
Associations of Sleep and Health Functioning with Premature Exit from Work: A Cohort Study with a Methodological Emphasis

 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.2.1. Indicator Variables of Sleep and Health Functioning for Repeated-Measures Latent Class Analysis (RMLCA)
Sleep Variables
Health Related Functioning
2.2.2. Other Variables
Outcome Variable
Background Variables
2.3. Statistical Analysis
2.3.1. First Analytical Step: RMLCA Based Classification
2.3.2. Second Analytical Step: Age-at-Event Analysis
3. Results
3.1. Descriptive Characteristics of the Study Sample
3.2. First Analytical Step: RMLCA Based Classification
3.3. Second Analytical Step
3.4. Baseline Self-Reported Sleep Duration Differences between RMLCA Groups
3.5. Third Analytical Step: Conventional Variable Oriented Approach
4. Discussion
4.1. Main Findings
4.2. Interpretation
4.3. Methodological Considerations
4.3.1. Limitations
4.3.2. Strengths
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| BMI | Body Mass Index |
| CI | Confidence Interval |
| HHS | Helsinki Health Study |
| HR | Hazard Ratio |
| JSQ | The Jenkins Sleep Questionnaire |
| LC1 | Latent Class 1 (Reference group) |
| LC2 | Latent Class 2 (Persistent sleep problems) |
| LC3 | Latent Class 3 (Poor health functioning) |
| LC4 | Latent Class 4 (Problematic sleep and health functioning) |
| MET | Metabolic equivalents |
| RMLCA | Repeated Measures Latent Class Analysis |
| SD | Standard Deviation |
| SF-36 | Short-Form 36 General Health Questionnaire |
| BP | Bodily pain subscale |
| GH | General health perceptions |
| GMH | General Mental Health subscale |
| SF | Social Functioning subscale |
References
- Lallukka, T.; Kronholm, E.; Pekkala, J. Work participation trajectories among 1,098,748 Finns: Reasons for premature labour market exit and the incidence of sickness absence due to mental disorders and musculoskeletal diseases. BMC Public Health 2019, 19, 1418. [Google Scholar] [CrossRef] [PubMed]
- Nurminen, M. Working-Life Expectancy in Finland: Development in 2000–2009 and Forecast for 2010–2015. A Multistate Life Table Approach. 2011. Available online: http://urn.fi/URN:NBN:fi-fe2015112619993 (accessed on 9 February 2021).
- Eriksen, W.; Natvig, B.; Bruusgaard, D. Sleep problems: A predictor of long-term work disability? A four-yearprospective study. Scand. J. Public Health 2001, 29, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Lallukka, T.; Haaramo, P.; Lahelma, E.; Rahkonen, O. Sleep problems and disability retirement: A register-based follow-up study. Am. J. Epidemiol. 2011, 173, 871–881. [Google Scholar] [CrossRef] [Green Version]
- Lallukka, T.; Haaramo, P.; Rahkonen, O.; Sivertsen, B. Joint associations of sleep duration and insomnia symptoms with subsequent sickness absence: The Helsinki Health Study. Scand. J. Public Health 2013, 41, 516–523. [Google Scholar] [CrossRef]
- Sivertsen, B.; Overland, S.; Pallesen, S. Insomnia and long sleep duration are risk factors for later work disability. The Hordaland Health Study. J. Sleep Res. 2009, 18, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Åkerstedt, T.; Kecklund, G.; Selen, J. Disturbed Sleep and Fatigue as Predictors of Return from Long-term Sickness Absence. Ind. Health 2010, 48, 209–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laaksonen, M.; Blomgren, J.; Tuulio-Henriksson, A. Sickness allowance histories among disability retirees due to mental disorders: A retrospective case-control study. Scand. J. Public Health 2016, 44, 291–299. [Google Scholar] [CrossRef]
- Mauramo, E.; Lallukka, T.; Lahelma, E.; Pietiläinen, O.; Rahkonen, O. Common mental disorders and sickness absence: A register-linkage follow-up study among Finnish municipal employees. J. Occup. Environ. Med. 2018, 60, 569–575. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E.; Snow, K.K.; Kosinski, M.; Gandek, B. SF-36 Health Survey Manual & Interpretation Guide; The Health Institute, New England Medical Center: Boston, MA, USA, 1993. [Google Scholar]
- Laaksonen, M.; Kääriä, S.M.; Leino-Arjas, P.; Lahelma, E. Different domains of health functioning as predictors of sickness absence—A prospective cohort study. Scand. J. Work Environ. Health 2011, 37, 213–218. [Google Scholar] [CrossRef] [Green Version]
- Bergman, L.R.; Trost, K. The person-oriented versus the variable-oriented approach: Are they complementary, opposites, or exploring different worlds? Merrill-Palmer Q. 2006, 52, 601–634. [Google Scholar] [CrossRef]
- Bergman, L.R.; Magnusson, D. A person-oriented approach in research on developmental psychopathology. Dev. Psychopathol. 1997, 9, 291–319. [Google Scholar] [CrossRef] [PubMed]
- Haaramo, P.; Rahkonen, O.; Lahelma, E.; Lallukka, T. The joint association of sleep duration and insomnia symptoms with disability retirement—A longitudinal, register-linked study. Scand. J. Work Environ. Health 2012, 38, 427–435. [Google Scholar] [CrossRef] [Green Version]
- Reynolds, A.C.; Appleton, S.L.; Gill, T.K. Sickness absenteeism is associated with sleep problems independent of sleep disorders: Results of the 2016 Sleep Health Foundation national survey. Sleep Health 2017, 3, 357–361. [Google Scholar] [CrossRef] [PubMed]
- Lahelma, E.; Aittomäki, A.; Laaksonen, M. Cohort profile: The Helsinki Health Study. Int. J. Epidemiol. 2013, 42, 722–730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saastamoinen, P.; Leino-Arjas, P.; Laaksonen, M.; Martikainen, P.; Lahelma, E. Pain and health related functioning among employees. J. Epidemiol. Community Health 2006, 60, 793–798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenkins, C.D.; Stanton, B.A.; Niemcryk, S.J.; Rose, R.M. A Scale for the Estimation of Sleep Problems in Clinical Research. J. Clin. Epidemiol. 1988, 41, 313–321. [Google Scholar] [CrossRef]
- Duruoz, M.T.; Ulutatar, F.; Ozturk, E.C.; Unal-Ulutatar, C.; Toprak, C.S.; Kayhan, O. Assessment of the validity and reliability of the Jenkins Sleep Scale in ankylosing spondylitis. Int. J. Rheum. Dis. 2018, 22, 275–279. [Google Scholar] [CrossRef]
- Ware, J.E.; Kosinski, M.; Keller, S.D. SF-36 Physical & Mental Health Summary Scales: A User’s Manual; The Health Institute, New England Medical Center: Boston, MA, USA, 1994. [Google Scholar]
- Hagman, E. SF-36 health survey as a measure of perceived health and functional capacity. Finn. Med. J. 1996, 51, 3534–3539. (In Finnish) [Google Scholar]
- Ware, J.E. SF-36 health survey update. Spine 2000, 25, 3130–3139. [Google Scholar] [CrossRef]
- Ware, J.E.; Kosinski, M. Interpreting SF-36 summary health measures: A response. Qual. Life Res. 2001, 10, 405–413. [Google Scholar] [CrossRef] [PubMed]
- Taft, C.; Karlsson, J.; Sullivan, M. Do SF-36 summary component scores accurately summarize subscale scores? Qual. Life Res. 2001, 10, 395–404. [Google Scholar] [CrossRef]
- Taft, C.; Karlsson, J.; Sullivan, M. Interpreting SF-36 summary health measures: A response—Reply. Qual. Life Res. 2001, 10, 415–420. [Google Scholar] [CrossRef]
- Kanerva, N.; Lallukka, T.; Rahkonen, O.; Pietiläinen, O.; Lahti, J. The joint contribution of physical activity, insomnia symptoms and smoking to the cost of short-term sickness absence. Scand. J. Med. Sci. Sports 2019, 29, 440–449. [Google Scholar] [CrossRef] [PubMed]
- Lahti, J.; Laaksonen, M.; Lahelma, E.; Rahkonen, O. The impact of physical activity on sickness absence. Scand. J. Med. Sci. Sports 2010, 20, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Collins, L.M.; Lanza, S.T. Latent Class and Latent Transition Analysis. With Applications in the Social, Behavioral, and Health Sciences; John Wiley & Sons, Inc: Hoboken, NJ, USA, 2010. [Google Scholar]
- Thiebaut, A.C.H.; Benichou, J. Choice of time-scale in Cox’s model analysis of epidemiologic cohort data: A simulation study. Stat. Med. 2004, 23, 3803–3820. [Google Scholar] [CrossRef] [PubMed]
- Ferrie, J.E.; Vahtera, J.; Kivimäki, M. Diagnosis-specific sickness absence and all-cause mortality in the GAZEL study. J. Epidemiol. Community Health 2009, 63, 50–55. [Google Scholar] [CrossRef]
- Vahtera, J.; Westerlund, H.; Ferrie, J.E. All-cause and diagnosis-specific sickness absence as a predictor of sustained suboptimal health: A 14-year follow-up in the GAZEL cohort. J. Epidemiol. Community Health 2010, 64, 311–317. [Google Scholar] [CrossRef] [Green Version]
- Baglioni, C.; Battagliese, G.; Feige, B. Insomnia as a predictor of depression: A meta-analytic evaluation of longitudinal epidemiological studies. J. Affect. Disord. 2011, 135, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Paunio, T.; Korhonen, T.; Hublin, C.; Partinen, M.; Koskenvuo, K.; Koskenvuo, M. Poor sleep predicts symptoms of depression and disability retirement due to depression. J. Affect. Disord. 2015, 172, 381–389. [Google Scholar] [CrossRef]
- Sivertsen, B.; Bjornsdottir, E.; Overland, S.; Bjorvatn, B.; Salo, P. The joint contribution of insomnia and obstructive sleep apnoea on sickness absence. J. Sleep Res. 2013, 22, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Svedberg, P.; Mather, L.; Bergström, G.; Lindfors, P.; Blom, V. Time pressure and sleep problems due to thoughts about work as risk factors for future sickness absence. Int. Arch. Occup. Environ. Health 2018, 91, 1051–1059. [Google Scholar] [CrossRef] [Green Version]
- Rahkonen, O.; Lallukka, T.; Kronholm, E.; Vahtera, J.; Lahelma, E.; Laaksonen, M. Sleep problems and sickness absence among middle-aged employees. Scand. J. Work Environ. Health 2012, 38, 47–55. [Google Scholar] [CrossRef] [Green Version]
- Lallukka, T.; Øverland, S.; Haaramo, P.; Saastamoinen, P.; Bjorvatn, B.; Sivertsen, B. The joint contribution of pain and insomnia to sickness absence and disability retirement: A register-linkage study among Norwegian and Finnish employees. Eur. J. Pain 2014, 18, 883–892. [Google Scholar] [CrossRef]
- Törnroos, M.; Hakulinen, C.; Hintsanen, M. Reciprocal Relationships between Psychosocial Work Characteristics and Sleep Problems: A Two-wave Study. Work Stress 2017, 31, 63–81. [Google Scholar] [CrossRef]
- Leger, D.; Scheuermaier, K.; Philip, P.; Paillard, M.; Guilleminault, C. SF-36: Evaluation of quality of life in severe and mild insomniacs compared with good sleepers. Psychosom. Med. 2001, 63, 49–55. [Google Scholar] [CrossRef] [Green Version]
- Biddle, D.; Hermens, D.F.; Lallukka, T.; Aji, M.; Glozier, N. Insomnia symptoms and short sleep duration predict trajectory of mental health symptoms. Sleep Med. 2019, 54, 53–61. [Google Scholar] [CrossRef] [Green Version]
- Lallukka, T.; Kaikkonen, R.; Härkänen, T. Sleep and sickness absence: A nationally representative register-based follow-up study. Sleep 2014, 37, 1413–1425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, C.B.; Gordon, C.J.; Toubia, L. Agreement between simple questions about sleep duration and sleep diaries in a large online survey. Sleep Health 2015, 1, 133–137. [Google Scholar] [CrossRef]
- Dziak, J.J.; Lanza, S.T. SAS Graphics Macros for Latent Class Analysis Users’ Guide. (Version 2.0); The Methodology Center, Penn State: University Park, PA, USA, 2015. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| All (n = 5148) | Women (n = 4204) | Men (n = 944) | |
|---|---|---|---|
| Sociodemographic characteristics | |||
| Gender (%) | 82 | 18 | |
| Age (mean ± SD) | 55.5 ± 6.6 | 55.2 ± 6.5 | 56.7 ± 6.5 |
| Marital status (%) | |||
| Married or co-habiting | 70.7 | 68.6 | 79.9 |
| Single | 12.6 | 13.2 | 9.8 |
| Separated or widowed | 16.7 | 18.2 | 10.3 |
| Education (%) | |||
| Basic | 38.2 | 39.0 | 34.7 |
| Secondary | 33.9 | 35.1 | 28.6 |
| Higher | 27.9 | 25.9 | 36.6 |
| Occupational class (%) | |||
| Managers & professionals | 31.9 | 28.3 | 47.9 |
| Semi-professionals | 21.4 | 21.7 | 20.4 |
| Routine non-manual | 33.0 | 38.3 | 9.2 |
| Manual workers | 13.7 | 11.7 | 22.4 |
| Health behavior | |||
| Leisure-time or commuting physical activity (%) | |||
| Physically inactive (MET < 14) | 23.2 | 23.4 | 22.6 |
| Physically active (MET ≥ 14) | 76.8 | 76.6 | 77.4 |
| Current smoking (%) | |||
| Yes (%) | 21.3 | 21.0 | 22.9 |
| Alcohol (%) | |||
| Not at all | 6.9 | 7.2 | 5.4 |
| max once/month | 32.3 | 35.0 | 20.3 |
| 2–4 times/month | 37.0 | 36.9 | 37.3 |
| 2–7 times/week | 23.9 | 21.0 | 37.0 |
| Health status | |||
| Limiting longstanding illness (%) | 30.5 | 30.8 | 29.4 |
| BMI (mean ± SD) | 25.4 ± 4.3 | 25.2 ± 4.4 | 26.3 ± 3.7 |
| Considered retiring before your actual retirement age (%) | |||
| No, I have not | 50.4 | 51.4 | 46.2 |
| Sometimes | 33.2 | 33.0 | 34.5 |
| Often | 15.1 | 14.4 | 17.9 |
| I have already submitted an application | 1.3 | 1.2 | 1.4 |
| Estimated ability to continue at your work until your normal retirement age (%) | |||
| Most likely | 57.5 | 56.0 | 63.9 |
| Not sure | 34.7 | 36.3 | 27.8 |
| I do not think so | 7.8 | 7.7 | 8.3 |
| All (n = 5148) | Women (n = 4204) | Men (n = 944) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Phase1 | Phase2 | Phase3 | Phase1 | Phase2 | Phase3 | Phase1 | Phase2 | Phase3 | |
| % | % | % | % | % | % | % | % | % | |
| Jenkins insomnia-related symptoms | |||||||||
| Difficulties falling asleep: | 7.4 | 11.1 | 10.9 | 7.7 | 11.5 | 11.3 | 6.0 | 9.0 | 9.2 |
| Nocturnal awakenings 1 | 22.4 | 30.4 | 29.9 | 22.8 | 31.1 | 30.3 | 20.2 | 27.3 | 28.2 |
| Non-restorative sleep 2 | 20.5 | 22.0 | 19.0 | 21.2 | 23.0 | 19.7 | 17.7 | 17.3 | 15.7 |
| SF-36 Health functioning subscales | |||||||||
| SF-36 BP: poor | 26.8 | 30.3 | 30.8 | 25.2 | 28.9 | 29.4 | 33.6 | 36.6 | 37.3 |
| SF-36 GH: poor | 25.6 | 32.0 | 33.2 | 25.5 | 32.5 | 34.1 | 25.9 | 29.9 | 29.0 |
| SF-36 GMH: poor | 18.7 | 18.8 | 17.1 | 17.5 | 17.7 | 16.2 | 24.5 | 23.7 | 21.2 |
| SF-36 SF: poor | 33.9 | 35.0 | 33.7 | 32.2 | 33.6 | 32.1 | 41.4 | 41.0 | 40.7 |
| Indicators of Latent Classes | G 2 | BIC | Proportion of Individual’s in Each of the Latent Classes (%) and Mean Classification Probability in Each Class | Chosen/Rejected | |||
|---|---|---|---|---|---|---|---|
| LC1% rel. | LC2% rel. | LC3% rel. | LC4% rel. | ||||
| Bodily pain (BP) + Difficulties of initiating sleep | 86.4 | 317.1 | 62.0% | 6.4% | 25.5% | 6.2% | chosen |
| 0.890 | 0.724 | 0.840 | 0.835 | ||||
| Bodily pain (BP) + Nocturnal awakenings | 164.2 | 395.0 | 49.1% | 17.9% | 20.5% | 12.6% | chosen |
| 0.870 | 0.725 | 0.774 | 0.827 | ||||
| Bodily pain (BP) + Non-restorative sleep | 195.8 | 426.5 | 55.0% | 11.7% | 23.3% | 10.0% | chosen |
| 0.873 | 0.799 | 0.755 | 0.820 | ||||
| General health perception (GH) + Difficulties of initiating sleep | 75.4 | 306.2 | 63.9% | 5.2% | 24.3% | 6.7% | chosen |
| 0.920 | 0.763 | 0.861 | 0.818 | ||||
| General health perception (GH) + Nocturnal awakenings | 410.1 | 640.9 | 53.0% | 8.0% | 27.5% | 11.4% | rejected 1 |
| 0.957 | 0.873 | 0.891 | 0.909 | ||||
| General health perception (GH) + Nonrestorative sleep | 212.1 | 442.9 | 58.3% | 10.9% | 19.9% | 11.1% | chosen |
| 0.900 | 0.801 | 0.785 | 0.829 | ||||
| General mental health (GMH) + Difficulties of initiating sleep | 133.0 | 363.6 | 73.0% 0.925 | 7.0% 0.743 | 15.0% 0.821 | 5.0% 0.858 | chosen |
| General mental health (GMH) + Nocturnal awakenings | 212.2 | 443.0 | 55.6% | 12.4% | 16.6% | 15.4% | rejected 2 |
| 0.905 | 0.864 | 0.627 | 0.839 | ||||
| General mental health (GMH) + Nonrestorative sleep | 247.7 | 478.4 | 67.9% | 11.4% | 10.8% | 9.9% | |
| 0.921 | 0.762 | 0.777 | 0.912 | chosen | |||
| Social functioning (SF) + Difficulties of initiating sleep | 143.7 | 373.6 | 58.6% 0.892 | 7.1% 0.762 | 28.2% 0.810 | 6.2% 0.752 | chosen |
| Social functioning (SF) + Nocturnal awakenings | 183.6 | 414.3 | 48.0% | 17.3% | 23.0% | 11.8% | chosen |
| 0.857 | 0.770 | 0.800 | 0.757 | ||||
| Social functioning (SF) + Nonrestorative sleep | 254 | 485 | 56.4% | 8.7% | 20.3% | 14.6% | |
| 0.904 | 0.766 | 0.731 | 0.876 | chosen | |||
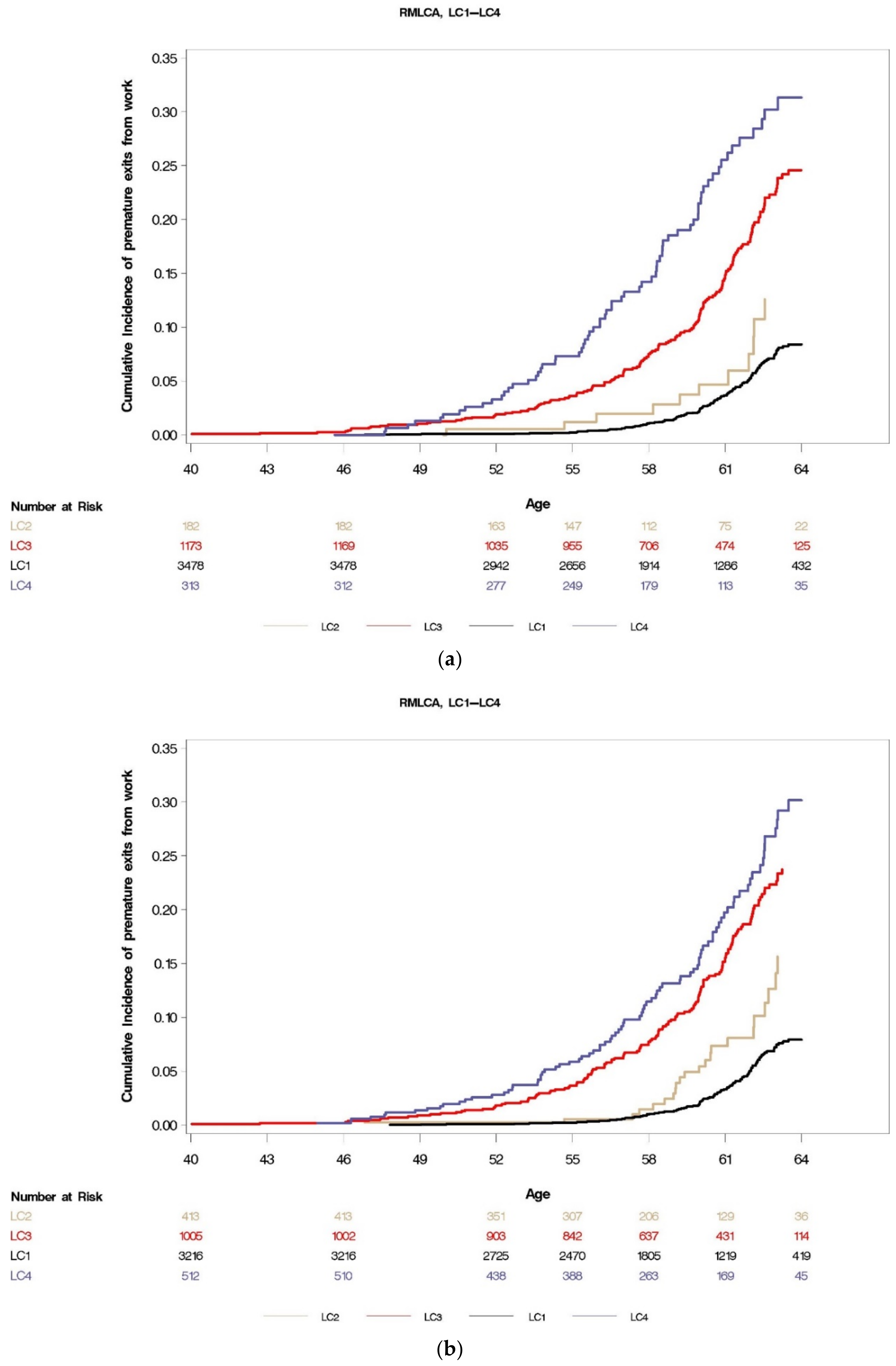
| SF-36: GH + Difficulties in initiating sleep as indicators of RMLC: 4 class solution (See also Figure 2a) | |||||
| Bivariable Cox model 1 | Adjusted Cox model 2 | ||||
| df = 3; Wald χ2 = 190.0; p < 0.0001 | df = 3; Wald χ2 = 103.1; p < 0.0001 | ||||
| LC | HR | 95% CL | LC | HR | 95% CL |
| LC1 | ref | - | LC1 | ref | - |
| LC2 | 1.69 | 0.91–3.13 | LC2 | 1.45 | 0.73–2.88 |
| LC3 | 3.96 | 3.12–5.03 | LC3 | 3.10 | 2.35–4.10 |
| LC4 | 6.48 | 4.78–8.78 | LC4 | 5.17 | 3.68–7.28 |
| SF-36: GMH + Nonrestorative sleep as indicators of RMLC: 4 class solution | |||||
| Bivariable Cox model 1 | Adjusted Cox model 2 | ||||
| df = 3; Wald χ2 = 64.4; p < 0.0001 | df = 3; Wald χ2 = 43.4; p < 0.0001 | ||||
| LC | HR | 95% CL | LC | HR | 95% CL |
| LC1 | ref | - | LC1 | ref | - |
| LC2 | 2.42 | 1.78–3.29 | LC2 | 2.27 | 1.62–3.17 |
| LC3 | 2.26 | 1.67–3.05 | LC3 | 2.07 | 1.50–2.87 |
| LC4 | 2.41 | 1.78–3.25 | LC4 | 2.19 | 1.58–3.05 |
| SF-36: GH + Nonrestorative sleep as indicators of RMLC: 4 class solution (See also Figure 2b) | |||||
| Bivariable Cox model 1 | Adjusted Cox model 2 | ||||
| df = 3; Wald χ2 = 177.7; p < 0.0001 | df = 3; Wald χ2 = 99.3; p < 0.0001 | ||||
| LC | HR | 95% CL | LC | HR | 95% CL |
| LC1 | ref | - | LC1 | ref | - |
| LC2 | 1.83 | 1.15–2.9 | LC2 | 1.95 | 1.18–3.21 |
| LC3 | 4.21 | 3.27–5.43 | LC3 | 3.20 | 2.39–4.28 |
| LC4 | 5.60 | 4.19–7.46 | LC4 | 4.88 | 3.52–6.77 |
| SF-36: GMH + difficulties in initiating sleep as indicators of RMLC: 4 class solution | |||||
| Bivariable Cox model 1 | Adjusted Cox model 2 | ||||
| df = 3; Wald χ2 = 65.4; p < 0.0001 | df = 3; Wald χ2 = 37.2; p < 0.0001 | ||||
| LC | HR | 95% CL | LC | HR | 95% CL |
| LC1 | ref | - | LC1 | ref | - |
| LC2 | 2.63 | 1.96–3.52 | LC2 | 2.11 | 1.53–2.90 |
| LC3 | 1.79 | 1.33–2.42 | LC3 | 1.64 | 1.18–2.28 |
| LC4 | 2.88 | 1.96–4.22 | LC4 | 2.54 | 1.69–3.81 |
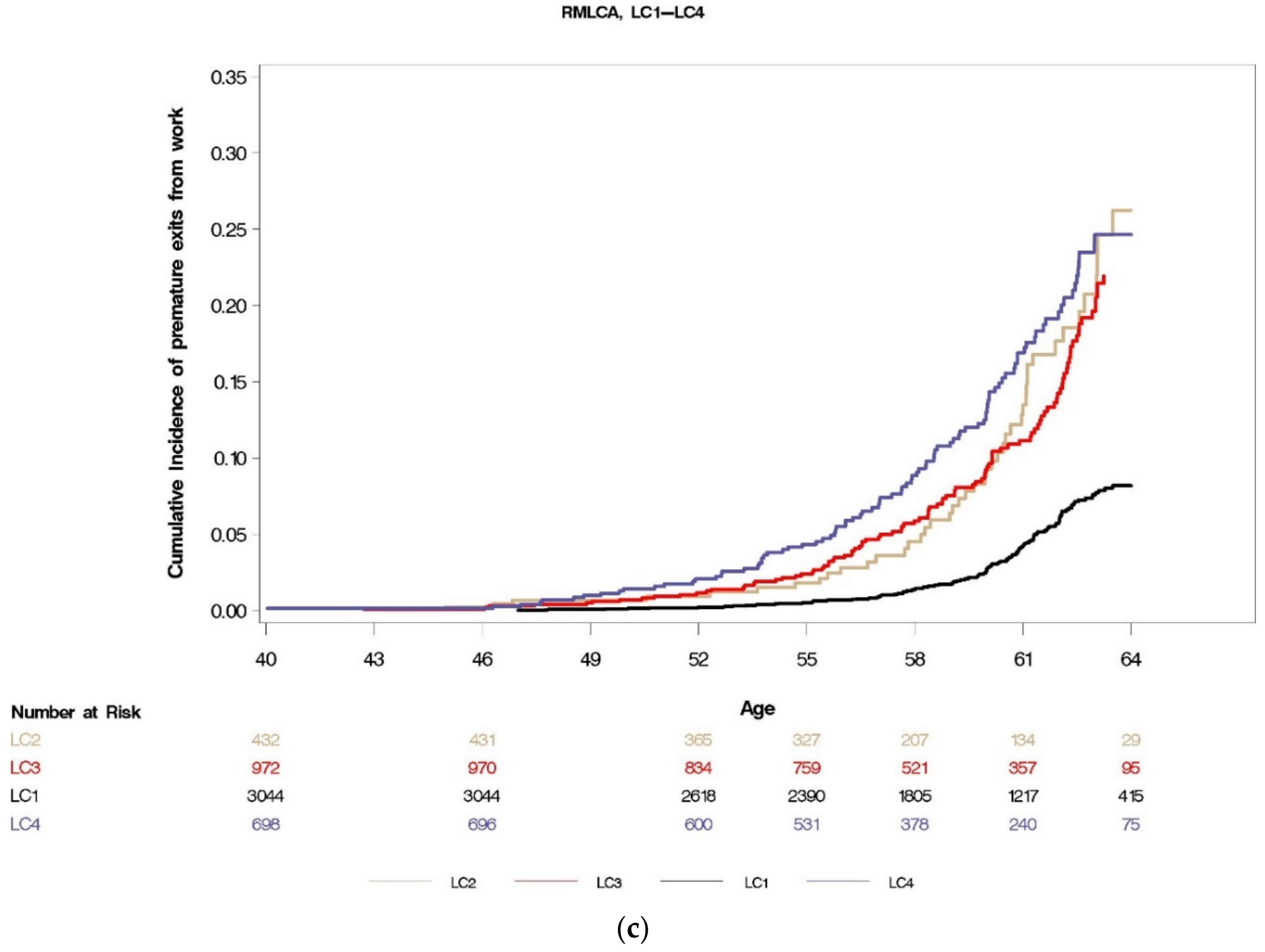
| SF-36: SF + Nonrestorative sleep as indicators of RMLC: 4 class solution (See also Figure 2c) | |||||
| Bivariable model 1 | Adjusted model 2 | ||||
| df = 3; Wald χ2 = 111.6; p < 0.0001 | df = 3; Wald χ2 = 70.1; p = < 0.0001 | ||||
| LC | HR | 95% CL | LC | HR | 95% CL |
| LC1 | ref | - | LC1 | ref | - |
| LC2 | 3.14 | 2.22–4.43 | LC2 | 2.96 | 2.04–4.31 |
| LC3 | 2.89 | 2.21–3.78 | LC3 | 2.48 | 1.84–3.33 |
| LC4 | 3.78 | 2.87–4.98 | LC4 | 3.27 | 2.40–4.46 |
| SF-36: PB + Nocturnal awakenings as indicators of RMLC: 4 class solution | |||||
| Bivariable Cox model 1 | Adjusted Cox model 2 | ||||
| df = 3; Wald χ2 = 147.8; p < 0.0001 | df = 3; Wald χ2 = 69.6; p < 0.0001 | ||||
| LC | HR | 95% CL | LC | HR | 95% CL |
| LC1 | ref | - | LC1 | ref | - |
| LC2 | 1.23 | 0.87–1.74 | LC2 | 1.18 | 0.81–1.71 |
| LC3 | 2.93 | 2.21–3.88 | LC3 | 2.06 | 1.50–2.82 |
| LC4 | 4.68 | 3.56–6.14 | LC4 | 3.41 | 2.51–4.62 |
| RMLCA Group | Maximum and Minimum Predictive Power (HR) of a Given RMLCA Group in Fully Adjusted Cox Models Predicting Premature Exit from Work | Self-Reported Baseline Sleep Duration (%) | ||
|---|---|---|---|---|
| ≤6 h | 7–8 h | ≥9 h | ||
| LC1 Reference | - | 18.7 * | 77.6 * | 3.7 * |
| LC4 Problematic sleep | HR max 5.17 | 42.4 | 52.8 | 4.9 |
| and health functioning | HR min 2.19 | 41.8 | 55.9 | 2.3 |
| LC3 Poor health functioning | HR max 3.20 | 22.9 | 72.9 | 4.2 |
| HR min 1.64 | 25.4 | 70.8 | 3.8 | |
| LC2 Persistent sleep problems | HR max 2.96 | 30.2 | 66.5 | 3.3 |
| HR min 1.18 | 25.3 | 72.2 | 2.5 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kronholm, E.; Marshall, N.S.; Mänty, M.; Lahti, J.; Lahelma, E.; Pietiläinen, O.; Rahkonen, O.; Lallukka, T. Associations of Sleep and Health Functioning with Premature Exit from Work: A Cohort Study with a Methodological Emphasis. Int. J. Environ. Res. Public Health 2021, 18, 1725. https://doi.org/10.3390/ijerph18041725
Kronholm E, Marshall NS, Mänty M, Lahti J, Lahelma E, Pietiläinen O, Rahkonen O, Lallukka T. Associations of Sleep and Health Functioning with Premature Exit from Work: A Cohort Study with a Methodological Emphasis. International Journal of Environmental Research and Public Health. 2021; 18(4):1725. https://doi.org/10.3390/ijerph18041725
Chicago/Turabian StyleKronholm, Erkki, Nathaniel S. Marshall, Minna Mänty, Jouni Lahti, Eero Lahelma, Olli Pietiläinen, Ossi Rahkonen, and Tea Lallukka. 2021. "Associations of Sleep and Health Functioning with Premature Exit from Work: A Cohort Study with a Methodological Emphasis" International Journal of Environmental Research and Public Health 18, no. 4: 1725. https://doi.org/10.3390/ijerph18041725