham, Switzerland, 2015; pp. 85–107. [Google Scholar]
- Baker, B.L.; Neece, C.L.; Fenning, R.M.; Crnic, K.A.; Blacher, J. Mental disorders in five-year-old children with or without developmental delay: Focus on ADHD. J. Clin. Child Adolesc. Psychol. 2010, 39, 492–505. [Google Scholar] [CrossRef] [PubMed]
- Neece, C.L.; Baker, B.L.; Lee, S.S. ADHD among adolescents with intellectual disabilities: Pre-pathway influences. Res. Dev. Disabil. 2013, 34, 2268–2279. [Google Scholar] [CrossRef] [Green Version]
- Salazar, F.; Baird, G.; Chandler, S.; Tseng, E.; O’sullivan, T.; Howlin, P.; Pickles, A.; Simonoff, E. Co-occurring psychiatric disorders in preschool and elementary school-aged children with autism spectrum disorder. J. Autism Dev. Disord. 2015, 45, 2283–2294. [Google Scholar] [CrossRef] [Green Version]
- Gjevik, E.; Eldevik, S.; Fjæran-Granum, T.; Sponheim, E. Kiddie-SADS reveals high rates of DSM-IV disorders in children and adolescents with autism spectrum disorders. J. Autism Dev. Disord. 2011, 41, 761–769. [Google Scholar] [CrossRef] [Green Version]
- Kanne, S.M.; Abbacchi, A.M.; Constantino, J.N. Multi-informant ratings of psychiatric symptom severity in children with autism spectrum disorders: The importance of environmental context. J. Autism Dev. Disord. 2009, 39, 856–864. [Google Scholar] [CrossRef] [Green Version]
- Guttmann-Steinmetz, S.; Gadow, K.D.; DeVincent, C.J. Oppositional defiant and conduct disorder behaviors in boys with autism spectrum disorder with and without attention-deficit hyperactivity disorder versus several comparison samples. J. Autism Dev. Disord. 2009, 39, 976–985. [Google Scholar] [CrossRef]
- Gadow, K.D.; DeVincent, C.J.; Drabick, D.A.G. Oppositional defiant disorder as a clinical phenotype in children with autism spectrum disorder. J. Autism Dev. Disord. 2008, 38, 1302–1310. [Google Scholar] [CrossRef] [Green Version]
- Whitaker, S.; Read, S. The prevalence of psychiatric disorders among people with intellectual disabilities: An analysis of the literature. J. Appl. Res. Intellect. Disabil. 2006, 19, 330–345. [Google Scholar] [CrossRef]
- Neece, C.L.; Green, S.A.; Baker, B.L. Parenting stress and child behavior problems: A transactional relationship across time. Am. J. Intellect. Dev. Disabil. 2012, 117, 48–66. [Google Scholar] [CrossRef] [Green Version]
- Hastings, R.P.; Daley, D.; Burns, C.; Beck, A.; MacLean, W.E. Maternal distress and expressed emotion: Cross-sectional and longitudinal relationships with behavior problems of children with intellectual disabilities. Am. J. Ment. Retard. 2006, 111, 48–61. [Google Scholar] [CrossRef]
- Baker, B.L.; Blacher, J.; Crnic, K.A.; Edelbrock, C. Behavior problems and parenting stress in families of three-year-old children with and without developmental delays. Am. J. Ment. Retard. 2002, 107, 433–444. [Google Scholar] [CrossRef]
- Mason, J.; Scior, K. “Diagnostic overshadowing” amongst clinicians working with people with intellectual disabilities in the UK. J. Appl. Res. Intellect. Disabil. 2004, 17, 85–90. [Google Scholar] [CrossRef]
- Burns, G.L.; Lee, S.; Servera, M.; McBurnett, K.; Becker, S.P. Child and Adolescent Behavior Inventory—Teacher Version 1.0. Pullman, WA, USA, 2015. [Google Scholar]
- Belmar, M.; Servera, M.; Becker, S.P.; Burns, G.L. Validity of sluggish cognitive tempo in South America: An initial examination using mother and teacher ratings of Chilean children. J. Atten. Disord. 2017, 21, 667–672. [Google Scholar] [CrossRef]
- Preszler, J.; Burns, G.L.; Litson, K.; Geiser, C.; Servera, M. Trait and state variance in oppositional defiant disorder symptoms: A multi-source investigation with Spanish children. Psychol. Assess. 2017, 29, 135–147. [Google Scholar] [CrossRef]
- Sáez, B.; Servera, M.; Becker, S.P.; Burns, L.G. Optimal items for assessing sluggish cognitive tempo in children across mother, father, and teacher ratings. J. Clin. Child Adolesc. Psychol. 2019, 48, 825–839. [Google Scholar] [CrossRef]
- Samejima, F. Graded response model. In Handbook of modern Item Response Theory; van der Linden, W.J., Hambleton, R.K., Eds.; Springer-Verlag: New York, NY, USA, 1997; pp. 85–100. [Google Scholar]
- Cai, L.; Thissen, D.; du Toit, S.H.C. IRTPRO User’s Guide; Scientific Software International: Lincolnwood, IL, USA, 2011. [Google Scholar]
- Timmerman, M.E.; Lorenzo-Seva, U. Dimensionality assessment of ordered polytomous items with parallel analysis. Psychol. Methods 2011, 16, 209–220. [Google Scholar] [CrossRef]
- Thissen, D.; Cai, L.; Bock, R.D. The nominal categories item response model. In Handbook of Polytomous Item Response Theory Models; Nering, M.L., Ostini, R., Eds.; Routledge: Oxfordshire, UK, 2010; pp. 43–75. [Google Scholar]
- Tay, L.; Meade, A.W.; Cao, M. An overview and practical guide to IRT measurement equivalence analysis. Organ. Res. Methods 2015, 18, 3–46. [Google Scholar] [CrossRef]
- Woods, C.M.; Cai, L.; Wang, M. The langer-improved Wald test for DIF testing with multiple groups: Evaluation and comparison to two-group IRT. Educ. Psychol. Meas. 2013, 73, 532–547. [Google Scholar] [CrossRef]
- Meade, A.W. A taxonomy of effect size measures for the differential functioning of items and scales. J. Appl. Psychol. 2010, 95, 728–743. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: New York, NY, USA, 1988. [Google Scholar]
- Barkley, R.A.; Murphy, K.R. Attention-Deficit Hyperactivity Disorder: A Clinical Workbook, 2nd ed.; Guilford Press: New York, NY, USA, 1988. [Google Scholar]
- Reise, S.P.; Waller, N.G. Item Response Theory and clinical measurement. Annu. Rev. Clin. Psychol. 2009, 5, 27–48. [Google Scholar] [CrossRef] [Green Version]
- Schalock, R.L.; Borthwick-Duffy, S.A.; Bradley, V.J.; Buntinx, W.H.E.; Coulter, D.L.; Craig, E.M.; Gomez, S.C.; Lachapelle, Y.; Luckasson, R.; Reeve, A.; et al. Intellectual Disability: Definition, Classification, and Systems of Supports, 11th ed.; American Association on Intellectual and Developmental Disabilities: Washington, DC, USA, 2010; ISBN 978-1-935304-04-3. [Google Scholar]
- Bailey, T.; Totsika, V.; Hastings, R.P.; Hatton, C.; Emerson, E. Developmental trajectories of behaviour problems and prosocial behaviours of children with intellectual disabilities in a population-based cohort. J. Child Psychol. Psychiatry 2019, 60, 1210–1218. [Google Scholar] [CrossRef]
- Bertelli, M.O.; Munir, K.; Harris, J.; Salvador-Carulla, L. “Intellectual developmental disorders”: Reflections on the international consensus document for redefining “mental retardation-intellectual disability” in ICD-11. Adv. Ment. Heal. Intellect. Disabil. 2016, 10, 36–58. [Google Scholar] [CrossRef] [Green Version]
- Deutsch, C.K.; Dube, W.V.; McIlvane, W.J. Attention deficits, attention-deficit hyperactivity disorder, and intellectual disabilities. Dev. Disabil. Res. Rev. 2008, 14, 285–292. [Google Scholar] [CrossRef]
- Levitt, H.M.; Bamberg, M.; Creswell, J.W.; Frost, D.M.; Josselson, R.; Suárez-Orozco, C. Journal article reporting standards for qualitative primary, qualitative meta-analytic, and mixed methods research in psychology: The APA Publications and Communications Board task force report. Am. Psychol. 2018, 73, 26–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, A.D.; Li, Z.; Zumbo, B.D. Decoding the meaning of factorial invariance and updating the practice of multi-group confirmatory factor analysis: A demonstration with TIMSS data. Pract. Assess. Res. Eval. 2007, 12, 1–26. [Google Scholar]
- Antshel, K.M.; Phillips, M.H.; Gordon, M.; Barkley, R.; Faraone, S.V. Is ADHD a valid disorder in children with intellectual delays? Clin. Psychol. Rev. 2006, 26, 555–572. [Google Scholar] [CrossRef] [PubMed]
- Robins, E.; Guze, S.B. Establishment of diagnostic validity in psychiatric illness: Its application to schizophrenia. Am. J. Psychiatry 1970, 126, 983–987. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Symptom 1 | Iteration 1 | Iteration 2 | ||
|---|---|---|---|---|
| Wald χ2 | p | Wald χ2 | p | |
| Argues with adults | 18.1 | 0.006 | 20.9 | 0.002 |
| Loses temper with others | 12.6 | 0.051 | 0 | 1 |
| Actively defies or refuses to obey adults’ requests or rules | 12.3 | 0.055 | 0 | 1 |
| Annoys others on purpose | 20.8 | 0.002 | 21.9 | 0.001 |
| Blames others for his or her mistakes or misbehavior | 3.1 | 0.797 | 0 | 1 |
| Becomes annoyed or irritated by the behavior of others | 9 | 0.173 | 0 | 1 |
| Appears angry or resentful toward others | 7.4 | 0.290 | 0 | 1 |
| Spiteful or vindictive toward others | 3.6 | 0.733 | 0 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arias, V.B.; Aguayo, V.; Navas, P. Validity of DSM-5 Oppositional Defiant Disorder Symptoms in Children with Intellectual Disability. Int. J. Environ. Res. Public Health 2021, 18, 1977. https://doi.org/10.3390/ijerph18041977
Arias VB, Aguayo V, Navas P. Validity of DSM-5 Oppositional Defiant Disorder Symptoms in Children with Intellectual Disability. International Journal of Environmental Research and Public Health. 2021; 18(4):1977. https://doi.org/10.3390/ijerph18041977
Chicago/Turabian StyleArias, Victor B., Virginia Aguayo, and Patricia Navas. 2021. "Validity of DSM-5 Oppositional Defiant Disorder Symptoms in Children with Intellectual Disability" International Journal of Environmental Research and Public Health 18, no. 4: 1977. https://doi.org/10.3390/ijerph18041977